SAs response to COVID-19 worsens the plight of waste reclaimers
- Melanie Samson
The clock is ticking: in the absence of government support, not being able to work means waste reclaimers don't have money to buy food.
Lockdowns to prevent the spread of the deadly coronavirus are dramatically transforming people’s daily lives across the world. One thing that remains unchanged is that we continue to produce massive amounts of waste each day.
This is thanks in large part to reclaimers who, through what I call their ‘separation outside source’ system, separate people’s recyclables, just outside their homes and at landfills. After salvaging the recyclables, the reclaimers haul them great distances, sort and clean them. They sell the materials to small buyback centres, who sell them to larger buyers. The recyclables are subsequently resold for export or as inputs for production.
South Africa’s 60,000 to 90,000 reclaimers collect an astonishing 80% to 90% of used packaging and paper that are recycled, providing crucial inputs for production and saving municipalities up to R750 million a year (US$41.7 million) in potential landfill costs.
Despite their significant contributions, reclaimers in South Africa (as in most countries) are not paid for the service they provide. Instead, they earn a pittance when they sell what they collect.
South Africa’s measures to flatten the COVID-19 infection curve are making reclaimers’ situation even worse. Since the country went on lockdown at midnight on March 26, 2020, reclaimers have been locked out of landfills and cannot work in the streets. They have also been excluded from all forms of government support.
A history of exclusion
That the measures announced by the government leave reclaimers out should come as no surprise. Current government policies on waste and recycling do not meaningfully include reclaimers. Their central role in the sector is overlooked by an economic model that assumes that a part of the economy can be hived off as “informal” and deemed irrelevant to policy development.
This has enabled municipalities to completely ignore the separation outside source system and implement recycling programmes that dispossess reclaimers. This is not unique to South Africa.
The exclusion of reclaimers continues through the government’s responses to COVID-19. Waste management was declared an essential service, allowing workers in this sector to keep working. Not so reclaimers. This, despite their crucial role in municipal solid waste management systems. Like millions of other workers considered informal, they are not eligible for government financial support programmes.
Many governments are disseminating information on how long the virus remains on different materials so that people can protect themselves when they purchase and use them. But, there are no public service announcements on how to dispose of the same products to minimise risks for reclaimers.
In South Africa, as in countries like Brazil and India, this burden has fallen on reclaimers.
An essential service
According to information gathered by the Global Alliance of Waste Pickers, reclaimers in a number of countries have been affected in similar ways by government responses to COVID-19 that ignore them. Some core demands are emerging. These include permission to continue working; personal protective equipment, soap and washing stations; free rapid testing and health care; a basic income; and food parcels.
In addition, reclaimers in South Africa are demanding inclusion in the R500 million (US$27.8 million) government fund to cushion small businesses from the ravages of the virus. The South African Waste Pickers Association and the African Reclaimers Organisation want a declaration that they are essential service providers, a simple process to obtain permits, and protective equipment.
The reclaimers’ demands are in line with the “Guideline on Waste Picker Integration for South Africa”, which recognises and values reclaimers’ role in the sector. Although it must still be published, the guideline was agreed by all stakeholders. The pandemic creates an opportunity for the government to implement the guideline and support reclaimers.
No time to waste
Whether and how industry and municipalities that rely on reclaimers for profits and savings will assist them is unclear. But the clock is ticking: reclaimers earn their incomes daily and are already struggling. In the absence of government support, not being able to work means they don’t have money to buy food.
It is crucial that the government designate reclaimers as essential service providers without delay, and give them masks, gloves, protective gear, sanitisers and access to health care. They need access to public spaces and buildings to store their materials, as well as trucks to transport them. Reclaimers need public washing stations, food packages, rapid testing and income support needed by millions of other South Africans.
Many livelihoods are at risk. Resources must be made available to fund reclaimers, along with other essential activities, vulnerable workers and the unemployed.
Crowdsourcing: Scale of COVID-19 calls for new approaches to research
- Chris William Callaghan
Crowdsourcing is a promising approach to biomedical research and development (R&D) and could produce solutions to pandemics like this one.
COVID-19 is not the world’s first pandemic. Nor is it the only type of big problem that the world faces. Environmental degradation and drug-resistant diseases are other examples.
What’s special about the new coronavirus is the speed with which it has arisen and multiplied.
The current system of scientific and academic research can’t respond fast enough to problems like these, especially when data is still being generated. But there are potentially ways of overcoming this mismatch.
I propose that crowdsourcing is a promising approach to biomedical research and development (R&D) and could produce solutions to pandemics like this one.
The biomedical research and development industry largely responds to private incentives – even if subsidised by governments. Drugs are more likely to be developed for wealthy markets offering opportunities for chronic medicines that need to be taken for the rest of one’s life. This is because drug companies face the challenge of very large initial investments which they might not be able to recoup if a drug is not profitable. There’s less incentive to do R&D that could have wider social benefits.
A large-scale response to the COVID-19 outbreak is under way and there are already vaccines under development. But there is no indication yet that they will be successful. The current R&D response may simply not be large enough to stop the pandemic quickly enough.
How do we stop COVID-19?
To stop this pandemic, it may be necessary to move activities out of already productive (and profitable) research activities. And this may have to happen on a scale that is proportionate to the scale of the cost of the outbreak. A radical restructuring of the incentives of the biomedical research industry may be necessary to shift this activity away from its profitable uses and into (uncertain) vaccine research.
Academic research suggests how this might be done. Probabilistic innovation theory suggests that problems such as COVID-19 need to be exposed to processes that radically increase their probability of success. This may require novel technologies and methods to greatly increase the chances of solving the problem such as biomedical crowdsourcing, machine learning and big data science.
These have already demonstrated their effectiveness in biomedical research, but not yet at the scale required to stop the pandemic. Another useful example of biomedical crowdsourcing is gamification, a process whereby complex biomedical problems are used as the basis for computer games, with the goal of solving them. The site FoldIt is successfully using protein folding games to solve these kinds of problems.
A useful way of thinking about this approach is in terms of a societal benefit ratio. This is the ratio of the research efforts invested in solving a problem to the consequences of the same problem. In other words, many problems with very high human and economic costs don’t receive enough problem solving resources – the scale of the investments in solving these problems should be appropriate to the scale of the problem, or it might not be solved.
Current R&D efforts aimed at tackling the pandemic may produce a societal benefit ratio that is too small. The COVID-19 pandemic potentially affects around 8 billion people. Estimates of necessary interventions suggest that, if not addressed, the damage to the global economy could be in the trillions of dollars. The problem with current approaches seems to be that they are largely rooted in the profit-driven structure of the biomedical industry. Even with academic collaborators, this restricts the size of the investments in solving the problem.
Existing efforts will surely come up with a solution given enough time. But it might be necessary to consider other scientific approaches that have already demonstrated their success in biomedical research, and try them at a large enough scale.
How crowdsourcing works
Advances in technology have made it possible to crowdsource solutions to biomedical problems. Biomedical crowdsourcing is a problem-solving methodology based on putting problems online as an open call for anyone to solve. Sites like InnoCentive provide platforms for the initiation and administration of scientific crowdsourcing, but a large-scale global project might be administered by the United Nations or the World Health Organisation.
The successes of crowdsourcing in biomedical research are well documented. Sites such as InnoCentive have shown that complex scientific problems can often be solved more cheaply and quickly than they would using in-house R&D departments.
It could be argued that the scale of the crowdsourcing efforts to date has been too small to force activity into uncertain avenues of research. If governments across the world were to pledge a portion of their ongoing economic costs of the pandemic, it might be possible to offer a large biomedical crowdsourcing award, for example in excess of a thousand billion dollars. The scale of this award would better match the scale of the consequences of the pandemic. Such countries would not have to pay a cent if a solution were not found. Those seeking to solve the problem (solvers) bear the cost and risk of these efforts. This makes it necessary to offer a very large award. These costs include opportunity costs, such as the costs of not doing other work in the meantime.
If crowdsourcing were to solve this problem, then what of others that we have failed to solve until now? The current pandemic might offer researchers a unique chance to test this methodology at a large scale. If necessity drives invention, then there is no more important time than this to try new ideas.
Personal versus public freedoms South Africa during COVID-19
- Harriet Etheredge
In restricting individuals' movements and interactions during any national disaster, the conflict between public interest and personal autonomy will get messy.
As the COVID-19 pandemic took hold in South Africa two weeks ago, the first glimpse emerged of the lengths to which people would go to avoid isolation. The country also saw what mechanisms law enforcement had at their disposal to impose such measures.
The case that received the greatest coverage involved a mother and daughter who had tested positive for COVID-19 fleeing a health facility with a third family member. The Department of Health applied for an urgent court order to track the family down and compel them into isolation. This was granted. The family was subsequently located and isolated.
Very soon afterwards the government sought to clarify the legal position around the event. It gazetted a new regulation for COVID-19 that makes it a criminal offence to refuse testing, treatment or isolation. If an individual does refuse isolation, they may be held involuntarily for 48 hours.
During this time an urgent warrant must be obtained to extend the isolation period. Any person who contravenes these regulations is subject to fines or imprisonment.
This case is polarising and peppered with prickly ethical issues. Many may be scandalised by the arrogant and irresponsible actions of the family. The opposing contention is that the family was hindered in exercising its autonomy.
In any national health disaster calling individuals to voluntarily restrict their movements and interactions, the tenuous no man’s land between public interest and personal autonomy is bound to become a messy quagmire. On one hand, there is the evasive action of those who feel their autonomy is being restricted. On the other hand are people seeking a larger public good. In this case it’s the quest to “flatten the curve” of the pandemic by reducing infection rates.
Public versus personal interests
Autonomy is a person’s right to self-determination. So, it’s my right to do what I want to, when I want to and in the manner I want to – provided the continued exercise of my autonomy does not infringe on the autonomy of another. Both ethically and legally, this is where autonomy meets its limit.
Through evading isolation, the family may have jeopardised the autonomy of many who are at risk of COVID-19 and are taking measures to avoid it, like social distancing. That’s surely enough to make people feel angry.
There is a great deal of historical precedent in ethics literature for curbing personal autonomy in the interests of the wider public. Some examples are so obvious we take them for granted because they are inherently “wrong”. They include murder, theft and kidnapping.
Other examples are more subtle and include the right to freedom of speech, which is limited at the point where it offends the privacy or dignity of someone else.
Modern health policy leans demonstrably towards public health interests over those of individuals. Hence, we have notifiable diseases like tuberculosis where disclosure is mandatory.
In the case of HIV the Health Professions Council’s guidelines allow healthcare workers to disclose the status of an HIV-infected individual to their sexual partner after sufficient counselling – even if the individual disagrees. Disclosure here is justified because it’s seen to be in the interests of the wider public.
In the case of COVID-19 it could argued that the demand on healthcare systems could be greater in developing countries than northern hemisphere countries. This suggests that the decision to impose lockdowns is all the more imperative.
The global south has weak health systems. It also has huge groups of individuals with diseases like HIV and TB. And millions of people live in very close proximity, in informal housing that facilitates the rapid spread of disease.
Because of this (and because in a novel pandemic like COVID-19 where there is very little data – and hence evidence – on which to base health recommendations) the decision to impose a lockdown makes sense. Under these circumstances, it is always advisable to proceed with utmost caution and in the interests of public health.
But a lockdown pits personal choice against collective good. Given the circumstances it appears reasonable to expect people to agree to limiting their freedoms.
Enforcing lockdown and adapting to it
Can authorities trust citizens to take measures like social distancing of their own accord?
The answer seems to be no and, in these cases, it has been necessary to cleave a legal framework compelling people to act in a morally responsible manner.
To ensure that principles like justice and equality across South African society don’t succumb to COVID-19, it will be necessary to clamp down on those who flaunt the law while the rest of the country abides by it.
But such enforcement must be elastic enough to respond to the South African context, and demonstrably address the practical and social challenges that many face.
SA needs to mitigate the worst of its inequalities in tackling COVID1-19
- Imraan Valodia and David Francis
South Africa won't flatten the COVID-19 pandemic curve unless all citizens have the means to stay at home.
As South Africa entered its 21-day lockdown, the political message was that South Africans were all in it together. However, it is clear that while society has been united politically to fight COVID-19, there are extreme and persistent economic and social inequalities. The lockdown confines everyone to their home for three weeks. But what does this mean in a country riven with inequalities?
The lockdown has illuminated how the spatial, economic and social inequalities which were characteristic features of the apartheid period have persisted in post-apartheid South Africa. Media coverage has shown inequalities in access to transport, shops, COVID-19 testing, and the very different ways the lockdown has been enforced and policed in different communities.
Here, we focus on the economic inequalities which have been highlighted by the lockdown. A time of crisis, such as this, shows the economy for what it really is. It strips it of all the trappings that often obscure the true economic relations. Events like this allow us to see how different parts of a society are structured to deal with distress, disruptions and economic shocks.
In South Africa, it’s a stark picture.
Deeply unequal
Economic data can help us construct a picture of the financial inequalities across South African households. If we divide households in the country into five groups (quintiles), from the poorest 20% to the richest 20%, we see how deep inequality is in the country. According to forthcoming research by our colleague Gabriel Espi at the Southern Centre for Inequality Studies, drawing from the National Income Dynamics Study from 2017, approximately 18 million South Africans live in the poorest 20% of households. Almost half of these poorest households are in rural areas. (While there are some doubts about the reliability of population counts generated by the National Income Dynamics Study, and whether the data underestimate poverty, the household-level insights it provides are very useful.)
On average, these poorest households have about five members and a total monthly household income of R2,600 (or about R567 per person in the household). Only 45% of households have an employed member. Much of this income would have been lost as the shutdown began. Indeed, a recent study by the Southern Africa Labour and Development Research Unit, which specialises in research on poverty and inequality, labour markets, human capital and social policy, found that the poorest 10% of households will most likely lose 45% of their income through the shutdown.
In contrast, 7 million people live in the richest 20% of households, with approximately two people per home (the average size is 1.93 people per household). The average monthly income for these households is almost R38,000 per month (or R21,000 per person). Almost 80% of these households have at least one employed member, and they work far more hours at a far higher wage than those in the poorest 20% of households.
Many of the people in the richest households are able to continue to earn an income by working from home, and many will actually save money due to reduced expenditure on things like eating out, holidays and entertaining.
For others, in lower-paid formal employment, the lockdown has exposed many to the risk that they could lose their jobs. For this group, the Unemployment Insurance Fund provides some temporary relief.
One particular group – informal workers – has no protection whatsoever, and the lockdown effectively removes their ability to earn any income at all.
Analysis of the Labour Force Survey data shows that there are 2.6 million South Africans working in the informal sector as own-account workers or their employees. Approximately a million more people are employed as domestic workers, many of whom do not have employment contracts or any unemployment benefits.
Many of these people would effectively have lost their jobs and their ability to earn an income at midnight on Thursday 26 March. When the lockdown ends, many of these workers, especially women, who often occupy the most precarious positions in the labour market, will find it very difficult to re-establish their work on the street corners, taxi ranks and train stations around the country. These workers, sometimes called “the precariat”, have work, but no protection whatsoever.
During events like a lockdown, or a protracted economic crisis, it is not income, but wealth, which sustains households. Here, the inequalities are unfortunately even more striking.
A forthcoming study by our colleagues Aroop Chatterjee, Léo Czajka and Amory Gethin of the Southern Centre for Inequality Studies and the World Inequality Lab finds that the poorest 50% of South Africans have an average net wealth of negative R16,000. That means their assets are less than their liabilities; they are deeply in debt. The richest 10% of South Africans, by comparison, have an average net wealth of R2.8 million per person (the top 1% have an average net wealth of R17.8 million per person).
While these individuals would have lost a portion of their wealth in the recent stock market crash, they are still substantially better off than most, and their household far better equiped to endure the lockdown.
Access to food
In terms of access to essential supplies, there is also a chasm between rich and poor. As we saw from the long queues in the shopping centres prior to the lockdown, those in the top quintile had sufficient income to go on a buying spree and stock up in anticipation of the lockdown. On the other hand, in the bottom quintile, millions of people had to queue in the supermarkets after the lockdown was in operation, jeopardising their health.
A recent study by the Institute for Land and Agrarian Studies finds that households with different incomes have very different access to food. The poor are at a significant disadvantage during the lockdown, with potentially catastrophic results for nutrition and hunger.
It is clear from these figures that while all households are locked down together, their abilities to manage the situation vary substantially. The resources to survive a three-week lockdown vary hugely between households. For the rich, this period may well mean an increase in savings. But for the poor, it means financial ruin. Most of the low wealth households will be plunged further into debt, as they are forced to liquidate their assets to survive the lockdown. The financial and economic consequences of the lockdown will be nothing short of catastrophic for many – if not most – South Africans.
What’s to be done?
The bold, decisive and evidence-based action by the government in response to the public health crisis the country faces should be applauded. The health response has, so far, been good. There has been rapid action to address some of the economic fallout of the crisis, including extraordinary tax relief, and bringing forward the payment of social grants.
But the current crisis is really worsening enormous existing inequalities, in addition to creating new ones.
Far more needs to be done to counter the economic destruction currently under way. South Africa cannot tackle the problem with marginal economic policy interventions. It needs immediate and drastic action informed by the best available economic evidence which is being offered by researchers across the country. South African society is at risk if it does not address these economic inequalities.
Indeed, the COVID-19 pandemic makes it clear how interrelated the society really is. The country can’t successfully flatten the curve of infection unless all have the ability to stay at home. For many the choice between staying at home and starving, or going out in search of work, is fast approaching.
For many others, spatial apartheid and extremely high levels of poverty make it virtually impossible to conform to the social distancing required to contain the spread of the coronavirus.
South Africa will not be able to tackle the COVID-19 crisis in a unified way if it does not mitigate the worst of its inequalities, and time is running out.
Covid-19 lockdown needs to protect inner-city communities
- Siyabonga Mahlangu and Matthew Wilhelm-Solomon
In South Africa, the collision of HIV, TB and Covid-19 could be devastating, and radical measures are needed to address the spread of Covid-19.
The lockdown rules require that residents only leave their homes to seek medical care and “buy food, medicine and other supplies or collect a social grant”.
The army and police have been deployed to enforce the lockdown.
In South Africa, the collisionof HIV, TB and Covid-19 could be devastating, and radical measures are needed to address the spread of Covid-19, particular with South Africa’s overstrained health system. However, if lockdown measures worsen the health conditions of the most vulnerable groups – including those living in inner-city occupations, both South African and foreign nationals – they could be counterproductive.
Police and private security have been moving through the streets of Hillbrow and Yeoville, Johannesburg, firingrubber bullets and beating pedestrians with sjamboks. A Jeppe resident we spoke to reported being fired at with no warnings by police on Monday night. Public order policing rules require that police give two warnings before using any force.
Police and private security violence is an all too familiar, rather than exceptional, sight for inner-city residents. While constitutional protections in the post-apartheid era provide radical and progressive protections and housing rights, inner-city populations have all too frequently been subject to raids, evictions, and, in the case of undocumented migrants, deportations.
According to 2011 statistics, more than 30,000 householdsand over 120,000 people were earning below the R3,200 per month necessary to accessmost decent rental housing in Johannesburg. There are likely to be tens of thousands living in unlawful occupations in high-rises, warehouses and houses, which have not been legally classified as “informal settlements”, but rather labelled “bad buildings” or “hijacked buildings”.
While there are cases of title-deed fraud and illegal rent collection, most of the residents of these buildings, both South Africans and foreign nationals, belong to low-income groups: informal workers and traders, recyclers, the unemployed and precariously employed, contract workers, cleaners, security staff, and beggars, among others.
The residents of these buildings have long been the targets of persecutory police action. The army and police have often been deployed against inner-city residents, in campaigns like the Zuma-led Operation Fiela in 2015. In 2017 the former Johannesburg mayor, Herman Mashaba, increased police raids on occupations while continuing to deprive their residents of access to basic services. The ICF, in collaboration with the Socio-Economic Rights Institute of South Africa (SERI)are contesting the legality of these raids, on the basis they were conducted without warrants and breached rights to privacy and dignity.
It is critical that police and army deployment for the Covid-19 lockdown does not result in the persecution of residents of unlawful occupations,along with others; this intervention needs to be gender sensitive and not allow for sexual harassment and xenophobic discrimination.
Furthermore, while Ramaphosa promised community health teams to low-income areas, which havebeen sent into townships, no residents in several inner-city occupations that we have spoken to have been visited by these teams.
President Cyril Ramaphosa and his advisers, aware of the potential impact on low-income groups, stated plans to take measures that include emergency water supplies “using storage tanks, water tankers, boreholes and communal standpipes” in “informal settlements and rural areas”. However, again this ignores that many inner-residents are living with inadequate access to water.
The Inner City Federation (ICF), founded in 2015, of which Siyabonga Mahlangu is general secretary, represents over 40 of these buildings. It began campaigning against evictions and for the provision of basic services, including water, to inner-city occupations before the Covid-19 outbreak. For instance, on 28 March, 2018 the ICF handed a memorandum to the mayor’s and president’s offices, demanding access to basic services, which was ignored by both offices.
Many Johannesburg residents feel that their rights, according to section 27 of South Africa’s Constitution, guaranteeing access to food, water and social security, have been infringed and violated by the City of Johannesburg.
In many inner-city occupations hundreds of people often have to share a single tap or water point, such as a fire hydrant. As water points and shared amenities are mostly communal, physical distancing is extremely difficult. In addition, many residents have to use buckets instead of toilets, or use public toilets. This, at night, is of course particularly dangerous for women and children. Several ICF members we’ve spoken to telephonically contend that they struggle to follow Covid-19 guidelines due to the difficulty in accessing water.
City officials need to ensure that water, soap and (where water is unavailable, and at key points like building entrances) hand sanitiser be provided to low-income groups who cannot afford these items, and that there is safe and free access to public toilets.
In addition, the national and municipal agencies need to work with NGOs on distribution of information, grounded in evidence, that is meaningful to residents living in stressed conditions (for instance,sanitising communal resources facilities, guidance on minimisingwater use in hand washing, the re-use of water, and water storage).
The current mayor of Johannesburg, Geoffrey Makhubo,has taken important steps in halting any disconnections of water and electricity, along withseveral other municipalities; however, it’s important that water is restored to those whose water has been cut. In addition, it’s important that water tanks are also provided, accessible to low-income inner-city residents without reliable water access.
In the inner city there are no street traders working. Yet many inner-city residents rely on informal trade for income and for food There are also severe concerns about food shortages among those who have lost incomes during the lockdown. Beggars are likely to be among the most vulnerable during lockdown, many of whom are blind and disabled, and will not have savings to survive on. Disability amplifies many of the difficulties of water access and protecting against Covid-19. In addition, children could be particularlysusceptible to malnutrition.
There needs to be food support for those who cannot go 21 days with no income. Finally, there needs to be a moratorium on forced evictions,as a coalition of social justice groups have called for, and a stop to all deportations which could worsen the spread of Covid-19 through scattering, and worsening the condition, of vulnerable groups.
Finally, there needs to be collaboration to provide food support for those who need it during the lockdown.
Civil society groups like Tshisimani are callingfor nationwide solidarityalong with income, water and food security. The challenges facing inner-city communities are not unique, but they should also not be ignored as part of a wider response, and the municipal and national government should actively support inner-city residents and civil society in the response to the pandemic. An effective public health response to Covid-19 requires that all residents in South Africa, no matter their economic condition or nationality, are included in the response.
It is critical that, along with other precarious populations, inner-city populations regardless of nationality are cared for and not persecuted during the lockdown.
President Ramaphosa’s team, together with the present executive mayor of Johannesburg, Geoffrey Makhubo, will be held to account and must attend to these concerns as a matter of urgency. The lockdown cannot be used to continue to suppress the rights and lives of inner-city residents, along with those living precariously, throughout South Africa.
Siyabonga Mahlangu is General Secretary of the Inner-City Federation (@InnerCityFed,innercityfederation@gmail.com), a community-based organisation founded in 2015 representing the residents of over 40 inner-city buildings. Matthew Wilhelm-Solomon (@wilhelmsolomon) is a lecturer in anthropology at the University of the Witwatersrand and an associate researcher on theMigration and Health Project Southern Africa. This article was first published in Maverick Citizen/Daily Maverick.
Centre for Deaf studies breaks the silence on COVID-19
- Wits University
The Centre for Deaf Studies (CFDS) at Wits is contributing to society by keeping the Deaf community informed about the coronavirus pandemic.
Thee COVID-19 pandemic has spread at an alarming rate over the past few weeks in the country. To date, over 1400 cases of COVID-19 cases have been confirmed in South Africa.
Government, media houses and various institutions have been disseminating important information and updates with the public around COVID-19 through various platforms.
To ensure that the Deaf community gained access to crucial information on the global pandemic, the CFDS at Wits has been playing an active role through a number of initiatives that filtered information to the Deaf and hard of hearing communities in South Africa.
When the President addressed the nation on 15 March, the CFDS ensured there was a full live stream interpreting by a Deaf person through the use of relay interpreting – a practise of translating messages from one language to another through a third language for a targeted audience.
“Deaf to Deaf communication is the best way of getting such crucial information across,” says Professor Claudine Storbeck, Director for CFDS.
In an effort to raise awareness around COVID-19, the Centre also produced “Corona Info for kids”, an educational video for children teaching them about the deadly virus. The aim of the video was to make information accessible for deaf children in a deaf appropriate way that would make an impact, which also included a fun handwashing-alphabet clip.
In recent weeks, since the coronavirus outbreak in South Africa, CFDS has been offering and sharing information through these videos in South African Sign Language (SASL) to ensure the Deaf Community could access information in their first language.
“In any form of crisis or trauma, people communicate best in their 'mother tongue' and therefore we are making sure that information is available in SASL. ‘If you talk to a man in a language he understands, that goes to his head. If you talk to him in his own language, that goes to his heart.’ This quote from Madiba is so appropriate when it comes to including the Deaf community in our planning around this pandemic,” says Storbeck.
While the focus is on the Deaf community, the Centre has added subtitles to the videos to create inclusivity and enable Deaf and hard of hearing people to watch and share these videos with their hearing family and friends. Here is a list of the videos produced by CFDS for the Deaf community:
With a week into the 21-day lockdown to reduce the spread of coronavirus, the Centre has cancelled their contact home-based support for families of deaf infants and young children (HI HOPES) and will be offering support via WhatsApp and videos. A five-week online SASL course will be released next week for hearing people wishing to learn about Deaf culture and how to communicate with the South African Deaf community without leaving their homes. A dedicated WhatsApp hotline (074 029 2764) has also been set up for Deaf children and adults to send their questions on the lockdown via either text or video. The hotline can be accessed via WhatsApp. Enquiries: claudine.storbeck@gmail.com
COVID-19 UPDATE (20) – WELLNESS UPDATE
- Wits University
The University’s wellness support services are here to help staff, students and the Wits community in dealing with the disruption of our normal lives.
Dear Colleagues and Students,
South Africa is about to complete its first week of the national lockdown. We wish to remind Witsies to continue protecting themselves, their families and the broader community by observing the call to #StayHomeSA in a bid to slow down the number of infections in the country. Sadly, many individuals and families are finding it hard to deal with the disruption to normal life during this period. It is normal and expected during difficult times.
The University’s wellness support services such as the staff counselling line, the Counselling and Careers Development Unit (CCDU) and the Gender Equity Office are available to assist during the lockdown.
The following services are thus available to Witsies:
Help for students
The CCDU Lockdown Wellness Chronicles offers daily coping strategies that can be used by all. The site has daily prompts to help structure and regain control of life and also to prepare for normalcy. Visit the CCDU website for more information on various mental health and wellness topics.
Students who would like to contact a counsellor for either personal, career or life coaching purposes can email the CCDU and leave their contact details and one of the team’s professionals will respond. Email info.ccdu@wits.ac.za.
The Wits Student Crisis Line is available to all Wits students for counselling 24/7/365 on 0800 111 331.
The Campus Health and Wellness Centre is available to assist with primary healthcare and mental health enquires:
- Primary healthcare enquiries – Call 0743077259 or 0824832251
- Mental health enquiries – Call 0766093924
Help for staff and immediate family members
The Impil’enhle programme launched by the University in September 2019 offers free services for staff and their immediate families to receive counselling for stress, anxiety, relationship and marriage problems, parenting, abuse, trauma as well as legal and financial advice. This independent service offered through Kaelo Lifestyle is provided in all South African languages 24/7 days a week.
Call 0861 635 766 OR dial *134*928 OR Send a ‘Please call Me’ to 072 620 5699 OR email asknelson@kaelo.co.za
COVID-19 Medical Line
Should you suspect that you have COVID-19, please contact the COVID-19 Medical Line during work hours for medical-related advice on prevention, diagnosis and treatment options - call 0861 493 587 and select option 2 for members and then select option 6. Alternatively, contact the National Institute for Communicable Diseases (NICD) on 0800 029 999. Still unsure about how to monitor yourself for symptoms of COVID-19?
Gender Equity Office
During this time of lockdown and looking after ourselves and our communities, we realise that there are some who will be in spaces where they are not safe. The Gender Equity Office is available via email info.geo@wits.ac.za or call (011) 717 9790. Alternatively, call the national gender based violence command centre on 0800 428 428 or send a "Please Call Me" to *120*7867#. It is important to remember that should you require a restraining order, courts continue to operate for this purpose. The GEO is available to guide you through the process and prepare you for what to expect when you apply for the order.
ADDITIONAL RESOURCES
Busting Myths
There are many myths circulating around the transmission and prevention of the coronavirus. Wits Lecturer Neelaveni Padayachee from the Department of Pharmacology explains the myth around drinking alcohol to prevent the virus.
Helping children cope with changes
The impact that Covid-19 might have on children will vary and their responses could be influenced by factors such as gender, social support, inherent resilience and the level of exposure to the virus. Dr Ajwang' Warria, a Senior Lecturer in the Department of Social Work offers guidelines on how to help children during this period. Read the article.
Coronavirus posters in multiple languages
There is a series of educational posters (some translated by Wits students) on coronavirus is available in multiple languages. Download, print or share the following resources in Sepedi, Sesotho, Setswana, siSwati, Tshivenda, Xitsonga, Afrikaans, IsiXhosa, IsiZulu and English.
Remember to practice good hygiene and to maintain physical distancing.
Stay safe
Wits COVID-19 Management Committee
2 April 2020
COVID19 Testing Station opens at Wits
- Wits University
A new COVID-19 Testing Station at Wits, managed by Gift of the Givers, is open to patients who fit NICD criteria and are referred by a doctor.
Wits University and the Gift of the Givers Foundation have opened a COVID-19 Testing Station on the Braamfontein Campus (Enoch Sontonga Road).
Tests will be conducted in an NICD approved, SANAS accredited laboratory with feedback to the NICD electronically. The turnaround time for results is between 24 and 48 hours.
Who can be tested?
Patients must fit the NICD case definition criteria and must have a doctor's referral before testing. This reduces contamination risk and contact time in the best interests of all concerned.
HPCSA rules require that the patient has to consult his/her OWN doctor if it's a telephonic consultation or any doctor if it's a face-to-face consultation.
Cost
The COVID19PCR testing costs R750, and payment is due via EFT before testing.
Bookings and operating times
Please note: Testing is strictly BY APPOINTMENT ONLY. NO WALK-INS permitted.
Bookings: Call the toll-free number on 0800 786 911
Operating times:Monday - Friday: 07:45 - 17:00
No fees will be earned by Wits University or Gift of the Givers. The fee simply facilitates a more affordable price for the public.
Wits School of Molecular and Cell Biology lends a hand with glove donation
- Wits University
The Wits School of Molecular and Cell Biology has donated medical gloves for frontline healthcare workers at Chris Hani Baragwanath Hospital in Soweto.
Healthcare workers treating COVID-19 patients urgently require medical gloves for their own protection and to avoid contamination. However, gloves and other personal protective equipment (PPE) is in short supply.
Protective equipment saves lives
The Director-General of the World Health Organisation (WHO) highlighted in his media briefing on 27 March 2020 that the chronic global shortage of PPE is one of the most urgent threats to our collective ability to save lives.
Prof. Yasien Sayed in the Protein Structure Function Research Unit (PSFRU) in the School of Molecular and Cell Biology coordinated the donation effort. Sayed was alerted to the critical need after Wits Medical School graduate, Dr Naeem Vallee, a first-year intern doctor at the hospital, relayed the shortage via a colleague whose wife is a Wits PhD candidate whom Sayed supervises.
Through the collective efforts of Sayed, Dr Pieter De Maayer, Dr Angela Botes and Dr Vanessa Meyer, a total of 56 boxes each containing 50 pairs of gloves were donated.
“At the moment, the Department of Internal Medicine at Chris Hani Baragwanath are full in the swing of preparing to deal with the impending COVID onslaught. Three wards have been specifically isolated to host and rehabilitate and treat the patients that will come back as COVID positive. It’s an extremely tense time. The lack of personal protective equipment is huge challenge we as healthcare practitioners face in dealing with this pandemic,” said Vallee, who took delivery of the donated gloves. Vallee graduated MBBCh from Wits in 2019.
“I’m extremely grateful to Prof. Sayed and his colleagues for recognising that we on the frontline need help, and for his generosity. This is a time where we all need to work together to prevent the spread and flatten the exponential growth curve of the COVID pandemic.”
Sayed, who personally delivered the boxes to the hospital, says: “The donation of gloves represents a small token of our appreciation of our healthcare workers’ selfless and admirable efforts, and we hope that these gloves will afford them some measure of protection against the virus.”
Fingering coronavirus ‘spike’ protein
The SARS-CoV-2 virus, the novel type of a coronavirus that causes coronavirus disease (COVID-19), has several glycoproteins on its surface. One of these proteins is referred to as the ‘spike’ protein, which is responsible for binding to receptors on the host cell prior to infecting the cell and hijacking the host’s cellular machinery for replication and reproduction of new viral particles.
The PSFRU investigates the structures, dynamics and energetics of a variety of proteins using a multidisciplinary approach that relies on the principles and methodologies of biochemistry, biophysics, molecular, and structural biology and bioinformatics.
Keeping Witsies safe
Prior to announcement of the lockdown on 26 March 2020, the School had manufactured and dispensed 70% EtOH (ethanol) surface disinfectant freely to Wits staff to minimise contamination by the coronavirus. The disinfectant comprises 95% industrial ethanol (also called alcohol) diluted with distilled water to a ratio of 70%. Alcohol kills germs effectively, as long as alcohol comprises 60% to 95% of the solution. This is a ratio shown to be effective against germs. Alcohol attacks and destroys the ‘envelope protein’ that surrounds some viruses, including coronaviruses. This protein is vital for a virus’s survival and multiplication.
“We use 70% ethanol to sterilize surface areas when we are required to work under sterile conditions in our laboratories, for example, when we do tissue cell culture work. The ethanol is effective in killing a number of germs, including viruses. Cleaning all objects and surfaces that we come into daily contact with is a sensible practice to protect against coronavirus,” says Prof. Marianne Cronjé, Head of the School of Molecular and Cell Biology.
Hay’khona Corona! Spreading the word, not the virus
- Wits University
A poster series to action South Africans on how to care of themselves and others.
Wits University students who participated in the South African leg of FameLab, an international science competition, helped to translate a series of posters with a key messages on how every South African’s actions can save lives.
The multilingual posters were produced by research communication specialists Jive Media Africa, and are published with a Creative Commons license so you are free to copy, print and share them (provided no modifications are made).
“Altruism is a strong motivator” says Jive Media Africa Director Robert Inglis, “People are looking for ways they can help, and sharing relevant, relatable messages is one of those ways.”
Hay’khona is an isiZulu expression signalling strong negative sentiment. Inglis says the posters say:
No, not here! to COVID-19
The posters have been translated into a number of languages from South Africa and other African regions, including IsiZulu, IsiXhosa, Setswana, Sesotho, Sepedi, SiSwati, Tshivenda, Xitsonga, Afrikaans, Yoruba, Luo and French.
- Dr Ajwang' Warria, Wits Department of Social Work
Strategies for parents to engage with their children at home during Covid-19 lockdown.
The national lockdown as a result of the coronavirus started in South Africa at 23:59 on Thursday, 26 March. Exposure to uncertainty has heightened anxiety levels and stretched the care and protection mechanisms normally provided at home.
Children, in particular, are vulnerable to the extraordinary circumstances of lockdown, social distancing, and a global pandemic.
The United Nations Convention on the Rights of the Child (UNCRC) indicates special obligations for the caregivers of children in times similar to these. The best interest principle stresses that children should be assisted and protected at all times and their developmental needs met.
Covid-19 presents parents and caregivers an opportunity to deepen their participation in the lives of their children, mitigate harmful consequences and thereby safeguard their children's futures.
The impact that the coronavirus might have on children will vary and their responses could be influenced by factors such as gender, social support, age, inherent resilience, and level of exposure to the virus. What remains evident is that children tend to rely on parents for their emotional needs. Thus, parents (and any primary caregivers) can play a crucial central role as children’s sources of safety, security, and information.
The family is one of the most important systems of a child’s life. The collective nature of care that happens within the home setting is crucial, as many people, including children, look to their family for support when they face challenges. Social and cultural factors influence the care that people give and receive within these networks of care.
Here are some strategies for parents to engage with their children at home during Covid-19 lockdown. These strategies are drawn from a published study, which investigated strategies used by parents in Kenya to support children during terrorism acts:
Engage the child in open conversations using a language that the child can understand. Avoiding discussions may make the child more fearful and anxious. During the lockdown, remember that parents might be the only available support to the child. However, this support could also (be nurtured to) include older siblings, grandparents, teachers, etc. who can be accessed online.
As parents/caregivers, manage your own anxieties, which will help your children cope. Your well-being is imperative to your children’s wellbeing and recovery, as children sometimes regulate their own emotions based on the emotional response of their parents/caregivers.
Answer your children’s questions. The kinds of questions asked by children range from issues of safety, access to medical care, recovery, death, schooling, friends, teachers, pets, etc. Parents should respond both to their children’s anxieties (emotionally, by providing reassurance) and to the question itself. Children can ask difficult questions, but parents should not shy away from answering. Do not give a child false information – rather provide reassurance and let your child know that you will look up accurate information and share it with them. Children’s questions are essential. Questioning permits children to exercise their right to participation on matters concerning them.
Listen! Children need to make sense of things happening around them. The ability of parents/caregivers to actively and intently listen to their child is crucial. Parents/caregivers who are constantly glued to their cell phones for coronavirus updates might miss the opportunity to provide the secure base needed for children to take risks and ask frightening questions.
Provide accurate, factual information. Generally, children might not have clear, factual information. It is vital that parents/caregivers help children to understand what is happening, i.e., tell the real story reassuringly and holistically. This also presents an opportunity to rectify any incorrect information or misconceptions your children might have heard about or read.
Covid-19- related events have altered the way we do and see things. Thus, it is important to maintain a daily routine. Performing everyday activities as far is possible is vital, as this routine provides the structure that children rely on. By maintaining familiar schedules, based on age, gender and culture, children can establish normalcy, which will reduce their anxieties.
Monitor exposure to media. Continuous repetitions of Covid-19 news in any form risks re-traumatising or causing secondary trauma to children. Protect your children from what you think and know would exacerbate their anxieties and that which is unhelpful towards their healing.
Help build resilience in your children by facilitating play, nurturing care and celebrating survival with them on an on-going basis. Resilience can go a long way post-Covid-19.
Consider and plan for the worst-case-scenario. Parents/caregivers need to think about and work out alternative care arrangements for their children, should the parents/caregivers fall ill or die. Discuss these arrangements with children (reassuringly!) in an age-appropriate manner and with those identified and expected to provide care.
Look after yourself. Care for parents/caregivers is also vital. Engage in a relaxing activity and check-in with other parents. Share problem-solving strategies and support each other towards for effective childcare. These safe spaces enable parents/caregivers to talk about their own Covid-19-related (parenting) challenges and pain. Parents/caregivers need to monitor their own mental health and, if they have difficulties caring for their children, seek professional help.
COVID-19 UPDATE (19) – TEACHING AND LEARNING (STUDENTS)
- Wits University
Message from the Deputy Vice-Chancellor: Academic regarding the resumption of the academic programme.
Dear Students
I hope that you are all well and that you are taking the necessary precautions to keep safe!
I know that many students are anxious about resuming the academic programme and doing so online.
The Senior Executive Team (SET) met recently and agreed to the following schedule:
1-14 April 2020
All academics will prepare to take lectures online.
15-19 April 2020
Online orientation begins this week for staff and students. All course outlines, lecture notes, reading lists and additional audio-visual material will be uploaded and tested during this period.
20 April 2020
The University opens for the second term and delivery of the academic programme begins online.
The almanac is currently being updated (we are consulting with faculties) and will be finalised early next week.
Learning Management Systems
All our Learning Management Systems (LMS) including Wits-e (Sakai) and Moodle will be hosted in the Amazon cloud to ensure that our systems have sufficient infrastructural support and that they are able to cope with large number of users accessing the systems at the same time.
Access to Smart Mobile Devices
We are aware that approximately 10% - 15 % of students may not have access to smart mobile devices (according to the results of the biographical questionnaires conducted over the last four years by Wits’ Business Intelligence Unit), and Faculties and Deans have been asked to develop specific plans in this regard.
Broadcast Options
We are exploring working with the SABC (Radio and Television), DStv and eTV to determine if it is feasible to broadcast key lectures on-air, particularly for those who do not have access to devices or data.
Access to Data and ICT Support
Wits has worked with Telkom, Vodacom and MTN to ensure that students can access selected learning sites without using data. Cell C is due to come on board shortly. All services will be activated within the next ten days. For a complete list of the zero-rated sites, visit: https://www.wits.ac.za/mywits/zero-rated-data-to-students-and-applicants/. Please note that students must have at least R1 worth of data loaded on a SIM card in order to access these sites. If you have any queries or concerns, please contact the ICT Service Delivery team via ithelp@wits.ac.za or call (011) 717-1717 or log a call via https://witshelp-ism.saasiteu.com/.
Faculty Support
You will receive a more detailed letter from the Dean of your respective Faculty later this week, followed by additional information from your School/Department and/or course coordinators. Please feel free to share your views on potential online/digital learning solutions with your respective faculties.
Additional Support
There is no doubt that we will offer additional support for students when we resume contact teaching. This could include additional lectures, boot camps, comprehensive laboratory sessions and additional tutorial support as appropriate.
Conclusion
We live through extraordinary times and have to develop extraordinary ways of teaching and learning. Our solutions may not be perfect but I would like to assure you that our academics and professional staff are working hard every day to ensure that we deliver a quality teaching and learning experience under the current circumstances. I know that you too will try your best to succeed. I have no doubt that we can overcome the many barriers that we will face and that together we can succeed.
Keep safe!
Professor Ruksana Osman
Deputy Vice-Chancellor: Academic
1 April 2020
COVID-19 UPDATE (19) – TEACHING AND LEARNING (STAFF)
- Wits University
Message from the Deputy Vice-Chancellor: Academic on the resumption of the academic programme.
Dear Colleagues
I hope that you are all well and that you are taking the necessary precautions to keep safe!
I write to you in my capacity as the Deputy Vice-Chancellor: Academic to share the thinking of the Senior Executive Team (SET) on the resumption of the academic programme and also to solicit your ideas and advice on best practices in your area as we move into an online teaching mode. Please read carefully through the attached Emergency Plan for Teaching.
The SET met yesterday and agreed to the following schedule:
1-14 April 2020
All faculties will prepare to take the academic programme online.
I know that many faculties are already off the starting blocks.
15-19 April 2020
This period will serve as the online orientation period for staff and students. All course outlines, lecture notes, reading lists and additional audio-visual material should be uploaded and tested during this period.
20 April 2020
The University opens for the second term and delivery of the academic programme begins online.
Please note that the almanac is currently being updated (we are consulting with faculties) and will be finalised early next week.
I know that many academics are enthusiastic about taking the academic programme online while others are anxious about doing so. This is new for many people and I would like to assure you that we have established both central- and faculty-based teams to assist you through the process. I would like to acknowledge the great coordination that is taking place between colleagues in CLTD, ICT and the Library to ensure that staff and students are fully supported and assisted as we transition to online teaching. The Emergency Plan for Teaching (attached) provides a step-by-step guide on how to begin this journey.
We have also ensured that all our Learning Management Systems (LMS) including Wits-e (Sakai) and Moodle will be hosted in the Amazon cloud to ensure that our systems have sufficient infrastructural support and are able to cope with the large numbers of users accessing the systems.
We are mindful that approximately 10% - 15% of our students may not have access to smart mobile devices (according to the results of biographical questionnaires conducted over the last four years by our Business Intelligence Unit), and Deans have been asked to develop plans to take this reality into account.
There is no doubt that we will have to consider additional support for students when we are able to resume contact teaching. This could take a variety of formats including additional lectures, boot camps, comprehensive laboratory sessions and tutorial support as required.
Conclusion
These solutions have been necessitated by the pandemic and have had to be devised quickly. We know that they are not perfect, and we are acutely aware that there is unevenness across disciplines, schools and faculties in the adoption of online teaching. In many cases, this is dictated by the particular demands of the programmes offered. However, we have to do all that we can to provide our students with a quality teaching experience so that we do not lose the academic year.
I am confident that we have some of the best academics in the sector, and coupled with our determination, resilience and ability to adapt to change, we will without a doubt succeed in these endeavours.
I envisage that there may well be some barriers along the way, but I also believe that we are well positioned to find solutions to the challenges that we may face.
Please feel free to write to me at Ruksana.Osman@wits.ac.za to share any suggestions or best practices that could be useful during this time.
Keep Safe!
Professor Ruksana Osman
Deputy Vice-Chancellor: Academic
1 April 2020
'You can do more,' economists tell SA government
- Wits University
50+ economists and others from Wits are part of a group of more than 78 who wrote an open letter urging President Cyril Ramaphosa for more significant action.
OPEN LETTER TO PRESIDENT CYRIL RAMAPHOSA AND THE CABINET FROM SOUTH AFRICAN ECONOMISTS, BUSINESS ANALYSTS AND ECONOMIC JUSTICE ADVOCATES:
Dear President Cyril Ramaphosa,
We commend you and your government for the bold and decisive public health measures that you have taken in response to the crisis precipitated by the COVID-19 pandemic. We welcome measures to stem the spread of the virus.
We are writing to you to suggest other measures that are urgently required to support and stabilise the economy and assist those hardest hit by the crisis. As you have noted, these public-health interventions will have significant adverse economic effects, compounding the persistence of inequalities in living conditions, wealth, income, and access to health and other services.
It is widely predicted that the virus will trigger a global recession, due to collapsing demand and the supply shocks this crisis will entail. It is estimated that South Africa’s GDP could contract by between 1.8 and 7%, with devastating impacts on jobs and livelihoods. This looming crisis requires large-scale economic interventions. For example, the United Kingdom, France and the United States have injected resources totalling 18.9%, 13.6% and 10.7% of GDP into their economies respectively. To date, the measures announced by the South African government, although welcome, do not match the scale of the challenge.
In the face of this looming crisis we believe more significant action is required. These interventions must protect the most vulnerable.
This response is different from previous attempts to resuscitate ailing economies. We must both acknowledge that physical distancing and a lockdown will slow economic activity, and that extraordinary measures are needed to cushion the resultant hardship and avoid long-term social and economic harm.
There is a significant risk that millions in poverty will fall into destitution; millions more, currently in work, will be driven into poverty and become unable to meet their basic needs; and thousands of businesses will be forced to close due to falling demand as a result of the lockdown, falling incomes and a contraction of economic activity. The self-employed, atypically employed, informal workers, and small businesses, are particularly vulnerable, but none will be exempt from its effects. Traditional social support networks will be disrupted. The long-term impact on business capacity, and physical, financial, and human capital, could be devastating to our already ailing economy. In any already deeply unequal society, we know that the hardship will fall hardest on black people, and especially black women and children.
Economic interventions must therefore aim to:
support households and communities,
protect workers,
sustain businesses,
strengthen public health interventions;
and strengthen the economy.
While we appreciate efforts already undertaken in each of these areas, we are concerned that they are not comprehensive enough, and are not being implemented sufficiently rapidly or on a large enough scale to prevent real hardship for millions of South Africans. While we recognise that the stringent social isolation measures are unavoidable, we need to commit as a society to ensuring they do not cause unnecessary hardship to our people, and especially to the working poor and other vulnerable groups.
The following measures indicate the kinds of opportunities that are available:
Support households and communities:
Income transfers to lower-income and affected households, in the form of a special COVID-19 grant, a top-up to existing grants, and/or a universal basic income grant. Creativity is needed to speed up delivery, including income transfers via digital payment mechanisms. We appreciate the practical difficulties involved.
Targeted, temporary and compulsory payment holidays from municipal taxes, rent and mortgages, and other debts owed, and a ban on evictions from houses, including on farms.
Undertake measures to relieve women of the burden of care, in and outside the home, for example, by the provision of childcare for essential workers and additional income support.
Ensure food security and food sovereignty through a coordinated and safe roll-out of food packages in food-stressed neighbourhoods, working with community groups to build collective action and solidarity. Children require special attention.
Protect workers:
Guarantee wage payments so that monthly wages of all workers are secured for the full duration of the lockdown. The expansion in UIF payments is both welcome and critical. , but this should be a fallback, not a default.
Rigorous implementation of leave requirements so that workers are not forced to use annual leave during the furlough period, and ensuring temporary workers as sufficiently accommodated.
Extend unemployment benefits to casual and informal-economy workers, including the provision of temporary unemployment payouts for lost income during periods of lockdown.
Ensure additional health and safety provisions are in place for essential workers and for when workers return to work.
Sustain businesses:
Significantly expand access to low-rate emergency loans, including through low-cost liquidity provision by the South African Reserve Bank. The current amount of funds available, and the voluntary nature of the “solidarity fund”, fall well short of the expected need. Moreover, there is some evidence that the solidarity fund has diverted donors from other charities that play a vital role in supporting the most vulnerable.
Targeted, temporary and compulsory payment holidays from municipal taxes, rent and mortgages, and other debts owed.
Other forms of targeted and temporary tax relief if low-cost loans and payment holidays are insufficient.
Increase the additional resources that are being directed to the health system, including for testing, treatment, medicines, community health care, and COVID-19 scientific research.
Strengthen public health interventions:
Strengthen the requirement for resources to be pooled between private and public healthcare providers, particularly for free testing and treatment of COVID affected patients.
Rapidly scale up government’s attempts at the local production of critically needed health products, medicine and equipment.
Scale up efforts to ensure greater access to water and sanitation, through the provision of water access points, safe ablution facilities, and removing restrictions on homes with water metres. The provision of soap and/or sanitiser is important.
Ensure free mobile data and public internet access, to keep the public informed and curb the spread of fake news.
Strengthen the economy:
Monetary policy measures to guard against capital flight and manage the exchange rate, ensure access to affordable credit, and ensure sustainable government bond rates. A “helicopter drop” of funds to households - for example, R1000 for each individual for a period of four months - could complement the grants discussed above.
Reviewing the current Medium-Term Expenditure Framework which requires considerable budget cuts, including in wages and healthcare.
We appreciate the Temporary Employment Relief Scheme, which aims to prevent retrenchments while maintaining standards. In the past, however, ensuring rapid and effective scaling up of the scheme has proven difficult. It is crucial that implementation be prioritised in the current crisis.
These measures will require additional government financing. We appreciate the effort to mobilise funds outside the fiscus - such as the Industrial Development Corporation (IDC), Public Investment Corporation (PIC), Unemployment Insurance Fund (UIF). However, the scale of interventions required will necessitate additional fiscal and monetary expansion by the Treasury and SARB respectively, as has been the case worldwide. A concrete plan for responsibly managing this must be tabled, a number of signatories are working on proposals in this regard. In addition, we support your call for global transfers and action on the international level.
Commitment, implementation and responsiveness remain a major challenge. While swift action has been taken on health responses, economic interventions have been subject to delay, confusion and incoherence. We need to accept that as with health policy, some risks will need to be taken in this unprecedented situation.
While the Presidency must direct interventions, as far as possible the economic interventions should seek to empower communities, promote their mobilisation, and build social solidarity, as has been noted by a wide number of civil society organisations.
The Presidency must reassure the most vulnerable people and businesses that they will be protected.
This moment calls for all South Africans to contribute. We are willing to support in advancing these shared objectives. We would welcome the opportunity to put these proposals before yourself and the appropriate forums and provide additional technical support as needed.
Yours sincerely,
[List of Wits University authors(*):]
Professor Vishnu Padayachee - Distinguished Professor and Derek Schrier and Cecily Cameron Chair in Development Economics, School of Economics and Finance, University of the Witwatersrand
Dr Gilad Isaacs - Co-Director, Institute for Economic Justice and School of Economics and Finance, University of the Witwatersrand
Lumkile Mondi - Senior Lecturer, School of Economics and Finance, University of the Witwatersrand
Professor Imraan Valodia - Dean of Faculty of Commerce, Law and Management, University of the Witwatersrand
Professor David Everatt - Head of School, Wits School of Governance, University of the Witwatersrand
Professor Uma Kollamparambil - Head of School, School of Economics and Finance, University of the Witwatersrand
Professor Pundy Pillay - Professor of Economics, School of Governance, University of the Witwatersrand
Dr Laura Rossouw - Senior Lecturer, School of Economics and Finance, University of the Witwatersrand
Professor Mills Soko - Professor of International Business and Strategy, Wits Business School, University of the Witwatersrand
Professor Ben Fine - Visiting Professor of Economics, University of the Witwatersrand, and Emeritus SOAS
Dr Mthokozisi Mlilo - Senior Lecturer, School of Economics and Finance, University of Witwatersrand
Dr John Khumalo - Senior Lecturer, Wits School of Governance, University of the Witwatersrand
Halfdan Lynge-Mangueira - Senior Lecturer, Wits School of Governance, University of the Witwatersrand
Dr Nicolas Pons-Vignon - Senior Lecturer, School of Economics and Finance, University of the Witwatersrand
Cheryl-Lyn Selman - School of Economics and Finance, University of the Witwatersrand
Sibulele Nkunzi - Lecturer, School of Economics and Finance, University of the Witwatersrand
David Francis - Deputy Director, Southern Centre for Inequality Studies, University of the Witwatersrand
Thabo Dikobe - Lecturer, Wits Business School
Ayanda Magida - Researcher, Wits Business School
Professor Rod Crompton - Adjunct Professor, Wits Business School, University of the Witwatersrand
Rubina Jogee - Lecturer, School of Economics and Finance, University of the Witwatersrand
Mark Everett - Executive Manager CLEAR-AA, University of the Witwatersrand
Aroop Chatterjee - Southern Centre for Inequality Studies, University of Witwatersrand
Avril Joffe - Head of Department, Cultural Police and Management, University of the Witwatersrand
Tlhalefang Moeletsi - Researcher, School of Economics and Business Science, University of the Witwatersrand
Professor Stephanie Allais - Associate Professor and Director of the Centre for Researching Education and Labour, School of Education, University of the Witwatersrand
Professor Tshepo Madlingozi - Director of the Centre for Applied Legal Studies (CALS), University of the Witwatersrand
Professor Jackie Dugard - Associate Professor, School of Law, University of the Witwatersrand
Professor Firoz Cachalia - Adjunct Professor, School of Law, University of the Witwatersrand
Professor Tracy-Lynn Humby - Professor, School of Law, University of the Witwatersrand
Sonia Newton - Senior Programme Manager, Wits Business School, University of the Witwatersrand
Kemantha Govender - Communications Manager, School of Governance, University of the Witwatersrand
Professor Jonathan Klaaren - Professor, Wits Institute for Social and Economic Research (WiSER), University of the Witwatersrand
Professor Vishwas Satgar - Associate Professor, Department of International Relations, University of the Witwatersrand
Sibusisiwe Ndlovu - Exams Marking Officer, Wits School of Business, University of the Witwatersrand
Professor Ian Goldman - Professor, Centre for Learning on Evaluation and Results, University of the Witwatersrand
Professor Emeritus Edward Webster - Professor Emeritus, Department of Sociology, University of Witwatersrand
Zubeida Bagus - Business Manager, Faculty of Commerce Law and Management, University of the Witwatersrand
Sky Konrad, Finance Officer - CLEAR-AA, FCLM, University of the Witwatersrand
Professor Anthoni van Nieuwkerk - Peace and Security Studies, Wits School of Governance, University of the Witwatersrand
Professor Jill Bradbury, Associate Professor, Department of Psychology, University of the Witwatersrand
Professor Michelle Williams, Professor, Department of Sociology, University of the Witwatersrand
Professor Salim Akoojee, Associate Professor and Senior Researcher, REAL at University of Witwatersrand and School of Education at University of Nottingham
(*) The list continues to grow as the letter reaches more people.
It would help if everybody comprehend that the world will not be the same after the dust settles on the pandemic.
Already, tonnes of writings have surfaced on the geopolitical implications of the coronavirus. Most analysts rightly concur that the world changed in those hard to pinpoint moments when the outbreak went globally viral.
It is now virtually cliché to refer to the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) that causes the Coronavirus Disease 2019 (Covid-19) or simply coronavirus as a global phenomenon. The World Health Organization (WHO) designated it a pandemic on March 11 – meaning a contagious disease that spreads around the world – after the fact. In other words, the novel coronavirus was global before it was declared pandemic.
What are the implications for Africa? It would help if the whole kit and caboodle of African governments, academics, businesses and civil society comprehended the fact that the world will not be same after the dust settles on the pandemic.
The words of Italian communist leader and scholar Antonio Gramsci uttered in 1929 ring true today: “The old world is dying and the new world struggles to be born”.
With lockdowns, curfews, conspiracies and moral panics, the whole world has not only dramatically changed but continues to do so before our eyes.
The suddenness and fluidity of the pandemic means that political, economic and financial projection and risk assessments for 2020 and the 2020s decade have to be re-analysed given the upended global optics. It is for this reason that rating agency Moody’s downgrading of the South African on March 27 is not only preposterous but also based on a world quite different from the one we knew just the other day.
Economic downturns in places like South Africa caused in part by poor governance and in places like Nigeria due partly to oil price wars between Russia and Saudi Arabia will have to be revised afresh.
Parallels have been drawn between the current crisis and past crises of all kinds. Because the pandemic is both a health and economic problem, the global financial meltdown of 2007/08 has particularly shown an unnerving similarity.
How the big powers in the global balance of power manage the crisis on their shores and abroad will be a major barometer for the new world that we are uncertainly entering.
During the 2007/08 crisis, talk of the decline of the West and the rise of what would be referred to as emerging economies was rife. It is perhaps time enough to revisit the works of analysts such as Dambisa Moyo (Dead Aid, 2010, How the West Lost 2011) and Fareed Zakaria (The Post-American World, 2008) to mention but two authors.
More importantly, the global power play revolving around the coronavirus-enforced dynamics will signal the geopolitical shifts that African countries would need to consider. One point among others is that the period immediately after the global financial meltdown over a decade, saw relations between African nations and emerging powers surging with China as the de facto leader. What happens now that both China and the West have been hammered by the virus?
The new normal post-Covid-19 might mean that African nations reliant on aid from the global north and some emerging economies find themselves on their own as hitherto wealthy nations – badly hit Spain, Italy and China come to mind – struggle to reconstruct their battered economies.
Six years ago when the Ebola virus ravaged Liberia, Guinea and Sierra Leone; the US, China and the EU stepped into the breach. Today African countries are virtually on their own as these countries battle the pandemic at home with limited wiggle room to extend a helping hand abroad.
The little we have seen in assistance is the $500 000 support by the USAID to South Africa, the African nation with the highest number of infections on the continent. China, where the virus is commonly believed to have started has been more agile in donating testing kits across the continent. At this point however, the assistance falls short of traditional American and Chinese responses to disasters of the Covid-19 magnitude on the continent.
The foregoing indicates that African countries that entertain the optimism of the world bouncing back to the pre-pandemic times would better get used to the fact the world is already moving in an entirely new direction.
Even though the WHO has been censured for slow action when the virus first surfaced in central China, it would appear that this UN entity is the one that has done the most in providing testing equipment and providing public health information the continent. Should African leaders therefore lobby for a bigger role for this cash-starved entity – and indeed the UN system in general – in the post-pandemic period?
The pandemic is a live demonstration and consequence of globalization while at the same time revealing and accelerating its fault lines.
Save for selected pockets such as South Africa’s fledgling tech industry, Kenya’s nascent innovation hubs and Nigeria’s tech-savvy Nollywood industry, many of the leaps in globalization eluded the African continent. For instance, appreciable use of the internet – globalization’s enabler – started gaining traction only in the mid-2000s long after it had become a way of life elsewhere.
Ironically, Africa’s late insertion into the heart of the globalization may have been a blessing in disguise, shielding the region from would be up early uptick in coronavirus cases.
As a demonstration and consequence of globalization, coronavirus has smashed the records in terms of reaching all the corners of the world at supersonic speed. The dense worldwide web of aerial, marine and terrestrial transport systems played a definitive role in the jumping of the virus from China to the rest of the world. These infrastructures that facilitate globalization ensured that the virus could be in one location in one hour and materialise in another location in a couple of hours.
An observation to make from the transportation dimensions of globalization is that Africa’s weak insertion into the networks meant that the first cases across the board came much later compared to the rest of the world. And, interestingly, the so-called imported cases emanated from Europe, not China!
As a threat to the essence of globalization, it is now evident that coronavirus will accelerate the dynamics in the global political economy that were already in play. Although primarily a health crisis, its magnitude is such that markets have quickly followed suit into pandemic mode.
Turbulence has been primarily seen in the slamming of the breaks on international travel and the closure of borders. In some form of reverse anti-globalism, African countries have been the ones to close their airports to arrivals from the developed world, foregoing the benefits of tourism in the process. It is there a possibility that these actions that have been subject of jokes on social media might lead into new migration and border management regimes between African countries and the rest of the world?
The upshot is that professionals paid to observe the geopolitical terrain will be busy at home in the coming days.
Would a Longitude Prize speed production of a Covid-19 vaccine?
- Chris Callaghan
To stop economic destruction, we need to refocus vast resources from other productive activity – a truly grand prize might do the trick.
The human and economic costs of the current coronavirus outbreak seem to be increasing exponentially as the search for a vaccine goes on. Great efforts in that regard are being made by academics and companies alike, and success seems inevitable given enough time. However, the exponentially increasing human and economic costs of the pandemic raise the question of whether progress could be accelerated.
An instructive case is Ebola. While the 2014-16 outbreak in West Africa was ultimately ended by academics working together with the pharmaceutical industry to developa vaccine, the initial response to the discovery of the disease in 1976 was very slow. Insufficient attention had been paid to the problem, particularly by a pharmaceutical industry focused on more lucrative markets than Africa.
The economic incentives for the industry to pull out all the stops over the new coronavirus seem much clearer given that any company that finds a vaccine will have a captive market of billions of people, including in the world’s wealthiest nations. But that economic return would potentially be quite short-term if the virus mutates again or disappears, as Sars did. Medicines for chronic diseases tend to be prioritised because these are the most profitable.
Yet while companies look to their balance sheets and scratch their heads, finance ministers and corporate leaders look at theirs and tear their hair out. To stop the pandemic before economies are destroyed beyond all medium-term remedy, it may be necessary for them to induce a radical, rapid refocus of vast amounts of resources from activities where they are already productively, profitably employed on to a new goal – finding a treatment or vaccine – with an uncertain pay-off.
Crowdsourcing has historically cracked scientific problems considered at the time not just to be time-consuming to solve but actually unsolvable. In 1714, for example, the British government’s Longitude Prize was used to successfully crowdsource a solution to a problem bedevilling maritime navigation. The effectiveness of crowdsourcing in biomedical research is also well documented. Sites such as InnoCentive demonstrate that the technique is often more effective, quicker and cheaper than in-house research and development.
What if it were possible to do something similar for Covid-19? One option would be for the World Health Organisation or the United Nations to ask countries across the world to pledge and guarantee some significant proportion of their anticipated future costs of the epidemic (one, two, or three years ahead): a figure that would amount to many billions of pounds. Although the R&D costs (as with almost all biomedical crowdsourcing projects) would be borne by the solvers, and although individual countries would pay nothing if a solution was not found, the sheer size of the award might incentivise academic, industrial and government scientists to collaborate at an unprecedented scale.
Given that any solutions would still have to undergo safety testing and clinical trials, biomedical crowdsourcing might be able to “crash” the timelines of the invention portion of the biomedical research process – the most uncertain part of the timeline. Differences in the capabilities of different stakeholders would provide opportunities to develop synergies and economies of scale. Such synergies might increase the chances of success, but policymakers might also need to act in a way that complements the effects of such a large incentive, to mitigate unanticipated outcomes.
While academics are probably less likely to respond to financial incentives, the sums on offer might at least broaden the range of people pursuing solutions beyond the obvious suspects in biomedicine. For example, it might catalyse the application to biomedical science of novel applications in machine learning, big data and artificial intelligence. Proteomics, for example, is a field that is concerned with the biomedical opportunities offered by almost infinite combinations of protein strings.
The academic publishing and grant funding mechanisms might also be used to focus broader academic attention on addressing the pandemic.
History suggests other benefits of such huge R&D efforts. The industrialisation that occurred in countries locked in to solving the singular problem of the Second World War seems to have created a 30-year period of post-war global growth. If a biomedical crowdsourcing effort were undertaken on a large enough scale, the resources brought into the field might provide the capacity to solve many other health-related problems that have hitherto been unsolvable, to the ultimate benefit of humankind
You might object that the UK’s revival of the Longitude Prize in 2014 to incentivise the search for new antibiotics has not yet led to the desired outcome. But this might be because the scale of the incentive – £10 million – is not large enough to shift activity out of already productive uses.
Just as lockdowns are large-scale efforts to match the scale of the coronavirus outbreak, a collaboration between governments to pledge a massive award would also be a response that is proportionate to the problem that they all face.
Chris Callaghan is a Professor in the School of Economics and Business Sciences and at Wits University, and Director of the Knowledge and Information Economics/Human Resources Research Agency (KIEHRA). This article was first published in Times Higher Education.
Bold programmes are needed to mitigate the economic crisis
- Imraan Valodia
The Covid-19 crisis is first and foremost a health and humanitarian crisis is likely to have lasting impacts on how we live.
It is also likely to have a lasting impact, in the long term, on how we conduct our economic lives. In the short term, we need to urgently consider how we manage the economic impacts in a way that does the least long-term harm.
The economic fallout from Covid-19 is unique for at least five reasons. First, unless you have lived through the Great Depression in the 1930s, the extent of the economic decline takes us into uncharted territory.
Second, and more complex, is the fact that we are unable to deal with the crisis employing the normal set of tools we traditionally use in an economic crisis. When an economic crisis occurs, and the level of aggregate demand in the economy falls, we find ways – typically through increasing government expenditure or loosening monetary policy – to boost the level of aggregate demand. In other words, policymakers act to counteract the factors leading to a fall in demand. The uniqueness of the current situation is that we are, from a health perspective, actively trying to suppress the level of aggregate demand.
In order to manage the spread of Covid-19, governments are being forced to ask the population to stay at home, closing schools and universities, and restricting spending in restaurants and bars. In other words, our policy response is further reducing the level of demand. Furthermore, our health policy actions are also impacting on the supply side of the economy. Asking workers to stay at home impacts negatively on firms’ ability to supply goods to the market.
As the level and rate of infections increases, we can expect that not only will we have to deal with increasing costs of healthcare service provision, but the economic dimensions of the crisis will deepen. Both the demand and supply side of the economy will have to be further constrained to manage the infections. In short, this is no time for traditional economic policy tools – we need a bold and different response.
Third, in designing a response to the economic challenges, it is worth noting that the economic fallout has very little to do with purely economic factors. However, unless we act to address the economic fallout, vast swathes of our economic system will be significantly undermined, if not destroyed.
Moreover, we cannot succeed in our health policy objectives to reduce infection rates and “flatten the curve”, if we ignore the realities of our economic life. How does one ask an informal worker not to operate her food stall at a busy intersection without providing relief to ensure that she can feed her family?
Fourth, we don’t know how long the crisis will last and what its final impact will be, but this crisis is a temporary phenomenon, which will end. From an economic perspective, it would be prudent for policies to assist to ride out the storm rather than pick up the pieces at the end. We should be implementing emergency measures to ensure that economic agents – firms, workers and households – are able to maintain as much of their economic infrastructure as possible.
Policies should be aiming to ensure that, as far as is possible, firms do not close down, workers do not lose their jobs and households are able to maintain their current economic standards. The economic costs of retaining firm capacity, jobs and economic life are likely to be much lower than the costs of re-establishing these after the crisis has run its course. Moreover, we cannot ignore the risks to peoples’ health and economic wellbeing.
In South Africa, the economic problems that we have faced for the last few years have already significantly undermined our productive capacity and that of households across the board, but especially so the lowest-income households, who have fewer resources than in previous years. The economic impacts of the Covid-19 infections will have to be absorbed by an already stressed economy.
Fifth, the pace at which the infections are spreading and will continue to spread, notwithstanding the social distancing measures, is exponential. The economic impacts are also being felt at a pace that we have not experienced before. Thus, governments need to act urgently. The Cabinet has acted decisively on the strategy to flatten the curve. We now need urgent action on the economic front.
The following is a set of programmes that could feasibly be implemented on an urgent basis:
The most urgent need is to adequately resource the health system, both public and private, to manage the immediate response to a rise in the level of infections. At least two areas of the health system will be severely challenged – our abilities to test and our abilities to manage the emergency response in hospitals. While healthcare professionals can design the response, they will require substantial additional resources. Based on the experiences of other countries who are further along the path than we are, the health department should be able to estimate, under different scenarios, the economic resources that will be required in the coming weeks. From a fiscal policy perspective, the government should urgently investigate the efficacy of a special appropriation bill to make the necessary resources available to the health system. If need be, the National Treasury will need to revise our fiscal policy and adjust the budget deficit. The economic and social costs of not acting now will be more significant than the economic costs of a temporary adjustment of our fiscal targets. The evidence from South Korea indicates that this health system response is a critical factor in reducing the infection rates and managing the crisis.
Given the challenges in aggregate demand and the complexities with supply chains, firms, both large and small, will have a significant fall in revenue, but not in costs (which may well increase). This will temporarily place pressure on firms’ and households’ liquidity and balance sheets. Unless we have measures to tide firms and households over this temporary “financial shock”, many will be forced to lay off workers and cease operations (for firms), or plunge into severe stress (for households). Here, collaborative strategies with development finance institutions and the commercial banking sector are likely to have significant ameliorative impacts – policies such as temporary mortgage holidays will give firms and households the breathing space to manage the challenge. Interventions of this sort are needed for more systemic temporary relief. Mortgage holidays for owners of a property will allow them to, in turn, allow temporary rent holidays to tenants. In short, we need to investigate temporary financial instruments to manage the pressure on the liquidity of firms and households.
Government has already announced measures to use the R180-billion surplus in the Unemployment Insurance Fund (UIF) to assist firms and workers. While these measures are to be welcomed, a short-term holiday on UIF contributions is unlikely to have a major impact. On a more positive note, using the Training Layoff scheme, which suspends the employment relationship and pays the worker 75% of the wage, will have a positive impact. Even this, however, may well be insufficient. It is interesting to note that even right-wing governments like the UK are providing guarantees to cover 80% of the salary of workers that may be temporarily laid off work.
Our most vulnerable group of South Africans are poor pensioners. This group has the highest level of risk and the least ability to themselves manage the challenge. South Africa is in the very fortunate position of having direct access to this group via the old-age pension and grants system. Policy interventions like one (or more) additional payments to this group (a 13th cheque) may go a long way to increasing their ability to manage the shock.
One particularly vulnerable group is workers in the informal economy. South Africa has approximately 3-million informal workers. This group is especially vulnerable because their daily work activity – selling small batches of tomatoes, preparing meals, collecting waste, etc. – is the only way by which they and their families are able to survive. Many of these workers are itinerant, and operate in areas like taxi ranks, where large numbers of people congregate. Unfortunately, we do not have an easy mechanism to provide support to this group, but unless we find a mechanism to do so, the repercussions will be serious, on both health and economic considerations. I am not, under normal circumstances, a supporter of a universal income grant, but in these extraordinary times, the government will have to provide income support to this group. A short-term, emergency universal grant to all South Africans for a fixed period of time, to be recovered later through the tax system, may well be a necessary and effective measure. A measure such as this, linked to an ID number to be cashed through the banking system or even at retail outlets, may well be feasible to implement, even for those without bank accounts.
The government should be careful not to focus exclusively on the poorest among our citizens. The economic impacts of Covid-19 will be felt by the middle classes too (in South Africa, the middle classes do not have particularly high incomes). Policies such as interest-free credit card purchases of food and medical supplies for a period of six months would go a long way toward protecting middle-income groups.
From a health response perspective, we are likely to face severe shortages of vital medical equipment and drugs – gloves, ventilators, drugs such as prednisone, etc. Special procurement arrangements with manufacturers, similar to those entered into for antiretrovirals, will not only boost economic output, but also build the capacity of the healthcare system to manage the upcoming challenge.
Our scientific capabilities to better understand the medical and social dimensions of the Covid-19 challenge will likely have a significant impact on our ability to manage the challenge. South Africa has excellent capacity in its universities and science councils to assist with the global effort to manage the crisis. Two interventions may be useful: first, to appoint a high-level scientific committee to advise (like many South Africans I am concerned about the plethora of advisory bodies, but this is a crisis and we should have the best minds advising); and to make available a competitive research grant fund for short-term research interventions to assist in managing the crisis.
Government has acted speedily to address the challenges of price gouging of critical products like food and medical supplies. In general, price controls are not a good idea because it creates further opportunity for hoarding and “black markets”. However, there may be a good case for the government to work with the private sector to establish price controls in a few very specific medical items. If the pandemic spreads as it is expected to, South Africa will need a significant capacity to test for the virus. We should urgently be developing local capacity to produce testing kits. Also, the price of a testing kit, whether in the public or private sector, should be set at a price that will be affordable. Currently, a Covid-19 test in the private sector costs between R1,000 and R1,200 – this is clearly unaffordable. If we are to make Covid-19 testing kits available to all, this price will have to be reduced.
Our economic policymakers need to be working in concert with each other. While respecting the independence of the South African Reserve Bank, we need a fiscal and monetary policy to be fully coordinated. Furthermore, it is important that our policies, both on health and economics, are aligned with countries in the region. While it is important to close borders to reduce the spread of infections, South Africa’s health and economic systems, however inadequate, are much better resourced than our neighbouring countries. We should be working collaboratively to manage the health challenges and coordinate our economic measures.
In summary, these are extraordinary times. The impact of Covid-19 will have to be absorbed by an already fragile economy. Millions of South Africans live well below any benchmark of a reasonable economic life and, unfortunately, this is precisely the group that will be most affected by the economic fallout from Covid-19. The 100-basis points reduction in the repo rate by the South African Reserve Bank provides some relief. However, this is hopelessly inadequate for the task at hand. What we need is an urgent economic policy action. Unless we address the economic challenges, our health policy efforts to flatten the curve will be compromised and the risks of economic inaction are significantly higher than decisive action now.
Professor Imraan Valodia is the Dean of the Faculty of Commerce, Law and Management at Wits University. This article was first published in the Business Maverick.
Covid-19, #ClimateEmergency and Lockdown
- Vishwas Satgar
The coronavirus is an opportunity to end the war with nature.It’s a moment to be humble and realise our finitude in a wondrous and infinite natural order.
Covid-19 has pushed an already weak and crisis-ridden global economy over the edge. Massive value has been erased from crashing stock market prices. Many commentators are talking about the return of economic conditions similar to the great financial crash of 2007-2009. The most powerful countries in the world from China to the US have ground to a halt.
This pathogen, possibly from delicate creatures like a pangolin or a bat, has engendered the worst global pandemic since the Spanish flu (1918-1920), which killed 100-million people. Death rates are going up globally. Right-wing nationalists in Europe and the USA have been confused as this virus has jumped racist border regimes, and infected all populations. Citizens are no longer concerned about their racist messages, but rather about how to survive.
Governments all across the world are seized with the challenge of protecting their populations, at least that is what it seems like given the people-centred rhetoric. The geo-politics of Covid-19, engulfing the entire globalised world in its rapid spread, is also a shot across the bow of carbon capitalism. Elite consumption of exotic animals, at high prices, in Wuhan, China unleashed the swift and lethal revenge of nature.
This does not mean that this is a “Chinese virus” as the racist Donald Trump has suggested. We are all susceptible and are trying to live through the fear, paralysis and risks brought by this pandemic. Overnight, jobs have disappeared, paycheques have shrunk, loved ones are in critical health situations fighting for their lives and hunger is knocking on the door of many. Healthcare systems, weakened and commodified through decades of marketisation, have or will be overwhelmed.
Yet the very same elites that caused the problem are not carrying the burden of the consequences of their actions. For climate justice politics, these injustices are not new. Elite use and consumption of fossil fuels is linked directly to extreme weather shocks such as heatwaves, droughts, floods and cyclones, for instance, which impact those most vulnerable the hardest. Yet there is no consequence for those responsible and the fossil fuel industry, carbon-addicted states, and the wealthy carbon-based consumers continue as though climate science does not exist.
‘Black Swan’ event, or worsening systemic crisis
In the business world, Covid-19 tends to be reduced to a “black swan event”. A sudden or unforeseen happening, with great consequence and rationalised after the fact. The idea was initially popularised by Nassim Nicholas Taleb’s five volumes on uncertainty including the famousBlack Swan, which has been described as one of the most famous books since World War II. While in his work, the concept has a richer philosophical grounding, it has become part of everyday risk management discourse. Business risk analyses missed the likelihood of a Covid-19 pandemic and it certainly was not a concern. Its occurrence, however, cannot be explained as a black swan event.
From an ecological Marxist perspective, it has to do with the contradictory relationship between natural and social relations, has a historical genealogy within how eco-cidal capitalism works and can be causally attributed. Simply, for Covid 19, this means it’s a dangerous problem that is engendered by capitalism’s persistent domination of nature.
It spread from a “wet market” involving organised crime syndicates, linked to shadowy global poaching, and smuggling networks that steal wild creatures from their habitats and place them on elite menus. Avaricious Chinese capitalism, with its appetite for resources and capturing markets, like the West, understands nature as a site of extracting value; nature must serve the juggernaut of accumulation.
South Africans are now familiar with the appetites and reach of this capitalism due to the annihilation of our rhino population merely for their horns. Wet markets also exist in other parts of South and East Asia, and have not been restricted, leaving open the possibilities of new waves of pandemics.
For many years, epidemiologists and environmentalists have been concerned about the public health consequences of such markets, given that animal to human transmission of deadly viruses is a known fact and has been implicated in avian flu (from birds), MERS (from camels) and ebola (monkeys), for instance. These animals are also traumatised and kept in unsafe conditions.
In Brazil, Jair Bolsonaro has unleashed land grabs in the Amazon – one of the most bio-diverse habitats on planet Earth. Industrial farming, mining, logging and wild animal poaching are ending the natural protective barriers between human society and ecosystems, heightening the risks of pathogens spreading, but in this case also contributing to climate change, given the role the Amazon plays in a planetary ecosystem to sequester carbon.
Climate scientists have already warned humanity that further warming of the Arctic, for instance, will not only release deadly greenhouse gases such as methane, but also pathogens that have been frozen into ice sheets. Like Covid-19, the worsening climate crisis and its global shocks, are not black swan events, but dangerous systemic crisis tendencies produced by a hard-wired logic based on the duality of capitalism versus nature. Science has provided us with understandings and warnings, and yet the global capitalist system persists in driving us towards harm and destruction.
Carbon capitalism and imposed collective suicide
A world led by those who place profit above human and non-human life, is placing us all in jeopardy. We are not given a choice as the eco-cidal logic of global capitalism destroys the conditions that sustain life. Our planetary commons – biosphere, oceans, forests, land and water sources – are all being commodified and destroyed to make a few wealthy.
On a planetary scale, we are living through an imposed collective suicide. As neoliberalism becomes authoritarian and mutates into the second coming of fascism to defend the wealth of the few, it is revealing a simple fact: It’s not learning lessons about the harm it is inflicting. Instead, it wants to defend at all costs a life-destroying system.
Karl Polanyi in the social science classic, theGreat Transformation(1944), drew attention to such elite behaviour when the ship is sinking. In the late 19thcentury, based on marketisation through the gold standard, the world was driven into World War 1. Lessons were not learned and the world was again locked into gold standard marketisation in the 1920s, and this gave rise also to fascism and World War 2.
This time, we are all dealing with the failure of capitalism’s conquest of nature through treating it as capital through financialisation. The science on biodiversity loss, climate and water, for instance, are all unequivocal that we are breaching limits and surpassing boundaries that endanger everything. At the same time, the raw and infinite power of nature is gathering pace. The present generation of young people understand the dangers of this very well. One of my former students, an extremely intelligent and sensitive young person, placed this public post on his Facebook page in the midst of the Covid-19 outbreak:
Tonight, for the first time in a long time, I cried. I felt everything inside of me: the depth and immensity of my pain, my sorrow, my grief, my lament, my worry, my confusion, my longing, my despair – I felt it all and wept, wept for the sadness I’ve kept hidden so long, wept for the loved ones I miss so dearly, wept for the suffering and uncertainty of the world, wept for reasons I don’t even understand.
Many of us weep for the collective suicide we are living through. This is not about victimhood, but about understanding the depth of crisis and the urgency to overcome this universal challenge of our extinction. It is a conscious knowing rooted in deep wells of pain, anxiety and existential suffering growing in prevalence among the young because of the collective suicide being imposed by financialised carbon capitalism.
Greta Thunberg and many of the young climate activists in South Africa such as Raeesah Noor Mohamed, Nosintu Mcimeli, William Shoki, Awande Buthelezi, Jane Cherry and Courtney Morgan, to name a few, understand this. They carry their pain, their understanding of injustice as they protest.
But is the present resistance enough? The cry of 1 degree Celsius movements – Sunrise Movement, Extinction Rebellion, #FridaysForFuture and the Climate Justice Charter process in South Africa – are all coming up against power structures and ruling classes not willing to break with the imposed collective suicide of financialised eco-cidal carbon capitalism. Yet in the context of Covid-19, not only are global populations shocked, but it has rocked, assailed and unhinged the very same power structure standing in the way of addressing the climate crisis. Covid-19 is forcing, even reluctantly, ruling classes to try to act with concern for life.
Lockdown and the ANC’s epidemiological neoliberalism
Covid-19 has thrown us into a state of exception. From a climate justice perspective, this is a dress rehearsal for a world that breaches 2 and 3 degrees Celsius in which climate shocks on a global scale imperil life-supporting socio-ecological systems such as food, water and health systems through unbearable temperatures. Waking up then is too late.
This is the underlying premise of climate justice activism, given that climate science is telling us what is arriving with business as usual or low mitigation trajectories. With the Covid-19 crisis, our governments seem to be suddenly realising markets and corporations are not more important than human life. Is this the case?
The disaster capitalism of Covid-19, as Naomi Klein reminds us, brings forth profit-making opportunities even from the suffering of the people. Trump is leading the way. His first crucial move was to build up fossil fuel reserves thus keeping oil prices bolstered, then he unleashed the privatised healthcare system and is now keeping pharmaceutical companies “free” to manipulate the prices of essential medical equipment instead of repurposing production through the Defense Production Act. However, this is not the end of the story and struggles inside US society will certainly determine if Trump’s epidemiological neoliberalism will triumph or not.
In South Africa, we have been witness to a sea change from kleptocratic state and neoliberal austerity policies (including cutting billions of rands from health spending), announced by Minister of Finance Tito Mboweni, to cross-subsidise corrupted and failing parastatals, to the war on Covid-19.
The country is going into this government-declared war with a dualistic healthcare system, with the vast majority dependent on a public healthcare system gutted by corruption, mismanagement and austerity. This healthcare system, with these specific features, is what is going to be overwhelmed not just by Covid-19, but by over two decades of ANC misrule. The lockdown of South Africa has to be understood in this context.
Put more sharply, the warped rationalities of commodified healthcare for a few and failing healthcare for the many is clearly the frontline the government is trying to avoid in the country’s Covid-19 response. For most South Africans, in a state of shock and panic, this lockdown crash-landing of the economy on the wretched lives of a precarious working class and poor seems like the best response.
Of course, this shock therapy has been administered repeatedly since neoliberal strictures informed the first democratic budget in 1994 and the macro-economic shift of 1996, kleptocratic neoliberalism of the Jacob Zuma project and now the new epidemiological neoliberalism of the ANC. In this context, the so-called China success story of shutting down Wuhan peppers government-speak.
But the other epidemiological success story of South Korea is not referenced. South Korea did not lock down its economy, but put the emphasis on: (1) intervening fast through test kits produced (100,000 a day), on a mass scale domestically; (2) test early, often and safely (it has conducted over 300,000 tests), such that detection happens quickly; (3) contact tracing, isolation and surveillance, which has used smart apps, mass messaging and has prevented an overload on the healthcare system; and (4) enlist the public’s help. While not perfect and easily replicable, it’s nonetheless an important alternative to lockdown.
South Africa’s lockdown has not been preceded by mass testing despite the two-month lead time the South African government had since the outbreak in China. Even as the country goes into lockdown, the costs of tests are prohibitive, there has been no clear communication about international partnerships to get testing going on a mass scale, there is no clear messaging on testing details and grassroots civil society has not been mobilised, despite its enthusiasm to rise to the challenge.
Instead, the lockdown has shifted the focus to managing economic chaos, mitigation measures and privatised charity through a “solidarity fund”. Deep anxiety, fear and insecurity is running through society. South Africa is going into the lockdown as one of the most unequal countries in the world.
The crisis of socio-ecological reproduction is deep as expressed through high levels of structural unemployment, intra-African income inequality, hunger and water inequalities (54% of South African households do not have access to clean water through a tap in their homes).
Lockdown means South Africa’s precarious working class and poor are now responsible for solving the Covid-19 problem because they carry the burden. Lockdown is meant to save their lives while worsening their already wretched life worlds. Hence the ANC government is off the hook with this cunning move of epidemiological neoliberalism while taking Covid-19 disaster capitalism to a new level.
Ending the war with nature
Covid-19 is an expression of contradictory natural relations. On the one hand, it is devouring the most vulnerable in our society and, on the other hand, it is prompting humanity to slow down collective climate suicide. Carbon emission data is certainly going to register deep drops since the onset of Covid-19, with airlines, shipping, cars and other carbon-emitting technologies brought to a halt.
Covid-19 has achieved what almost three decades of UN multilateral negotiations have failed to achieve. If governments can take the Covid-19 emergency seriously, they can take the climate crisis seriously. The UN climate meeting in Glasgow this year has to open with lessons learned from Covid-19 to address the global climate emergency. In this context, South Africa will have to tell its story to the global public. However, there is a lot the South African government should consider as this pandemic unfolds, including its war-on-Covid-19 approach.
South Africa’s government declared Covid-19 a disaster in terms of the Disaster Management Act. It has unleashed an important coordination capacity in the state, preventative regulations, is disseminating information, has imposed a 21-day lockdown and introduced economic mitigation measures. The command structure is led by the president. The Disaster Management Act was not kicked into gear during the worst drought in South Africa’s history (2014-till now), which ravaged numerous communities, collapsed part of the globalised food system and pushed up food prices. Many communities still have acute water needs and are being challenged to maintain basic hygiene.
As Covid-19 transmission spreads, water-stressed communities are going to be hotspots as these are poor communities and very likely to also have many with compromised immune systems. If the drought was handled properly by the ANC government, water issues would not have been a problem now.
Moreover, if the ANC government did not get caught up in the tides of populism around the land question and listened to the South African Food Sovereignty Campaign, including taking seriously their Peoples Food Sovereignty Act handed over to Parliament, we would be sitting in the midst of Covid 19 with more communities, villages, towns and cities having localised agro-ecological food sovereignty pathways to cope with the current situation. Instead, we are living the drama of a war-centred crisis management approach.
The war approach to Covid-19 is limited in three respects and holds out dangers for how leadership is practiced now and what capacities we build in this defining moment. First, war works with a simple logic. There’s an enemy, militarise (build war-making capabilities), mobilise your society in the effort and deploy this to destroy the enemy. It is a reductionist way of thinking; it is not a systems view of the world.
Covid-19 is manifesting in our midst together with other systemic crises, such as economic crises and climate crises. Financialised capitalism has produced an unstable global economy and grotesque inequalities. It has not worked. The climate crisis is worsening with a lack of will to phase out fossil fuels and decarbonise.
We are facing a 1.5 degree celsius increase in planetary temperature most likely in the next five years, accompanied by intensifying climate shocks. These crises are interconnected, cascade into each other and push our socio-ecological orders towards collapse. A war mentality does not appreciate the interconnectedness of all of this.
Put differently, even if Covid-19 is addressed with war-like precision and the epidemiological curve flattens globally and in South Africa, we are not returning to a new normal. We are returning to a world in permanent crisis; a new abnormal. Hence, how we address Covid-19 and reconstruction after it, must lock in democratic systemic reforms that cushion us from more crises.
South Africa will need an eco-justice stimulus package to tackle the impacts of Covid-19, the economic crisis and worsening climate crisis. South Africa’s climate justice charter is a crucial point of departure in this regard.
Second, a war approach to Covid-19 is based on dangerous philosophical foundations. It continues the anthropocentric conquest of nature, central to capitalist thinking. Killing Covid-19 in this frame is about us being the dominant species. We demonstrate to the forces of nature our superiority. This is really a conceit which fails to understand that nature has been and will always be more powerful than us.
Moreover, we are extremely dependent on nature as a species to ensure our reproduction. With Covid-19, we are really trying to mitigate the revenge blow from nature. It’s a moment to be humble and realise our finitude in a wondrous and infinite natural order. We are just one little part of a vast and delicate web of life. Ending Covid-19 should be about ending the war with nature. This includes ending wet markets for exotic animals, ending globalised industrial agriculture and rapidly phasing out fossil fuels.
Third, the war on Covid-19 keeps us bound up in an ethical knot and derives from deeply oppressive ways of thinking. Violence whether colonial, imperial, patriarchal, racist or eco-cidal is not what the world needs. Modern industrial scale violence that is calculated, instrumental in its reason and deadly is breeding a fast violence from nature. A violence we cannot match. Everyday violence of poverty and structural inequality has to be addressed as we come out of this pandemic moment.
Complex and holistic systems thinking, grounded in an ethics of care rather than war has to prevail. Put differently, if Covid 19 helps jettison the Thatcherite neoliberal subject – competitive, greedy and possessive individual – for a more humane state of being and solidarity-based society, it would have produced our strongest defense against a crisis-ridden world. It would have also affirmed an ethics of care for our natural relations that nurture us, feed us and enable us to have life.
Dr. Vishwas Satgar is an Associate Professor of International Relations, Wits. He edits the Democratic Marxism series, is the principal investigator for Emancipatory Futures Studies and has been an activist for four decades. He is the co-founder of the South African Food Sovereignty Campaign and the Climate Justice Charter process. This article was first published in the Daily Maverick.
Foreign migrants must be included in Covid-19 response
- Jo Vearey and Sally Gandar
Why South Africa needs to actively engage all foreign migrants in its response to Covid-19.
It is a well-established fact that for infectious disease control measures to stand any chance of success, they need to reach everyone. This is no different in the case of Covid-19 in South Africa, yet our response to controlling the spread of the virus, and protecting those most vulnerable to infection, continues to exclude marginalised foreign migrants.
Our response to more privileged international tourists and visitors, and those in South Africa for the purposes of work and study, has, however, been far moreproactive. Covid-19, as with any other communicable disease, knows no borders and its spread within South and southern Africa is inevitable. We need to slow down the spread of infection so that our region’s already over-burdened and struggling health systems have a chance to respond.
International travel restrictions
On Sunday 15 March 2020, President Cyril Ramaphosa announced the National State of Disaster in terms of the Disaster Management Act, outlining a number of drastic steps to try and curb the spread of Covid-19. On Wednesday 18 March 2020, some of these actions came into effect, one being a range ofinward travel restrictionsimplemented by the South African Department of Home Affairs (DHA).
These restrictions – designed to reduce the spread of Covid-19 by supporting its containment – are applicable to inbound travel from countries that DHA has defined as “high-risk” – those where there is ongoing, the community-level transmission of Covid-19 as per thedaily situation reportspublished bytheWorld Health Organisation (WHO).
Underthe International Health Regulations (IHR), the decision to implement any restrictions on inbound travel is a sovereign one, meaning that any given country can choose which countries to include – or not – within their respective travel restrictions. Travel restrictions are, themselves, matters of “health diplomacy” and states must balance the need for an effective public health response to the control of infectious disease with the negative impacts of restricting travel, which can include detrimental effects on the movement of goods and disruptions to social structures.
While there is evidence to suggest that travel restrictions can be effective at the start of an infectious disease outbreak by delaying the spread of disease and – importantly – allowing for the implementation of national preparedness plans, once community-level infections become more established the positive impact of travel restrictions lessens. An example of the negative consequences of travel bans includes a report from the Minister of Health, Dr Zweli Mkhize, who indicated on Thursday evening (20 March) that Covid-19 test kits on their way to South Africa had not yet arrived due to the cancellation of international flights.
The current travel restrictions are applicable to air, land and seaports of entry, and interventions implemented include closing35 of South Africa’s 53 land borders, reducing the number of seaports where crew and passengers can disembark from ships, and restricting entry to individuals travelling from or through countries deemed “high risk” by the DHA.
In fact, the DHA has now prohibited entry of all foreign travellers coming from, or via, high-risk countries, regardless of pre-existing visa or visa waiver agreements. Visa waiver agreements with medium-risk countries are also suspended. This applies to persons holding passports who would usually be exempt from requiring a visa to enter South Africa, or who would usually obtain a visa upon arrival.
A selective right to remain
Citizens of countries the DHA has deemed high or medium risk – which corresponds to many European countries and the US – who hold a valid visa, and who wish to remain in South Africa, can extend their visas, as perImmigration Directive 7 of 2020, dated 17 March 2020. Such persons “will be allowed to re-apply for such visa” subject to certain requirements, and visas valid to 31 July 2020 may be issued. If these foreign nationals do not meet all the requirements, they may be able to apply for a waiver subject to further requirements.
In addition, the directive allows for people from these high-risk countries whose visa has expired since 1 December 2019, to “re-apply for such visa”; they will be exempt from the usual conditions associated with “over-staying” on an expired visa. How the bureaucratic processes regarding these applications will be managed remains to be seen but it is going to place further pressures on an already struggling DHA.
While these efforts by the DHA are welcomed as part of a national and international solidarity in response to Covid-19, we have serious concerns about who we are leaving behind and the resultant risk for the health of all who live in South and southern Africa.
Key here is to ask what these special measures – particularly in relation to visa extensions and “the right to remain” – mean for foreign migrants currently in South Africa who have travelled from neighbouring countries that arenot(yet) considered high-risk. Presently, citizens of European countries and the US currently in South Africa are protected by the new Immigration Directive, but it is silent on foreign nationals from the region whose visas may have expired. This group of migrants are likely to be afraid to test or report to others that they are unwell for fear of arrest, detention and deportation, with particularly worrying implications for contact-tracing.
Solidarity or securitisation?
In Monday’s media conference, the Minister of Home Affairs, Dr Aaron Motsoaledi, spoke of the importance of “international solidarity”, acknowledging that South Africa has more cases of Covid-19 thanneighbouring countriesand, as a result, has a responsibility to protect countries elsewhere in the SADC region.
The minister also indicated that the choice of the 35 ports of entry that will be closed, was motivated by the aim to “stop the virus from moving through our borders”. Motsoaledi stated that they would be “putting up a lot of higher walls in this war” (presumably against Covid-19) and this was clearly no metaphor aswe now see a R37.2-million wall being builtalong the border between South Africa and Zimbabwe. To date, Zimbabwe has not reported any cases.
On Thursday evening, during a Q&A session about Covid-19 with the South African Medical Association, the minister of health stated that South Africans must recognise that neighbouring countries do not pose any risk to South Africa. Rather, it is our infection rates that pose a risk to them.
Regardless of the seemingly contradictory positions of the two medical doctors currently steering our response to Covid-19, R37.2-million is being spent on a border wall. Is this the most appropriate use of taxpayers’ money? How many test kits could be purchased for the same amount? Intensive care beds? Respirators? Personal Protective Equipment (PPE) for frontline healthcare workers?
Each Covid-19 test done by the National Institute for Communicable Diseases (NICD)costs the stateR300. That means that the amount spent on the fence would fund 124,000 testing kits. The private pathology labsare chargingbetween R900 and R1,400 for the test. The amount spent on the fence would thus fund between 41,333 and 39,333 testing kits at private laboratory rates.
Similarly, if one looks at wages, the living wage calculator indicates that a living wage in South Africa is R6,570/month. The amount being spent on the fence would equate to assisting 5,662 persons with a living wage for one month to try and ameliorate the impacts that the Covid-19 pandemic may have. A further comparator that we can use is the SASSA Older Persons Grant, which many people across South Africa rely on to survive. This grant amounts to just over R1,780 per month. The R37.2-million to be spent on a fence, would provide for the equivalent of 20,898 old age pension grants, or if made available to persons for a three-month period to try and ameliorate the impacts of Covid-19 on the economy, it would assist over 7,000 people for that period. These may seem like small numbers when we think of the numbers of the South African population that will be impacted by Covid-19, not necessarily by being infected but by losing their income, but one thing is certain, building walls – or a fence – will help no one.
It is not the time to implement such securitisation measures (many of us would argue that there is never such a time); the spread of Covid-19 will not be stopped by a border fence. The effects of such a response are likely to cause further harm to all in South Africa and the region by forcing individuals – particularly those currently holding an irregular status – to cross the border through other means, resulting in migrants being further distanced from any public health intervention.
Urgent measures are required to ensure we include all foreign migrants – not only tourists and international travellers from high- and medium-risk countries – in our response to Covid-19. There needs to be assurance that, regardless of their current documentation status, no foreign migrant willface any sanctionswhen engaging with state authorities, including when seeking healthcare or being included in contact tracing. Without this, our efforts to reduce the spread of Covid-19 will fail.
Jo Vearey is with the African Centre for Migration and Society (ACMS), Wits University. Sally Gandar is with the Scalabrini Centre of Cape Town. This article was first published in the Daily Maverick.
Hypocrisy in the time of Covid-19
- Jo Vearey
The sanctimony of moving from blaming foreign migrants to rendering them invisible in a critical public health moment will have implications for our response.
Before Covid-19, the South African field of migration, health research and advocacy meant investing energy in countering prevailing, unfounded negative public and political discourse that incorrectly blames foreign nationals for the failures of the South African public health system.
This dangerous, xenophobic and racist rhetoric positions certain migrants who have travelled across the country’s borders as “contagious” and as importers of infectious disease. This scapegoating, in addition to the various structural challenges faced by foreign migrants (including difficulties in accessing the documentation required to be in the country legally), has resulted in a plethora of negative outcomes that affect everyone in South Africa. One such result, of particular importance in the time of Covid-19, is the challenges that foreign nationals reliant on the public healthcare system face when trying to access the services to which they are legally entitled; we need to think carefully about the implications of this for an effective national, and regional, response to Covid-19.
Numerous evidence-informed callshave been made for ensuring that migrant and mobile populations are included in the development of responses aiming to achieve universal health coverage in South Africa, the Southern African Development Community (SADC), and globally. Such calls are about far more than the right to good health; they are about implementing a public health approach that will address the political and social determinants of poor health, including those that result in poor access to healthcare. In turn, such a public health approach aims to support the goal of improving health for all.
The fear, however, is that South Africa and SADC may now experience the public health consequences of xenophobia, racism and blame.
South Africa is currently making difficult decisions about how best to “flatten the curve”, determining the most appropriate interventions to slow down the spread of Covid-19 and protect the most vulnerable in our society. Yet there is a notable absence of visible engagement with the very population who have, until now, been unfairly placed at the forefront of many South African debates relating to a struggling public healthcare system and a high prevalence of communicable diseases, notably HIV and TB.
This hypocrisy – of moving from blaming foreign migrants to now rendering them invisible in a critical public health moment – will have implications for our response to Covid-19. It is essential that we effectively include foreign migrant populations in our programming. A failure to do so risks devastating impacts not only for foreign migrants, but for all in the South and southern African population as a whole.
And this includes the Department of Home Affairs thinking carefully about its role and responsibility in the time of Covid-19; for example, what are the public health implications of DHA’s approach to border management and requirements for asylum seekers to renew their permits every 3-6 months?
With Dr Aaron Motsaledi in place as the minister of home affairs – a former minister of health and medical doctor – this should be an obvious way to go,but recent history has told us otherwiseand it is now time to turn the tables. We need SADC member states to be bold and develop regional responses. Now is not the time – we don’t have the time – for diplomacy. Political differences in what a regional health approach should look like need to be set aside in order to ensure we have cross-border Covid-19 responses in place.
A public health approach is not only relevant in the time of an epidemic, it is based on principles of justice, equity and respect. Now, more than ever, we need to enact these values. We need to target interventions to those who have been left behind. Evidence generated over the past few decades, which has been regularly communicated and shared with key decision-makers, service providers, and the wider public, clearly indicates that there are populations in South and southern Africa who have been left behind in our public health planning. This includes certain groups of foreign migrants, sex workers and others working in the sex industry, and members of the LGBTQI+ community.
In addition, we know that while there have been gains made – mostly attributed to the actions of civil society and public health advocates – in the provision of health interventions to residents of informal settlements and hostels, as well as to those who are incarcerated in prisons and within the Lindela detention centre, we know that these populations remain left behind in our preventative and curative health responses.
HIV and TB are concentrated in these spaces, the result of persistent structural and political determinants of poor health, placing these populations at an increased risk of the worst health outcomes associated with Covid-19. People reliant on overcrowded public transport and housing solutions can do little to effectively practice social distancing or self-isolation. It is especially ironic that – among other groups – the very population who, until now, have been considered responsible for poor health in South and southern Africa are being left-behind: foreign migrants.
Whether the apparent lack of consideration of foreign migrants is a result of their continued exclusion in public health planning, or due to the initial cases of Covid-19 identified in South Africa being imported from outside of the African continent, is irrelevant. Perhaps the tables have turned and recognition of the ways in which international tourist travel can be associated with the spread of infectious diseases has been brought to light, challenging and perhaps even silencing, at least for now, the pervasive blaming of foreign migrants for the health challenges faced in South Africa.
Jo Vearey is an Associate Professor and Director of the African Centre for Migration & Society (ACMS) at the University of the Witwatersrand. She is also Vice-Chair of the Migration Health and Development Research Initiative (MHADRI). This article was first published in the Daily Maverick.
Wits Covid-19 Update (18)
- Wits University
The role of essential staff during the national lockdown.
MESSAGE FROM THE SENIOR EXECUTIVE TEAM
Dear Colleagues
Please note the University’s position on the role of essential staff during the national lockdown period:
1. Staff that are not essential services staff and are able to work from home during the lockdown period are required to work;
2. Staff that are not essential services staff and are not able to work from home but would ordinarily be required to work are not expected to come to campus and work; and
3. Staff that are essential services staff are required to work on a rotational basis where appropriate.
In terms of Section B(1) of Annexure B of the amended Regulations issued in terms of the Disaster Management Act, 2002 on 25 March 2020 (“the Regulations”) the following categories of staff are considered essential services staff:
a. Medical Services;
b. Animal Care Services;
c. Financial Services necessary to maintain the functions of the payments environment;
d. Laboratory Services;
e. Cleaning, Sanitation and Waste Removal Services;
f. Security Services;
g. Critical Maintenance Services; and
h. Staff assisting with accommodation for essential services staff.
The relevant line managers, who have been appropriately authorised, will be in contact with employees who form part of essential services with a plan on how operations will be expected to continue during the lockdown period. Essential services employees will be issued with a formal letter and permit from the University which authorises them to leave their places of residence to attend to work.
The University will ensure that the proper precautions are taken in the workplace to mitigate against the risks identified in the context of COVID-19.
The Senior Executive Team is finalising a protocol around leave and other arrangements. This will be shared with organised labour and staff in due course.
Once again we thank all staff for their contribution to the University and society during these exceptionally difficult times.
SENIOR EXECUTIVE TEAM
26 MARCH 2020 (16:00)
Wits COVID Update 17: Staff Appreciation and Reopening
- Wits University
Prof. Adam Habib addresses staff on living through the COVID19 pandemic and expresses his appreciation to staff for their contribution during this period.
The target date for Wits to reopen is 20 April 2020, in line with the rest of the higher education sector, but this is dependent on how the pandemic evolves. The mode in which the second block is likely to be online and staff are thus advised to prepare to take teaching online with the support of Wits ICT, the Centre for Learning, Teaching and Development, and Faculty Teaching and Learning units. Students will also require additional support when contact teaching resumes in the form of additional lectures, tutorials and boot camps, as appropriate.
The video addresses issues related to the digital divide, access to smart mobile devices and data, and the University’s agreements with ICT providers to zero-rate sites. Wits has reached out to broadcasting houses to determine if they can provide a solution to reach 10% of Wits’ students who do not have access to smart mobile devices. Faculties should also explore other practical ways in which this can be achieved.
Wits COVID Update 17 (Students): Wits to reopen on 20 April
- Wits University
Prof. Habib speaks on living through the COVID-19 pandemic, and the Senior Executive Team’s (SET) decision to go into early recess and to evacuate residences.
The target date for Wits to reopen is 20 April 2020, in line with other universities in the higher education sector, but this is dependent on how the pandemic evolves. The mode in which the second block will open is likely to be online and students are thus advised toprepare to go online. Professor Habib addresses issues related to the digital divide, access to smart mobile devices and data, and the University’s agreements with ICT providers tozero-rate sites. Wits has reached out to broadcasting houses to determine if they can provide a solution to reach the 10% of Wits’ students who do not have access to smart mobile devices. This figure is based on the results of a comprehensive biographical questionnaire conducted annually by Wits. Faculties are also exploring a range of other possibilities to ensure that all students are appropriately supported.
Amongst the best in their fields, Wits experts are at the frontlines and behind-the-scenes against COVID-19, the respiratory disease caused by the coronavirus.
Eminent academics at Wits University in disciplines including epidemiology, medicine, public health, biomedical engineering, governance, and others, are the unsung heroes leading the charge against COVID-19.
The pandemic galvanized President Cyril Ramaphosa on Sunday, 15 March 2020, to invoke a state of disaster in South Africa, and then a national lockdown effective midnight, Thursday, 26 March 2020.
There is hope against this viral pandemic, however.
In concert with the National Institute of Communicable Diseases (NICD), the Department of Health, and the South African government, an army of heroic scientists at Wits are helping to understand, predict, and contain COVID-19, manage the public health and socio-economic impact, and develop treatment and care regimens.
The Wits heroes mentioned here represent just a fraction of the University’s community of academic, professional, and support staff who all are working tirelessly and contributing in multiple ways to mitigate this state of disaster.
We salute you all.
Understanding the enemy
Professor of Epidemiology in the Wits School of Public Health, Cheryl Cohen is a medical doctor and co-head of the Centre for Respiratory Disease and Meningitis at the NICD. Through her work she aims to generate evidence to guide policy for the control of respiratory diseases. In 2009, she led the establishment of a national surveillance programme in South Africa for severe acute respiratory infections. She is at the forefront of COVID-19 case-finding, diagnosis, management and public health response. In this video, Cohen explains how the NICD Help Lines can assist the public and healthcare workers respectively.
Adriano Duse is Professor and Head of Department of Clinical Microbiology and Infectious Diseases at Wits. On 12 March 2020, Duse delivered a public lecture entitled, Myths and Facts about SARS-CoV-2: The COVID-19 Outbreak 2019-2010 – What you can do to reduce infection risk, hosted by the Wits Students’ Pathology Society. In January 2020, Duse delivered a radio Masterclass on Superbugs. Listen to the podcast.
Kerrigan McCarthy is a clinical microbiologist and Head of the Division of Public Health, Surveillance and Response at the NICD. Here her responsibilities include oversight of the Outbreak Response Unit, Notifiable Medical Conditions and GERMS-SA surveillance. McCarthy lectures in the Wits School of Public Health.
Amongst the virus hunters interrogating the epidemiology [patterns and causes of disease] of Covid-19 is microbiologist Lynn Morris, a Research Professor in the School of Pathology at Wits and the Interim Executive Director of the NICD. Morris is internationally recognised for her work in understanding how the antibody response to HIV develops. A National Research Foundation A-rated scientist, she is amongst the most highly cited researchers in the world. Morris has a lifetime’s experience fighting viruses. She explains why COVID-19 presents one of the greatest challenges yet for South Africa and the world.
Understanding each other
A Distinguished Professor of Medical Anthropology and Public Health, Lenore Mandersonis internationally renown for her work in anthropology, social history and public health. She has played a leading role in training and research in inequality, social exclusion and marginality, the social determinants of infectious and chronic disease, gender and sexuality, immigration and ethnicity, in Australian, Asian and African settings.
The advent of COVID-19 prompted the Institute of Plumbing South Africa (IOPSA) to contact Wits for an expert to deliver a Q&A webinar for their members. Given the requirement of taps and plumbing for hand-washing, hygiene and sanitation against the virus, coupled with social distancing, quarantining and isolation protocols, plumbers were understandably concerned. Manderson participated in a 1.5-hour long Q&A session for IOPSA. Watch the PIRB Breakfast Tech Talk – Virus Q&Awebinar.
Associate ProfessorJo Veareyis the Director of the African Centre for Migration & Society at Wits and Director of the African Research Universities Alliance (ARUA) Centre of Excellence on Migration & Mobility. Given that the coronavirus spread originally via travelling, Vearey cautions against “hypocrisy in a time of Covid-19” and advocates that foreign migrants be included in the Covid-19 response. “The sanctimony of moving from blaming foreign migrants to now rendering them invisible in a critical public health moment will have implications for our response to Covid-19,” says Vearey.
In this podcast, Vearey discusses how South Africa’s impending winter, an historical HIV-AIDS pandemic, and xenophobic attitudes combine to generate surprising and unexpected responses to Covid-19.
Towards treatment
Professor of Vaccinology and paediatrician, Shabir Madhi is Director of the Medical Research Council Respiratory and Meningeal Pathogens Research Unit (RMPRU) at Wits. Madhi holds the NRF/SARChI Chair in Vaccine Preventable Diseases. His research has focused on the epidemiology and clinical development of lifesaving vaccines against pneumonia and diarrhoeal disease and has informed the WHO recommendations on the use of the lifesaving pneumococcal conjugate vaccine, rotavirus vaccine, and influenza vaccination of pregnant women.
Madhi is the immediate past Director of the NICD and former President of the World Society of Infectious Diseases. He has consulted to the WHO in the fields of vaccinology and pneumonia and to the Bill and Melinda Gates Foundation on pneumonia.
Watch Madhi explain how coronovirus enters the body. Read why pregnant women are not more prone to contracting COVID-19.
On the treatment front, Professor Helen Rees is Executive Director of the Wits Reproductive Health and HIV Institute (Wits RHI). She chairs the World Health Organization’s (WHO) African Regional Immunization Technical Advisory Group and she is Co-Chair of WHO’s Ebola Vaccine Working Group. South Africa is one of 10 countries involved in an urgent global trial, "Solidarity", announced by the WHO to identify the most effective treatment for coronavirus. Listen to Rees discuss South Africa's role in this global study.
Renowned HIV expert, ProfessorFrancois Venteris Director of Ezintsha and Deputy Executive Director of Wits RHI. With an active interest in public sector access to HIV services, medical ethics and human rights, Venter is attuned to the impact of COVID-19 on those with comorbidities such as HIV and TB. He is an advisor to the South African government, to the Southern African HIV Clinicians Society and to the WHO. Venter speaks from quarantine about the changing landscape of COVID-19 and the fundamental role that behaviour change plays in reducing infection.
Caring for the sick
Professor Feroza Motara is Academic Head of Emergency Medicine in the School of Clinical Medicine at Wits and at Charlotte Maxeke Johannesburg Academic Hospital - where the first COVID-19 patient in Gauteng was treated. Motara has since December 2019, when news of the virus broke, been preparing her team and the hospital to care for the ill. Read Motara’s comments about how healthcare workers on the frontline of the pandemic are coping. “We’re in the profession because there is that dedication and commitment. You still have to go to work and do what you need to do,” she says.
Big Data battle lines
Predicting and anticipating the trajectory of the virus to mitigate casualties and inform policy requires number-crunching, modelling, and analysis of Big Data. An interdisciplinary team of researchers at Wits this week launched the most comprehensive data dashboard to date on the COVID-19 virus in South Africa. Wits School of Physics Professor Bruce Mellado-Garcier, who initiated the project, says: “We are experts in analysing and interpreting big data, and we believe that it is important that someone put this data together and present a bigger picture of the impact of the virus on the country.”
Similarly, the Gauteng City-Region Observatory (GCRO) has developed an interactive map showing the province’s vulnerability to Covid-19. Dr Julia De Kadt, et al, devised this Map of the Month. The GCRO is a partnership between Wits University, the University of Johannesburg, and the Gauteng Provincial Government. Its mandate is building strategic intelligence through improved data, information, analysis and reflective evaluation, for better planning, management and co-operative government.
Expert commentary advancing policy
Professor Karen Hofman is Director of the SAMRC/Wits Centre for Health Economics and Decision Science (PRICELESS SA), a research-to-policy unit that provides evidence, methodologies and tools for effective decision-making in health. PRICELESS SA analyses how scarce resources can be used effectively, efficiently, and equitably to achieve better health outcomes. Some PRICELESS SA research has shown how fiscal, regulatory and legislative levers can improve health via social determinants.
Hofman, with Susan Goldstein, Deputy Director of PRICELESS SA, wrote one of the earliest articles advocating hand-washing, which has since become COVID-19 protocol.
Economist Prof. Imraan Valodia, Dean of the Faculty of Commerce, Law and Management at Wits, is currently coordinating an international study, in 10 cities, of the informal economy. His research interests include employment, the informal economy, gender, and industrialisation. He is a part-time member of the Competition Tribunal and a Commissioner on the Employment Conditions Commission and Chair of the National Minimum Wage Advisory Panel.
“The COVID-19 crisis is first and foremost a health and humanitarian crisis that we are all living through, which is likely to have lasting impacts on how we live. It is also likely to have a lasting impact, in the long term, on how we conduct our economic lives”, says Valodia. Read his analysis of the risks on economic inaction of COVID-19.
In the School of Governance, Adjunct Professor Alex Van Den Heever holds the Chair in Social Security Systems Administration and Management studies, which seeks to develop the field of social security postgraduate teaching and research in Africa and South Africa. Van Den Heever has worked in the areas of health economics and finance, public finance and social security. His research interests span healthcare management, healthcare quality, healthcare delivery, cost and economic analysis, health equity, health inequality and disparities, and preventive medicine. Read Van Den Heever’s analysis of the health and economic ramifications of COVID-19.
Innovating against infection
In the Faculty of Science, Head of the School of Molecular and Cell Biology, Prof. Marianne Cronje and her team took the initiative to synthesise virus-killing surface disinfectant and provided limited quantities of this disinfectant freely to University workers ahead of lockdown. The production plant has now been shifted to PIMD, while the school retains scientific oversight.
In the school’s Protein Structure Function Research Unit, Prof. Yasien Sayed coordinated the donation of 56 boxes of protective gloves to healthcare workers at the Chris Hani Baragwanath Hospital, after a Wits medical intern mentioned the shortage. Gloves and other PPE (personal protective equipment), such as masks, are critical to preventing infection.
Michael Lucas, a PhD candidate in the School of Mechanical Engineering has developed a revolutionary infection control solution. WATCH Lucas explain how his self-sanitising surface coating will help to address nosocomial [hospital-acquired] infections, as well as mitigate contamination of food processing plants and public transport surfaces. The Antimicrobial Coating Technology is now in its fifth year of development, with implications of preventing infection beyond COVID-19.
Adjunct Professor in Biomedical Engineering David M. Rubin leads the Biomedical Engineering Research Group in the School of Electrical and Information Engineering at Wits. Rubin and biomedical engineer and lecturer, Adam Pantanowitz are working on a model to show the effect of intermittent quarantines. It is currently very limited, but may have some benefit in terms of maintaining essential services and some continuity of economic activity. “At this stage, we’re only demonstrating the concept on standard viral epidemic models rather than a specific COVID-19 model,” cautions Rubin.
Official government regulations for #21DaysLockdownSA
- Government Communications Department
Government has released the early directives following President Cyril Ramaphosa’s address on Monday night.
The Department of Government Communications and Information System issued the following information on Tuesday, 24 March 2020, about the National Lockdown due to COVID-19:
A 21-day national lockdown has been declared:
The lockdown will begin on the evening of Thursday 26 March 2020 at 23:59. The lockdown will remain in force for 21 days. All South Africans will have to stay at home until midnight on Thursday 16 April 2020. The categories of people exempted from this lockdown are as follows:
• Health workers in the public and private sector, • Emergency personnel, • Security services – such as the police, traffic officers, military medical personnel, soldiers and, • Other persons necessary for our response to the pandemic.
It will also include those involved in the production, distribution and supply of food and basic goods, essential banking services, the maintenance of power, water and telecommunications services, laboratory services, and the provision of medical and hygiene products.
Will I be able to leave my house?
There is no need for panic, as lockdown does not mean a shutdown. People will still be allowed to get to shops and access essential goods and services but in small numbers. It is up to all of us to minimise our movement. Only undertake essential trips outside your home such as to get food, seek medical care or access supplies. When leaving your home try and go out alone, plan your trip and get in and out of your destination as quickly as possible. Practice hygiene when you go out, wash your hands when leaving home, do so again at your destination and before you depart for home.
What about homeless people and those who cannot self-quarantine?
Temporary shelters that meet the necessary hygiene standards will be identified for homeless people. Sites are also being identified for quarantine and self-isolation for people who cannot self-isolate at home.
We are all in this together
All sectors and citizens are working well together to fight the Coronavirus and we must continue to do so. Aggressive containment measures are essential to ensure that the virus does not spread any further. Please continue to exercise caution and avoid unnecessary travel. We call on everyone to cooperate with government and other sectors to implement the measures.
What services will remain open?
Most shops and businesses will be closed. The police, metro police, military and emergency services will continue to operate. Health care services such as hospitals, clinics, doctors, pharmacies and laboratories will remain open. Banks and essential financial and payment services, including the JSE will remain open. Supermarkets will remain open so that citizens can continue to care for themselves and their families. Petrol stations will remain open. Companies that are essential to the production and transportation of food, basic goods and medical supplies will remain open.
We are expanding efforts to contain the virus
This nationwide lockdown will be accompanied by a public health management programme which will significantly increase screening, testing, contact tracing and medical management. Community health teams will focus on expanding screening and testing where people live, focusing first on high density and high-risk areas. South African citizens and residents arriving from high-risk countries will automatically be placed under quarantine for 14 days. Non-South Africans arriving on flights from high-risk countries will be turned back. International flights to Lanseria Airport will be temporarily suspended. International travellers who arrived in South Africa after 9 March 2020 from high-risk countries will be confined to their hotels until they have completed a 14-day period of quarantine.
A number of economic interventions are being put in place
We have set up a Solidarity Fund, which South African businesses, organisations and individuals, and members of the international community, can contribute to. The Fund will focus efforts to combat the spread of the virus, help us to track the spread, care for those who are ill and support those whose lives are disrupted. The Fund has a website – www.solidarityfund.co.za – and contributions can be deposited via the fund. The Fund will be administered by a reputable team of people, drawn from financial institutions, accounting firms and government. To get things moving, government is providing seed capital of R150 million and the private sector has already pledged to support this fund with financial contributions. We will be spending money to save lives and to support the economy. We must applaud the commitment made in this time of crisis by the Rupert and Oppenheimer families of R1 billion each to assist small businesses and their employees affected by the coronavirus pandemic.
We are assisting businesses
We will be assisting businesses in the informal sector such as spaza shops. Registration is now open, on www.smmesa.gov.za, for small and medium-sized businesses that require help during the coronavirus crisis. The department of Small Business Development has a debt-relief fund for small businesses. Small businesses affected by the outbreak of the coronavirus will be required to produce proof of negative impact as a result of COVID-19. We will further be assisting small businesses to avert job losses through the Small Enterprise Development Agency (SEDA). Government has urged malls and retailers to consider rent and payment holidays to tenants negatively affected by the lockdown.
There is no need to stockpile food
Government calls on everyone in the country to avoid panic buying. We are aware that many South Africans are worried about the impact of the coronavirus on essential supplies and food in the country. As government, we are doing everything we can to ensure that we have enough food and all essentials we need. Government has had discussions with manufacturers and distributors of basic necessities, who have indicated that there will be a continuous supply of these goods. Let us be considerate and responsible to ensure that we have enough for everyone especially the most vulnerable in our society.
Our social safety net remains in place
All grants will continue to be paid. To alleviate congestion at payment points, old age pensions and disability grants will be available for collection from 30 and 31 March 2020, while other categories of grants will be available for collection from 01 April 2020. All channels for access will remain open, including ATMs, retail point of sale devices, Post Offices and cash pay points.
Let us stand and face this together
The actions we are taking will challenge us as a nation. But we are convinced that the cost of not acting now would be far greater. In the days, weeks and months ahead our resolve, our resourcefulness and our unity as a nation will be tested as never before. Let us all play our part and ensure that we emerge stronger and more united.
You are not alone!
It is important that you stay connected via the phone, social media or email. Maintain your networks and speak to friends or family regularly. Keep doing enjoyable and relaxing activities such as reading, pc, board or card games, social networking or watching television. Stay informed by getting the facts, not rumours or fake news. Engage children in your care in creative ways; create fun learning activities, play games and try to keep their daily routine going. Stay active by doing simple exercises within your home or garden. Or create an exercise plan specifically to suit your environment.
Coronavirus: how big, how bad, and what to look out for
- Shabir Madhi
Cases of illness from the new coronavirus (SARS-CoV-2) disease, known as COVID-19, have been confirmed in more than 100 countries.
Coronaviruses are a family of viruses that cause illnesses that can range from a common cold to more severe diseases such as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS). The Conversation Africa’s Ina Skosana spoke to Shabir Madhi about the situation.
What percentage of people who get the virus are dying from it? Is this high compared with other infectious diseases?
There’s no straightforward answer to this question because the epidemic is still at an early stage. It all depends on what the denominator is, which influences the case fatality risk. And we’re still working with unknowns.
The current estimate is that between 1% and 3% of people diagnosed with COVID-19 die. The problem with this estimate is that the starting point is when individuals have become ill, rather than when they were infected. The actual number of people who are infected might be much higher than the actual number of cases that are presenting for medical care.
The implications of this are huge. For example, if the number of people who have been infected but haven’t gone on to develop the disease is high it would mean that the case fatality risk would go down.
The numbers in Iran point to further difficulties with calculating the fatality rate. Initial reports from Iran indicated a case fatality of 10%. This seems very unlikely. This indicates that a large number of cases were going undetected and possibly that mainly very severe cases were being investigated. When investigating very severe cases the case fatality risk is going to be higher.
A 1% fatality risk is moderate and is in the ballpark of other viruses such as respiratory syncytial virus associated with hospitalisation in children. It is, however, lower than the case fatality risk was for the coronavirus strains that caused the SARS epidemic in 2002 – which was 10% – and for MERS in 2013, which was about 35%.
Nevertheless, based on current knowledge, the case fatality risk for COVID-19 is higher than observed for seasonal influenza virus, which has a fatality risk of about 0.1%. Annually, seasonal influenza virus is estimated to cause up to 290,000 deaths globally. Currently, the global number of deaths due to COVID-19 is approximately 4,100.
Is the reaction overblown?
No. It’s warranted. This is because we don’t know how this epidemic is going to pan out. So even if the case fatality risk is very low, if a high percentage of a population becomes infected that low fatality risk could result in a large number of deaths. For example, if an epidemic involves 100 people with a case fatality risk of 10%, 10 people will die. But if an epidemic infects a million people with a case fatality risk of 1%, there will be 10,000 people dying.
The case fatality risk needs to be interpreted in the context of the number of individuals who are going to become infected to be able to understand the total impact of the epidemic. And right now we don’t know what percentage of the different populations will become infected.
Who is most vulnerable to dying from infection?
Current experience – which is largely driven by what has come out of China and more recently from Iran and Italy – is that people over the age of 50 seem to be more susceptible, particularly if they have underlying medical conditions or co-morbid conditions. These include cardiac problems (case fatality risk 10%), diabetes and lung disease (case fatality risk of 7%). People over the age of 70 have a case fatality risk of 14%.
The big unknown for Africa, particularly countries like South Africa, is what the impact will be on populations with a high prevalence of HIV and TB.
The epidemic has only broken out in countries with very low HIV prevalence, so we don’t know to what extent individuals living with HIV might have an increased susceptibility to severe disease. This is true of TB too. Because TB affects people’s lungs it means that people with the disease have a low tolerance threshold for an additional assault.
In the context of HIV, we have shown that even in the era of antiretroviral treatment, individuals with HIV still have a 10-fold greater susceptibility to severe influenza illness than the general population, and a higher case fatality risk. We expect there may be differences in susceptibility and outcomes for COVID-19 cases in settings such as South Africa.
What are the symptoms that should get me worried?
The symptoms are very non-specific and very similar to other viral infections like the influenza virus. Unfortunately there isn’t a particular trigger that’s different to any of the other viruses.
But people can be mindful of a few things. For example, their travel history to a place where the virus is circulating. Or whether the person has come into contact with someone who has visited one of the places where the virus has been shown to be circulating.
Of course this isn’t definitive.
The classical signs and symptoms one can look out for include a fever, cough, headache and myalgia (muscle pain). Again these are very non-descript.
What treatment is available?
Currently there’s no specific antiviral treatment to cure SARS-CoV-2 infection. Besides supportive care, no therapeutic agent has been proven to be effective in treating or improving the outcome of COVID-19 cases. There are clinical trials under way and others are being planned to evaluate different antiviral agents and other possible therapeutic options. The biggest concerns are about a more severe disease, where patients may end up with pulmonary damage which requires supportive care including supplemental oxygen and then might have to be put on to ventilator. Current estimates are that 15% of COVID-19 cases result in severe disease.
Most low- to middle-income settings have fragile health care systems that lack resilience against external shocks such as the demands posed by unexpected epidemics. These countries may lack the capacity to scale up curative services over a relatively short period of time. Such a scale-up of curative services was undertaken in Wuhan to complement existing curative services.
But a quick-fix solution to address an increase in demand for curative health-care services is unlikely in most African countries should SARS-CoV-2 start circulating widely on the continent. This is a culmination of the systematic lack of investment in health care in most countries. It’s not something that can be rapidly fixed in the middle of a pandemic.
Wits PhD student develops novel infection control solution
- Wits University
New self-sanitising surface coating will help to address infection control in hospitals, food processing plants and public transport surfaces.
The Antimicrobial Coating Technology by PhD student Michael Lucas, now in its fifth year of development, is a novel solution to address the problem of nosocomial infections. These infections, acquired during hospital stays, are a significant and persistent issue faced by hospitals across the world.
“Infection control is an ongoing challenge in hospitals. Surface contamination and subsequent microbial transmission are known contributors to this. My design for a self sanitizing surface coating serves to address this growing problem, and the results are very promising. These antimicrobial coatings can be applied to high contact surfaces where there is a risk of contamination, including medical facilities, food processing plants and public transport surfaces,” says Lucas.
Metal coated plastics are an emerging field of research and development with a wide range of applications. The distinguishing features of Lucas' research include the novelty of multi-step and multi-process additive manufacturing through the use of cold spray and polymer 3D printing. These manufacturing techniques offer design freedom and manufacturing versatility. This means that manufactured parts can be retrofitted into existing hospital surfaces.
The coatings are made up of various metals with known antimicrobial properties, including combinations of copper, silver and zinc. The uniqueness of Lucas' innovative way of depositing the coatings is a competitive advantage that Wits University is protecting through a patent.
“Research is a process of exploration and it's this aspect that appeals most to me. I enjoy problem solving and seeing the application of research,” says Lucas, who won the prestigious Prix Hubert Tuor Innovation Award for his technology last year.
The most promising particle-embedded cold spray polymer metallised coatings were found to be effective self-sanitising surface coatings. Under simulated touch-contact conditions copper coatings on various polymer substrates, for example, repeatedly achieved complete microbial elimination within only a 15 minute contact period. These tests were conducted under laboratory conditions against a variety of dangerous pathogens that are found in hospital high contact surfaces including a multi-drug resistant Staph strain. Thus, the potential of these coatings for the mitigation of surface contact transmission of infections was confirmed.
Preliminary pilot studies validated this, using coated security access cards and a custom coated smartphone cover exposed to various healthcare associated environments within the University of Witwatersrand’s Medical School and adjacent Charlotte Maxeke Academic Hospital.“The next steps include verifying the safety of the coatings for the intended application and to assess the coatings’ efficacy in real world hospital high contact surface environments. This would be the start of taking the technology to market,” says Michael, adding that he sees an opportunity to turn his technology into a viable startup business.
The development of the technology is ongoing, having started during Lucas' undergraduate research project and continuing into his doctoral studies. Together with the now late Professor Ionel Botef from the Schoo l of Mechanical, Industrial and Aeronautical Engineering, Lucas has worked on further developments with Professor Sandy van Vuuren in the Wits Pharmacy and Pharmacology department. Financial assistance has been provided by the DST-NRF Centre of Excellence in Strong Materials (CoE-SM) and SITA Information Networking Computing UK.
The development of the technology is ongoing, having started during Lucas' undergraduate research project and continuing into his doctoral studies. Together with the now late Professor Ionel Botef from the Schoo l of Mechanical, Industrial and Aeronautical Engineering, Lucas has worked on further developments with Professor Sandy van Vuuren in the Wits Pharmacy and Pharmacology department. Financial assistance has been provided by the DST-NRF Centre of Excellence in Strong Materials (CoE-SM) and SITA Information Networking Computing UK.
Lucas graduated with a Bachelor of Science in Engineering (Mechanical Engineering) from Wits in 2016. Before graduating, he was asked to present his undergrad research into biomaterials via cold spray and 3D printed polymers at the 2015 Mechanical, Industrial and Aeronautical Engineering (MIA) annual valediction. He was subsequently awarded the best presentation in the Mechanical Engineering programme by the South African Institution of Mechanical Engineers (SAIMechE). Due to the novelty and sophistication of the development, his master's in Engineering was upgraded to a PhD research study under the title: Antimicrobial surface coatings via cold spray and 3D printing technologies, which he is currently completing at Wits University.
Wits acts to manage Covid-19 exposure
- Wits University
Wits acts swiftly to manage student who came in contact with COVID-19 carrier.
The Wits COVID-19 management committee would like to advise the Wits community that a medical student has been quarantined after it was found that the student came into contact with a person who had been identified with COVID-19.
The student is being monitored closely and has not displayed any symptoms of COVID-19. The student has been screened and the test results are expected later today. However, as a precautionary measure the Faculty has cancelled the clinical activities scheduled for the student’s class today. All other activities continue as scheduled.
Further information will be made available when it becomes available.
Wits COVID-19 Management Committee
13 March 2020
Student tests positive for Covid-19 and Wits reaches out to affected class
- Wits University
Wits University has just been informed that the medical student who has been quarantined since last Wednesday has tested positive for the coronavirus (COVID-19)
The student was asymptomatic and attended classes last Monday and Tuesday, without knowledge that the student had contracted the virus.
In light of this, the University has made the following immediate decisions:
The cancellation of all contact classes for the Graduate Entry Medical Programme 1 - MBBCh 3 classes. The academic programme will continue online.
All students in the affected student’s class have been instructed to go into self-quarantine for 14 days with immediate effect.
The Faculty is personally reaching out to each of the 350 students who could be affected. They will receive the full support of the Faculty, including the requisite monitoring and testing.
The Dean of Students, Mr Jerome September will coordinate arrangements for students who live in residences, and who require self-isolation. All students who require assistance should contact Thembelihle Dlamini on 0728390223. Those who require counselling can call the 24 hour Wits student support number on 0800 111 331.
The Department of Health’s WhatsApp number is 0600123456 and provides additional information about COVID19. The NICD website (www.nicd.ac.za) is a credible source of information on COVID-19.
The Wits Senior Executive Team is meeting this afternoon to decide on the way forward for the Faculty and all other University activities. An update will follow this evening. In the interim, we appeal to the Wits community to remain calm. Please be assured that we are managing this issue and making decisions based on the best medical advice available.
This is an anxiety causing time for the University community and the country as a whole. However, if we all take a pragmatic approach to this pandemic it is very likely that the country will get through this crisis. Importantly, it is everybody’s responsibility to protect themselves so that we also protect all other South Africans and most importantly the most vulnerable in our society.
We will get through this difficult period together.
SENIOR EXECUTIVE TEAM
WITS UNIVERSITY
15 MARCH 2015 (13:30)
All contact teaching postponed for Monday, staff to continue with work
- Wits University
Wits announces measures to curb the spread of COVID-19.
The Senior Executive Team of the University of the Witwatersrand met on Sunday, 15 March 2020, and made the following decisions:
All contact teaching and University activities involving face to face interaction are postponed, including tests, for Monday, 16 March 2020. All students are requested to remain at home or to confine themselves to their rooms in residence. Students are encouraged to follow the social distancing policy and to limit interaction where this is possible.
Special arrangements are being made for students who usually eat in dining halls.
Employees are expected to come to work in order to ensure that operations continue. Employees are requested to maintain social distance, and where possible meetings and group work should be conducted telephonically, online, or via video conferencing. We continue to follow the NICD’s protocols in this regard.
All graduations will be postponed until further notice. New arrangements will be communicated in due course.
A temporary moratorium has been placed on all travel, both outbound and inbound, and applies to both local and international travel. This also means that people who have travelled into South Africa, should not be allowed to enter the University.
Remember to also make use of the NICD’s Coronavirus Emergency 24-hour hotline number and to visit the NICD’s website at www.nicd.ac.za if required. For those who are tested at independent laboratories, remember that these are preliminary results. All positive results must be verified by the NICD.
We will keep the Wits community informed as to plans from Tuesday onwards after consultation with the Department of Health and the Department of Higher Education and Training. In the interim, student queries should be directed to the Dean of Students via Jerome.September@wits.ac.za whilst employees with queries should email their line manager, Head of School or respective Senior Executive Team member.
Thank you
SENIOR EXECUTIVE TEAM
15 MARCH 2020 (20:00)
Wits announces early recess
- Wits University
Wits University will be in recess from Tuesday, 17 March 2020, four days earlier than scheduled.
Following meetings with the NICD, experts in infectious diseases and designated government departments, it has been determined that the University is currently in a low-risk moment and that taking the appropriate decisions now may enable the moderation of staff and student exposure to COVID-19.
As a result, the Senior Executive Team has made the following decisions:
The mid-term break will be brought forward and the University will be in recess from Tuesday, 17 March 2020, four days earlier than scheduled. This means that all academic activities for this week will be rescheduled.
Wits will reopen on 30 March 2020 as per the almanac, but this date and the form of the academic programme may change, depending on national and global developments around the containment of the health pandemic.
After consulting with key health experts, the executive has taken the difficult decision to request all students to vacate their residences within the next 72 hours. We are deeply cognisant that students may have some concerns and challenges around this decision but we believe that we are acting in the best interests of students and the broader public. Minimising exposure in the institution extends beyond face to face contact within the academic programme but also in our residences, especially at this relatively early stage of the pandemic. The Dean of Student Affairs and his team will steward this process and will be available to attend to any challenges that students (including international students) may experience.
The University will continue to operate on essential and skeleton staff during this period. Over the next 72 hours, managers and executives will consult with staff in their departments to put in place arrangements for essential services to continue up until 30 March 2020. All executives, managers and essential staff will be required to ensure the continuity of operations during this time.
In addition, academic staff may work from home but are allowed to come onto the Wits campuses as appropriate or if required, to ensure the long-term continuity of the academic programme.
Non-essential professional and administrative staff may remain at home unless they are required to report for duty. Matters related to leave and working conditions during this period will be addressed by our Finance, Human Resources and Legal Divisions in consultation with unions and other stakeholders.
[WATCH] Wits Vice-Chancellor Professor Adam Habib announces early recess
As stated yesterday, all graduation ceremonies will be postponed until further notice and more information will be sent to graduands in due course.
South Africa, and the higher education sector has never before confronted a pandemic on this scale. If we are to get through this period with the minimum impact on society, the Wits community and the academic programme, it will require an unprecedented solidarity from all stakeholders. This in principle means that we all need to reflect on how we can contribute to our institution, our country and the collective good of our communities during this time of crisis.
We are in a crucial moment in the life of this pandemic and it is important that we work as a collective for the benefit of our society. We urge all members of the Wits community to heed the words of President Cyril Ramaphosa: “This epidemic will pass. But it is up to us to determine how long it will last, how damaging it will be, and how long it will take for our economy and our country to recover. It is true that we are facing a grave emergency. But if we act together, if we act now, and if we act decisively, we will overcome it.”
Thank you
SENIOR EXECUTIVE TEAM
16 MARCH 2020 (20:00)
Who should test for COVID-19
- Wits University
Answers to common questions asked by the Wits community.
Dear Colleagues and Students
We have been inundated with requests from students and staff who are concerned about their health and who are requesting to be tested for COVID-19. Here are some answers to the common questions.
Who should be tested for COVID-19?
Persons who may have the following symptoms:
Fever + a cough OR
Fever + shortness of breath
AND
who may have returned from a high-risk country in the last 14 days
AND
who may have been in close face-to-face contact (within 2 metres) in a closed environment for an extended period of time with a confirmed or probable COVID-19 positive person.
[WATCH] World Health Organization explains who is at risk
Persons who have been in the same enclosed vicinity of a confirmed or probable COVID-19 positive person for an extended period of time should self-quarantine isolate for a period of 14 days. If symptoms develop during this period, they should call ahead and visit a healthcare professional, and follow their advice. These persons may require testing at this time.
People who may walk through the same corridor as someone who has tested positive for COVID-19 or a large classroom are at low risk and should monitor their health carefully. They do not require testing.
How is COVID-19 diagnosed?
Where can I get tested?
COVID-19 is diagnosed by a laboratory test known as the polymerase chain reaction (PCR) molecular test on a respiratory tract sample (e.g. sample from nose, throat or chest).
If you have no symptoms, self-monitor. If symptoms develop, go into self-isolation and then call ahead and visit your healthcare professional, and take their advice. They will refer you to a laboratory to be tested if required.
Where are the high risk countries?
Do all Wits students need to be tested?
Do students need to be tested before leaving residences?
A. No. Only those students who meet the criteria above. All students who may have been at risk have already been identified and placed into self-quarantine. This group is being monitored and is receiving the support of the Faculty of Health Sciences and the Office of the Dean of Students Affairs.
A. No. Students do not need to be tested before leaving residences.
No. Experts in infectious diseases have advised that the University is currently in a low-risk moment and that taking the appropriate decisions now may enable the moderation of staff and student exposure to COVID-19 as we are still in the early stages of the pandemic. We believe that we are acting in the best interests of students and the broader public by bringing the mid-term break forward.
A. Students, call the ICAS hotline on 0800 111 331
Staff, call the AskNelson Hotline on 0861 635 766 or dial *134*928# or send a ‘please call me’ to 072 620 5699 or email asknelson@kaelo.co.za
SENIOR EXECUTIVE TEAM
17 MARCH 2020 (15:00)
Wits COVID-19 Update 13: Students urged to go home
- Wits University
Message from the Wits Dean of Student Affairs.
Dear Students
We are living through a difficult time and we are doing all that we can to ensure the safety of our students, based on the advice that we are receiving from experts.
We would like to thank those students who have vacated their residences, in line with the call made by the University and the directive of the President, the World Health Organization and other experts.
Following this morning’s court order, which implored all students to follow the directives referred to above, the majority of students have now left our residences. We urge those who remain to vacate as soon as possible. Many have arranged to leave overnight and those with special challenges are being assessed on a case by case basis. Those who have requested assistance (including international students) from my Office will be advised in the next few hours as to the nature of the assistance that the University can provide.
In light of the steady rise in the number of people infected with COVID-19, the University urges all remaining students to leave immediately. This is in the best interests of the student body, the University community and the general public. Please note that all catering, cleaning, ICT and other services will be suspended as from tomorrow morning.
We have received many queries from students who are concerned about the submission deadlines for their academic work. The SET has agreed that these deadlines will be extended into April and that new deadlines will be communicated in due course.
We wish all students a safe journey home.
Mr Jerome September
Dean: Student Affairs
Wits COVID-19 Update (15): Wits prepares to go online
- Wits University
Wits from the Senior Executive Team of Wits University.
Dear Colleagues and Students
This is an uncertain time for all of us – staff, students, members of the Wits community, and society. The sands are shifting daily and many of us are feeling anxious about what happens next – to our health and safety, livelihood, to our education, to our research, to our freedoms and to life as we know it.
Whilst we practice physical distance and social solidarity, this disruption also provides us with an opportunity to reimagine how we live, how we work and how we learn. It also allows us to exercise control over the aspects that we can change – and in this instance, how we can learn and work remotely.
Given the potential of a lockdown and uncertainty around movement in the months ahead, after a deliberative meeting (via Microsoft Teams) this morning, we agreed that:
all faculties must prepare to take the academic programme online within the next two weeks (with the full support of the Centre for Learning, Teaching and Development and the Wits ICT teams),
all Deans (with the input of Heads of Schools and academics) will maintain a spreadsheet that will determine how programmes can be transitioned to a remote format,
students will have to prepare to work online, and
the precise date on which the University will reopen and the format in which the academic programme will commence, is still to be determined.
Some of the issues that were discussed are reflected below, including:
the digital divide and how to mitigate against deepening this divide,
a database analysis indicates that only about 25 out of Wits’ 38 000 students do not have a mobile phone,
access to smart mobile devices (a quick survey has determined that about 90% of first year students have access to a smart mobile device) and Deans and faculty will look for practical solutions for the remaining students,
access to data (the University has secured zero rated sites from MTN, Telkom and Vodacom, which means that staff and students can access these sites at no cost), and
the anxiety of some staff members who are used to contact teaching and who have not been exposed to online learning systems or software (it was agreed that CLTD and Wits ICT would talk academics through these aspects).
We are still deliberating on a number of issues including the minimum requirements for online and distance learning and teaching (infrastructure, data, content modification) and the potential for introducing alternative assessments where applicable. A plan which details the form in which online teaching will take place will be shared in the coming days, in consultation with staff in the faculties.
Please send all your questions, suggestions and concerns to vco.news@wits.ac.za.
In the meanwhile, please keep calm, keep safe, and look out for our latest updates at www.wits.ac.za/covid19. We can overcome this global challenge together.
Thank you
SENIOR EXECUTIVE TEAM
23 MARCH 2020 (18:00)
Wits researchers launch most comprehensive COVID-19 dashboard in South Africa
- Wits University
The dashboard is aimed at informing government, scientists, the media and general public with quick, easy-to-understand information on the current situation.
An interdisciplinary team of researchers at Wits University has launched the most comprehensive data dashboard on the COVID-19 virus in South Africa to date.
The dashboard, that shows the latest statistics on how the virus is affecting the population of South Africa, is updated on a daily basis, using official statistics from both local sources, such as the National Institute for Communicable Diseases (NICD) and international sources such as the World Health Organisation (WHO). The statistics on aspects such as the cumulative confirmed cases in South Africa, the daily confirmed cases, relative increases of infections are presented in colourful, easy-to-interpret visualisations. Other statistics include infections by gender, province, age and transmission routes.
“We are experts in analysing and interpreting big data, and we believe that it is important that someone put this data together and present a bigger picture of the impact of the virus on the country,” says Professor Bruce Mellado from the Wits School of Physics, who initiated the project. The team working on the project includes computer and data analysts, engineers and physicists.
The dashboard is aimed at informing government, scientists, the media and the general public with quick, easy-to-understand information on the current situation. It is updated every day approximately an hour after the release of the official COVID-19 update from the NICD. As more data becomes available, more features will be added to the dashboard.
Mellado is in talks with several government departments to get them to recognise as well as to add to the database, in order to make it a powerful tool in the fight against the virus.
“Our team believes in the power of knowledge to solve complex issues, and we hope that our strong ties and cooperation between the scientific community, the executive and the public can help overcome challenges such as the COVID-19 pandemic,” says Mellado.
Wits engineers make face shields to protect healthcare workers
- Wits University
A team of innovative Witsies is using their design and engineering skills to create face shields in aid of the fight against COVID-19.
An amazing sense of social solidarity and patriotism has pervaded South Africa recently with many people offering their knowledge and skills to aid the country in its fight against the coronavirus.
The escalating spread of the virus has increased the demand for personal protective equipment (PPE) and medical supplies as more people test positive for COVID-19 daily. Healthcare facilities in the country are seeing a shortage in these supplies for their staff.
On Friday, 27 March 2020, Netcare 911, one of the healthcare facilities currently experiencing a massive shortage of protective gear, called on the 3D printing community to assist with printing head rings for face shields for use by medical staff treating patients with COVID-19.
Teams at Wits from the Digital Incubator at the Tshimologong Precinct, the School of Mechanical, Industrial and Aeronautical Engineering (MIA) along with the Transnet Centre of Systems Engineering (TCSE) and the Transnet Matlafatšo Centre (TMC) heeded the call and used their engineering prowess to assist with a solution to the problem.
Recognising that each head ring for the face shields would take approximately 90 minutes to produce and with limited 3D printing capacity, a team – made up of Guy Richards, Letlotlo Phohole, Moses Mogotlane, Palesa Riba and Randall Paton, ,decided on a laser cut solution that would save time.
“Netcare was going to provide the actual shield and clips to put it together. We were not happy with the limitation and wanted to use what is readily available to us, cheap to make, and light-weight. Most of all, we wanted to produce a complete product. We also anticipated long printing times with a 3D printer and possible filament shortages given the national drive for face shields and masks,” said Letlotlo Phohole, Acting Director of TCSE and TMC.
After numerous attempts on Monday, 30 March to cut the shield from downloaded files from GitHub and Thingiverse – a software development platform where over 40 million developers collaborate online to host and review code, manage projects, and build software – the Wits team re-designed the original designs, applying rapid prototyping processes, which they then cut using their laser cutter.
The face shields, which are made from polyvinyl chloride (PVC) sheeting, are a flat pack consisting of two pieces that can be rapidly assembled. “The School had stock of the PVC sheeting from another earlier project. The shields are therefore being provided at no cost to the hospitals”, says Paton.
Adhering to best safety practices is crucial in the production of these face shields.
“We ensure that after production they [face shields] are washed, rinsed, and dried to remove any potentially harmful residue from the laser cutting. This is done in a production line fashion and is now the tightest bottleneck in the project, given that we only have one working laser cutter,” added Paton.
With an average production time of 3 minutes (including setup time) to cut a set of pieces for each face shield, the team anticipates making 200 to 500 shields a day to help meet the growing demand of protective gear for medical staff.
“We have developed a system that lets us feed the rolled plastic directly into the cutting bed and draw more through when done so speed is climbing,” said Paton. The team has reduced the cutting time to 90 second per shield but the washing and drying still add to that time.
Four days since the call from Netcare 911, by Tuesday, 31 March, the Wits team had produced 140 face shields and distributed 120 to the Wits Donald Gordon Medical Centre and another 20 to the Wits Protection Services staff. An additional 300 face shields have been produced to date, of which 200 will be donated to Charlotte Maxeke Johannesburg Academic Hospital and 100 to Rahima Moosa Mother and Child Hospital. The Wits engineers hope to distribute face shields to Helen Joseph and Chris Hani Baragwanath hospitals, which are also Wits teaching hospitals.
Head of MIA, Professor Robert Reid hailed the team for their extraordinary contribution to society saying that they are upholding one of the five core values of the School, botho (humanity).
“A core value of our School is botho. We strive to nurture and develop the community of which we are part. During this time of national crisis, it is imperative that we use our skills and facilities in any way that will serve our community. I am therefore delighted that we are able to help keep safe the healthcare workers on the frontline in their fight against this awful pandemic.”
Paton said the nationwide response to the call had inspired him.
“I think that many South Africans, as a nation of ‘make-a-plan’, are frustrated by not being able to help in a tangible way during the lockdown and this has channelled that energy somewhere. This has been as inspiring to be a part of as watching everyone trying to help Netcare with 3D printing for the face shields. These are extraordinary people in extraordinary times.”
The Faculty of Engineering and the Built Environment plans to develop other medical equipment, including respirators, devices to prevent people from touching their faces, and medical masks (with filters made out of vacuum cleaner bags and make-up cotton pads designed by students of their own volition). These cross-disciplinary projects will involve people from different faculties at Wits and other stakeholder groups.
Over R100 000 has been raised for this initiative from 68 donors. If you would like to make a tax-deductible donation towards this cause or other initiatives at Wits University against COVID-19, please follow https://wits.devman.co.za/devman/covid-19/giving/ and donate directly to the Wits Covid-19 Discretionary Fund or donate to the Wits Foundation. Bank details:
Wits University Foundation Standard Bank of South Africa Ltd Current Account number: 002900076 Branch code: 00 48 05
New features added as inter disciplinary and inter-institutional collaboration data on the pandemic grows.
Wits University’s COVID-19 South Africa Dashboard has grown with new data features, including snapshot views of how the pandemic is spreading in Africa, as well as statistics showing world trends, being added. (As featured in this article in TIME Magazine.)
The dashboard, launched on 22 March, by Professor Bruce Mellado from the Wits School of Physics and Senior Scientist at iThemba LABS, has gained momentum with a number of volunteers from different disciplines working 24/7 to develop and maintain the dashboard. Wits university is working in collaboration with iThemba LABS of the National Research Foundation.
The visualisation of large quantities of data on the pandemic is a critical step in the analysis of that data. It provides an essential input for analysts to develop the first intuition with which to devise models. The relevance of the visualisation that the dashboard provides is therefore significant.
“The design, development and updating of the dashboard requires a large collaborative effort,” says Professor Barry Dwolatzky, Director of Wits University’s Joburg Centre for Software Engineering (JCSE). “I am assisting in the coordination of the project. Under Bruce Mellado’s leadership a team of highly dedicated and motivated student volunteers, drawn from a variety of disciplines, is working to develop and maintain the dashboard. Although all of us are locked down and working from home, a strong team spirit has developed. I find it interesting that few of us have actually met."
The dashboard is maintained daily and updated within minutes of Government’s announcements on the latest statistics. It provides historical data of relevant parameters, provincial and other breakdowns and it has undergone a number of upgrades since its release.
“Many of the upgrades have been requested by scientists and journalists from all over the country to improve the presentation of the South African data. Currently the site averages about 10 thousand views a day,” says Mellado.
One of the upgrades performed on the dashboard is the addition of a dashboard for the African continent that includes a detailed account of total cases, mortality and recoveries for all African counties. This addition has triggered a collaboration with the Botswana International University of Science and Technology (BIUST) to develop the first COVID-19 dashboard for Botswana, using data from the National Emergency Operation Centre of Botswana.
“This adds a new and important dimension to our existing collaborations with Wits and iThemba LABS,” says Professor Gregory Hillhouse, Head of the Department of Physics and Astronomy at BIUST.
“It is gratifying to see that one of our MSc students who has been trained at iThemba LABS, Mr Otsile Tikologo, is actively involved with this project.”
Another upgrade illustrates the global analysis of the spread in the conditions of containment (or “lockdown”) using epidemiological models. A number of countries have been selected for which containment measures have led to significant reduction in the rate of spread.
Data analysis and statistical treatment of this feature are performed using a frequentist framework. For this purpose the data processing framework ROOT developed by the European Laboratory CERN is used. Results are presented in terms of lower and upper curves for the cumulative number of positive cases as a function of time. These are estimated on the basis of a 68% confidence level. Predictions are updated on a daily basis.
“Understanding the impact of containment measures on the spread of the virus is essential to managing this crisis. Global data provide an invaluable insight into the dynamics of this complex problem,” says Mellado.
There is a dire need to boost SA’s stimulus package
- William Gumede
Countries such as the US, Germany, India and Brazil have launched help for all sectors of their economies — South Africa needs to follow.
To prevent Covid-19 from destroying their economies many dynamic countries have introduced large emergency economic stimulus packages that comprise significant proportions of their countries' GDPs. These combine monetary and fiscal measures, prioritising injecting cash into the wider economy, rescuing vulnerable businesses, supporting self-employed individuals and providing support to the unemployed.
Many countries rightly see the Covid-19 peril as similar to a war situation, which demands extraordinary measures not usually used in peace-time. Some countries are funding their stimuluses packages through debt, setting aside existing fiscal and monetary restrictions or using reserves kept for emergencies.
Singapore unleashed a stimulus package of almost $55bn, or 11% of the country’s GDP, to prevent it from plunging into recession because of Covid-19. It widened the country’s budget deficit to 7.9% from a previous target of 2.1%, and drew as much as $17bnfrom reserves. The Singapore Monetary Authority manages monetary policy through tuning the exchange rate, letting the local currency fall or rise against the currencies of its main trading partners, rather than adjusting interest rates. As part of the stimulus package the authority eased the exchange rate in the most aggressive way since the 2008/2009 global financial crisis, by adopting a zero percent annual appreciation rate.
The Singapore stimulus included scrapping property taxes for hotels, restaurants and shops; wage support for businesses, particularly in most vulnerable sectors such as aviation, food services and tourism. It also provided direct cash to the self-employed, including freelancers, lower-income workers and the unemployed. It provided funding to civil society and community organisations and charities involved in community help. Grocery vouchers were given to the needy. Housing loan payments were deferred for up to six months.
South Korea released an economic stimulus package of $13.7bn, just under 1% of the country’s GDP. Part of this will be financed by a combination of reprioritising fiscal resources, debt and treasury bonds to be issued later this year. The Bank of Korea slashed interest rates by 50 basis points. The bulk of the emergency stimulus is aimed at strengthening the public health system, SMMEs and subsidising the wages of struggling companies. It relaxed loans for all exporters. Those who have lost their jobs will be retrained. The government provided childcare subsidies over the lockdown and made cash payments of $816 to each family except the richest 30%. SMMEs are exempt from certain taxes and utility bills over the lockdown period.
Brazil has unleashed a $29bn stimulus package, about 5% of GDP. The stimulus is based on reprioritising existing fiscal resources. The government has refashioned current monetary, fiscal and budget policies to tackle the Covid-19 emergency. It deferred company taxes and allowed employees to make withdrawals from their Employee Indemnity Guarantee Fund, to which all employees have to contribute 8% of their salary. Companies have been allowed to postpone their contributions to the fund for up to three months. The government also lifted import tariffs on medical products and gave tax exemptions to locally produced medical products.
Private banks agreed to extend the maturity dates for personal, household and SMME loans by two months. Banks were asked to renegotiate easier terms of existing loans of struggling companies without charging extra. The Brazil central bank cut interest rates by 50 basis points and repurchased dollar-denominated sovereign bonds to stabilise financial markets. It eased the capital requirements for banks, to make funds available for them to lend during the crisis. The government lifted its fiscal target to free up financial resources. Those who are self-employed, in informal employment or unemployment will get a basic income grant of $125 a month for three months.
India unveiled a $22bn stimulus package or 1% of GDP, and an additional $2bn to support the public health system. The Reserve Bank of India cut interest rates by 75 basis points to 4.4%. It also cut the case reserve ration, the amount lenders must hold in reserve, by 100 basis points to increase liquidity in the economy. It put a three-month moratorium on loan repayments by banks and informal lenders. The government will deliver 5kg of grains and 1kg of lentil rations monthly to 800-million people, among a range of other direct assistance measures to the poor by civil society organisations, and targeted relief by banks.
Germany has rolled out a €750bn economic stimulus package, about 5% of GDP, financed by new borrowing. It will take on new debt for the first time since 2013, representing 10% of GDP. The stimulus will fund unlimited loans to large companies, pay 60% of salaries of companies going into short-time and provide financial support to the self-employed. Up to €100bn will be used to take direct equity stakes in failing companies to prevent collapses or foreign takeovers.
The US has unveiled a $2-trillion coronavirus rescue package, 11% of GDP, for struggling companies and employees. This includes loans, equity stakes in struggling companies and direct payments to companies and individuals. Mid-size companies with between500 and 10,000 employees can access loans with interest rates no higher than 2%, and those with 500 or fewer can access loans from banks to cover more than two months of operational costs and payrolls, with the government covering repayments for the first eight weeks. Struggling airline companies, which are deemed critical to national security, will get $60bn in loans and grants to help with operational costs and pay employees. The government is paying $1,200 to all families earning less than $99,000 a year.
Given these examples, SA's response so far seems inadequate. It should reduce the reserve requirements for financial institutions to allow them to lend at easier terms to struggling firms. The Reserve Bank could and should cut interest rates further. Personal and corporate taxes should be deferred. The Unemployment Insurance Fund should be used to finance those who have lost their jobs because of Covid-19. Government’s contingency reserve of R5bn should be mobilised for targeted intervention in the crisis. And alleviating the economic crisis is also a credible reason for funds of the Public Investment Corporation to be used.
A basic income grant to the poor, unemployed and homeless could prove crucial to helping them through the coronavirus crisis. Food vouchers should be considered to allow the poor to buy food at retailers. The other option is to distribute food parcels to those in need. However, it will be difficult to reach everyone, even if the food is distributed by the army or civil society organisations. Well-off individuals can pitch in with food parcels or vouchers and contribute towards rolling out a basic income grant. Ultimately, government, the private sector and civil society will have to work more closely together than ever before, whether in the health sector, sharing expertise or supporting the vulnerable.
South Africa needs to end the lockdown: here’s a blueprint for its replacement
- Shabir Madhi, Alex van den Heever, David Francis, Imraan Valodia, Martin Veller and Michael Sachs.
Academics call on government to develop a comprehensive health and economic strategy if it is to prevent long term socio-economic damage caused by pandemic.
The public debate on strategies to tackle COVID-19 often unhelpfully positions health and economic considerations in a diametric fashion – as trade-offs. In fact, economic policy has health consequences. And health policy has economic consequences. The two need to be seen as parts of a coherent whole.
In the case of South Africa, the country currently faces three interrelated problems. These are the public health threat from the COVID-19 pandemic, the economic and health effects of the lockdown, and a range of intractable economic problems not directly due to the current pandemic. These include high unemployment, low economic growth and falling per capita income.
Any potentially viable response to COVID-19 needs to address all three aspects in concert. This is particularly important as the country plans for the next stage of its response after the lockdown. Focusing only on the health challenges and not paying attention to the economic issues will result in significantly higher economic costs, and will also undermine the health imperatives.
Our view is that a protracted lockdown won’t necessarily have the effect of ridding the country of the virus, but it will result in unacceptably high health and economic consequences.
The cost
The initial lockdown was prudent and is likely to have lowered the risk of community spread of SARS-CoV-2.
But the true number of COVID-19 (the disease caused by SARS-CoV-2) cases is difficult to quantify. A limited number of tests have been done, and community-wide screening for suspected infectious cases has been delayed.
The available evidence on the COVID-19 pandemic suggests that any initial containment of the disease through a lockdown will be short-lived. Also, it’s likely to result in a rebound of cases in the absence of aggressive community-wide screening for SARS-CoV-2 infectious cases, isolation of the identified cases and quarantine of their close contacts for at least 14 days.
On top of this, South Africa may find itself permanently harmed by the simultaneous destruction of both the demand and supply sides of the economy under an extended generalised lockdown.
This will have other unintended long term health and economic consequences. For example, an extended lockdown could result in the undermining of other health services, such as the immunisation of children.
The economic effects of a lockdown, too, are severe.
Early forecasts suggest significant economic disruption from the current lockdown, which is costing the economy an estimated R13 billion per day. Preliminary projections by the South African Reserve Bank indicate that South Africa could lose 370,000 jobs in 2020. Projections by private banking analysts (based on the initial 21-day lockdown) suggest a GDP contraction of 7% during 2020, leading to a fiscal deficit of 12% of GDP (forecast at 6.8% in the 2020 budget) and a debt-to-GDP ratio in excess of 81% in 2021. This means that the country’s already limited public finances will be further constrained.
Towards a post-lockdown strategy
Globally, attention is turning from initial containment through generalised lockdowns to short- and medium-term risk-based public health and economic strategies. We present some considerations for a health and economic policy beyond the lockdown in South Africa.
In this we proceed from the following assumptions:
The SARS-CoV-2 will not be eliminated in South Africa until either a vaccine is introduced (yet to be developed), or sufficient natural immunity in the population is achieved. It is therefore necessary to put in place and maintain a sustainable mitigation strategy for COVID-19 for the remainder of 2020, or until a vaccine is available (an optimistic timeline for this is 18-24 months).
A generalised lockdown is not a viable long-term prevention strategy for COVID-19 due to its deleterious effects, including the resultant long-term impact on society, public health and the economy.
Removal of the lockdown without appropriate health and economic measures will result in an excess mortality from COVID-19, resulting in further economic hardship.
South Africa’s health and economic strategy beyond the current lockdown must be designed to ensure good health care and be economically sustainable. We argue that the country needs to transition to a risk-based strategy which offers effective health protection and allows for the resumption of some economic activity.
This approach has been advocated by researchers in both Germany and the Indian state of Kerala.
First, mitigate the rapid spread of the virus, while allowing for natural immunity in the population to increase gradually.
Second, strengthen health care systems to ensure optimal treatment for as many patients as possible, both those with COVID-19 and those with other serious illnesses.
Third, protect individuals at high risk for severe COVID-19 disease; and
Fourth, make economic activities possible with measures in place to manage the health risks associated with these activities.
Economic and health strategies
At the highest level, there are three broad intervention strategies available to South Africa (summarised in the table below), adapted from a recent article by leading Australian health academics James Trauer, Ben Marais and Emma McBryde. We believe that option three is the only practicable one for South Africa. And the details of its implementation matter.
Table 1: Typology of interventions and risks
Adapted from (Trauer et al., 2020)
A health strategy based on an extended generalised lockdown is economically unsustainable. It is also damaging to public health. Instead, we need a unified health and economic strategy that allows for some economic activity while inhibiting the uncontrolled spread of the virus. This requires a number of health and economic measures to be implemented in a coordinated manner.
First, to reduce the rate of infections, the country must have ready the capability of mass virus testing and efficient contact tracing before the end of April 2020. This must be accompanied by a comprehensive approach to social distancing. Relying solely on screening of symptomatic individuals will not effectively reduce the rate of infection because high viral loads of SARS-CoV-2 in the upper airway occur in pre-symptomatic and possibly asymptomatic people.
To be successful, the scale of testing needs to be at least equivalent to that in South Korea (17,322 tests per day in South Africa, eventually testing 1 in 150 people). At best, it must be equivalent to that carried out in Germany (36,399 tests per day in South Africa).
Test turnaround times must result in identification of infected individuals within 12 to a maximum of 24 hours. This must be followed by immediate isolation and contact tracing. Isolation of infected individuals and contact quarantine must last for at least 14 days, either at home, if suitable, or in designated isolation and quarantine facilities.
The annual cost of conducting 17,000 tests per day is approximately R5 billion. There would perhaps be an additional annual cost of R4 billion for contact tracing and quarantine. These costs compare favourably to the daily economic cost (R13 billion) of the generalised lockdown.
Secondly, economic activities must be allowed in a way that is consistent with the aim of preventing the uncontrolled spread of the virus. Within the constraints of the health strategy outlined above, a risk-based economic strategy is required that balances economic and health imperatives.
Decisions on differential opening of the economy should be made in line with the criteria proposed in a recent paper by German researchers. This includes, for example, opening sectors with low risk of infection (highly automated factories) and less vulnerable populations (child-care facilities) first. It could also include areas with lower infection rates and less potential for the spread of COVID-19. Of course, these decisions will have to be based on a careful assessment of factors such as household structure and composition in South Africa, and public transport.
To do this, the country will need excellent data on the extent and location of any community outbreaks of the virus. Such data will be generated by mass testing, and accurate information about the ability of certain sectors of the economy to reopen safely and in compliance with the health protocols.
The health and economic strategy will thus need to be implemented in a dynamic fashion, responding to the latest evidence.
This article has been amended to reflect updated estimates of the daily cost of the lockdown.
Cas Coovadia, member of the University of the Witwatersrand Council, also contributed to the discussions that led to the writing of this article.
Message from Professor Zeblon Vilakazi, Vice-Principal and Deputy Vice-Chancellor: Research and Postgraduate Affairs.
Dear Postgraduate Students
I hope that you are all well and keeping safe. This is a difficult time for all and I hope that you remain in high spirits.
You should have received an email earlier this week pertaining to the commencement of the academic programme, which is scheduled to resume online on 20 April 2020. As postgraduate students, and particularly those conducting research at the Master’s and Doctoral levels, your course of action is slightly different. Due to the diversity of research being conducted and the great breadth and scope of the disciplines being explored, it is impossible to address postgraduates as a homogenous cohort.
I would therefore like to advise you to work directly with your supervisor during the lockdown period and beyond, in order to ensure that your research continues from wherever you may be geographically located. A number of online resources have been made available to you during this period to make it easier for you to work from where you are.
Should you have any problems or issues, please raise them with your supervisor or with your relevant Faculty Dean.
Regards
Professor Zeblon Vilakazi
Vice-Principal and Deputy Vice-Chancellor: Research and Postgraduate Affairs
3 April 2020
Resources for postgraduate Students
Access to Data and ICT Support
Wits has worked with Telkom, Vodacom and MTN to ensure that students can access selected learning sites without using data. Cell C is due to come on board shortly and all services will be activated within the next ten days. For a complete list of the zero-rated sites, visit: https://www.wits.ac.za/mywits/zero-rated-data-to-students-and-applicants/. Please note that you must have at least R1 worth of data loaded on a SIM card in order to access these sites. If you have any queries or concerns, please contact the ICT Service Delivery team via ithelp@wits.ac.za or call 011 7171717 or log a call via https://witshelp-ism.saasiteu.com/.
Learning Management Systems
All our Learning Management Systems (LMS) including Wits-e (Sakai) and Moodle will be hosted in the Amazon cloud to ensure that our systems have sufficient infrastructural support and are able to cope with a large number of users accessing the systems.
Access to Smart Mobile Devices
We are also aware that approximately 10% - 15 % of students may not have access to smart mobile devices (according to the results of the biographical questionnaires conducted over the last four years by our Business Intelligence Unit), and Faculties and Deans have been asked to develop a plan in this regard.
Access to Digital Library Resources
There are several resources available to students, including:
Search NWU Accredited Journals and click open on 3rd field down. This will give a list of all the DHET OA accredited journals.
Access to the Wits University Press eBook collection
In this time of unprecedented crisis, when universities are developing online teaching systems and academics are working from home, Wits University Press is joining a large number of international university presses and academic publishers in providing free access to content for students and researchers.
Wits switches to remote online teaching and learning from 20 April 2020
- Wits University
Wits institutes an emergency remote teaching and learning programme as one measure to help minimise the time lost in the academic project.
Dear Colleagues and Students
We are living through an unprecedented era which has tremendous implications for humanity and for us as the Wits community. We know that through our collective efforts we can stave off the coronavirus, and that through physical distancing, testing and quarantining, we can flatten the curve and eventually overcome the disease. But what we do not know, is exactly how long this will take and the exact nature of the resources that will be required.
As the Wits community, we are thus left with some difficult options – wait out the pandemic (and potentially lose the 2020 academic year) or switch to emergency remote teaching and learning alongside a range of other contingency and continuity plans. After consultation with our various constituencies, we have opted for the latter.
We are cognisant of the tremendous effort that has been expended by academics and professional and administrative staff in recent weeks, who have tirelessly prepared online material, who have learnt to switch between pedagogies, and who now have a better understanding of our learning management systems.
At the same time, we are acutely aware of the anxiety and uncertainty that this mode of learning presents for both our colleagues and students. The world as we know it is in flux, and it will take our collective courage, dexterity and commitment to fend off the effects of this pandemic and to adapt to new ways of teaching and learning.
We are aware that the playing field is uneven and that whilst many in society and our community enjoy greater levels of privilege, the consequences of the pandemic have illuminated and amplified the existing inequalities in our society – with the poor, marginal, precarious and under-resourced disproportionally experiencing its fallout. We understand that our emergency remote teaching and learning plan has to take into consideration the different learning environments of our students and their access to learning resources, appropriate devices and data.
Our success is dependent on how we respond as a community – our Senior Executive Team members have to be agile enough to ensure that requisite plans and resources are in place to switch to the emergency remote teaching and learning programme. Our Deans, Heads of Schools, academics and professional and administrative staff have shown that they are able to adapt to a changing environment and are now going beyond the call of duty to ensure student success. Our students will have to exercise their own agency and will have to make an extraordinary effort to adapt to remote online learning with the requisite support from faculties, particularly over the next few months. We acknowledge the importance of the University to provide support but it is also important for our students to develop their own agency to overcome the challenges that confront us today.
Wits re-opens online on 20 April 2020
The next few days (15-19 April 2020) will be used to transition to the online environment with the University officially opening for the second block on 20 April 2020. The almanac has been revised but is dependent on how the crisis unfolds in the months ahead. To be clear, the University is not transitioning to a permanent online modality for all courses, nor are we becoming a correspondence institution. We are instituting an emergency remote teaching and learning programme as one measure that will help us to minimise the time lost in the academic project.
We are clear that the emergency remote teaching programme will not serve as a comprehensive solution to our current challenges. There are specific disciplines that may be patient-based, laboratory-based, studio-based or involve creative practices that cannot be undertaken online. In these instances, we will have to explore high intensity immersion classes when we resume contact teaching, resequencing the academic year to allow for theory to be taught online upfront followed by the practical and laboratory-based components later in the year, and perhaps even recalibrate the almanac.
Access to devices, data and learning resources
Multiple surveys across the institution have revealed that between 10% and 15% of students do not have access to appropriate computing devices, adequate access to data or conducive learning environments. To this end, we are putting in place the following measures to ensure that the majority of students are able to learn remotely:
Wits has established a Mobile Computing Bank (MCB) which will enable qualifying students who do not have access to appropriate mobile learning devices to loan basic devices from the MCB. These basic computing devices will be suitable for educational purposes and will be pre-loaded with the required learning resources before being delivered via the South African Post Office to students who absolutely need them. The cost of the device will be added to students’ fee accounts and will be reversed if the device is returned in good order at the end of the 2020 academic year. The students most in need will be prioritised when devices are allocated.
The University has finalised an agreement with four telecommunications service providers: Telkom, MTN, Vodacom and Cell C to zero-rate Wits’ library and learning management sites from 15 April 2020. The full list of zero-rated sites is available via this link:https://www.wits.ac.za/mywits/zero-rated-data-to-students-and-applicants/
We are working through Universities South Africa to reach agreement with telecommunications service providers to ensure that other products and sites like Microsoft Teams, Zoom and other learning sites are either zero-rated or reverse billed to the University. These sites may have to be accessed via the Wits VPN. Negotiations are underway and we will keep the University informed of these matters in the coming days.
In cases where students do not have access to any device or data, other options are being explored, including the possibility of using the South African Post Office to deliver paper-based material to our students. Additional support will be made available for students when contact teaching resumes, and particularly for students who will have had difficulty in transitioning to online learning. It may be necessary for face-to-face lectures to be extended through the September and December vacation breaks and for some cohorts, to extend the academic programme into 2021.
Students who have queries related to the academic programme should contact their respective schools. Students who do not have access to adequate mobile computing devices and cannot secure them elsewhere, should contact the following Faculty representatives:
As per the communique sent to all postgraduate students on the 6th of April 2020, those students pursuing their Masters or PhD degrees should engage directly with their supervisors to ensure that their research continues. A list of the library sites that have been zero-rated has already been shared with all postgraduate students. In cases where patient-based, studio-based or laboratory-based work is required, these matters should be discussed with the supervisor, Head of School and/or Dean of the respective Faculty.
Conclusion
The next few weeks are going to be challenging for us as a country and as a University. We have no choice but to stand strong in order to overcome this common invisible enemy. We should galvanise our resources to achieve one common goal – to see our students succeed and complete the academic year, despite the inequalities that pervade our society. In so doing, we will develop the high level skills to rebuild our country and produce the problem-posers and problem-solvers needed to tackle the complex problems that confront our society.
We will emerge from this crisis – stronger and more resilient than ever. This is a complex challenge that will require multiple responses from all of us. Let us use this time to find each other and to work together towards a common goal for our students, our staff and our common humanity.
Keep healthy and stay safe.
SENIOR EXECUTIVE TEAM
14 APRIL 2020
Process to apply for mobile computing devices
- Wits University
This communique outlines the process through which students who require assistance with a loan device can apply.
MESSAGE FROM THE DEAN OF STUDENT AFFAIRS
Dear Students
This communication follows the email that you received yesterday and will specifically outline the process through which students who require assistance with a loan device can apply.
COVID-19 is challenging us all to do things differently and to adjust to a “new normal”. We do this from very different circumstances. The University acknowledges these disparities and is doing all it can to ensure that our students are supported during this difficult time. As previously indicated, the remote online teaching and learning programme will start on 20 April 2020.
Whilst we have addressed the majority of the issues related to data access, we understand that some students still do not have access to devices appropriate for online and remote learning. We have thus secured a limited number of devices suitable for educational purposes that will be made available to students in need. Applications will be considered on a case by cases basis, and will take the needs of each applicant into account. These limited number of devices will be delivered to students in need.
Please note these are basic devices, will be on loan to students and will be charged to fee accounts. The charges will be reversed if the device is returned in good working order at the end of the academic year. Whilst we acknowledge that it may be difficult for some students to do so, we want to encourage those students who are able to, to continue their own efforts in securing an appropriate device.
Who may apply for a loan device?
Students registered for a full-time degree in 2020;
NSFAS funded and “missing middle” students with a family income of less than R600 000 annually. Bursary/scholarship funded students who have not received devices from their funders. (Please note that all information supplied will be verified); and
Students who do not have their own device, or who do not have access to a device.
Due to the challenges with delivery, regrettably only students residing within the borders of South Africa are eligible for this assistance.
Devices will be allocated in the following order of priority: final year undergraduate students, first year students, other undergraduate students and then postgraduate students.
Conditions
Devices will be made available on a case by case basis, and decisions are made on the basis of the information available and/or provided. In addition:
All devices must be returned by the end of the 2020 academic year. Where devices are not returned, students will be charged for the full cost of the device;
Where a device is damaged and/or lost, a student will be liable for the full repair and/or replacement cost of the device; and
Wits takes no responsibility for maintenance or the insurance of the device.
Application process
Students in need may approach their respective faculties for assistance, provide all the information required and note the conditions for assistance. Recommendations for assistance may also be made to faculties through student leaders (the SRC, school councils and class representatives) and the Division of Student Affairs, provided that all the relevant information is supplied. Incomplete applications will not be considered.
As the academic programme starts on 20 April 2020, those needing assistance are urged to apply through their faculties as soon as possible.
Students must make sure that they provide the following information:
A brief motivation (including proof of income, if possible);
Name and Surname,
Student Number,
Identity Document Number,
Year of Study,
Physical delivery address details (including province) on the application for assistance, including providing their up to date contact mobile numbers; and
Name and contact details of a next-of-kin, parent, or guardian (the University may contact the next of kin / parent/ guardian to verify information provided).
Applications are made through Faculties, via the details listed below:
We hope that these loan devices will go a long way in supporting students in need. Online and remote learning will require some adjustment to your way of learning. It won’t be easy. Some mistakes will be made and lessons will be learnt. We will do our best to support you towards your academic success and the realisation of your dreams.
Stay safe!
Jerome September
Dean: Student Affairs
COVID-19 Update 23: Wits opens online on Monday, 20 April 2020
- Wits University
Wits will commence with emergency remote online teaching and learning from Monday, 20 April 2020.
Dear Students
We hope that you are all in good health.
As you know, Wits will commence with emergency remote online teaching and learning from Monday, 20 April 2020. Whilst many students are looking forward to starting the second teaching block, we understand that many of you may feel uncertain and anxious about learning online. We would like to reassure you that we are on hand to support you as we embark on this different learning journey together.
A phased approach to online learning
The academic programme will be introduced in phases over the next few weeks, so that you have time to adjust to the new learning environment. All lectures will be available on our learning management systems and can be downloaded at any time. If you are still waiting for your mobile computing device to be delivered or your data to be connected, do not despair – you can access your lectures and other resources from Sakai or Moodle as soon as you are connected. Whilst we will be resolute in our efforts to recover the lost elements of the 2020 academic year, we remain committed to you, our students who are an integral part of the Wits community.
Tests and assignments
No assignments or tests will fall due or be scheduled until the 4th of May 2020. These measures will ensure that students are not academically disadvantaged in any way.
Mobile Computing Devices dispatched
We are cognisant of the digital and related learning inequalities in our society and we are doing our best to ensure that we address your needs. Hundreds of mobile computing devices have been pre-loaded with the requisite software and have already been dispatched. Staff are working through this weekend to ensure that the remaining devices are pre-loaded and dispatched, so that they reach students on Monday or during the course of next week.
Zero-rated sites
Wits has negotiated with telecommunications service providers to have learning and library sites zero-rated so that you can access them at no cost to users. You may require R1 of data to be loaded before you access these sites: https://www.wits.ac.za/mywits/zero-rated-data-to-students-and-applicants/. (P.S. Zero-rating means that you are not charged when you access these sites.)
Access to data
The University has signed a contract with MTN to provide 30 gigabytes of data (10GB Anytime and 20GB Night Express) at no cost to you (Wits students) for one month, to kick-start your online learning journey. It is imperative for your mobile number to be updated on the student self-service portal if you wish to make use of this service, as these numbers will be provided to MTN.
Help is a click away
Please direct academic enquiries to your respective faculty as follows:
Our academics and professional, administrative and support staff have worked tirelessly over the past few weeks to prepare to go online. We have galvanised our resources to support you over the next few months and your success is our priority. We accept that this is a new learning experience and that there may be some challenges, but we are on hand to solve them together. Please feel free to share suggestions on how we can improve emergency remote online teaching and learning over the next days, weeks and months.
Look after yourself and keep healthy and safe.
SENIOR EXECUTIVE TEAM
17 APRIL 2020
COVID-19 Update 24: How to access your data
- Wits University
Dear Students
ACCESS TO DATA – MTN and VODACOM
Yesterday we informed you that the University had signed a contract with MTN to provide 30 gigabytes of data (10GB Anytime and 20GB Night Express) at no cost to you (Wits students) for one month, to kick-start your online learning journey.
We are pleased to let you know that Vodacom came on board this morning with an equivalent offer and will provide details on this in the course of the next 48 hours.
MTN is in the process of verifying information and will be activating the data before Monday morning. Please access the attached information for MTN users to see how to check balances.
If you are using an alternative service provider you may wish to purchase a sim card and then get yourself on to either the MTN or Vodacom network. Please bear in mind that you would then need to update your cell number on the self-service portal. Your new number will only be relayed to MTN and Vodacom on Monday.
It is imperative for your mobile number to be updated on the student self-service portal if you wish to make use of this service.
Please note that this offer runs for one month from 20 April 2020, so please use the data responsibly for educational and learning purposes.
Should you encounter any problems – please contact the service provider in the first instance and then the University via ithelp@wits.ac.za or log a query via https://witshelp-ism.saasiteu.com on Monday.
SENIOR EXECUTIVE TEAM
18 APRIL 2020
COVID-19 Update 24: Data access: All four major mobile service providers on board
- Wits University
Students will get 30GB of data if registered on MTN, Vodacom, Cell C or Telkom.
Dear Students
Wits University is pleased to announce that you can now access 30GB of data (10GB Anytime & 20GB at night) if you are registered with any of the four networks - MTN, Vodacom, Cell C or Telkom. This service is at no cost to students. The offer is valid for one month starting on 20 April 2020, and should be used wisely for online learning and educational purposes.
Here are some tips to maximise your data usage:
Streamline social media apps to save bandwidth. Visit https://wits-e.wits.ac.za/x/FZjd2e to find information on how to reduce data usage on YouTube, Twitter, Instagram and Facebook.
Turn off automatic media downloads in apps such as WhatsApp
Turn off auto play in video apps like YouTube
When viewing videos, select low resolution options. High Definition (HD) videos use high volumes of data.
Turn off automatic system updates and if possible, choose critical updates only. Schedule these to take place at night.
Email documents in a zipped format but use email as a last resort. Content should rather be loaded on Moodle/Sakai where possible.
Turn off cloud storage and syncing options such as iCloud.
If your device has low data or data saver modes, activate them.
Use the following links to streamline data usage on your devices:
Android devices
Tips on how to reduce data usage for Android devices.
Tips on how to reduce data usage for iOS devices. These steps will vary depending on the model of the device that you are using as well as the version of iOS you have installed. Please refer to the online user manuals if your version isn't covered here.
Turning on low data mode
Limiting apps using data
Limiting background data usage
Turning off the iCloud drive
Turning off automatic downloads
We hope that these are helpful. We wish you all the best on your online learning journey.
SENIOR EXECUTIVE TEAM
19 APRIL 2020
[COVID-19 UPDATE 25] Wits VC wishes students well as online learning begins
- Wits University
Video: Professor Adam Habib wishes students well as they begin their online learning journey.
Habib speaks on social justice and the inequalities in our society and elaborates on Wits’ efforts to ensure that all students have access to mobile computing devices, access to data and free access to Wits’ library and learning management systems and sites.
He elaborates on the 5 000 laptops that are being delivered to students who are disadvantaged and the 30GB of data available to every Wits student (at no cost to students) on any of the four major networks for one month from 20 April 2020, in order to kick-start the online learning process.
Habib also explains why it is important to complete the academic programme and encourages students to rise to the challenge and to defeat the effects of the pandemic through online learning. He concludes by saying that Wits University is ready to support students and to walk this journey together.
Debunking 9 popular myths doing the rounds in Africa about the coronavirus
- Neelaveni Padayachee and Lisa Claire du Toit
Some of the false claims about coronavirus may be harmless. But others can be potentially dangerous.
In the second week of March the World Health Organisation (WHO) declared COVID-19 a pandemic. By mid-March the disease had spread rapidly in many countries around the world.
Governments are taking drastic steps, including the complete lockdown of cities, as well as extensive health interventions to try and stem the disease which is caused by a new coronavirus called SARS-CoV-2.
There is still a great deal that’s not known about SARS-CoV-2. This limited scientific information has contributed to a slew of myths and misconceptions. Some claims being made are harmless. Others can be potentially dangerous.
We have identified nine misconceptions doing the rounds on social media in Africa and set out to counter them. The purpose of debunking these myths is to provide people with trusted information. And to provide people with valid scientifically backed answers which they can share on social media to counter the misinformation and disinformation out there.
Myth 1: SARS-CoV-2 does not affect Africans
Across the continent rumours have been rife that the virus does not affect black people. This was fuelled partly by the fact that a Cameroonian student in China, who was among the first people to contract the disease, responded well to treatment.
But there is no proof that melanin protects black people from the coronavirus. There is also no scientific evidence that African blood composition prevents Africans from contracting the coronavirus.
This misinformation persisted even after the deaths of high-profile black Africans, such as legendary Cameroonian musician Manu Dibango, and Zimbabwean media personality Zororo Makamba.
This myth is not limited to Africa. Twitter has recently been abuzz with claims of African-Americans being immune to coronavirus
Myth 2: SARS-CoV-2 cannot survive in Africa’s warm climate
This myth arose after research, which hadn’t been peer reviewed, pointed to temperature having a role in the survival of the virus. One of the most widely quoted sources was John Nicholls, a pathology professor at Hong Kong university who said that “in cold environments, there is longer virus survival than warm ones”.
This claim, however, was not based on verified research. It was nevertheless seized on as proof that the virus cannot thrive in Africa’s warm climate.
The only continent that has no cases of COVID-19 is Antarctica. This could change.
Myth 3: Spray alcohol and chlorine all over your body
Using hand sanitisers that contain 60% or more of alcohol has been found to kill the coronavirus. But, there has been a myth that spraying alcohol and chlorine will kill the virus.
Spraying alcohol all over your body can be harmful, particularly to your eyes and mouth. Importantly, the alcohol in the sanitiser is not the same as the alcohol that people drink. The latter ranges up to 40% while hand sanitisers need to be 60% and above.
Myth 4: Drink black tea first thing in the morning
The media in Kenya have been reporting on false claims that drinking black tea first thing in the morning is effective against the COVID-19 disease.
This is untrue. There is no evidence to suggest that tea can protect a person from the virus. These claims can result in a sense of false security and can be dangerous.
World-renowned Cameroonian musician Manu Dibango’s death from coronavirus hasn’t stopped people claiming blacks are immune to it.EFE-EPA/Daniel Karmann
Pepper has anti-oxidant, detoxification and antimicrobial properties. But, there is no evidence that it prevents or kills SARS-CoV-2. It is also a rich source of vitamin C, which helps maintain a good immune system.
Likewise, lemon and lime also contain high amounts of vitamin C. But there is no evidence to support the claim that they flush the virus out of an infected person’s system.
Myth 6: Steam your face with and inhale neem tree leaves
There have been claims, mostly in Ghana, that steam therapy with neem can prevent COVID-19. What we know is that according to ayurvedic medicine experts, neem can assist in strengthening the immune system and prevent viral infections.
Neem is known to exhibit immunomodulatory, anti-inflammatory, antihyperglycaemic, anti-oxidant and anticarcinogenic properties. But, the Centres for Disease Control and Prevention has emphasised that there is no clinical evidence to suggest that steaming and inhaling with neem will prevent coronavirus.
Myth 7: Vitamin C tablets prevent COVID-19
Vitamin C is a known anti-oxidant. It prevents damage to tissue in the body by neutralising free radicals, which are charged particles that cause damage to cells and tissues and result in inflammation. Vitamin C is also known to protect against pathogens.
But there is no proof that vitamin C can prevent one from contracting COVID-19 though there are trials being undertaken on the use of vitamin C among COVID-19 patient. None has provided conclusive proof.
Malaria – which is caused by a parasite and is transmitted from the bite of an infected Anopheles mosquito to humans – used to be treated with the drugs chloroquine and hydroxychloroquine. These have been used, respectively, as an anti-malarial and as an auto-immune disease drug for inflammation.
The over-hyping of chloroquine has led to worldwide shortages and resulted in people self-medicating. Experts have warned that high doses of the drug are toxic.
Humans have been known to be affected by six coronaviruses, four causing the common cold. The other two were the severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV) in 2002 and 2012, respectively.
South Africa is bent on austerity and should change track
- Dr Gilad Isaacs
The South African government should be spending more, not less, to boost economic growth and create jobs.
As government, economists, activists, business leaders and the public debate the size and scope of government support to the COVID-19 hit economy, it is worth asking a simple question: what is the impact of government spending?
This forms part of a wider debate over whether South Africa should continue on the path of austerity – cutting expenditure with the aim of reducing debt – or undertake a fiscal stimulus – spending with the aim of growing the economy.
Recent research by Professors Enno Schröder and Servaas Storm from Delft University of Technology throws useful light on this question. The research was prepared for the Institute for Economic Justice’s on-going research into the viability, scope and nature of an appropriate fiscal stimulus for South Africa. The research was undertaken before COVID-19 hit. It is even more relevant now.
The research shows that for every R1 billion government spends, gross domestic product (GDP) increases by R1.68 billion and 6,900 jobs are created. This means that spending 6% of GDP, R305.6 billion, would increase GDP by R513.4 billion and support the creation of 3,542,460 jobs.
Thus government spending is able to grow the economy, to the extent that it could lower the debt-to-GDP ratio. It also shows that additional government expenditure could sustain the economy through the current crisis period.
Does the economy have room for expansion?
An economy’s ability to grow can be constrained by factors that limit its ability to produce goods and services – “supply-side” factors like poor infrastructure or a lack of education. It can also be constrained by a lack of funds to purchase the goods and services it does produce – “demand-side” factors.
The International Monetary Fund and South Africa’s national treasury argue that the country’s poor growth performance over the past decade is due to supply-side factors. These include infrastructural bottlenecks in electricity generation and supply, over-regulated (formal) labour markets, and increases in product market concentration (as seen in rising profit mark-ups).
The IMF and treasury therefore support budget cuts, labour market deregulation and tax cuts, all of which purportedly will promote private-sector led and inclusive growth.
Here the assumptions lead to the conclusions obtained. If the South African economy is assumed to be supply-constrained then naturally only supply-side interventions such as lowering labour costs will enhance growth. If this is the case, so the argument goes, then fiscal stimulus, which aims to raise demand in the economy, is a blunt tool, providing little opportunity for economic revival.
But this does not factor in the room for economic expansion that clearly exists.
According to the country’s statistics agency, Stats SA, utilisation of production capacity – the capacity of the economy to produce goods and services, for example, through factory output – is on the decline. Between 2018 and 2019, production capacity declined by 2%, with eight out of ten manufacturing sectors showing a decrease.
At the same time, unemployment is unconscionably high, at 29.9% in the last quarter of 2019, and inflation is falling, now below the middle of the South African Reserve Bank’s target range.
It is true that infrastructural shortages such as expensive internet or inefficient rail transport can constrain economic performance. But targeted fiscal expansion – investment in free broadband or investment in rail freight services – can remove these bottlenecks and expand supply capacity, while also boosting demand.
South Africa’s fiscal multipliers
The impact of fiscal expansion (and fiscal consolidation) is ultimately determined by the size of the fiscal multiplier. A fiscal multiplier measures the impact that each additional rand of government spending would have. Schröder and Storm estimate both the “income multiplier” – the impact of spending on GDP – and the “employment multiplier” – the impact of spending on employment growth.
In their first estimation, increasing demand in the economy (via government spending) will initiate additional production. That will require more labour input (a direct effect). The higher demand for labour services will increase labour income. This will cause higher consumption spending in a particular industry (an indirect effect) and in connected industries (an induced consumption effect).
The results of this first technique indicate that a fiscal stimulus of R1 billion will raise South Africa’s GDP by R1.5 billion and create 6,100 jobs. This is in line with previous studies using this technique.
In their second estimation, they include an induced investment effect. This refers to a change in output, income and employment that would come from firms investing a fraction of the additional profits earned in supporting industries.
For this technique, the estimated income multiplier shows that R1 billion increases GDP by R1.87 billion and generates 7,700 jobs.
The authors prefer an average of the two techniques, showing that a fiscal stimulus of R1 billion will generate R1.68 billion extra income and create 6,900 new jobs. This is because the first technique leaves out investment effects, but the second overestimates these because the data does not distinguish between private-sector and public investment.
These figures allow us to calculate the impact of different levels of additional government expenditure. Increasing spending by 3% of GDP, or just over R150 billion, leads to an expansion of GDP of just over R250 billion and almost 1.8 million jobs. Spending of 6% of GDP (just over R300 billion) leads to over R500 billion in additional GDP and 3.5 million jobs, and spending of 10% of GDP leads to an increase in growth of just over R850 billion and also 6 million new jobs.
Yet the path that the South African government has chosen is to reduce rather than increase government expenditure.
Fiscal consolidation and growth
South Africa’s 2020 budget proposes, over the next three years, tax relief and rebate measures combined with reductions in public spending of approximately R48 billion (when taking account of both government cuts and increases, and comparing these to what an inflation-based increase would be). The argument goes that austerity will help revive the stagnating South African economy and kick-start economic growth by inspiring “confidence” in the business sector and global financial markets and contribute to the sustainability of public debt. This is the conventional wisdom.
Another view has it that austerity has in fact contributed to the slow growth of the South African economy and to the growing income inequality experienced in the 2010s. Schröder and Storm argue that continued fiscal tightening is counter-productive to the aim of raising the country’s long-run growth performance.
In fact, the multipliers above suggest that the proposed cuts in public expenditure, of R48 billion, will likely reduce South Africa’s GDP by R81 billion over the next three years 2020-2022. This amounts to a decline in GDP growth of around 0.5 percentage points, accompanied by the likely destruction of around 330,000 jobs.
The 2020 austerity budget is socially and economically destructive.
The present moment
The present context has made the picture more complicated, but this analysis even more essential. It has become clear that the economic fallout from the COVID-19 pandemic, and measures taken to stop its spread, will be massive. The economy could shrink by as much as 8.3%, some estimates show. This calls for bold interventions by government.
These interventions will not take the path of a traditional economic stimulus as the lockdown and associated measures purposefully attempt to slow the economy. Rather, the economy is being put on life support.
This life support must ensure that a viable economy still exists when the spread of COVID-19 is eventually contained. This will require an unprecedented increase in government spending. It’s therefore essential to know how effective each rand of government spending will be in sustaining GDP.
COVID-19 risks forcing SA to make health trade-offs it can ill afford
- Karen Hofman and Susan Goldstein
South Africa could lose many children due to a measles outbreak which is completely preventable.
South Africa’s health authorities are testing, quarantining and treating individuals who have been exposed to the new coronavirus. And the country is in lockdown in an attempt to slow the spread.
Much has been said about balancing the economic trade-offs with the lives the country needs to save versus the social and economic costs of doing so. Less discussed are the trade-offs being made within health care as services are focused on COVID-19.
Child health is of particular concern. South Africa has 5.8m children under 5 years of age. This group appears to be less susceptible to COVID-19. But, if the country doesn’t pay attention, the death rate for these children will soon increase.
The reason for this is measles, a highly contagious disease that mostly affects children under the age of 5. The basic reproductive number of measles in a susceptible population is between 12 and 18. This means that on average every person with measles will infect between 12 and 18 people. While we don’t know with certainty, the reproductive number of symptomatic cases of SARS-CoV-2 is thought to be between 2 and 3.5.
Measles remains a threat in countries across the world despite the fact that a safe and effective vaccine has been available since 1963.
Most measles-related deaths are caused by complications. The most serious includes brain swelling, severe diarrhoea and related dehydration, pneumonia, blindness and deafness. Severe measles is more likely among poorly nourished, young children. With 27% of the country’s children either stunted or wasted, any relaxation of the vaccination regime would place them at high risk of severe disease.
The danger is that health workers will be diverted to other tasks related to COVID-19, further compromising immunisation. This could well mean that South Africa will lose many children due to a measles outbreak which is completely preventable.
The measles threat
Previous research on the impact of measles catch-up campaigns on routine immunisations in 2010 can help inform the country’s thinking. These campaigns – or supplementary immunisation activities – required the mobilisation of a large health workforce from within health system.
This had a severe effect on the delivery of health. For example, the research showed that during a three week campaign in 52 districts in 2010 there was a 30% decrease in children completing the primary course of immunisation. In addition, there was a 10% decrease in antenatal visits and a 12%-17% decrease in use of injectable contraceptives.
The COVID-19 epidemic has resulted in the provision of only “essential” health services in some provinces. If routine immunisation is not classified as an essential service there will likely be severe consequences.
In particular, measles will start rearing its ugly head and children will die needlessly. This has occurred in pockets all around the world as a result of campaigns run by parents who refuse to have their children vaccinated. Globally there were 140 000 deaths in 2018 – all avoidable.
The South Africa government should urgently put in place a plan that can be implemented once the lockdown is over. It should, for example, consider opening schools or day care centres as sites for immunisations. The campaign could use a mobile – information providing cell phone application called Mom Connect to send messages to those caring for children under 2 asking them to bring them to the chosen sites. School nurses together with a volunteer corps of retired doctors and nurses could administer vaccines.
Additional trade offs
The country risks making other health trade offs too.
South Africa is still in the midst of an HIV epidemic – with 7.9 million people infected. Some 2 million, however are not on treatment, which puts them at high risk for COVID-19
An important lesson the country has learnt about the HIV epidemic is that prevention is critical. And that it needs to be started early (in the epidemic and in life) and needs to be continued for decades. This lesson has not yet been extended to health overall and health literacy for the whole population is a critical base on which to engage a population when it comes to an epidemic.
South Africa has other areas of vulnerability when it comes to health. The country lags behind other comparable developing countries. We don’t achieve “a good bang for the buck” in terms of health. Peer countries such as Thailand and Brazil spend less on health and achieve better outcomes. For example, under 5 mortality in Brazil is half of South Africa’s 32 deaths per 1000 live births.
The danger is that these statistics will get worse as a result of efforts to curtail COVID-19.
Other areas of concern are the growing burden of obesity-related disease such as hypertension, diabetes and common cancers, diseases related to tobacco use and alcohol misuse. Over the past two decades South Africa has not maximised cost effective investments in preventing and treating these conditions.
This means that millions of South Africans are now more vulnerable to COVID-19.
What needs to be done
South Africa needs to begin with prevention of disease and promoting health by focusing on risk factors, many of which are in sectors other than health. These include inequality and poverty, access to clean water and sanitation, healthy nutrition, alcohol and tobacco control.
Without this we will be even less prepared for the next pandemic.
Karen Hofman, Professor and Programme Director, SA MRC Centre for Health Economics and Decision Science - PRICELESS SA (Priority Cost Effective Lessons in Systems Strengthening South Africa), University of the Witwatersrand and Susan Goldstein, Associate Professor in the SAMRC Centre for Health Economics and Decision Science - PRICELESS SA (Priority Cost Effective Lessons in Systems Strengthening South Africa), University of the Witwatersrand. This article is republished from The Conversation under a Creative Commons license. Read the original article.
Coronavirus myths: Lessons from an AIDS study
- David Dickinson
Attempting to defeat these folk theories with science achieved little; the myth busters of the AIDS epidemic talked past those they were trying to convince.
The coronavirus pandemic is accompanied by what the World Health Organisation describes as an “infodemic” – misinformation, disinformation or conspiracy theories: “coronavirus myths”. These circulate on social media and are further disseminated by influencers, the click-bait infotainment “penny dreadfuls” of the internet, mainstream media which repeat them for audiences to shake their heads at the apparent credulity of others, and some world leaders.
In response, myth-busters attempt to squash coronavirus myths. The modus operandi is to report the myth and then rebut it with science, medical research and expert opinion. The problem with this approach is that science, medicine and experts are, for now, handicapped. There is no vaccine and they have no other easy solution to offer. Given this, alternative explanations are bound to emerge.
All epidemics are accompanied by what leading academic Paula Treichler described, in the context of HIV/AIDS, as epidemics of signification. The key difference with the internet is that contestation over the disease is easier to access.
But, just as in the early years of HIV/AIDS, science is once again on the back foot. This means that today’s batteries of myth busters will be just as ineffective as their pre-internet predecessors.
In 2008 and 2009, before residents in South Africa’s townships – where much of the poor and predominantly African population lives – had significant internet access, I conducted an action research project with working class HIV/AIDS peer educators to investigate and combat the many non-scientific explanations of HIV/AIDS .
The project took seriously the HIV/AIDS myths that the peer educators were encountering. In doing so we were able to gain insights into the origin of these myths and why they were so durable in the face of public health campaigns. As an action research project we used these insights to develop responses based not on repeating scientific information, but on messages that would resonate with beliefs and ideas within the communities of the peer educators. I believe there are lessons here for the current coronavirus pandemic.
Insights
One myth doing the rounds at the time was that whites created AIDS to control the African population. This had circulated for decades despite sustained public health messaging.
Then, as now, science was on the back foot, with no cure for the disease.
I came to see these alternative explanations not as myths, or nonsense, but folk theories which, in the minds of many, were legitimate alternative explanations to that science. Along the lines of the explanation provided by Hungarian philosopher of mathematics and science Imre Lakatos of scientific research programmes, these myths about the disease were “auxiliary theories” linked, within the South African AIDS epidemic, to a trinity of “core ideas”: a belief in God, racial oppression, and traditional African beliefs.
Attempting to defeat these folk theories with science achieved little; the myth busters of the AIDS epidemic were talking past those they were trying to convince.
Convincing people to follow public health responses is much easier when the peril can be seen. But with AIDS the long incubation period, and stigma, hid the disease. One of the challenges with COVID-19 is that someone can be infected, but not show symptoms. And once they are visible the opportunity for effective public health responses in poor and crowded communities is compromised.
A different approach
Rather than repeating accurate, but ineffective, public health messages over HIV/AIDS, I worked with peer educators on alternative ways of shifting attitudes.
We identified HIV/AIDS folk theories circulating in their communities and ran workshops designed to develop stories, sketches and parables in local idiom that could counter these in easy to grasp and engaging ways. For example, to the belief that God could cure AIDS and that antiretroviral treatment was unnecessary, they developed the story of a man who encounters a lion and, kneeling to pray, pleads with God to save him. The lion devours him. The message? He should have run and asked God to help him run faster. The lesson? Take antiretroviral drugs and pray that God will keep you healthy.
Verifying the impact of specific interventions aimed at behavioural change within the complex reality of an epidemic is all but impossible. Nevertheless peer educators reported the interventions positively, and said that they helped them move from previous efforts too often limited to “preaching to the choir”.
As the coronavirus pandemic unfolds so too a matrix of folk theories, reflecting deep beliefs, fears and concerns, is becoming visible. These include xenophobia, nationalism, new technologies, surveillance, and distrust of global elites.
These folk theories resonate with people whose trust in science or experts is, at best, conditional. Confronting them with science in an attempt to overcome resistance to public health measures and social distancing practice will have limited impact.
An approach that reaches beyond “the choir” is needed.
Next steps
Front-line health and community workers should be linked to storytellers, comedians, directors, scriptwriters and others to develop, in local idiom, easy to understand messages about the virus and preventative behaviour in entertaining and catchy formats. These should, indirectly, be aimed at countering the impact of identified folk theories and promoting behavioural change, not in headlong, hectoring attacks but using softer power and where possible acting in tactical unity, as with The Man Who Met A Lion.
The HIV/AIDS peer educators had to slip their stories and parables one by one into ongoing, real-time conversation. Today, the outputs from collaborations could be inserted into social media networks, to “fight fire with fire”. They could be released as amateurish-feeling and unbranded video clips, voice messages and memes.
The degree to which these were forwarded, and effective, would depend on how arresting and entertaining they were.
Such a response will not solve the increasingly recognised cause of the pandemic’s ferocity on precarious individuals and groups. But it would provide a low-cost, complementary approach to mitigate the impending catastrophe in poor communities.
South Africa needs a post-lockdown strategy that emulates South Korea
- Alex van den Heever, David Francis, Francois Venter, Imraan Valodia, Lucy Allais, Martin Veller, Michael Sachs and Shabir Madhi
South Africa cannot afford to embark on a strategy of extended periodic lockdowns. It needs to shift to mass testing and contact tracing.
What strategy should South Africa follow to contain the outbreak of the SARS-CoV-2 virus after the current 35-day lockdown? Any strategy should be informed by the trajectory of the disease, the effectiveness – or otherwise – of the current lockdown and how the particularities of the country will interact with the virus. These include high levels of HIV infections and the complexities of social distancing in lower-income neighbourhoods.
It must also be informed by economic considerations as these have their own, real impact on public health. South Africa has this far relied exclusively on epidemiological criteria for ending the lockdown.
What is clear is that the lockdown has an extremely high economic cost. The country should be looking to alternatives that will be less costly and also more effective in the long term at protecting its communities, its health system and its economy.
We have developed a model that draws on the experiences of other countries, particularly South Korea. We argue that South Africa needs to urgently prioritise its mass testing and contact tracing capacity, which gives it the best chance of saving the nation’s health and economy.
The cost of this programme, even at its most expensive, would be a tiny fraction of the costs of a prolonged lockdown. The South Korean programme had the benefit of attacking the epidemic when it was still small and containable. South Africa retains this advantage over the worst hit European countries. The question now is how to effectively use the time under lockdown to ensure that it is able to contain the spread of SARS-Cov-2, manage the health risks and minimise the economic costs.
Early responses
The implementation of the country-wide lockdown on 27 March 2020 was timeous and necessary. It bought the country valuable time to increase its testing and contact tracing capacity, and to prepare its health system. But South Africa’s initial response to the emergent epidemic in Wuhan, China, in January 2020 was similar to much of the rest of the world – watchful waiting but, with hindsight, perhaps insufficient contingency planning.
South Korea is a notable exception. Due to its experience of the MERS outbreak in 2015, it was better prepared. Instead of embarking on a total lockdown, the country had a more nuanced approach by enforcing, with citizen buy-in, extensive social distancing coupled with scaling up of other preventative and precautionary measures.
Crucially, at the centre of that strategy is aggressive screening for the SARS-CoV-2 infection and isolation of infected individuals, and the tracing and quarantining of their contacts. This enabled South Korea to keep a substantial proportion of its economy open. It did, however, rapidly close its borders, thereby minimising imported infections.
Mass testing and contact tracing work best when the epidemic is still at a relatively low level. This is because the reproduction rate of the disease, often referred to as R or Ro, is so high that a country needs only to be off guard for around two weeks before effective public health intervention options seriously narrow.
Roughly speaking, the R for SARS-CoV-2 is estimated to be about 2.5 every four days. That is, one person infected by the virus infects approximately another 2.5 people over a period of four days. That may not appear fast – but at that rate everyone in this country will get infected within the space of a couple of months, if no prevention to reduce this infection rate is implemented.
Where transmission of the virus becomes widespread, at the community level, the scale of the infections severely limits the effectiveness of mass testing and contact tracing. This is because the infected population is so widespread and growing all the time, while many of those infected are asymptomatic – by some estimates up to 80%.
The only option then is to drag the infection rate down to manageable levels by severely limiting the movements of the population for a period of up to two to three months – a generalised and long-term lockdown.
Mass testing and contact tracing
South Africa’s saving grace is that it implemented the lockdown at a much earlier stage of the epidemic than many other countries. At that point most new infections were those who had returned from international travel and at the time it seemed that community-based infections were confined to the affluent population.
As the country then did not have the capacity to undertake mass testing and contact tracing, precious time was bought with a lockdown that was gradually scaled up. But it came at a very high economic cost.
We have developed a COVID-19 intervention model which is able to analyse some possibilities for the course of the epidemic, and to assess possible responses and costs. Models are a useful and effective tool (although of course not infallible), under conditions of uncertainty, for providing us with an informed and systematic way to compare the impact of a range of policy interventions.
We estimate that if South Africa were to rely exclusively on lockdowns to keep the epidemic under control during 2020, approximately 192 days of lockdown would be required, divided into three episodes. This is because the epidemic is likely to resurge the moment any lockdown is removed unless there are strong public health interventions in place. These interventions include testing at scale, isolation of infectious cases, and high levels of tracing and quarantine of their close contacts.
The cost of lockdown
Given that the lockdown effectively closes down both the supply and demand sides of the economy, the loss of gross domestic product (GDP) is nearly complete – by our estimates roughly R13 billion per day. Over 192 days, the loss of GDP is of the order of R2.5 trillion – almost 50% of GDP.
The lockdown strategy will clearly lead to an economic collapse of a magnitude that will impact health, lives and livelihoods. This is why it is so important that the next stage in the country’s COVID-19 strategy is informed by both health and economic considerations because the two are so tightly intertwined. It would be a grave mistake to rely only on epidemiological factors and ignore the looming economic catastrophe and its dire impact on public health.
Our projections are based on South Korea’s successful prevention strategy of mass testing and contact tracing. Early evidence shows this is also working in Hong Kong. If successful, this strategy reduces the probability of having to resort to repeated and extended generalised lockdowns. Lockdowns would only need to be implemented selectively if localised outbreaks were identified and could be contained.
The opening of the economy would, however, still be subject to:
continued social distancing;
strict implementation of health protocols for employers;
ongoing self-isolation of high risk groups; and
measures to mitigate the risk of viral spread in the country’s mass transport systems.
It would also require very careful systems and support to manage risk and spread within health care facilities.
At the South Korean levels of testing of around 17,000 per day, the annual cost of this strategy would be around R5 billion. At 36,000 a day (the Department of Health target for 30 April), this grows to R10.5 billion. At the target set by the UK of 100,000 per day, the cost would be R29.2 billion per year. This is cheap if it is considered that these annual costs represent respectively 0.4, 0.8, and 2.2 times the single-day cost of a lockdown.
A programme of mass testing and contact tracing is challenging, particularly in the South African context. The persistence of spatial apartheid, and a large number of multigenerational households, and concerns about our state’s capacity, mean that South Africa faces a number of challenges not present in South Korea.
Despite these risks, South Africa cannot afford to embark on a strategy of extended periodic lockdowns. It is critical that the capacity for mass testing and contact tracing is in place prior to the end of this lockdown. The country’s health system must be given every support to ensure its success.
Women and children face even more alarming levels of abuse due to COVID-19 lockdown.
The Covid-19 emergency package of government fails glaringly to provide protective measures to save vulnerable women and children from violence and abuse during the lockdown and the follow-on lockdown.
The lockdown may have been effective so far in slowing the spread of Covid-19, but confining people to homes raise the specter of all ready alarming levels of violence and abuse against women and children, to explode to terrifying levels.
South Africa already has among the highest levels of violence and abuse against women and children per capita outside war zones.
The “cabin fever” phenomenon, whereby long isolation leads to fear, anxiety and a sense of powerlessness could increase the incidents of violence against women and children.
In addition, the Covid-19 related economic downturn, business closures and looming unemployment, increasing fear, stress and anxiety and stress, which can often result in men taking out their frustrations against women and children.
Moreover, because of inequality, most men are still the major or only income earners, which means abused partners are often financially dependent on their abusers.
The movements of vulnerable women and children during the lockdown are restricted, like everyone else, so they cannot easily leave violent or abuse households or seek help. The restrictions of movement during the lockdown also constrains the reach of civil society organisations dedicated to fight violence and abuse against women and children.
Sadly, the army and the police, 26 years since the end of apartheid are still stunningly poorly trained, sensitized or emphatic to deal with violence against women and children. In fact, many of their members often perpetrators of violence and abuse against women not only within their own ranks, but against the very same vulnerable women and children they are supposed to protect.
Incidents of domestic violence and abuse in many other countries have also dramatically increased during lockdowns.
United Nations Secretary General Antonio Guterres in a video message posted on Twitter this week warned about a “horrifying global surge” in domestic violence during the Covid-19 crisis. “We know lockdowns and quarantines are essential to suppressing Covid-19. But they can trap women with abusive partners,” he said.
The South African Police Services said it had received 87 000 gender-based violence calls during the first week of the lockdown.
The French government this week for example approached hotels to have women victims of violence to stay in vacant and for the state to pay for it during their Covid-19 lockdown. Some countries have created pop-up counselling centres at retail stores, pharmacies and other essential service points for women who are experiencing violence and abuse.
The UK this week released a £750million Covid-19 emergency funding package for charities and civil society organisations, including those work with women and children victims of domestic violence and abuse. Australia released US$100million for support services to combat Covid-19 related domestic violence and abuse.
Brazil, like South Africa, has high levels of gender inequality and gender-based violence, has given women money directly, to empower them, by providing a basic income grant of US$125 over three months over the period of their lockdown. India, another developing country with high levels of gender inequality and gender-based violence has paid cash amounts to vulnerable women with bank accounts who are already linked to a government backed financial inclusion programme to empower them; and food parcels are directly given to women.
In South Africa, the police and army patrolling the streets to enforce lockdown must be given instructions to listen to women and children complaining about abuse. Off course, it goes without saying the police and the army should not themselves be perpetrators of violence and abuse against women and children. Prosecution of perpetrators of violence and abuse against women must be swift; with special courts set up if necessary.
Retailers, pharmacies and other essential services could serve as pop-up counselling centres. Funds must also be set aside to support victims of violence and abuse during the Covid-19 lockdown period. As part of the emergency economic measures, civil society organisations dealing with abuse against women and children should get special funding during the lockdown to continue what they do. Food vouchers that can be used at retail stores or food parcels which can be distributed by the army, must be given to all those in need. A basic income grant to all indigent will make them less dependent on men during the Covid-19 lockdown.
Hotlines, shelters and legal assistance for victims of gender-based violence must not only remain open, but should be generously resourced. Individuals who can, must volunteer to help at hotlines and shelters and provide financial, legal and accommodation assistance. Telecommunications companies such as Telkom, Vodacom and MTN, could make a simple key or function available on mobile phone platforms, similar to if one wants to dial for airtime or data, which serves as free hotline to report violence and abuse against women and children.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand; and author of Restless Nation: Making Sense of Troubled Times (Tafelberg).This article was first published in the Sunday Times.
If you think lockdown is bad, spare a thought for SA’s prisoners
- Nkateko Mabasa and the Wits Justice Project (WJP)
How more restless are those living in prison and confined to a small cell, who are now completely cut off from the outside world and their families?
A “stay at home order” means different things to different people living in South Africa. Confined to our homes, we are now experiencing the restlessness that comes with being held in one place. Some are restricted to their small apartments, while others are in crowded shacks and lucky few have a piece of land. For the most part, we are locked in with loved ones and have some access to the outside world.
For the 164,000 or so prisoners in South African prisons, on the other hand, a coronavirus lockdown is a different experience. The four walls of a prison cell are small, and in South Africa’s case, the cells are often overcrowded.
The Judicial Inspectorate for Correctional Services (JICS) – a prisons oversight institution – in itsannual report, noted that the prison population remains overwhelmingly overcrowded with a national bed space of a little under 120,000 across the 243 facilities nationwide, leaving more than 45,000 inmates without proper accommodation.
On 20 March 2020, five days after President Cyril Ramaphosa announced the National State of Disaster, the Minister of Justice and Correctional Services, Ronald Lamola, announced, at a media briefing in Pretoria, the measures that the department was “currently implementing in all centres to protect offenders”.
These included sanitising and cleaning strategic areas across all centres, availing basic hygiene essentials to offenders and officials, distributing essential equipment such as gloves and masks, and “disinfecting keys and shackles”. And more stringently, prohibiting prison visits by family members and friends as well as suspending the parole boards.
The Department of Correctional Services (DCS) would also be “identifying isolation areas in all our centres,” added Lamola.
So far there have been94 casesof Covid-19 recorded within correctional services facilities, half of which are inmates. Most of these cases are concentrated in one facility. Of the confirmed Covid-19 cases, 87 are at the East London Correctional Facility for Women and six are spread out across St Albans in Eastern Cape, Worcester Correctional Facility in the Western Cape, Kutama Sinthumule Private Facility in Limpopo and Warm Bokkeveld in the Western Cape. The DCS head office in Pretoria has recorded one case from a staff member.
Nationally, as of Monday 20 April, there were3,158 confirmed Covid-19cases and 54 people had died of the virus. While most people are able to self-quarantine at different homes, according to the justice minister,“infected prisoners”have “been placed in single cells on a separate quarantine site” of the prison.
This raises questions of whether this will not infringe on the UN Mandela Rules’ basic standards for the humane treatment of prisonerswhere prison isolation can be torturous.
Only after the National Institute for Communicable Diseases (NICD) conducted a mass screening at the East London centre on 8 and 9 April, was the DCS able to get a full grasp of the spread of the virus. However, according to Professor Salim Abdool Karim, a clinical infectious diseases epidemiologist, who spoke to Newzroom Afrika it takes about two weeks for an infected person to show symptoms. He said the confirmed cases so far are infections that occurred two weeks prior to testing, so the real current figures could be higher.
During a prison visit to the East London Facility for Women, on 12 April, Lamolaremarkedhow the spread of the virus initially began with a prison official “who tested positive” after having “attended a funeral where she interacted with people from overseas”. And when she came back to work, she came into contact with “30 officials” who were subsequently requested to self-quarantine while waiting for their test results.
On the outside, suspending basic civil liberties on the population to combat the pandemic might be frustrating to most citizens, but it is an entirely different matter from the more drastic change of daily routine for prison life. According to Africa Check,“problems plaguing SA prisons”include overcrowding, a lack of accurate prison data and transparency, the prevalence of infectious diseases such as TB, and human rights violation such as assault, torture and isolation.
Further precautionary measures to combat Covid-19 include the restriction of access to the courts, court precincts and justice service points and limiting the number of persons entering court buildings. And the number of trials are limited to urgent matters only. Concurrently, there are more than 46,000 inmates in remand awaiting trial.
These restrictions, although meant to protect prisoners, infringe on the rights of those waiting to argue their case in court. The high numbers of those awaiting trial, coupled with limited court functions during the lockdown mean that those in remand face longer periods in remand and risk exposure to the coronavirus while locked up.
Remand centres are a hotbed for respiratory illness transmissions. Most overcrowding in prisons happens in remand centres. In 2016, Sonke Gender Justice andLawyers for Human Rightslaunched acourt challenge against the“inhumane conditions suffered by detainees awaiting trial in Pollsmoor Remand Detention Facility”, after an inmate contracted TB.
Lawyers for Human Rights found that as of “24 October 2016, Pollsmoor Remand was operating at around 249% capacity”. According to Africa Check, after the Western Cape High Court ruled the conditions at the Pollsmoor prison unconstitutional, the department was able to reduce prison overcrowding to 149% – which is still uncomfortably high.
And although DCS has so far achieved an83% TB cure ratewithin its facilities, the lockdown regulations will disrupt any programmes to stop TB infections amid overcrowding. These conditions – the lack of social distancing space and prevalence of a respiratory disease – are the perfect breeding ground for the spread of Covid-19, and substantially increase the numbers of those who are at risk of developing life-threatening complications from the virus due to weakened immune systems.
Any efforts to combat the pandemic in South Africa’s prisons will mean a serious disruption to the already limited prison infrastructure and further limits to the few privileges offenders are afforded on their journey to rehabilitation. It begs the question then, is DCS not one step behind the pandemic’s spread inside prison facilities? And is adequate personal protective equipment afforded not only to the prison officials but to the prisoners also?
Before any cases were discovered in the East London prison, the Department of Correctional Services had initially stated that:
“DCS reassures all officials that care for our staff remains one of our highest priorities. Every precaution is being taken to safeguard the department against the coronavirus and to ensure a safe working environment. This includes provision of the necessary tools to prevent the spread of the virus, and increasing protection in the workplace.”
The prison official who exposed inmates and other officials at the East London Correctional Female Facility subsequently became a super spreader – where one person spreads the virus to large groups of people at different social events and work space. And for prisoners, whose daily lives are dependent on their routine interaction with prison officials, the DCS is their only recourse for safety from the virus within the prison facilities.
At the St Albans facility, 85 officials are waiting for their results. And at Worcester Correctional Facility, DSC is still conducting contact tracing. While this is going on, those who are under the care of the state for rehabilitation are stuck together with infected individuals in overcrowded cells and have to interact, daily, with prison officials.
Further compounding the issue, the Judicial Inspectorate for Correctional Services, the institution responsible for carrying out prison oversight, has suspended all its prison visits during the lockdown. JICS has to, during the lockdown, depend on the department it is supposed to oversee for information regarding prison conditions. Without proper oversight, it’ll be difficult to know whether DCS is indeed complying with safety standards and preventative measures.
There have been recent reports, byDaily Dispatch, about prison officialsfeeling neglectedby the DCS because they have not been provided with proper protective gear. Those who have tested positive for C0vid-19 report being told to self-quarantine at home or at a DCS guesthouse. The Eastern Cape-based media outlet reports that officials feel like they “have been left to die” by the Department of Correctional Services.
Further reports include a large crowd of prisoners in the Mdantsane Prison, in East London seenplaying soccer outsidein contravention of the lockdown regulations.It is understandable, of course, how hard it must be for those already living in prison to stick to the self-distancing rules and the “stay at home” order in their cells.
Since the 21-day lockdown was extended by an extra two weeks, citizens have made representations for the president to loosen some restrictions for recreational activities, business dealings and other essential services to continue.
How more restless are those living in prison and confined to a small cell with barely enough room to move around, who are now completely cut off from the outside world and their families?
This article was produced for the Wits Justice Project (WJP). Based in the journalism department of the University of the Witwatersrand, the WJP investigates human rights abuses and miscarriages of justice – including wrongful convictions – related to SA’s criminal justice system. This article was first published in Daily Maverick.
The case for a citizens’ basic income grant in South Africa
- Vishwas Satgar
With Covid-19 and the lockdown there is no room for denial of how large parts of South African society suffer.
High-income earners have gone online, fridges are stocked and uncertainty is mitigated by healthy bank balances. Low-income households are writhing with anxiety at job losses, are pushed into hunger by the suspension of income-generation opportunities, even in the informal economy, and informal settlements do not have stocked fridges.
We are a society marked by a racialised and gendered social class divide; a cruel society, even 26 years into post-apartheid democracy.
However, the irony of our situation is that we have had black rule in post-apartheid South Africa. The African National Congress (ANC) has led the post-apartheid order and it has nothing short of a strange commitment to black lives.
On the eve of lockdown, the Minister of Education, Angie Motshekga, on national television, trumpeted that “our people have coping mechanisms” thus implying all will be well. This “we know best” attitude gave South Africa a glimpse of the disconnect between the ruling party and lived realities. The reams of economic data on racialised and gendered inequality in South Africa speaks for itself as a counter to ruling party arrogance.
A few years ago we were told ANC cadres did not struggle to be poor. Due to their mythic role in a complex struggle, involving sacrifices by people from all walks of life, they deserved a post-apartheid dividend; we owed our liberators. And of course, they cashed in on this with rampant looting. It is time the mangled, hypocritical and tortured soul of the ANC-led alliance, which is there for all to see, gets a speedy send-off.
However, before then and just maybe somewhere in the Kafkaesque world of the ANC, driven by jostling self-serving factions, there is a residue of genuine concern for black lives and South Africa in general. Just maybe, in the decisive leadership being provided on Covid-19 and ostensibly out of concern for us all, it is capable of understanding that now is the time to give concrete expression to the living hope of the many. This of course does not mean authoritarian populism Malema-style, but rather there still might be an intellectual capacity to grasp the opportunities for strategic transformative change.
Covid-19 and the space for transformative change
While South Africa has been busy coming to terms with the shock of lockdown, two important developments have taken place.
First, the shift towards systemic state intervention to enhance the societal response to Covid-19. Despite the silo approach to governance and competition between Cabinet ministers to shine, and with strategy being about what your ministry can bring to the challenge, some important shifts in state practice are happening in the midst of incoherence and uneven capability.
Announcementsby state armaments parastatals, Denel and Armscor, that they would be repurposing production for ventilators, sanitisers and even converting military vehicles into ambulances is a welcome shift from arms production in a time of crisis.
Such a breakthrough confirms the potential of repositioning these enterprises to also play a part in producing renewable energy technologies and public transport systems for the just transition to avert a 2ºC increase in planetary temperature and bring down South Africa’s carbon emissions.
Minister of Human Settlements, Water and Sanitation, Lindiwe Sisulu,announcedshe would be commandeering all water resources in the country under the control of water boards, water associations and other mechanisms. Through ministerial control she effectively ensured water as a public good was now nationalised in terms of government control.
Minister Sisulu was also at pains to clarify that water used by the government would be compensated. In a water-constrained country, in which 62% of water resources are controlled by commercial farmers, this is a crucial move to ensure the water needs of citizens are met during Covid 19. Her rollout of 41,000 water tanks (only17,631had been delivered by 9 April) and commitment to use schools as sources of clean water for communities is a crucial crisis management intervention, but has to be tracked and monitored by communities. Many of these communities have been denied water due to mismanagement, corruption and failed ANC government leadership, including during South Africa’s drought.
Similar potential exists with integrating public and private health into a functional, affordable and citizen-driven system. But the leadership provided by the minister of health will determine the fate of our post-Covid-19 health care system.
Reframing the role of the state
Nonetheless, all these systemic shifts, actual or potential, are crucial to reframe the role of the state to allocate structural capacities and resources to meet societal needs. More can be done in post-Covid-19 conditions, given the struggles from below, to also ensure these changes bring workers and society into these processes. In other words, we shift from state provisioning to democratic provisioning including democratic public utilities.
But will these shifts endure as we confront the dramatic impacts of Covid-19, economic recession and climate crisis?Or will South Africa merely revert to a financialised market-centred script that has benefited a few corporations and a few wealthy individuals? The battle lines are being drawn right now as we grapple with our post-Covid-19 future. Despite the outcome, what is clear is that the arguments for climate emergency measures have just been strengthened in the midst of the pandemic.
Finance capital is not standing back and is trying to shape a post-Covid 19 world. This relates to the second important development in this conjuncture.
On Friday 27 March, Moody’s followed two other credit rating agencies and downgraded South Africa’s sovereign debt rating to junk. This means the cost of borrowing for South Africa is on its way up and will increase financial stress. These credit-rating agencies are part of a globalised disciplinary complex protecting the interests of globalised finance and the Dollar-Wall Street regime. They do not care what the needs of countries are except to ensure return on capital. They are also dubious and certainly not the bastions of creditworthiness integrity, given they were giving triple-A ratings to Wall Street finance houses before the crash of 2008-2009.
South Africa has been in the grip of global finance for too long and has had to forego its democratic commitments to its people, to ensure the “sovereign interests” of global finance come first. Moody’s and credit rating agency downgrades have laid the basis for austerity macro-economic policy; cutbacks in state social spending and a further squeeze on the precariat coming out of Covid 19.
This will be disastrous. We have to break the grip of global finance on the South African economy now.
In the midst of the global pandemic there is space to break with a one-size-fits-all approach in economic thinking so we can innovate, be bold and heterodox in how we deal with economic and climate challenges. Liberal globalised capitalism and its finance-centred economic orthodoxy has been suspended in this crisis. Credit rating agencies, creditors and multi-lateral institutions and neoliberals in the state will want to bring it back from the dead after the pandemic. This is not going to be easy given the state of the world economy and the challenges facing the three main economic centres that drive global capitalism.
China, US and the Germany-led European Union
China is not going to lead the bounce-back of the global economy any time soon. It went into the Covid-19 crisis with high levels of debt in its financial system, property bubbles, declining trade with the US and even if it uses its surplus ($3-trillion) to launch an expansionary stimulus there is no external demand for Chinese manufacturing, at least for the next few months and possibly for the duration of the pandemic.
China will have to rethink its role as a globalised economy in this context. Also, dependencies built on China for essential medical goods, inputs and other critical manufactured goods are certainly going to be rethought by importing countries, given the prospects of more pandemics and climate shocks. It would be naïve to think a China-centred low-wage manufacturing world is returning after Covid-19.
The US is currently in turmoil and will be the worst impacted Western country by current trends. Trump will realise his wish of making the US great in everything, including Covid-19. On 7 April, the US had more infections (367,650 ) and already had more deaths (10,943 ) than 9/11 (about 3,000 at the Twin Towers).
The US spent trillions on the war on terror (according to Brown University’sCosts of War project almost $6.4-trillion), one of the longest wars in the modern world. Yet Trump and the ruling class are playing partisan games with the Covid-19 response and are merely willing to make modest concessions.
The trillion-dollar stimulus plan, while providing for $1,000 cash transfers to adults and $500 to children is an immediate relief measure, merely about $500 billion. A lot more will go to small business and mainly big business like airlines and shipping for bailouts.
Like 2007-2009, business is going to win again in terms of state support, affirming a neoliberal truism: the people are not too big to fail.
However, the US is still in the upswing of Covid-19 infections, unemployment is skyrocketing, a global recession has kicked in and climate shocks like wildfires in California are coming soon in the summer.
The US has already incurred massive costs due to climate crisis-induced tornadoes (including over Easter weekend in Louisiana) and hurricanes (Harvey cost $125-billion). A few more of these extreme weather events will certainly induce fiscal limits and also challenge the capacities of the US state, in the midst of dealing with Covid-19 or its aftermath.
Quantitative easing, the favourite monetary policy tool of the US state, from printing money to the Federal Reserve purchasing financial securities, is going to face limits with synchronised systemic crisis tendencies hitting at once. Moreover, Trump’s divisive politics also makes the US dollar and US government bonds risky as a safe haven. China might also, given worsening domestic economic constraints, cash in on US bonds to re-adjust its own economy.
Germany, the strongest economy in Europe, is also facing serious challenges. Already in 2019, it was experiencing a slump in economic growth. The steep drop in car exports has placed major stress on one of its leading manufacturing sectors. Massive layoffs of metal workers were instituted and have continued in the context of Covid-19. Retail and commercial industries are also facing massive contractions, bankruptcies and retrenchments.
The stimulus package of the Merkel government is inadequate and still heavily credit-driven, providing a debt-based lifeline to stressed enterprises. The European Union is facing closed borders and an ineffectual European Commission in terms of co-ordinated and effective fiscal policy. Unconventional economic tools, measures and responses are coming to the fore.
South Africa’s Covid-19 state managers have thrown existing fiscal resources, within key institutions, such as the IDC, Department of Agriculture and small business relief funds towards failing businesses. Tax relief and unemployment benefits ( a temporary employee relief scheme) have also kicked in with the UIF making R30-billion available. Just before lockdown theClimate Justice Charter processcalled for stronger mitigation measures such as a substantive basic income grant, together with the trade union federation Saftu. This has also been echoed by the C-19 People’s Coalition.
Many economists and academicshave questioned the lack of stronger mitigation measures and have also called for a citizens basic income grant (BIG) to be considered in the context of lockdown.
What will South Africa be like if a substantive BIG is implemented now?
If South Africa implements a substantive basic income grant during the pandemic, a cash transfer to all citizens of R4,500 per person, per month, and subject to progressive taxation if your income exceeds R20,000 per month (currently South Africa has about 7.6 million taxpayers), these are its implications.
Providing a means to address hunger– about 14 million people went to bed hungry in South Africa in 2019 and we can assume this increased with the suspension of livelihoods when lockdown kicked in. In rural areas, 80% of 700,000 farm workers (plus their families — about 2.5 million people) experience hunger, given the exploitative wages earned (the minimum wage is R18.68 per hour). About nine million children receive a nutritious meal during school, but under lockdown this has been compromised in various parts of the country.
Provide a cushion for unemployment– before South Africa’s lockdown, and based on the narrow definition of unemployment, 5.9 million were unemployed. It is estimated that between 900,000 and three million more workers will lose their jobs due to the lockdown. According to the International Labour Organisation, due to digital technologies, global value chains and other structural factors, unemployment is very likely to go up on a global scale in the foreseeable future. For South Africa, the much-vaunted Fourth Industrial Revolution is certainly a strategy to displace labour.
Handwashing and sanitation will be enabled– about 1.4 million people living in informal settlements do not have access to water in their homes or yards. Almost three million (of 19 million) in rural areas lack access to a reliable supply of water.
End precarity— 2.6 million in the informal sector (and about 60,000-90,000 waste reclaimers, who save municipalities about R750-million a year in landfill costs) and an additional one million domestic workers, are all precarious without benefits including unemployment benefits.
Increase the redistributive bargaining power of labour– by ending dependence on low-wage work. The fragmentation of labour unions has weakened their institutional power to ensure higher wages and non-wage benefits. This was reflected in the minimum wage secured of (R20.76 per hour) R3,653. Other categories without powerful union densities or unions earn less, such as domestic workers (R15.57 per hour) and public works programmes (R11.42 per hour). A higher wage floor based on a BIG of R4,500 and with workers having pooled household income, gives labour greater bargaining power.
Increase household income and fiscal stimulus— South Africa has 18 million very poor households (about nine million in rural areas) that have five members with a total monthly income of R2,600. Many of these households are highly indebted. Social grants mitigate this situation for 17.6 million beneficiaries but not all these households have grant recipients. Moreover, the child-support grant (R445 per month covers 12.5 million children), old-age grant (R1,860, or older than 75, R1,870, covers 3.5 million people) and the disability grant (R1,860 covers just more than one million people) are just not keeping pace with increasing living costs. A family of four needs at least R2,500 per month just to cover food staples. Competing needs for transport and now sanitisers and soaps place immense pressure on such limited resources. More income in households will also have impacts on aggregate demand and kick-start the economy.
Fiscal consolidation– currently the state spends R162.9-billion (2018/2019) on social grants. This is meant to go up to R202.9-billion in 2021/22. The Unemployment Insurance Fund, even after allocating its R30-billion for Covid-19, has R160-billion in investments. A BIG can also be funded through a wealth tax based on income, inheritance and land, as well as a progressive carbon tax on wealthy consumers and carbon-intensive industries. All of these resources can be consolidated together with all grants into one consolidated BIG budget, effectively laying the basis for a “post-work” society.
Institutional rollout— to all South Africans through consolidating biometric information contained in Sassa, SARS, the Home Affairs department (based on identity document data) and from banks. In this regard, either Sassa and/or the Post Office could be crucial mechanisms to achieve the disbursement, including digitally.
Time has come to build an emancipatory future
South Africa cannot continue a lockdown and confront this pandemic without stronger mitigation measures like a BIG. In the midst of Covid-19,Spain is the first countryto commit to rolling out a BIG as a response to the crisis and this will be a democratic systemic reform that will persist beyond the pandemic.
The BIG has a history that goes back to the Enlightenment. In the 2oth century, many experiments and forms of BIG interventions have been tried since the 1970s in the US, Canada, Kenya, Namibia and Finland. Each of these trials were based on specific parameters: target groups, social objectives and levels of income.
All the research shows positive outcomes when assessing the social efficacy for the BIG. This has ranged from more investments in human development, less stress, lower health costs, greater labour market leverage for workers and less food vulnerability. In the context of the climate crisis and deep just transition the BIG is an absolutely necessary democratic system reform to enable the ecological restructuring of our society without harming those least responsible for the problem.
If South Africa does not embrace the BIG in the context of Covid-19, together with other public goods, this will be a serious historical mistake and a missed opportunity for a more emancipated future.
Vishwas Satgar is an Associate Professor of International Relations at Wits University. This article was first published in Maveric Citizen/Daily Maverick.
Covid-19: Treatments, but at what cost?
- Marisol Touraine and Malebona Precious Matsoso
Accessible & affordable medicine: We cannot wait for treatments to be available in high-income countries in order to negotiate prices for the rest of the world.
The World Health Organization (WHO) has sounded the alarm. While we race against time in our own countries, absorbing our resources and energy, we must not forget the world’s most vulnerable populations.
Solidarity is first and foremost a moral duty. All of humanity is affected today, and our prosperous societies would be wrong to abandon the most vulnerable. This moral duty is also a practical one; in the face of a global pandemic, only a global response can be sustainable. A disjointed response would run the double risk of allowing the disease to migrate further or to re-emerge.
Twenty years ago, the certainty that only a global effort could overcome pandemics led to the creation of new organizations, which in recent weeks have mobilized to confront COVID-19:Gavi, which specializes in vaccines, is stepping up its campaigns; theGlobal Fundis enabling countries to use up to five percent of approved grant funding to help protect and treat vulnerable communities (about US$500 million is available for that purpose);Unitaid, which promotes innovative projects that promote equitable access to health care, is investing in diagnostics, treatment and triage tools for respiratory diseases.
But we need to go further.
Traditional development assistance programmes, as indispensable as they are, will not be enough. Initiatives are springing up, all of them useful. We must prepare for the time when treatments and vaccines will become available. But these treatments and vaccines must be accessible to all, everywhere and at the same time.
This is an appeal to the international community.
We cannot wait for treatments to be available in high-income countries in order to negotiate prices for the rest of the world, as happened in the case of HIV. The exceptional circumstances of the COVID-19 pandemic call for an exceptional response. The World Trade Organisation (WTO) Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS, 1995), including those recognized in the Doha Declaration (2001), already allow countries to issue compulsory licences for treatments in the case of pandemics.
We propose to go further.
We ask that governments and institutions currently financing or contributing to the development of drugs, vaccines or technologies for COVID-19 agree from the outset in their contracts with industry to the sharing of intellectual property rights taking into account the urgency we find ourselves in. We are talking about sharing, not giving up. In practical terms, once public money is invested in the race to find treatments for this pandemic that threatens the entire planet, states must demand in return from the outset that companies give up their licences without geographical limitations to a structure that would guarantee the production of treatments that are effective and safe, and – in return for public investment – at affordable prices, everywhere.
This is not a utopian dream.
Ten years ago, Unitaid created theMedicines Patent Pool(MPP), which allows pharmaceutical companies to license their rights on a voluntary basis. This has enabled the production of generics that treat tens of millions of people around the world. Thanks to the MPP, for example, an annual treatment for HIV/AIDS costs less than US$70 in Africa, compared to the US$10,000 it costs in Europe.
Back then we had to wait almost ten years between these medicines being available in high-income countries and their arrival in less well-resourced countries. In the face of COVID-19, we must act now to ensure that everyone, everywhere, has access to treatment at the same time.
This would be a first. The shortage of several important health products and equipment caused by COVID-19 has galvanized and encouraged both governments and industry to cooperate and share technology, and enter into agreements to cooperate and to enable an increase in manufacturing capacity. Already countries including Germany, Chile, Australia and Canada have passed resolutions allowing them to move in this direction.
South Africa itself adopted a policy on intellectual property in 2018 and should prioritize enactment of legislation that allows for the use-all policy tools needed to address urgent public health concerns. Some companies have also said they are ready. The World Health Organization is working to increase transparency of the more than 700 trials ongoing around the world looking into COVID-19 treatments and vaccines.
It is the entire international community that must commit itself and move forward together, in a spirit of solidarity. We call on all the G20 governments and international institutions to make this commitment, along with the World Health Organization. The world needs your dedication to eradicate COVID-19, and to save lives in Europe and around the world.
Marisol Touraine, Former French Minister of Health and Social Affairs, and Chair of the Executive Board of Unitaid. Malebona Precious Matsoso, Director of Health Regulatory Science Platform, Wits Health Consortium, University of Witwatersrand, Johannesburg, South Africa; and Member of the Executive Board of Unitaid. This article was first published in Daily Maverick/Maverick Citizen.
Wits COVID-19 dashboard gets grant award from the IEEE
- Wits University
New features added as inter disciplinary and inter-institutional collaboration data on the pandemic grows.
Wits University’s COVID-19 dashboard has received a grant award by the IEEE. The IEEE is the world’s largest technical professional organisation dedicated to advancing technology. The IEEE has over 400,000 members from all continents. Through its members the IEEE promotes the development of research and technology transfer activities across 40 societies, which span a wide range of disciplines ranging from Aerospace to Vehicular technology, going through computing, electronics, industry applications and many others.
The grant award supports COVID-19-related visualisation and analytics for Southern Africa. The nature of the project is interdisciplinary, where medical data and expertise need to be combined with the wealth of methodologies and algorithms used in advanced analytics, Big Data and Data Science. Assumptions used in the project revolve around our current level of understanding of advanced analytics driven by Data Science and other disciplines. Both main-stream statistical frameworks, frequentist and Bayesian are an underlying assumption to model development. Input from the different medical, virology and custodians of static data pertaining to populations, social and medical vulnerabilities, access to medical infrastructure, prevalence of various relevant pre-existing conditions are also underlying assumptions.
"The project encapsulates methodologies in Data Science and Artificial Intelligence that effectively combine medical and other data to provide a comprehensive synthetic view of the predictive landscape.” says Professor Bruce Mellado of Wits University and iThemba LABS.
The chief goal of the project supported by the IEEE grant award is to control the number of people infected, hospitalisations, ICU admissions and mortality in South Africa and other countries. These outcomes will be predicted as a function of non-pharmaceutical interventions in the post-lockdown period to allow for the economy to reactivate. Analytical and predictive tools developed by these projections will assist policy makers to enact rules and regulations with which to revive economic activity, while preventing a massive outbreak of the virus. This is essential to alleviate the economic impact of the virus in African countries, in particular to slow down the rate of job losses.
This grant award provides various forms of support, including support for the organization of monthly webinars. “These webinars will be hosted by Wits University’s Joburg Centre for Software Engineering (JCSE) and will bring together panels of experts who are actively collaborating and working on the Wits COVID-19 dashboard project, including data scientists, modellers, medical experts and software engineers. The webinars will be open to all and will be advertised shortly,” says Professor Barry Dwolatzky.
Wits University’s COVID-19 dashboard continues to expand. A dashboard for the Gauteng Province has been put in place. Following a successful collaborative model developed with the Botswana International University of Science and Technology, three new dashboards have been launched: Nigeria, Eswatini and Namibia. This takes place in collaboration with local universities and institutions. Collaborative efforts have been established with Zimbabwe, Morocco and Senegal.
Saluting all Witsies combating the COVID-19 pandemic
- Wits University
These Wits heroes represent just a fraction of the clinical, academic, professional and administrative staff, alumni and students responding to this disaster.
The COVID-19 pandemic has disrupted life as we know it. But it has also galvanised our rapid adaptation to change and the adoption of new technologies.
This newsletter acknowledges all those Witsies on the frontline in testing stations, hospitals, laboratories, computer centres, innovation labs and those who from their homes confront this pandemic and its effects on South Africa and the world.
The Wits heroes mentioned here represent just a fraction of the clinical, academic, professional and administrative staff, alumni and students who are contributing in multiple ways to respond to this disaster.
We salute them all.
Practical protection for people
With personal protective equipment (PPE) in short supply globally, Wits engineers and students last week custom designed, manufactured and delivered their first batch of laser-cut face shields to protect healthcare workers. As COVID-19 infections and hospitalisations increase, respiration and ventilation become literally a matter of life or death.
These same Witsies have now turned their engineering prowess to devising assistive breathing devices for patients. We invite you to contributeto this life-saving innovation.
Combatting contamination through biomedical engineering, PhD candidate Michael Lucas pioneered a revolutionary self-sanitising surface coating. This infection control solution helps mitigate hospital-acquired infections and Lucas’ biomedical alchemy can prevent COVID-19 contamination.
Diary of a disease
Understanding the coronavirus pathogen is critical to protection and prevention. In concert with the National Institute of Communicable Diseases (NICD) and the National Department of Health (NDOH), Wits epidemiologists, virologists, biologists, and others at the vanguard of science are working to decode, predict, tame, and suppress COVID-19, and manage the public health and socio-economic impact.
Wits Professor of Epidemiology Cheryl Cohen analyses the distribution, patterns and determinants of disease. Now a household name, Cohen is at the forefront of COVID-19 case-finding, diagnosis and public health response, management and coordination. She recently delivered an on-air COVID-19 masterclass.
Cohen works closely with Dr Kerrigan McCarthy, a clinical microbiologist explaining here how the coronavirus is transmitted:
Amongst the virus sleuths is microbiologist Lynn Morris, a Research Professor in the School of Pathology and the Interim Executive Director of the NICD. Morris explains in this in-depth interview why COVID-19 is one of the greatest challenges of our time.
Predicting and anticipating the trajectory of the virus to mitigate casualties and inform policy requires number crunching, modelling, and analysis of Big Data. Physics Professor Bruce Mellado leads a multidisciplinary team that developed the comprehensive COVID-19 South Africa Dashboard – a data dashboard to help track and visualise local COVID-19 infections, as well as in Africa, and the monitoring tool can be used to provide predictions for the virus’ spread and impact.
“Test! Test! Test!” is the message from Professor of Vaccinology Shabir Madhi, who advocates physical distancing, mass testing for COVID-19, and quarantining the infected as the optimal public health strategy.
Expert analysis informs us of the impact COVID-19 will have on our world but how will our healthcare workers in hospitals cope?
Professor Feroza Motara is the Academic Head of Emergency Medicine in the School of Clinical Medicine at Wits and the Charlotte Maxeke Johannesburg Academic Hospital. She has prepared her team and the hospital to care for those infected with COVID-19. Feroza explains how healthcare workers on the frontline cope.
Physical distancing, hand-washing, and cough etiquette govern our mobility and behaviour like never before. Listen to renowned HIV scientist and activist Professor Francois Venter, Director of Ezintsha and Deputy Executive Director of the Wits Reproductive Health and HIV Institute (Wits RHI), discussing the fundamental role that behaviour change plays in reducing COVID-19 infection.
President Cyril Ramaphosa has appointed Professor Martin Veller, the Dean of the Faculty of Health Sciences to a Ministerial Committee to provide clinical management advice on COVID-19. He, together with five leading Wits professorsproposed a blueprint to replace the current lockdown.
Several other Witsies including Professor Glenda Gray have also been appointed to government committees or sub-committees.
The COVID-19 crisis is first and foremost a health and humanitarian crisis that we are all living through, which is likely to have lasting impacts on how we live.
He explains how we can manage the economic impacts in a way that does the least long-term harm and writes with David Francis, that South Africa won’t flatten the curve unless all citizens have the means to stay home.
Wits researchers and academics across faculties have articulated the impact of COVID-19 in their disciplines and displayed social leadership to educate, advocate, influence, and inspire:
There are numerous other experts from Wits who comment regularly in the media.
Keep informed, safe and healthy
Visitwits.ac.za/covid19regularly for the latest updates, news, analysis and expert opinions in our fight against the coronavirus.
Witsies are tackling the COVID-19 pandemic on all fronts and we laud each and every person who is playing a role in combating this pandemic. We are in a crucial moment in the life of this pandemic and it is important that we work as a collective for the benefit of our society.
We urge all members of the Wits community to heed the words of President Cyril Ramaphosa:
This epidemic will pass. But it is up to us to determine how long it will last, how damaging it will be, and how long it will take for our economy and our country to recover. It is true that we are facing a grave emergency. But if we act together, if we act now, and if we act decisively, we will overcome it.
Toward a risk-based strategy for managing the COVID-19 epidemic: A modelling analysis
- Alex van den Heever
Given the protracted nature of the risk posed by the COVID-19, this paper seeks to address the need to match health prevention and a viable economy.
The central premise of this paper is that there are no zero-sum options. By this it is meant that the health prevention strategy most compatible with the maintenance of continued economic activity is an unavoidable policy imperative for South Africa.
This paper addresses this discussion in three stages. First, it examines the factors that should influence the main strategic choices. Second, it examines the consequences of two alternative pathways leading to a preferred approach. Third, it offers an overview of the key features of a preferred approach.
The paper engages with the above through the use of a model (van den Heever, 2020) which attempts to compare alternative health prevention strategies. As a consequence, part of this paper involves a brief write-up of the methodology used.
Introduction
As yet, there are no proven formula to balancing the effort to fight the Covid-19 pandemic with the simultaneous and equally important need to sustain livelihoods and keep open pathways to economic participation. Whereas these objectives are sometimes argued to be in opposition –save lives versus save the economy– crude distinctions are not helpful when facing the complex set of risks implied by the prospect of a protracted struggle to contain the epidemic.
In the absence of a cure or a vaccine, disease prevention approaches need to find ways to separate the infected from the uninfected members of the population. When interventions occur late, the intervention options narrow considerably to cruder forms of social separation, such as lockdowns. If caught early, however, mass testing coupled with rapid contact tracing offer surgical approaches to separating the infected from the uninfected.
As a preventive strategy for COVID-19, according to emerging experience, mass testing and contact tracing should occur together with social distancing measures, border closures and the observance of health protocols (such as the requirement to wear masks when outside the home) where people cannot avoid some form of social contact. The distinction between the lockdown approach and mass testing and contract tracing is that the former shuts down a substantial part of the economy while the latter is compatible with continued economic activity.
This distinction is an important consideration where the direct effects of a lockdown disproportionately harm vulnerable workers and businesses. While Government can attempt to support the vulnerable, the extent to which this is possible depends on whether the institutional mechanisms exist to identify compromised individuals and businesses sufficiently for them to be supported. It also depends on the length of time for which support is required. The longer the period, the harder it is to keep businesses open, and the harder it is to raise the tax revenues and the debt required to finance support for vulnerable individuals.
In the early phases of the COVID-19 outbreak, it is clear that Government lacked the capabilities to introduce the most effective strategy. The need for urgent action left no opportunity to scale up the measures required to prevent an exponential increase in infections. South Africa was just not geared for an epidemic of this nature. Consequently, the 21-day lockdown implemented on 27 March 2020 was appropriately timed and self-evidently essential.
The extension of the lockdown for a further two weeks however raises important concerns. Two implications can be drawn. First, the extension suggests that the lockdown period has not been adequately exploited to ramp up the testing and contact-tracing regime. Second, it indicates that the narrow testing regime adopted to date (designed to merely identify imported infections rather than community-based outbreaks) cannot be relied upon to confirm whether the lockdown has succeeded outside of the affluent communities where the epidemic started.
While the two-week extension could be argued to provide some breathing space for the implementation of the preferred strategy of mass testing and contact tracing, any continued failure to put in place the required machinery will result in incremental extensions to the lockdown with all the economic and social consequences that will go with it.
An obvious further concern with this trajectory is the high likelihood that a successful lockdown within the South African context is essentially a leaky bucket. While it may prove effective in the more affluent suburbs, it may fail in the townships and informal settlements. The current lockdown may have therefore only reduced, but not prevented, the spread of the disease into the general population. Although these infection levels may be relatively low at present, it won’t take long for them to become uncontrollable.
Background
The pandemic resulting from the SARS-COV-2 virus has elicited an emergency response from virtually all countries around the world. The high levels of transmission, taken in this analysis at 2.5 (over a period of four days)[1]for every infected person, would not be a serious concern if the disease (COVID-19) did not also result in sufficient severity for a proportion of the infected population to require hospitalisation, and, more importantly, access to ventilators that are typically only located in intensive care units (ICUs).
Where ventilators are not available for those who need them, the health outcome will be death. For those that require access to ventilators and obtain treatment, over 70% will in any case die. Patients who develop severe symptoms appear to be associated with weaknesses in the immune system, either due to age or co-morbidities typically correlated with age (hypertension, diabetes, and various cardiac conditions). People with co-morbidities associated with the respiratory system are also at risk regardless of age.
Given this context, to avoid significant preventable levels of morbidity and mortality, the most efficient approach to reduce the spread of the disease is to reduce the reproduction rate of the disease (referred to as R) from 2.5 to below 1 (the rate at which the disease will ultimately be eliminated). This is achieved through various interventions, the most effective being the introduction of a vaccine to a sufficient number of the population such that herd immunity is achieved.[2]
Where a vaccine is not available, and the mortality would be too high to permit herd immunity to occur naturally, the only option is to actively interrupt the spread of the disease from person to person such that R is held below 1 for a long enough period to eliminate the disease. Quite simply, such strategies involve keeping infected people away from uninfected people.
There are two broad options. Either infected people are identified quickly and isolated; or, where infected people have not been identified quickly enough, everyone is separated from everyone else for a sufficient time for the disease to self-eliminate. In practice strategies involve a mix of associated interventions.
Internationally, two distinct approaches have emerged. The first is to test, trace and quarantine at scale. The second, involves a generalised lockdown on the movement of people. The first option tends to be exercised by countries that are well-prepared and intervene at scale at early stages of the epidemic. The second, tends to be applied where countries are poorly prepared to react, and a runaway community-based epidemic is well underway before interventions are considered.
South Africa’s response to the emerging pandemic was slow at first, with no border closures considered, and only very basic forms of border screening applied at airports. Given that we knew early on that many infectious persons are also asymptomatic, this approach was ill-advised and exposed the country to the inevitability of imported infections.
This (arguably) casual response to the emerging pandemic changed when the first cases were diagnosed in South Africa in early March 2020 and also where it had become evident that many other countries were experiencing full-blown epidemics arising from imported infections.
Evidently informed by standard epidemiological modelling of the emerging epidemic, aided by a wealth of information collated by international researchers and the World Health Organisation (WHO), the South African government acted immediately to implement social distancing, followed on 27 March 2020 by a generalised lockdown. However, as the modelling has never been made public, it is unclear what scenarios were presented. Needless to say the analysis was clearly compelling at the time.
The lockdown was however implemented at an early stage of the epidemic, as there was very limited evidence at the time of a generalised community-based outbreak.[3]This differs from some other countries where lockdown approaches were introduced only when they had lost control of the epidemic and they were all out of options.
However, the countries that avoided lockdowns and managed their epidemics did this through rapid border closures, the rapid development of tests for the disease, generalised testing with rapid turnover (12 to 24 hours), contact tracing and quarantining of infected individuals.[4]Broadly speaking their approach can be characterised as getting ahead of the disease rather than chasing it.
Consistent with countries that have not been able to manage their epidemics, South Africa also adopted the testing regime characterised as “chasing the epidemic”. It did not test the general population, or even those with mild symptoms. Instead it tested only people who had travelled internationally (when they came forward voluntarily), had contact with a traveller or had contact with someone diagnosed with COVID-19. This effectively blinded the testing regime to community-based outbreaks. In addition, the testing programme was so constrained that the public sector had only performed 3% of the total tests, with the remainder performed by the private sector. This has apparently changed, with more generalised testing on the increase, although still low.
So what does this mean for South Africa’s strategy going forward?
First, we are left without a clear measure of the success or failure of the lockdown. On the one hand we cannot fully trust the incidence reports. On the other hand, the mortality levels appear consistent with a contained or low-level epidemic.
Second, the economic consequences of a lockdown are so large, that it cannot be relied upon as the principle prevention strategy if the epidemic is protracted. This requires that a health strategy compatible with reopening the economy is imperative.
Third, the public reports on readiness by the public health team to implement a benchmark strategy are unclear at best, and suggest undisclosed challenges regarding readiness. The question is whether the bottlenecks to a more nuanced strategy can be rapidly addressed.
How effective is a generalised lockdown?
Of considerable concern is the possibility that a generalised lockdown approach applied within the South African context will only be successful in relatively affluent communities, with townships “unlockdownable”.
As mentioned above, the testing protocol applied to date has been biased toward (implicitly) measuring the (imported) outbreak in affluent communities. The publicly reported new infections would therefore accurately reflect the lockdown impact on the relatively affluent population, but not on outbreaks in the general population.
The apparent containment of the epidemic in affluent communities is therefore potentially misleading. It can create the impression that the lockdown is working (false evidence of success), but it may equally fail to offer the required evidence that a generalised lockdown cannot work successfully in South Africa (false evidence of failure).
As the outbreak in South Africa derived from the affluent population, as they tend to travel internationally, the initial lockdown was probably the best available strategy to block transmission from the affluent communities to the population at large. However, to the extent that the population at large has been infected,a general lockdown may prove equivalent to no intervention.
As a form of contingency planning for the South African context, therefore, the following should be noted:
A lockdown may be a viable prevention strategy, but different approaches would be required for different contexts (i.e. what works in relatively affluent areas may not work in townships or informal settlements); and
An undetected outbreak may have already occurred in the general population which is invisible to the current testing regime (noting that there are significant moves to expand the testing protocol and programme).
Given the need for a “must not fail” health prevention strategy, it makes sense to prepare for what will work in all scenarios, rather than an approach which will only workif we are very lucky.
Strategic options
Important considerations
There remains considerable uncertainty as to whether the pandemic can be completely eliminated during 2020. Strategies that are successful in bringing country-level epidemics under control therefore face the realistic prospect of a resurgence for an extended period of time. Within the South African context this requires that effective containment of the epidemic will require public health interventions of one form or another throughout 2020.
The need to maintain public health interventions for such an extended period of time therefore has important implications for the design of the 2020 strategy. A brief public health crisis addressed through emergency interventions can be expected to have a different design to a protracted affair. However, if the state of readiness is not adapted to reflect the protracted nature of the crisis,the strategy may unwittingly default into treating the protracted crisis as a series of brief crises.
Two clear strategic options emerge. The first defaults back to generalised lockdowns when surprised by a resurgence, and the second actively manages all the risks associated with a protracted epidemic.
Option 1–Lockdown dependent approach, where the lockdown is extended on some basis after the 35-days as the central pillar of any response to contain the epidemic; and
Option 2– Risk-based strategy, where a prevention strategy compatible with the local domestic social context and a safe re-opening of the domestic economy is pursued.
A brief description of the methodology required to model the above two options is outlined below.
Method
Approach
The options are examined using a model, theCOVID intervention model(van den Heever, 2020), to determine the length of time a particular public health intervention package needs to be in place to keep the local epidemic controlled for the entire 2020 period.
Generating parameters from international contexts
This section examines the trajectories of various country epidemics following the introduction of major prevention strategies and uses them to calibrate the model. First, a range of countries are reviewed to identify those that may exemplify particular interventions. Second, from those countries two are selected, that best reflect a lockdown intervention and a mass testing and contact-tracing intervention.
The selection criteria for the group of countries was based on: those with significant epidemics (United Kingdom, Italy, Spain)[5]that are engaging in lockdowns; countries that have experienced significant epidemics and have successfully contained them using lockdowns (China); and countries that avoided lockdowns through early interventions that made substantial use of mass testing and contact tracing (South Korea).[6]Data on new infections is examined in each country after the first 100 cases.[7]
An attempt is made inFigure 1to compare all five countries.
The patterns for the three European countries are strikingly similar on the upward trajectory. As the countries are at different stages in their epidemics, only two of them, Italy and Spain, show a downward trajectory after the introduction of the lockdown. The United Kingdom is yet to reach a turning point (at the time of writing this brief). The post-lockdown downward trajectory for China is however a lot steeper than Italy and Spain, and is as steep as that achieved by South Korea using mass testing and contact tracing.
The lockdown trajectories for Spain and Italy are consistent with a relatively high R, although still less than one. The implied intervention Rs for South Korea and China are however more pronounced. It should however be noted that the both Spain and Italy intervened at a very late stage in their epidemics, which may have complicated their outcomes in ways that are not yet understood. With China, there is a question concerning the reliability of their reporting.[8]As a consequence, for the purposes of parametrising the model, it makes more sense to use the more conservative trajectory consistent with either Italy or France. As Italy effectively has a longer time series, it is therefore preferred over France for this purpose.
Figure 2illustrates the Rs that best match the Italian epidemic, both before and after the lockdown intervention. Here different values of R are used to drive a model result that is close to the actual trajectory of all phases of the epidemic. This suggests that a lockdown in cold weather is broadly consistent with an average R of 0,96. The early stages of the epidemic are consistent with an R of 1.98, dropping to 1,58 as a consequence of initial, but inadequate, interventions. The lockdown R is however quite close to 1, suggesting a fairly tenuous impact.
An estimate of the R consistent with the South Korean mass testing and contact tracing intervention is provided inFigure 3. The period prior to the main public health intervention is consistent with an R of 1.6, while the mass testing and tracing intervention results in an R of 0.7 in cold weather. This is a superior result relative to protracted lockdowns in Italy and France. This could be the result of many factors, such as,inter alia, the early stage of the intervention and the efficiency of a well-prepared country response. It is therefore possible that other countries may not implement the same response with the same efficiency. This is however not taken into account in the parametrisation for this exercise.
The intervention packages used by both Italy and South Korea however extend beyond lockdowns and mass testing and contact tracing. For instance, all include border closures, social distancing requirements (including requirements to wear masks when outside the house) and targeted lockdowns (to address disease clusters). The intervention packages generated through the parameterisation exercise take this into account. This is discussed further in the next section.
Model parameters
This section provides an indication of the model parameters used, guided by the analysis of Italy and South Korea discussed above.
The model parameters are specified at three levels. First there are individual interventions, each with an associated reduction in R (Table 1).[9]Second, there are combinations of interventions, or packages, each resulting in an aggregate R (Table 2). Third, there are scenarios over the 2020 period, where different packages are applied by day of the year, depending on the seriousness of the epidemic.
It is important to note that the Rs for the individual interventionsdo not have a strong empirical basis. The true test of their usefulness is therefore how well they match the South African epidemic thus far when combined within packages of responses (i.e. no intervention occurs in isolation of some others). To the extent that they do, they can be used to estimate the trajectories resulting from different packages over the full 2020 period.
As indicated inTable 2there are five overall response levels provided for, from level 0 (L0) (do nothing) to level 4 (L4) (lockdown). There are two versions of each response level depending upon whether or not it occurs in warm or cold weather conditions.
For the purposes of this analysis the package configurations associated with a general lockdown (L4) and mass screening and contact tracing (L3) reflect the outcomes in Italy and South Korea respectively discussed above.
Mass screening and contact tracing is treated as a level 3 (L3) intervention as this is naturally prior to the full lockdown – at least for countries with well-prepared public health response systems. South Africa’s adoption of a level 4 (L4) response before level 3 is assumed to have occurred because it was not prepared for the epidemic and was therefore not in a position to implement mass testing and contact tracing in the natural sequence of escalating responses.
The application of the parameters to the South African epidemic
This section discusses whether the parameters developed for the model are able to predict the known part of the South African epidemic.
Figure 4illustrates how interventions associated with assumed reproduction rates (R) generate estimates of new infections for the periods where we have reported information on new infections.
Three intervention packages are applied to specified periods broadly in accordance with actual events.
First, there is the “limited intervention” from the early period of March 2020 to around 22 March 2020, which has an R of 2.2.[10]Here it is assumed that no meaningful public health prevention intervention is in place. The value of R is reduced to account for the warmer climate.
Second, there is stepped up “social distancing” (referred to above as a level 2 (L2), or “intermediate”), which occurs from 23 March 2020 to 26 March 2020, with an associated R of 1.6.[11]This period includes the closure of international borders, schools and universities.
Third, is the 27 March 2020 “lockdown” intervention package, which has an associated R of 0.7 (which is lower than that for Italy to account for the warmer weather). The lockdown period includes the social distancing interventions and border closures. It therefore has the deepest overall impact.
Figure 5shows that the warm weather andsocial distancinginterventions on their own do not bring R below 1.0 (the rate at which the disease will dissipate). The R of 1.3 for this period therefore appears justified.
The lockdown intervention does however appear bring R to below 1.0, apart from the most recent reported infection data. There is therefore some uncertainty about the trajectory of the lockdown. Whereas during the initial period of the lockdown the reported new infections went into decline as expected, the trend from 29 March onward could be regarded as ambiguous. While the model suggests a more pronounced decline, the actual trend could be consistent with a range of Rs from 1.0 to 0.6.
One possible interpretation is that the lockdown, in context, is not sufficient to eliminate the disease. Consistent with this possibility, this trend (i.e. relatively flat after the initial decline) could reflect a transition from theimported outbreakin the affluent community to adomestic community-based outbreakin the general population. While the former may be sensitive to a lockdown, the latter may not, with an R greater than 1.0even with the lockdown. This period could therefore reflect a simultaneous decline of one outbreak with an increase in another.
Nevertheless, based on information to date, and using the data from the Italian epidemic, an assumed R of 0.7 for a lockdown with warmer weather appears (for now) consistent with the reported information. Using the model to estimate the effectiveness of the Italian lockdown produced an R of 0.96 for winter. The 0.7 assumption used for South Africa includes an adjustment for warm weather and is therefore only applied to the remaining days of summer. The cold weather assumption is applied during winter.
Scenario results – options for 2020
Overview
Two scenario options for 2020 are examined here. Option 1 involves a lockdown-dependent strategy, where any surge in the epidemic involves the package associated with a general lockdown (L4). Option 2 however limits the use of a lockdown to the period already designated for lockdown in South Africa. Thereafter, it reverts to periods of mass testing and tracing (L3), with periodic reversions to L2 (intermediate interventions). Both options are required to eliminate the risk of a serious epidemic during 2020.
It is important to note that the model results are stylised reflections of the trajectory of the epidemic and unknown real world factors would also be expected to play a role.
Option 1 – Lockdown-dependent strategy
In this scenario option the lockdown is permitted to end from 1 May, with a reversion back to an intermediate intervention package. However, according to the model, the disease resurges and requires a further lockdown toward the end of May, extending all the way to October (Figure 6). During October an intermediate package is implemented. A further lockdown of 16 days is required in November/December to prevent a further resurgence. The required overall number of days for lockdowns is 193 days.
The headline results, reflected inTable 3, are consistent with an overall strategy that keeps the epidemic in check for 2020. In total 29,046 people test positive with mortality of 439. The demand peak for ICU beds (used as a proxy for ventilators) is 175, which would be well within the capability of the overall health system. There would only be a slight risk of insufficient High Care (HC) beds in the public sector. When seen together with the private sector capacity and the timely reorganisation of public sector beds, there are sufficient beds.
Option 2 – Risk-based strategy
The risk-based strategy looks to minimise the use of lockdowns as the primary measure required to bring the epidemic under control. Although it retains the lockdown as implemented to date from 27 March to 30 April, it moves to an aggressive mass testing and contact-tracing regime thereafter. This lasts until the epidemic is brought under control. In total there are 35 days of lockdown, 184 days of mass testing and contact tracing and 61 days of the intermediate package. (Figure 7)
The headline results shown inTable 2reflect the total containment of the epidemic, with only 2,595 people infected and total mortality of 39. It should be noted that the actual trajectory of the disease could take the overall totals over these numbers by the end of April. These estimates should therefore be treated as indicative of a direction rather than offering a predicted outcome with a high level of specificity. This scenario indicates that bed demand is kept low, and no crisis of access to critical care beds would materialise. The demand for ICU beds peaks at the relatively low value of 43, with High Care at only 63.
Discussion of results
Both options modelled contain the epidemic, and, to that extent, reflect equivalent levels of success in the management of the health crisis. The differences in headline results (reported inTables 3and4) should be disregarded, as they reflect an artificial structuring of option 1 – to fit a pattern of reverting to lockdowns when the disease resurges. Option 1 could also be structured without significant resurgence. This would however require a slight increase to the number of lockdown days.
The main result from this exercise is the number of days required to control the epidemic in 2020 using lockdowns as the primary intervention package. In total, the requirement for 193 days in 2020 is significant, and raises serious questions about the sustainability of this approach as the default strategy. While an economic analysis would provide concrete information on the implications for South Africa’s gross domestic product (GDP) of option 1, it is self-evident that this option would be ruinous.
The model indicates that the epidemicwillresurge after a lag when the most effective interventions are withdrawn. In the real world, a resurgence would occur if merely one asymptomatic positive case was left in the community, or where a failure to eliminate the pandemic internationally resulted in a single undetected imported infection. In the former instance, the resurgence would be expected to be faster than the model suggests (as the model trajectory escalates based on fraction of a residual single person).
Given the protracted nature of the public health risk, the analysis suggests that an economically viable health prevention strategy will be required for most of 2020. As the implications of option 1 cannot be shouldered by the South African economy, the selected health strategy should be designed to be compatible with as broad an opening of the economy as is possible. Under these circumstance, a strategy broadly consistent with option 2 appears necessary. The specific features of such a strategy are broadly outlined in the next section.
Features of a risk-adjusted strategy
Overview
The COVID-19 epidemic poses a complex set of risks for South Africa over-and-above the morbidity and mortality associated with the disease itself. The knock-on effects of border closures, restricted movement and closed businesses, if not well addressed, will have long-term consequences for the economy.
While it could be argued that economic considerations should not be given precedence over health risks, in reality economic failure on the envisaged scale will have serious short- and medium-term implications for society at large, well before we get to the long-term. Shocks to employment levels will shift many into poverty, including many who were on a pathway out of poverty.
While Government could provide an economic bridge for some (but not all) where the periods of economic closure are limited, protracted lockdowns and business closures will result in a fiscal death spiral, with tax revenues falling precipitously while expenditure commitments rise precipitously.
The only viable pathway out of the COVID-19 crisis is therefore to integrate the health and economic strategies into a single all-of-government approach. This requires a total strategy of Government – one that is weighted proportionately to address the principal risks facing the country at this time.
There are five strategic considerations to such an all-of-government risk-adjusted approach.
First, the health prevention strategy must be organised with two objectives in mind: first, it must be compatible with an opening of the economy; and second, it should be designed to have positive economic spinoffs.
Second, social programmes aimed at income protection, such as social grants and unemployment insurance, should be implemented at scale to simultaneously address social protection needs and the need for domestic economic demand stimulation.
Third, non-health-related economic strategies need to address the shocks to both the demand and supply sides of the domestic economy.
Fourth, those parts of the strategy that require ongoing rapid decisions and the deployment of resources need to be supported by an all-of-government command structure that is fit-for-purpose.
Fifth, all parts of the strategy require rapid feedback on performance and constant useful public communication.
Once the only viable strategic approach has been determined by Government,it has to adopt it together with all the associated interventions with a high degree of urgency, commitment and adaptability.
An indicative approach to the health prevention strategy
This section provides a brief overview of a strategic approach to the risk-adjusted health prevention strategy. This involves a five-level response framework, a post-lockdown approach, transparency requirements and the achievement of operational integrity.
Five-level response-framework: Consideration should be given to a formalised five-level response framework for this epidemic and all future epidemics. The lowest level would be activated when an epidemic risk is identified. A set of pre-prepared responses would then be triggered. Each subsequent (triggered) level would involve increases in risk and urgency. A lockdown would only be considered as a last resort (last level) if the interventions in the previous levels fails to cope.
South Africa should have had a level 3 option, mass testing and contact tracing, but was not adequately prepared. As a consequence, arguably two levels were skipped, at great cost to the economy. While this may be seen as a long-term issue, it is relatively easy[12]to implement in the current crisis, and would prove to be a useful tool for decision-making in 2020. This is because there may be a need to move up and down levels all through the year depending on the success or failure of a response level. These movements up or down could also be area or cluster-specific, rather than seen purely at a national level.
Level 0:Routine surveillance of risks. When there are no threats, redundant capacity in infectious disease responses needs to be readied. This can involve: the identification of quarantine sites; the maintenance of contact-tracing machinery; and the preparation of a legislative framework for infectious disease outbreaks. This legislation should, inter alia, cater for emergency test development, requisitioning of equipment, rapid contact-tracing frameworks and preparations for mandatory quarantining of suspected and confirmed cases. Both public and private hospitals should be required to maintain a minimum number of isolation wards.
Level 1:Trigger – identification of a threat, by which is meant a highly infectious disease with significant morbidity and mortality. This may involve: the implementation of a central response platform for Government; the development of tests; the identification of possible shortfalls in testing equipment; the preparation of treatment facilities; the maintenance of basic border surveillance; the identification of high risk transport routes; mandatory testing and quarantining for people from high risk zones; the establishment of testing machinery for all persons presenting with symptoms; and where no test has yet been developed, suspected cases should be quarantined for appropriate periods. In all this, it would be important to coordinate with the private health system to agree on aspects that require a joint response.
Level 2:Trigger – imported infections identified together with first community-based infections. This would involve: border closures, together with mandatory across-the board testing and quarantining of travellers entering the country; the mandatory wearing of masks (if the disease has an airborne elements; mandatory social distancing; and mandatory (pre-prepared) health protocols implemented at workplaces, transport hubs and bulk transport; the temporary closure of schools and universities; the prohibition of mass meetings of any form (funerals, church gatherings, etc.); and an expansion of the testing framework to be able to detect community-based infections.
Level 3:Trigger – significant increase in community-based infections, but below 100. In addition to the level 1 and 2 interventions, implement mass testing and contact tracing, together with the quarantining of suspected cases and those identified as positive. This testing regime supplements the testing of suspected cases introduced from level 1.
Level 4:Trigger – community-based infections continue to increase exponentially. This would involve: general lockdowns initiated in areas with identified disease clusters; the closure of all non-essential businesses; and the closure of all bulk transport systems.
Post-lockdown health strategy: It is imperative that from 1 May 2020 South Africa is ready to implement a health prevention strategy that allows for a measured and safe movement from a level 4 response framework to level 3. The key elements of this approach could be expected to include:
Mass testing and contact tracing. This needs to be complemented with the rapid identification and follow-up of outbreak clusters.
All laboratory results must be available within 12 to 24 hours after the test.
Ambulances need to be in place for the transportation of confirmed cases.
At all times doctors, nurses and paramedics working in clinical areas should wear three layered surgical masks as well as gloves. Where close contact with patients are anticipated, full PPE is required, including N95 masks.
Health protocols must be developed for all organisations. A compliance framework to ensure adherence is also required.
Health protocols are required for all transport hubs and all forms of mass transport.
Health protocols are required for all places of education.
A distance learning framework needs to be developed for scholars without appropriate access to the internet and online teaching platforms.
Health protocols are required for social grant collection sites. This includes sites for food parcel distribution. These are also appropriate sites for mass testing and the distribution of masks.
The general public requires access to basic methods of personal protection. This includes hand sanitisers, masks (reusable) and gloves.
During the entire period of the emergency, it should be mandatory for all to wear a mask outside of their homes.
Transparency
The successful pursuit of a public health strategy relies on a high degree of voluntary consent to comply with appropriate public health measures as well as personal preventive conduct. In addition, researchers and businesses constantly need to make sense of the epidemic. This requires that detailed information on the trajectory of every aspect of the epidemic needs to be made public. Furthermore, the actions taken by Government need to be justified through the disclosure of the information upon which major decisions are made.
Operational integrity
An epidemic is a moving target which requires a whole-of-government response. However, the platform established to make rapid decisions needs to be fit-for-purpose and regularly reviewed. It is presently unclear how effective the current command structure is. In particular, whether it is able to constantly adjust to changing circumstances and configurations of risk and priorities.
Conclusion
This brief has provided an overview of the possible trajectory of the COVID-19 disease in South Africa under different intervention scenarios using an intervention model. The purpose of the modelling approach is to support decision-making in the face of the complex set of risks facing the country in 2020, and possibly beyond.
The modelling analysis suggests that it is unlikely that the disease will be eliminated as a risk in 2020. Given the protracted nature of the emergency, the public health strategies need to be designed to be compatible with continued economic activity.
Were South Africa to rely exclusively on lockdowns to contain the epidemic, a total lockdown period of 193 days may be required. This assumes, however, that lockdowns actually work in the South African context. At this stage it cannot be confirmed that the lockdown approach works in the densely populated informal settlements and townships. A total lockdown period of 193 days is however inconceivable from an economic perspective, and an alternative risk-based approach is therefore appropriate.
A risk-based approach seeks to manageallthe risksassociated with the epidemic, and not only the disease itself. The current health strategy places the economic welfare of more than 70% of the population in jeopardy, with Government only in a position to provide remedial support to only a subset of the group at risk of destitution. The sustainability of the programmes of support also ultimately depend on the sustainability of government finances, which in turn depend on the existence of a working economy. A lockdown-dependent strategy substantially erodes the ability of Government to bridge the social and economic impacts.[13]
Given this, strategic decisions are required at this point in the emergency which favour a risk-based approach rather than a lockdown dependent approach. However, a risk-based approach requires that the groundwork is properly laid. It is far from clear, however, that this necessary work has been done. But there is stilltime. But much depends on what use is made of the limited time.
Liu, Y., Gayle, A. A., Wilder-Smith, A., & Rocklöv, J. (2020). The reproductive number of COVID-19 is higher compared to SARS coronavirus.Journal of Travel Medicine, 27(2). doi:10.1093/jtm/taaa021
van den Heever, A. (2020).COVID-19 Intervention Model for South Africa.
Zhang, S., Diao, M., Yu, W., Pei, L., Lin, Z., & Chen, D. (2020). Estimation of the reproductive number of novel coronavirus (COVID-19) and the probable outbreak size on the Diamond Princess cruise ship: A data-driven analysis.International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases, 93, 201-204. doi:10.1016/j.ijid.2020.02.033
[1]There are numerous attempts to estimate R for COVID-1 (Liu, Gayle, Wilder-Smith, & Rocklöv, 2020; Zhang et al., 2020), Estimates do range from below 2 to around 3. The baseline assumption used in the report is merely used as the point-of-departure for assumed reductions in R due to interventions.
[2]This is where immunity levels are sufficiently high that R is always significantly below 1.
[3]The number of infected individuals totalled only 1,170 on 27 March 2020 when the lockdown began.
[5]The United States was excluded as the lockdown is incomplete (or partial) and the peak of the epidemic has not been reached. It therefore cannot assist in the development of parameters for the model.
[6]Note that the South Korean data inFigure 1is presented on a different scale to that for the other countries. This is because the size of the epidemic in Korea was far less than for the other countries, making it difficult to compare them side-by-side.
[7]The data source for international trends was from (European Centre for Disease Prevention and Control, 2020).
[8]The new infection data from China reflected so many inconsistencies however that it was necessary to smooth its upward trajectory. The new infection data from China has also been adjusted to iron out clear timing errors in reporting. This involved developing a linear equation for a period of apparent consistent reporting and extrapolating for the period of inconsistent reporting. The total number of infections was however retained. Only the trajectories were smoothed.
[9]These reductions in R effectively work back from the overall R totals developed using the Italian and South Korean epidemics.
[10]The 2.2 assumption is lower than the assumed average in cold climates of 2.43. The reduction from this baseline of approximately 0.3 is to account for the warmer climate at this time in South Africa.
[11]While this is shorter than the official intervention period, it is assumed that actual social distancing occurred with a lag of a few days.
[12]This is however subject to the release of public information indicating whether there are any fatal bottlenecks to the timeous expansion of testing to the scale required to manage the epidemic.
[13]It is worth noting that conventional views of deficit-financing rescue packages don’t fully apply to the current economic situation. The indefinite closure of businesses raises the uncomfortable prospect that the sale of government treasury bills could dry up – leaving the Government in a state of default. Virtually every revenue source for Government is compromised by a lockdown. Maintaining a posture of uncertainty regarding future lockdowns clearly places government finances in an untenable position. It should also be noted that industrialised countries can withstand these circumstances for a far longer period than South Africa.
Professor Alex van den Heever holds the Chair in the field of Social Security Systems Administration and Management Studies at the Wits School of Governance. This paper has been published in full on Maverick Citizen/Daily Maverick.
Numbers can kill: politicians should handle South Africa's coronavirus data with care
- David Everatt
We’d all love to know more about our neighbours – from COVID-19 data, census data and other official data sources – but we shouldn't.
Numbers tell stories. Usually, stories of people – often happy stories, like births, marriages, finishing school, getting a degree, getting a job. Even paying taxes. Sometimes they tell sad stories – death, divorce, disease, liquidations.
Statistics do not provide a cold or inanimate way of dealing with the world – they are one key part of the world, waiting for someone to spin the tale they tell.
At a time of heightened fear such as the world is currently living through, ensuring statistics of death and disease are handled with sensitivity should be self-evident, most particularly to politicians.
It appears not.
No one controls who talks to data once they’re in the public domain. No one stops journalists or students or politicians from analysing official stats as they see fit, thus creating their own narrative. That is why there are clear ethical and legal protocols in place.
The most basic of these is never to release data that may allow respondents to be identified.
In the case of South Africa this means that, in practice, Statistics South Africa (Stats SA), the country’s national statistical service, anonymises data it does release and has legal rules for the “level” at which data can be made available. This refers to both individuals and small, identifiable communities.
This is appropriate. It prevents the potential violation of confidentiality – the ability to point accusatory fingers because you choose to read (or misread, exaggerate, over-state) numbers in a particular way.
But is this basic protocol being adhered to during the COVID-19 pandemic?
Sadly not. An early case in point is the Western Cape, where premier Alan Winde released remarkably detailed figures on the local level sites of COVID-19 infection in the province.
Today (March 29) we have started providing sub-district information across the Western Cape, including in the city of Cape Town. The stats show us that this virus is spreading, reaching communities across our province. Each and every one of these cases, from Khayelitsha and Mitchells Plain to Mossel Bay — is of very serious concern for my government.
He went on to give detailed data for the Cape. Winde’s example has since been followed by other premiers, mayors and many others. This is not a party political point-scoring piece.
The obvious question is: why tell us, at such granular level?
Winde was no doubt acting from good intentions, one most people would share, which is that the more information people have, the more they may appreciate risk, and the better they may respond to the constraints of the COVID-19 lockdown.
Police monitor compliance with COVID-19 regulations in the Diepsloot informal settlement, Johannesburg.Michele Spatari/AFP/GettyImages
And, quite rightly, he was trying to put out the flames of potential stigma – as every politician subsequently repeats as they intone the nightly death toll. He and others have tried to say the disease knows no race or age or class. It can get anyone.
But the path to hell, as we know, is paved with good intentions.
The politics of death
When the first South African COVID-19 infection was reported on 5 March, almost immediately a video was circulated by some political figures that made it clear this was a rich white problem. Who else visits Italy in March?
It pointed to the immediate racialisation of the first South African infection. This was a disease of white globe-trotters. This was a problem for rich whites, not for “us” (mainly poor black people). It fed on the political discourse that marked the 2019 election – “protect our borders” (from “them”), take back “our” land and jobs (from a different “them”).
COVID-19 is everyone’s disease as well, as people are grudgingly accepting. But the race and class profile – of this being a problem for rich white people, that started with South Africa’s infection #1 – created a discourse that has not disappeared. It is fuelled by the country’s existing racialised inequality and people’s genuine fear of this invisible virus.
The release of data showing that “rich white” suburban parts of Cape Town and Johannesburg are the epicentres in both city and province is problematic. It feeds into and amplifies South Africa’s tendency to default to race, and creates real local divisions that mirror and deepen those already hardcreted into South Africa’s cities by apartheid spatial engineering.
Controlling the narrative
But why did stigma exist (and why so early)?
In no small part, because government didn’t control the narrative from day one. As a result, every session now includes the repetition that the virus cares not a jot for race. But, though government spokespeople also reassure South Africans that it doesn’t care if you’re rich or poor, a new narrative is taking root, that “the poor” are “the problem” – that enforced proximity coupled with poverty and compromised health means the epicentre will be informal settlements.
This is because we are so fundamentally unequal that this virus (like HIV before it) is going to disproportionately affect the poor. And the poor are overwhelmingly black. So the prejudice that welcomed COVID has created its own truth.
Statistics do tell stories. But they are understood in different contexts. So while everyone would love to know more about their neighbours – from the census, from COVID-19 data, from income and expenditure surveys, and other official data sources – they can’t. And they should not be able to – that way lies stigmatisation, racist and nationalist narratives, and worse.
In many countries across the world narratives of “our” jobs apparently being “taken” by others are becoming increasingly common in the wake of COVID-19. This, as has been shown in South Africa prior to the pandemic, leads to xenophobic violence and more death, as happened immediately after the 2019 national elections.
Politicians should take heed. Good intentions do not guarantee good outcomes. Stop imagining that granular data helps – it doesn’t. Stick to the protocols – and the law. Statistics South Africa does not release this type of data, precisely to protect people from one another. Leaders need to do the same, or the country may be divided after the COVID-19 crisis than it was before it hit.
Africa must make sure it’s part of the search for a coronavirus vaccine
- Gale Ure
To refuse inclusion would prevent Africa’s researchers from being significant players in the universal fight against the virus.
The search for a COVID-19 vaccine has sparked international media controversy and negative sentiment around the potential harm of people taking part in clinical trials once the research enters its human testing phase.
A wave of anger was ignited when two top French doctors said on live TV that coronavirus vaccines should be tested on poor Africans. The doctors later apologised for suggesting that COVID-19 vaccine trials should be carried out on a continent where the people were largely impoverished, with limited resources, and unable to protect themselves.
The statements made by Camille Locht and Jean-Paul Mira fed into a world already fissured by deep-rooted racial and economic discrimination.
Stigmatisation and discrimination in previously colonised African countries swung into focus, resulting in research becoming the target of populist rhetoric. Didier Drogba, a retired footballer, raised the issue that African people should not be used as guinea pigs in a testing lab. Samuel Eto’o, another retired footballer, called the doctors “murderers”.
The comments also resulted in the launch of a social media initiative in the form of a Change.org petition to stop coronavirus trials in Africa. The reasoning was that “Africa and developing countries have been testing grounds of large pharmaceutical companies” using the poor as the “guinea pigs of the wealthy”.
Not unlike fake news, the resultant outcome of the doctor’s racist comments was worldwide misinformation. Modern day research and clinical trials are highly regulated. In a COVID-19 world, scientific activity to develop a vaccine for global use is under careful scrutiny. Short of finding a cure, a vaccine is the only viable means to manage the devastating future outcome of the disease. A vaccine will need to be tested, and the world is watching. The doctors’ racism, however, unequivocally reminded the African continent of past medical discrimination at the hands of European countries. The result was a gratuitous attack on scientific research.
Finding a vaccine for COVID-19 is a worldwide medical emergency, necessary to prevent the death of millions of people. Should Africa participate in a global clinical trial? Absolutely. To refuse inclusion would prevent Africa’s researchers from being significant players in the universal fight against the virus.
The extreme reaction from Africa was not entirely without merit. There are countries on the continent where vaccines and medical research are viewed with suspicion, and where both have been linked to activities, in the name of medicine, which were carried out in a grossly unethical manner.
During a meningitis outbreak in Nigeria, pharmaceutical company Pfizer tested Trovan, an experimental antibiotic drug, on 200 children without proper consent. In Malawi, during an AZT trial, in spite of there being alternative treatment available, a placebo was given to pregnant women enrolled on the trial. There is an ethical standard in research where a placebo, a substance which is of no therapeutic benefit, may not be given when investigating the efficacy of a new drug or drug regimen in cases where there is appropriate treatment available.
That medical research and medicine were involved in historical abuse cannot be argued, but clinical trials in the 21st century look very different.
A changed environment
Globalisation in the past decade has shifted the trend in research activity from being done in developed countries to include trials in low- and middle-income countries.
Fears that countries may not have the institutional capacity to carry out research to the same ethical standards as their western counterparts have disappeared. Instead global health research partnerships have sprung up across continents. This has led to increased collaboration between European and African research organisations.
Research which takes place in Africa is predominantly funded by northern sponsors, with national academics and clinicians partnering in the research process. This has had a balancing effect – sponsored projects assist African research institutions to acquire funding for their own projects, to facilitate publishing of results, and to upscale research knowledge.
The ethical frameworks of these trials are stringent. International research organisations provide oversight to ensure that participants are protected.
Research carries risk, which is why there are international codes which protect participants. Each country has national legislation and standards to ensure that research is carried out ethically. This means that:
No person can be enrolled in a clinical trial without first giving their informed consent. To give informed consent, the potential participant must have the entire process of the project explained to them. This includes all of the possible risks and harms, as well as the expected outcomes. This must be done in a language and at a level that the participant is able to understand.
Participants may not be enrolled without being given the opportunity to leave the project at any time.
A participant’s personal information must be confidential, and the researcher may not use the participant’s information if the person has withdrawn.
There are agencies where the participant can lay a formal complaint.
All participants must be followed up after involvement in a research project, and there must be a plan in place to assist any participant who requires additional care arising from the trial.
COVID-19 trials
COVID-19 medication trials are taking place around the world. In Asia 1000 participants have already been recruited in to test Remdesivir, a drug developed by an American pharmaceutical company, Gilead. In the US the first trials of a vaccine are being run on 45 healthy participants.
Legitimate medical research activities are important to ensure that pandemics like the COVID-19 tragedy can be managed. Should Africa not be involved in the fight, it will be an indictment against medical research’s basic foundation – to allow people to choose to be part of the solution or to refuse on informed and valid grounds. The alternative is to sit idly by, as part of the global furniture waiting to be saved.
A major step forward, but some warning lights are flashing. President Cyril Ramaphosa’s social and economic rescue package leaves some questions unanswered.
The Covid-19 economic rescue package announced on Tuesday night by President Cyril Ramaphosa is a major step forward. If effectively implemented, it will make a material difference in the lives of millions of people, and support tens of thousands of businesses. However, although the absence of details makes the package difficult to analyse, a number of weaknesses exist.
The size
Last week the Institute for Economic Justice (IEJ)arguedthat the rescue package should be commensurate with the scale of crisis.
As a rule of thumb, special Covid-19 government spending announced around the world has been roughly equal to the size of the expected economic contraction in each country. This is because, in the economics of lockdown, each rand spent is likely to have less of a stimulatory impact than in normal times.
In South Africa, estimates of the economic contraction have increased from 4% of Gross Domestic Product (GDP) two weeks ago, to 6 to 8% last week, to around 10% before the announcement of the package. 10% of GDP is just over R500 billion. This is the total the President announced.
But not all of it is new spending, nor necessarily government spending at all.
On the revenue side, R130 billion is to come from “reprioritising” existing planned budget expenditure. It makes sense to use money that may have been saved during the lockdown. But shifting money from one budget line to another will not necessarily be a long-term net gain for the economy. This is particularly true if we underfund long-term “capital expenditure” (investments in roads, ports, trains and so on).
On the expenditure side, R200 billion is in the form of loan guarantees, and R70 billion in the form of tax deferments or deductions. This is not additional government spending, though it will be an important lifeline for businesses and households.
This means there is R230 billion in spending, or 4.5% of GDP (shown in the table below). If R130 billion of this is from “reprioritisation” and R100 billion from the Unemployment Insurance Fund (UIF), then the package doesn’t necessarily cost the fiscus anything. This means that far greater spending should be leveraged for additional rescue measures and to set the economy on a new footing in the medium term.
Breakdown of R500 billion spending
Health interventions
R20 billion
Municipalities support
R20 billion
Social grants
R50 billion
Job support
R100 billion
Wage guarantees
R40 billion
Loan guarantees
R200 billion
Tax and payment deferrals and holidays
R70 billion
Income support
Researchers, activists, and some admirable government officials won the day and forced the National Treasury to concede to R50 billion in additional spending on social grants. This was a month-long battle that should never have had to be fought. The top-up to existing social grants will directly benefit over 18 million people, and indirectly another 14 million, many of the most vulnerable.
Unfortunately, the numbers don’t add up so it’s difficult to tell what’s going on here.
The proposed increase to the child support grant amounts to R36 billion, and increases to other grant beneficiaries amount to R8 billion – R44 billion in total.
A special Covid-19 grant is to benefit those “who are currently unemployed and do not receive any other form of social grant or UIF payment”. The President didn’t tell us how many people this will reach.
The most recent proposal on the table covered 8 million people – aged 21 to 59, earning below R3,500, not employed, and not getting another social grant. But at R350 a month for six months, that would amount to almost R17 billion. Those who proposed the grant originally sought to cover between 13 and 15 million people (R27 to R32 billion).
This amounts to a total package of at least R61 billion, as opposed to the R50 billion total announced by the President.
Presuming this R61 billion is correct, this will cushion the rise in extreme poverty and hunger. But depending on the fall in incomes in both formal and informal economies, a rise in poverty may still occur. Further, despite proposals on the table, the Covid-19 grant at R350 per month is too small, and its targeting will be complex to administer. A once-off universal basic income grant, at a significantly higher level (certainly not less than R500 per month), would be a better option.
Protecting jobs
How the R100 billion set aside “for the protection of jobs and to create jobs” is to be spent is also unclear.
R40 billion is allocated for supporting wage payments for businesses unable to pay their workers – presumably via the current Temporary Employer / Employee Relief Scheme (TERS) administered by the UIF. It’s unclear whether this includes the R30 billion already allocated to TERS, or is in addition to it. The IEJ showed that the original R30 billion did not guarantee a minimum wage and would only be enough to cover about 2.4 million workers, a share of those affected.
It is also uncertain whether the other challenges facing TERS will be attended to. It is slow, cumbersome, and difficult to access. The UIF seems ill-equipped to administer the scheme and it should be moved to the South African Revenue Service. And the current, illogical, requirement that it only covers businesses who have experienced a total or partial closure of operations as a direct result of Covid-19, must be removed. Restrictions on other funding streams, for example, a requirement of local ownership, also need to be relaxed.
Tax
R70 billion is dedicated to tax relief. Most of these measures delay the payment of taxes, although there are some tax deductions and holidays. How households (as opposed to businesses) will benefit is unstated.
There is also, it seems, no concrete package of compulsory measures around deferral of rent, mortgage or other loan payments. This can’t be left to the goodwill of the private sector to offer, and must be regulated.
Loan guarantees
The largest chunk of money – R200 billion – is dedicated to a loan guarantee scheme. Essentially, banks will extend special loans to struggling businesses and the National Treasury and South African Reserve Bank will bear the risk of default.
This is an important step forward and the commercial banks should be effective at getting this relief to businesses. But there are four issues to consider:
The Reserve Bank, not the Treasury, should stand behind these loans and absorb any losses, protecting funds for future expenditure.
Some businesses need bailouts not loans. As the IEJ notes: “additional debt, even at concessional interest rates, will not be appropriate for businesses facing a risk of insolvency. Similarly, it may prove optimistic that short-term tax deferrals will be an adequate or effective measure given the likely persistence of severe disruption and low demand beyond the end of the lockdown.”
Strict conditions should accompany these loans. For banks, the loan guarantee scheme should impose maximum interest rates and fees, limiting the scope for profiteering. For the businesses, borrowing conditions restricting executive bonuses, safeguarding jobs, and promoting equity requirements should be considered. These should not be so onerous as to discourage businesses from making use of the scheme.
There doesn’t seem to be a provision for big business (with turnover above R300 million a year). How many of these businesses are in trouble isn’t clear, but support may be needed. This support should also come with strings attached, and if the money is in bailouts, then government should receive a commensurate equity stake in the companies.
Financing
The President says that we will pay for all this from “local sources, such as the UIF, and from global partners and international financial institutions”.
This is the weakest element of the package.
The President’s plan is silent on additional tax measures. (The IEJ has estimated that “solidarity taxation” on rich people could yield R48 billion.) It is also silent on a special Covid-19 solidarity bond that would secure funds, on favourable terms and at low interest rates, from public and private institutional investors. Only an estimated R108 billion can be safely unlocked from the UIF. Private local finance must step up to the table.
The World Bank and International Monetary Fund are viewed, rightly, with great suspicion in South Africa. They are notorious for accompanying loans with anti-poor, pro-market measures of deregulation and slashing government and social spending. The IMF appears to have stepped back from this during the crisis but a flashing neon “proceed with caution” sign is required. While we should support global transfers from developed to developing countries, we should ensure that these loans come without strict anti-poor conditions, and that the loan terms are agreed to by all major social partners.
The bigger picture
The President’s address is bookended by references to the need to ensure “structural reforms” in the post-Covid recovery phrase. While economic reform is certainly needed, “structural reform” – as articulated by the Minister of Finance – is usually code for privatisation, cutting wages, and slashing spending. In line with this logic, the rescue packages do not include the necessary measures to stabilise the economy – further reducing borrowing costs, stabilising the exchange rate, and imposing measures to limit money leaving South Africa.
These worrying elements are, however, at odds with more progressive pronouncements by the President, for example that we should not “merely return our economy to where it was before” but “forge a new economy”.
The Covid-19 crisis is teaching the world that there is a need for more effective governance and a more proactive role for the state. It is showing South Africa that despite a decade or more of waste, corruption, and mismanagement, the state can play a developmental – and life-saving – role.
Gilad Isaacs is Co-Director of the Institute for Economic Justice and School of Economics and Finance, University of the Witwatersrand. This article was first published in GroudUp.
Wits publishes first clinical data on COVID-19 in South Africa
- Wits University
Health professionals will face difficult ethical decisions when it comes to dealing with COVID-19 patients.
For example, do they resuscitate patients even though the prospects of recovery are slim and the risk to the healthcare team high? How should healthcare workers respond?
This is one of the topics covered in the COVID-19 Special Issue of the Wits Journal of Clinical Medicine. The journal, published by Wits University Press under open access conditions, presents the first clinical data on COVID-19 published in South Africa.
The special issue covers a range of aspects of the pandemic, from the clinical, through ethical, to the social dynamics of its impact.
Editor-in-chief of the Wits Journal of Clinical Medicine Professor Pravin Manga says it is important for health professionals and the public to have access to scientific information: “Social media is awash with all sorts of quackery regarding prevention and treatment remedies for COVID-19 and it is during these times that we need to be rational and be guided by science rather than by emotion.” Manga is Professor of Internal Medicine, School of Clinical Medicine, in the Faculty of Health Sciences at Wits.
In addition to being a public resource, more than 10 articles in this issue aim to guide healthcare workers. These address the ethical aspects related to the pandemic – which patients should healthcare workers admit to already-filled intensive care units and who decides this? Associate Professor Kevin Behrens, Director and Head of the Steve Biko Centre for Bioethics discusses such ethical conundrums in his review.
*Covid-19 Resources for Academics and Students: Access the entire Wits University Press eBook collection in your university library through JSTOR and Proquest until 1 July 2020.
SA faces food riots and breakouts from the lockdown
- William Gumede
Getting food to the vulnerable, needy and poor during the COVID-19 lockdown is now increasingly urgent.
Getting food to the vulnerable, needy and poor during the Covid-19 lockdown is now increasingly urgent.
If not, South Africa face the specter of slowing down the spread of Covid-19, but large numbers of people dying of starvation, and possible food riots and breakouts of the hungry from the lockdown.
The overwhelming majority of South Africans are either unemployed, eke out a living in the informal sector or survives on one form of government social grant. Those who are unemployed, working in the informal sector or are self-employed have no income during the movement, trading and buying restrictions of the lockdown.
The restrictions on movement of the lockdown makes it difficult for civil society organisations who distribute food to assist the needy. Even so, civil society organisations and charities do not have the funds and resources to distribute food to all who need it.
So far, even the few food parcels being distributed by the state, private sector and civil society organisations, hardly reaches those who need it most.
Large numbers of poor South Africans get their food from community feed schemes every day; whether run by the state, civil society organisations or the private sector. Furthermore, millions of children from poor families who received their meals from the state school feeding scheme now are at home under lockdown with no food.
Roughly 10 million school-going children get their basic daily food from school feeding schemes. During lockdown such daily meals are not available. They face mass starvation. Not providing food to millions of needy, is a shocking omission in government’s Covid-19 emergency plan. There has to be a simple way of food reaching the needy quickly.
Providing food to the needy during the lockdown is a government responsibility, but the private sector, and well-off individuals who can contribute, should also do so. Individuals of means can donate food to the needy. As part of a solidarity social pact, government, private sector, civil society and ordinary citizens can club together to provide and distribute food to the needy over the lockdown period.
Government must partner with civil society organisations, charities, churches, business and citizens to distribute food to the poor. Retailers could make unused food available to the poor, rather than it to be allowed to go to waste.
Food must be distributed door to door to vulnerable families. Civil society organisations and charities who are traditionally involved in distribution food to the need must be given essential service status, given government and business funding. Well-off private citizens must also donate to such food distribution civil society organisations. They must also volunteer their expertise, if practical.
The private sector involved in logistics could help with the transport of food. Retailers almost everyday transport food from depots to stores. Food distribution to the poor in outlaying townships and informal settlements could for example piggy-back on such transport.
Telecommunications companies could help with either a short message system, social media application or an easy toll-free number for the needy to request or make application for food relief.
Every city, township or village could have a coordinating committee of civil society organisations, private sector, government and private individuals which can coordinate the receiving and distribution of food into the community. Government halls, community centres, churches or schools could be used as local food distribution hubs.
Although a better food relief strategy during the Covid-19 lockdown for the poor given the complexity of distributing food to the vast numbers of the poor, is to make food vouchers available which can be redeemed at certain retailers. The success of providing food relief to the poor during the lockdown will ultimately determine whether the lockdown explode into social upheaval, riots and breakouts.
Off course, the best strategy to provide food is to give a basic income grant to all the unemployed and poor, over the period of the lockdown, which will give people cash in hand, which could be paid out at Post Offices, banks or retailers. As for the argument that there is no public money to provide regular food, a food voucher or a grant to the needy over the lockdown period; the R50bn that government has set aside to foster “big” black economic empowerment (BEE) industrialists should instead to be used to feed the poor.
The terrifying social costs of not providing food to the needy: food riots, people dying of starvation and the deaths that will be caused by an accelerated spread of Covid-19 because the hungry break out of lockdowns, makes it crucial that money be found for food for the needy.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand, and author of Restless Nation: Making Sense of Troubled Times (Tafelberg). This article was first published in the Daily Dispatch.
Complaints against SANDF
- William Gumede
The SANDF and SAPS should not enforce the COVID-19 lockdown at the expense of undermining human rights, personal dignity and common sense.
The South Africa’s Military Ombudsman received at least 33 complaints from the public of excessive force, physical abuse and brutality against the military during the COVID-19 lockdown.
The Independent Police Investigative Directorate (IPID), which monitors police abuse, has registered 39 cases of complaint against police wrongdoing, with six incidents of “death as a result of police action” during the first week of the lockdown, and is investigation 13 complaints related to police shooting and 14 of police assault.
In the first few days of the lockdown, more people died from police and military heavy handiness then from the coronavirus itself.
A number of videos have circulated of police and army enforcing the lockdown who were beating people they believe were not confirming to lockdown rules. In Hillbrow in the Johannesburg inner city police sjambokked people they believed were not following lockdown rules. In Soweto, soldiers have forced people do push-ups for not adhering to the lockdown rules.
One policeman has so far been arrested for a killing a citizen who was shot dead by police after following the man from a bar to his house.
After 26 years since the end of apartheid, the South African police appear still not to have been trained, neither have they inculcated a culture of human rights-policing. Equally, the army, although it is now involved in numerous peace making missions abroad, are also not at times performing their duties in such a way to respect basic human rights, dignity and compassion.
It does appear that both the police and army culture is based on using violence, humiliation and aggression to enforce rules.
Nosiviwe Mapisa-Nqakula, the Minister of Defence said in response to the death of an Alexandra man allegedly assaulted by SANDF soldiers: “We hang our heads in shame.”
But there has been incidents where the police and the army go against common sense and arrest law-abiding citizens who are within the rules. There has been a number of cases where people have legitimately gone to the shops, pharmacy or other essential business who have been then been arrested for contravening the rules.
Last week Allan Kirby, a diabetic, from Somerset West was fined by the police for going to his local pharmacy, because he did not have his prescription on hand.
The South African Human Rights Commission (SAHRC) has urged the South African Police Service (SAPS) and the South African National Defence Force (SANDF) to “exercise greater tolerance and apply minimum force in the execution of their duties as has been urged by the President”.
The police and army should not discriminate against people based on race, religion or class in their enforcement of the lockdown rules. Poor communities, already vulnerable people and the homeless appear to be particularly at the mercy of police and army abuse.
It was important that Minister of Communications, Telecommunications and Postal Servicers Stella Ndabeni-Abrahams was charged with contravention of regulation 11B of the Disaster Management Act; because the lockdown rules must be seen to be enforced without discrimination based on privileged, political connectedness or influence.
The family of an Alexandra township man, Collins Khosa, who died after allegedly been assaulted by soldiers during the lockdown enforcement in the township, has gone directly to the Constitutional Court to hold government accountable, have the soldiers involved fired and to seek compensation for his death. It is important that citizens use the courts to hold government accountable if other official oversight institutions do not so.
Freedom of expression during the lockdown must be defended. Criticism of the president or the government’s measures to tackle Covid-19 or the behaviour of the police or army is not illegal. Off course, spreading fake news is unacceptable, and should be dealt with by the authorities.
Citizens must report police and army abuse even if they may not be able to precisely identify a particular individual responsible for manhandling them. The media, civil society organisations and oversight organisations such as the Human Rights Commission must monitor police and army abuse.
The media, civil society and oversight organisations must support vulnerable, marginalised and powerless communities and citizens who appear to be on the receiving of disproportional police and army brutality.
All complaints against the police and army must be thoroughly investigated. Police and army officers found to have to be abusive should be disciplined. They should be held to account publicly.
In the long-term, the training curriculum of the police and army must be overhauled to make it more human rights based.
The organisational culture of the police and army, which clearly is based on humiliation, aggression and abuse should be thoroughly shaken up to focus on compassion, human rights and decisions based on common sense.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand, and author of Restless Nation: Making Sense of Troubled Times (Tafelberg). This article was first published in the Daily Dispatch.
Coronavirus: why South Africa needs a wealth tax now
- Aroop Chatterjee, Amory Gethin and Léo Czajka
A wealth tax on the top 1% of South Africans could raise R143 billion. This corresponds to 29% of the R500 billion COVID-19 package announced by the government.
The consequences of the COVID-19 lockdown are yet to be fully determined and understood. But one thing we can be fairly certain of – in South Africa its impact will be shaped by the country’s inequalities.
Our study reveals that half of the adult population survives with near-zero savings, while 3,500 individuals own 15% of the country’s wealth. The response to the crisis must take this into account to help the most vulnerable while still safeguarding fiscal sustainability.
Based on our new study on wealth inequality in South Africa, we propose a progressive solidarity wealth tax. This would allocate the fiscal burden of current interventions on those most capable of paying. It is in line with the recommendations recently made by the International Monetary Fund to equitably attain fiscal sustainability and better position the economy for post-COVID recovery.
We show that a wealth tax on the richest 354,000 individuals could raise at least R143 billion. That equates to 29% of the announced R500bn fiscal cost of the relief package.
Unequal distribution
A lot of studies show how extreme income inequality is in South Africa, but little has been documented about wealth. Net wealth is the sum of all assets less any debts. Assets include cash, bank deposits, pensions, life insurance, property, bonds and stocks. Debt includes mortgages and other loans such as retail store credit accounts or loans from friends, family and money lenders.
In our new paper, we combine national accounts statistics, household surveys and exhaustive tax microdata to assess the reliability of available data sources. We also provide the most comprehensive possible picture of the distribution of wealth. This is the first time this has been done in South Africa.
Better data is needed – about direct ownership, capital income and assets held through trusts. Nevertheless, our results give a good sense of the magnitude of the disparities. Three key results are worth mentioning.
Firstly, in 2017, the 10% richest South Africans (all adults with a net worth over R496,000) owned 86% of wealth, with an average of R2.8 million per adult. In contrast, about 18 million (the poorest 50%) were either in debt or had near-zero savings. With an average net worth of R486 million, the richest 3,500 owned 15% of wealth. This was more than the 32 million poorest altogether.
Secondly, these extreme inequalities extended to all forms of assets. The richest 10% owned 99.8% of bonds and stock – which accounted for 35% of wealth. The top decile also owned 60% of housing wealth and 64% of pension assets. Housing wealth amounted to 29% of wealth and pension assets to 33%.
Thirdly, we show that wealth concentration has remained broadly stable since 1993, and may even have increased within top wealth groups. Wealth inequality remains significantly higher than what could be estimated in Russia, China, India, the US or France.
Why wealth inequality matters now more than ever
Our findings are particularly relevant to the current crisis. South Africans are unequally armed to survive the contraction of the economy produced by the lockdown. Our paper helps get a sense of the size of the population likely to be under intense stress in the very short term.
Before the lockdown, about half of the population was already in debt, or had near-zero net wealth. Therefore, this crisis will at best sink millions of people further into indebtedness or force them to beg, loot or starve. Conversely, our paper shows that a minority of individuals are in a much less vulnerable situation.
The policy solutions needed to absorb the shock and recover fast must be carefully designed to take these factors into account. Principally, they need to reallocate resources to give everybody equal chances to survive the shock.
In this unprecedented crisis, the government announced a relief package with a R500 billion fiscal cost. One key remaining question is how such a plan will be funded.
The possibility of collecting additional tax revenue from those most able to contribute has not yet been brought to the table. We believe it should be considered. Our estimation suggests it would raise significant revenues. And it would allow the country to allocate the cost of the national response on the least vulnerable.
In the spirit of solidarity, a wealth tax could be part of the solution to safeguard long-run fiscal sustainability and inclusive growth.
How much could a wealth tax raise?
We propose a progressive wealth tax, which would apply only to South Africans with a net wealth currently superior to R3.6 million, that is the richest 354,000 (1% of the adult population).
The first bracket – all wealth between R3.6 million and R27 million – would be taxed at a 3% rate, the second bracket (R27 million to R119 million) at 5%, and all wealth above R119 million at 7%. Individuals with less than R3.6 million would be exempt. A billionaire would face a 6.7% tax rate: she would pay 3% on the fraction of her wealth higher than R3.6 million but lower than R27 million; 5% on wealth higher than R27 million but lower than R119 million; and 7% of the R821 million she owns above R119 million. This would leave her with post-tax wealth of R933 million.
Other tax schedules could of course be designed. The objective here is to give an order of magnitude of the expected revenues.
Taking into account the recent Johannesburg Stock Exchange All Share Index drop in value and assuming a 30% evasion rate (as available evidence suggests), we simulate that such tax would raise R143 billion.
It would still leave rich individuals with very high levels of wealth: for each of the brackets, post-tax wealth would on average be R9.3 million, R50 million and R376 million respectively.
A realistic policy
Critics of a wealth tax argue that it would be too costly and complex to implement. But South Africa is well positioned to administer this tax cost-effectively.
Firstly, the tax base we consider covers very few individuals, reducing the administration required.
Secondly, South Africa already has in place third-party reporting by financial intermediaries straight into the South African Revenue Service, providing information on capital income and ownership. Existing municipal valuations could be used to value property assets. This would cover the major components of asset holdings, especially stocks and bonds.
Capital flight, through offshoring or migration, is a potential risk. We account for this by making conservative assumptions about avoidance and evasion, and still project sizeable revenues. There is also markedly more cooperation between tax authorities to clamp down on undeclared incomes and assets in foreign jurisdictions, including tax havens. The premise is not a given. Capital flight implies forfeiting opportunities that considerably enriched them for the sake of avoiding a tax that barely makes an impact on their total wealth. Importantly, the wealthy themselves have said now is the time for solidarity.
A wealth tax, contrary to popular opinion, would not necessarily discourage job-creating investments. Maintaining fiscal sustainability while sparing the most vulnerable is more important to ensure a quick recovery and attract investments. Moreover, inherited wealth has a significant role in South Africa: we find high levels of wealth concentration even among 20-year-olds. Diminishing the importance of inherited capital with a wealth tax may actually be a better collective strategy to improve social welfare, including growth.
In light of the lessons learned from the Zondo commission of inquiry into corruption, taxpayers would need guarantees that this special tax will be properly collected and spent. The national treasury already uses ringfencing mechanisms to make revenue and spending for specific projects accountable. To answer potential criticism, the government could build on such rules to generalise more transparent practices.
There may be theoretical implementation challenges of such a wealth tax. But we would argue that South Africa is well placed to overcome these.
When designing the radar for Britain during World War II, Robert Watson-Watt justified his choice of a nonoptimal frequency as follows:
Give them the third best to go on with; the second best comes too late, the best never comes.
This radar was pivotal in allowing Britain to overcome a larger, more sophisticated German air force.
In our situation, we cannot let perfection be the enemy of progress, or in this case, survival.
Aroop Chatterjee, Research Manager: Wealth Inequality, Southern Centre for Inequality Studies, University of the Witwatersrand; Amory Gethin, Research Fellow - World Inequality Lab - Paris School of Economics, and Léo Czajka, Research fellow - World Inequality Lab - UCLouvain
Communities, not government, can and are fighting COVID-19
- Karl von Holdt and Tasneem Essop
The heavy-handed, top-down approach during the lockdown has not worked; NGOs, coalitions and community networks have.
A popular movement has arisen with extraordinary rapidity in response to the Covid-19 pandemic. With the announcement of a state of disaster, activists in communities across the country mobilised to protect their communities.
For example, the Amadiba Crisis Committee, established to fight against the destruction of land by mining on the Wild Coast, formed teams to move from household to household distributing sanitiser and talking about the necessity for physical-distancing.
In Khayelitsha, Cape Town, the Social Justice Coalition formed a community action network (CAN) and mobilised to demand water tanks from the city — which actually arrived within a week. The CAN, too, organised teams to inform community members about how to respond to the pandemic. The broader CAN movement in Cape Town has expanded to play a similar role.
In Ekurhuleni, the General Industries Workers Union of SA and the Casual Workers Advice Office printed 700,000 pamphlets about the coronavirus, distributing these at taxi ranks and in communities, and also made their own sanitiser for distribution. The street patrollers in the Yeoville Community Policing Forum marshalled at the long queues at local supermarkets, encouraging physical-distancing and resolving conflicts.
These few examples show faster, more agile and more effective responses than most state activities.
Meanwhile, at the national level, a diverse network of activists came together with the aim of co-ordinating a popular response to the state of disaster and the pandemic.
They were motivated by three overriding concerns: to strengthen community responses; ensure government responses did not exacerbate inequality and exclusion; and propose measures that would not only counter the immediate social and economic crisis, but also lay the foundations for a different kind of future.
Within a week they had established a broad coalition, which, by now, is supported by 250 movements, NGOs, trade unions, informal sector workers, feminist groups, faith-based organisations, research centres and public health networks — the biggest coalition SA has seen since the 1983 formation of the United Democratic Front.
The coalition has about 20 working groups, undertaking work ranging from building community organisation to distributing food parcels, and from policy work to repression monitoring and gender organising.
These and other initiatives that are not part of the C19 People’s Coalition reveal a vibrant and resourceful set of movements and networks with deep roots in communities and workplaces. Yet despite efforts, and notwithstanding some ad hoc local collaborations, there has been no systematic engagement from a government which, it is increasingly clear, is too distant and disorganised to directly access communities and ameliorate desperation and social distress.
Its food parcel efforts are hindered by bureaucratic processes to limit beneficiaries to the “deserving poor”, and failed promises have provoked tensions and food riots in some areas.
Indeed, the state’s most visible presence in communities is in the form of the police, municipal law enforcement, and the army, which has been set the often unattainable task of enforcing the lockdown in communities where compliance is impossible. This has led to many instances of brutal, illegal and unjustifiable force being used against people across the country.
These have turned fatal in some cases — the death of Collins Khoza in Alexandra, who was allegedly assaulted by soldiers; the death of Sibusiso Amos in Vosloorus allegedly from the intervention of Ekurhuleni metro police and private security; and the Independent Police Investigative Directorate is now investigating the death of a man in Soweto, who was allegedly assaulted by police. Multiple reports received by the coalition provide a snapshot of the abuse of power, corruption, human rights abuses, humiliating treatment and violent assaults perpetrated by security forces.
Colonial roots
To make matters worse, local governments, together with security forces, have also carried out illegal evictions in Cape Town, Johannesburg and Ethekwini, where the ANC authorities have continued their vicious vendetta against Abahlali baseMjondolo [a shack-dwellers’ movement that campaigns both against evictions and for public housing]under cover of the lockdown.
In all three metros there are reports and images from informal settlements and land occupations of people being assaulted, shot at and dragged out of shacks by law enforcement who have been sent out to tear down these structures. Cape Town’s mass internment camp for the homeless in Strandfontein has also been severely criticised for being overcrowded, unsafe and flouting the health requirements for curbing the spread of the coronavirus.
This is not the way to fight the pandemic. Quite the opposite — it is more likely to accelerate the pandemic and produce non-compliance in alienated and starving communities. These failures by the government suggest it is still trapped in a view of its poor and working-class as passive recipients of charity incapable of agency; generally undeserving of support, unless at starvation’s door; sources of infection who must be quarantined; and “dangerous classes” who pose a threat to authority and order.
These attitudes have deep colonial roots. Using repressive state machinery for public-health purposes serves to further entrench the historic frictions that already exist between the police, army and society. It weakens the relationship between state institutions and communities even further and increases the frustration of individuals and communities.
If President Cyril Ramaphosa and his government are to have any hope of managing the public healthcare crisis they need to decisively dispense with this apartheid heritage and work closely with popular movements, unions and civil society to educate, provide services and food, and devise appropriate public-health strategies and lockdown codes for precarious, overcrowded and desperate communities.
Where there is political will there is a way to work across sectors
- Lungiswa Nkonki and Sharon Fonn
COVID-19: There are lessons for the health sector - the need for more coherent integration is undeniable.
South Africa reported its first case of coronavirus disease 2019 (COVID-19) on 5 March 2020. In the weeks that followed the country saw decisive, strong leadership from President Cyril Ramaphosa. It has also seen significant, important and necessary co-ordination between different ministries. These have included education, justice, health, trade and industry, transport, public works and infrastructure and finance.
The rapid pace at which steps were taken was impressive. More important was the all-encompassing intersectoral approach. Ministries with different mandates and areas of focus are working in concert for a common cause.
Intersectoral action recognises that health and wellbeing is influenced by where and how people live, where they work, what transport they use, and their access to water, sanitation, economic hubs and services. Health is socially determined. To improve health, coordinated action is required between ministries that don’t have health as their core mandate.
This is what “Health in All Policies” is about – a coherent approach to health policies set out by the World Health Organisation that’s been adopted by a number of countries, but by no means all. Without this coordination a long and healthy life for all cannot be achieved.
COVID-19 has dramatically highlighted the need for a more integrated healthcare system.
In a letter published in the South African Medical Journal we argue that the threat that COVID-19 presents has resulted in both leadership from government and apparent willingness of all South Africans to play their part. It presents a number of opportunities that should be exploited to the full.
One stark insight is that pooling resources across the health sector is needed to address this pandemic. This includes the rational use of hospitals, high care beds and laboratory testing capability.
The exemption seeks to promote co-ordination, sharing of information and standardisation of practice across the entire healthcare sector. The aim is to facilitate cost reduction measures, allowing possible procurement efficiency in purchasing of diagnostic tests, treatment and other preventive measures.
In particular the exemption seeks to promote agreement between the national department of health and the private sector to make facilities available to the public sector. For example, if government wants to use private sector bed capacity it may be able to use its drug related single exit price experience to negotiate the cost.
The makings of a roadmap
Late last year South Africa released a Health Market Inquiry report. It found excessive use of private health care; more care was delivered than could be explained by the level of illness of the private sector population.
The report also found that the sector would benefit from better regulation.
It made a number of recommendations that promote standardisation and knowledge-sharing as well as a method to deal with pricing within the functions of the proposed supply-side regulator.
The supply-side regulator includes systems which would allow for a real time description of:
providers – which ones exist and where they’re operating
where beds are located, their purpose (medical or surgical) and level of care (general, high care or intensive care), and
information on utilisation rates.
The report set out how the regulator could rationalise various functions which are currently poorly coordinated or absent across the private and public sector.
The report emphasised that the efficiency of, and access to, care required having information about health sector capability and quality across the entire health sector. This would enable resources to be used rationally.
The COVID-19 pandemic has underscored that such an approach is essential.
Set up this way, the regulator would form an essential mechanism going forward to ensure that South Africa was prepared for possible future emergencies.
Learning from COVID-19
There are two lessons here. For the health sector the need for more coherent integration is undeniable. Perhaps this exemption and working together to protect South Africa from the effects of this pandemic can build trust between players and will ease South Africans into a more rational and integrated healthcare system.
The second lesson is about intersectoral action and Health in all Policies that South Africa has seen illustrated to mitigate the threat of COVID-19. Poverty, inequality and unemployment similarly threaten the wellbeing of individuals in South Africa.
Equally urgent is the need to develop a mindset that understands that all policies aimed at development require integrated action. This means involving a range of players across government departments, across the public private divide, and must include social mobilisation and engagement with communities. The response to COVID-19 illustrates this well.
South Africa has managed to do this for health. It must be possible to do it in other areas of public policy. This needs to be extended further to build a more equal South Africa.
Can the philosophy of ubuntu help provide a way to face health crises?
- Evanson Z Sambala, Lenore Manderson and Sara Cooper
There are lessons for the health sector - the need for more coherent integration is undeniable.
South Africa reported its first case of coronavirus disease 2019 (COVID-19) on 5 March 2020. In the weeks that followed the country saw decisive, strong leadership from President Cyril Ramaphosa. It has also seen significant, important and necessary co-ordination between different ministries. These have included education, justice, health, trade and industry, transport, public works and infrastructure and finance.
The rapid pace at which steps were taken was impressive. More important was the all-encompassing intersectoral approach. Ministries with different mandates and areas of focus are working in concert for a common cause.
Intersectoral action recognises that health and wellbeing is influenced by where and how people live, where they work, what transport they use, and their access to water, sanitation, economic hubs and services. Health is socially determined. To improve health, coordinated action is required between ministries that don’t have health as their core mandate.
This is what “Health in All Policies” is about – a coherent approach to health policies set out by the World Health Organisation that’s been adopted by a number of countries, but by no means all. Without this coordination a long and healthy life for all cannot be achieved.
COVID-19 has dramatically highlighted the need for a more integrated healthcare system.
In a letter published in the South African Medical Journal we argue that the threat that COVID-19 presents has resulted in both leadership from government and apparent willingness of all South Africans to play their part. It presents a number of opportunities that should be exploited to the full.
One stark insight is that pooling resources across the health sector is needed to address this pandemic. This includes the rational use of hospitals, high care beds and laboratory testing capability.
The exemption seeks to promote co-ordination, sharing of information and standardisation of practice across the entire healthcare sector. The aim is to facilitate cost reduction measures, allowing possible procurement efficiency in purchasing of diagnostic tests, treatment and other preventive measures.
In particular the exemption seeks to promote agreement between the national department of health and the private sector to make facilities available to the public sector. For example, if government wants to use private sector bed capacity it may be able to use its drug related single exit price experience to negotiate the cost.
The makings of a roadmap
Late last year South Africa released a Health Market Inquiry report. It found excessive use of private health care; more care was delivered than could be explained by the level of illness of the private sector population.
The report also found that the sector would benefit from better regulation.
It made a number of recommendations that promote standardisation and knowledge-sharing as well as a method to deal with pricing within the functions of the proposed supply-side regulator.
The supply-side regulator includes systems which would allow for a real time description of:
providers – which ones exist and where they’re operating
where beds are located, their purpose (medical or surgical) and level of care (general, high care or intensive care), and
information on utilisation rates.
The report set out how the regulator could rationalise various functions which are currently poorly coordinated or absent across the private and public sector.
The report emphasised that the efficiency of, and access to, care required having information about health sector capability and quality across the entire health sector. This would enable resources to be used rationally.
The COVID-19 pandemic has underscored that such an approach is essential.
Set up this way, the regulator would form an essential mechanism going forward to ensure that South Africa was prepared for possible future emergencies.
Learning from COVID-19
There are two lessons here. For the health sector the need for more coherent integration is undeniable. Perhaps this exemption and working together to protect South Africa from the effects of this pandemic can build trust between players and will ease South Africans into a more rational and integrated healthcare system.
The second lesson is about intersectoral action and Health in all Policies that South Africa has seen illustrated to mitigate the threat of COVID-19. Poverty, inequality and unemployment similarly threaten the wellbeing of individuals in South Africa.
Equally urgent is the need to develop a mindset that understands that all policies aimed at development require integrated action. This means involving a range of players across government departments, across the public private divide, and must include social mobilisation and engagement with communities. The response to COVID-19 illustrates this well.
South Africa has managed to do this for health. It must be possible to do it in other areas of public policy. This needs to be extended further to build a more equal South Africa.
Let’s talk about ethics and treatment for COVID-19
- Christopher Wareham and Kevin Gary Behrens
In this episode of The Conversation - Africa's podcast, Pasha, Wits bioethics researchers discuss the difficult decisions facing health professionals.
With COVID-19 cases continuing to rise in South Africa, health professionals will have to make important decisions on who gets what treatment. But how do these decisions get made?
In today’s episode of Pasha, Kevin Behrens, director of the Steve Biko Centre for Bioethics, and Christopher Wareham, a senior lecturer at the same centre, discuss the ethics surrounding coronavirus topics.
Wits needs 300 volunteers for COVID-19 rapid test study
- Wits University
Have you tested positive for coronavirus or been near someone who has? If so, your country urgently needs you for a South African COVID-19 rapid test study.
This study, led by the Wits Department of Immunology, aims to ensure that existing rapid tests for COVID-19 are accurate.
Qualifying volunteers will need to submit blood and saliva samples for serological testing for COVID-19. This includes the rapid antibody tests and the formal serology assays. [An assay is a laboratory procedure to measure quantities].
Serological tests measure the amount of antibodies or proteins present in the blood when the body is responding to a specific infection (such as COVID-19).
Antibody tests check for the small molecules that the body produces to fight infection. These antibodies are very specific to particular infections and form the basis of serology testing for many infectious diseases.
Why this study is important
South Africa urgently needs to increase testing for COVID-19 so that infection can be identified, traced, isolated and contained. Although a number of rapid diagnosis tests are already available in South Africa, they are not consistently reliable. Inaccurate test results could lead people to believe they do not have the coronavirus, so they don’t self-isolate and then inadvertently infect others.
“Although there are rapid diagnostic tests available that can test for antibodies in the blood and deliver a result within minutes, these tests have not performed consistently well,” says Professor Elizabeth Mayne, Head of the Division of Immunology at Wits and Principal Investigator for this study.
“To check that the various rapid tests being brought into South Africa work, we need blood and saliva samples from 300 people who tested positive for coronavirus, or who were in close contact with someone who tested positive".
The role of volunteers
On volunteering for the study, you will be briefed fully and will have the opportunity to ask questions.
You will be asked questions about your age, any underlying conditions you might have, such as high blood pressure and chronic lung diseases, any medications being taken, when you tested positive, your travel history and whether or not you had any symptoms.
A nurse will be dispatched to your home. The nurse, wearing full personal protective equipment (PPE), will extract around eight teaspoons of blood from you, as well as some saliva and some mouth/throat swabs.
These bio-samples of your blood and saliva will be used to create banks of known positive and negative controls, which scientists around the country can use to quickly and accurately evaluate any rapid or serological tests.
About the study
The study is approved by the Human Research Ethics Committee at Wits University.
A minimum of 300 participants are required for the study.
The study is ongoing, so participants can volunteer at any time.
Participation is entirely voluntary and participants can withdraw consent at any time without giving a reason. Such withdrawal will have no effect on participants' diagnosis or treatment.
Participants will not be paid or in any way be financially remunerated for participating.
Participants will not be able to get the results of their tests.
How to volunteer
If you meet the criteria and wish to participate please email Elizabeth.mayne@nhls.ac.za or call 082 337 6349 for a comprehensive briefing and enrolment.
About the Principal Investigator
Professor Elizabeth Mayne holds an MBBCh and MMED in haematology from Wits University. She is a specialist haematopathologist has since 2018 been Head of Immunology in the School of Pathology in the Faculty of Health Sciences at Wits. She is collaborating with Professor Wendy Stevens and Professor Ian Sanne on this project.
Why South Africa needs to ensure income security beyond the pandemic
- Hannah J. Dawson and Elizaveta Fouksman
Economic distress was the norm for many before the coronavirus outbreak. The pandemic is an opportunity to provide an economically secure future for all.
A slew of countries ranging from the US to Brazil to Singapore to South Africa have decided to give people money in response to the economic crisis caused by the coronavirus pandemic.
While the amounts and details of the grants have varied, these governments have all made it clear that such payments are a short-term emergency response to an exceptional situation. But is the economic uncertainty caused by COVID-19 as exceptional as it seems? Might the reasons for guaranteeing economic security be valid even without a global pandemic?
Take the case of South Africa.
The government has decided to substantially bolster the social security net, directing R50 billion to those most acutely affected by the crisis over the next six months. This will be distributed in the form of increasing the current child support grant. In addition, pensions and disability grants will go up. But the biggest change is the introduction of a special “COVID-19 Social Relief of Distress grant” to be paid to people who are currently unemployed and do not receive any social grant or unemployment insurance for the next six months.
The new COVID-19 grant is the first time unemployed working-age adults are being included in the social grant system. Since 1994, the African National Congress government has resisted including them. And the resistance remains.
South Africa’s treasury has been busy making it clear that the new direct cash transfers are exceptional and temporary. At a recent media briefing, finance minister Tito Mboweni repeated again and again that the additional grants were temporary. His anxiety that people will expect the additional grants to remain in place – and that they will become “agitated” when the grants are taken away – is palpable.
Economic distress – before the pandemic
The name of the new grant shows exactly what it’s meant for. Calling it the COVID-19 Social Relief of Distress grant makes it clear that this is an emergency measure, here only to relieve the distress of COVID-19.
But economic distress was the norm for many before the coronavirus outbreak. Illness, ill-fortune and economic precarity existed long before this pandemic. The outbreak only makes the economic crisis broader, deeper and more visible.
An accident, a family death, or a delayed train can happen to anyone. But for the large number of people in South Africa who work for low wages without a proper contract, or who simply cannot find work at all, one of these events can be the tipping point into destitution.
They don’t need a pandemic to experience economic distress.
We would argue that South Africa needs more than emergency provisions such as a short-term new social grant or an emergency basic income. Rather, it needs a permanent form of economic security, be it in the form of a universal basic income that is given to all and then taxed back from those that don’t need it, or some other form of income guarantee for all.
Work does not provide economic security for all
Politicians are now willing to guarantee citizens some measure of economic security through the state because they cannot ask them to leave their homes and find economic security through work. But in a place like South Africa, finding economic security through wage labour was never the solution. It is just wishful thinking.
The current economic distress brought on by the pandemic is not a brand new crisis. It’s an amplification of what was already reality for many South Africans. Indeed, it deepens economic insecurity around the world: globally, over 60% of workers are in “non-standard” employment – that means it’s precarious, short-term or informal.
The link between wage labour and economic security has long been a mirage in South Africa. Mass unemployment and precarity are neither new nor temporary. They are structural and enduring features of South Africa, further compounded as companies collapse and invest in labour-saving technologies. The need to provide economic security beyond the labour market has long been political reality.
Guaranteeing economic security
The idea that economic security should be a universal right – much like universal access to health care – has been around for centuries. At its core, it’s simply the argument that no matter who they are or what they do, every human being should be guaranteed enough resources to stay alive.
Ray van Heerden, a car guard, from the poverty-stricken shantytown of Munsieville, cannot work due to the lockdown.EFE-EPA/Kim Ludbrook
There are many ways to provide this kind of economic security. It could be via a social grant given to everyone who needs it. Or a negative income tax, a payment through the tax system that tops up the income of the poor to a basic level. Or it could be via a universal basic income – a regular payment to every resident, with no conditions or targeting.
Universal basic income has the advantage of simplicity. There’s no need for a bureaucracy to decide who should get it and who should not. And while many people critique it for being expensive and going to people who already have money, this is not the case. It goes to everyone, but is taxed back from the wealthy who don’t need it – meaning it both costs less than you might think, and ends up helping only those who really need it.
The biggest source of resistance to providing economic security to all, be it through universal basic income or other forms of guaranteed income, is the idea that people have to work for money – that “you can’t get money for nothing”. This is why, despite a big push for basic income in the early 2000s, the South African state has always resisted the idea. But work has never been able to provide economic security for all in South Africa. Why keep expecting the poor to receive money through work only, when work is unavailable, or unstable and badly paid?
The fact that many countries are now giving citizens emergency cash could be a step in the right direction. Finally, anyone who needs it can access some form of economic support from the state. But this should not be a temporary measure. It does not address a new problem, but rather a very old one that is suddenly worse. What the country needs is not an emergency basic income, but a permanent income guarantee. In fact the Spanish government plans to maintain the basic income it is implementing beyond the pandemic.
No longer business as usual
The circumstances that necessitate an income guarantee have long existed in South Africa. It is time for the government to acknowledge this. There can be no return to business as usual, because business as usual means poverty, suffering and ongoing economic distress.
The poor and most vulnerable understand that the economic insecurity they face is not a state of exception. It is the default. It will not end after the easing of the lockdown.
This international Workers’ Day, the COVID-19 pandemic provides an opportunity to see things as they are – that work cannot be assumed to shelter everyone from economic distress. It also provides an opportunity to delink basic livelihood from wage labour, and begin to develop policies that deliver an economically secure future for all.
The impact of coronavirus could compare to the Great Depression
- William Gumede
And a corresponding rise in nationalism and xenophobia may follow, just as it did in the 1930s.
The coronavirus crisis will be the biggest financial crisis of our generation, much larger than the 2007-2009 global financial crisis.
It is very likely that the economic impact of the coronavirus crisis will be comparable with the Great Depression, the period of devastating economic decline between 1929 and 1939, which saw mass unemployment, factory closures and the accompanying personal trauma.
The coronavirus outbreak will bring an economicdepression- that is, a severe and prolonged economic decline with high levels of unemployment and company closures.
Record numbers of people will likely suffer from post-traumatic stress disorder (PTSD), the combination of stress, anxiety and depression that develops in some people who have experienced a traumatic event.
The coronavirus outbreak is already such an event. More than three million people around the world have been infected by the virus and more than 200,000 have died of it. Estimates show that the coronavirus may kill 100,000 Americans, the equivalent todoublethe number of Americans who died in the Vietnam War.
By comparison, the Spanish flu pandemic of 1918-1919 infected 500 million people, or one-third of the world's population, with 50 million deaths, of which 675,000 occurred in the US. The world's population in 1918-1919 was estimated at 1.5 billion. If one translates this to today's figures, with a world population of 7.8 billion, it would be the equivalent of 2.6 billion people infected and 250 million deaths.
The United Nations Conference on Trade and Development (UNCTAD), the UN's trade and development agency, says the slowdown in the global economy caused by the coronavirus outbreak is likely to cost at least $1 trillion in 2020 alone, in terms ofreduced growthmeasured in gross domestic product (GDP).
Over time, the cost to the global economy is likely to be three or four times that figure.
As a comparison, it is estimated that the 2007-2009 global financial crisis cost the US around$4.6 trillionin terms of lost growth in GDP, or 15 percent of its GDP compared to the years before the financial crisis.
During the Great Depression, unemployment in many countries hovered around 25 percent, with one in four people in industrial countries made jobless by it. In the US, nearly half of the banks collapsed, 20,000 companies went bankrupt and 23,000 people committed suicide.
The current pandemic will cause individual economies to plunge into recession; businesses will close down and jobs will be lost at similar levels to that of the Great Depression. Moreover, the pandemic is impacting both industrial and developing countries; whereas the Great Depression was largely concentrated in industrial countries.
The International Labour Organization (ILO) has predicted that the pandemic will wipe out 6.7 percent of working hours in the second quarter of this year - the equivalent of195 millionfull-time workers.
This is already playing out. In the US, more than 22 million people filed claims for jobless benefits in the four weeks ending April 11, according to the US Department of Labour. To put these latest numbers into context, in 2008, at the height of the global financial crisis, 2.6 million people in the US filed forunemploymentin that year, making 2008 the year with the biggest employment loss since 1945.
Suicides, domestic violence and murders increase during times of economic hardship and this may be further exacerbated by lockdowns and self-isolation.
Wealthier countries such as Germany, the UK and the US have rolled out large aid programmes - larger than those which appeared in the aftermath of the 2008 global financial crisis - to support businesses, the self-employed and the unemployed for loss of income during the lockdown. Germany will give unlimited loans to large companies, pay 60 percent of salaries of troubled companies to allow them to reduce the working hours of employees without having to lay them off and financial support to the self-employed.
The US has unveiled a $2 trillion coronavirus rescue package for struggling companies and employees, which includes loans, equity stakes for government in businesses in strategic sectors and direct cash payments to individuals.
While these bailouts might provide interim relief, they will plunge countries, companies and families into debt for years, while we will also have to deal with the social crises of deaths, suicides and mental disintegration for a long time after the coronavirus pandemic.
After the Great Depression there was a rise in nationalism around the world - as a direct result of the financial, social and emotional hardships of the depression - creating the conditions that eventually led to the second world war.
There has been a similar rise innationalism, populism and xenophobia during the coronavirus outbreak. Of course, this had been growing for many years before the pandemic, in part as a result of austerity measures that caused financial hardship in the aftermath of the 2007-2009 financial crisis.
The coronavirus crisis will likely make those austerity measures worse.
Although there have been pockets of solidarity in response to the coronavirus - Cuba sending medical personnel to Italy and China sending medical equipment to Poland, for example - some countries have stopped vital medicines, equipment and food from being exported to other countries.
Once the crisis has passed, some countries may continue turning themselves into fortresses, excluding outsiders, whether immigrants, refugees or foreign companies.
Nationalist, populist and extremist leaders and governments could ride the wave of post-coronavirus financial and emotional hardships, in the same way they did after the Great Depression. There is a real danger that the hardships caused by the coronavirus pandemic will lead to authoritarian governments coming to power in many countries, while those already in power become more entrenched.
If they do, the methods used to prevent the virus from spreading: sealing off borders, tracking infected individuals using surveillance technology and restricting people's movements, could be used for more menacing purposes.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand, and author of Restless Nation: Making Sense of Troubled Times (Tafelberg). This article was first published on Al Jazeera.
African countries are moving to make masks mandatory: key questions answered
- Shaheen Mehtar, Lucille Blumberg and Marc Mendelson
Wearing masks is being introduced in conjunction with maintaining a physical distance of at least 1.5 metres; following hygiene measures such as hand washing.
Many countries, including South Africa and Nigeria in Africa, are moving to make it mandatory to wear non-medical cloth masks when people are outside their homes. The move is seen as a vital additional measure to prevent the spread of SARS-CoV-2, the novel coronavirus causing COVID-19.
Wearing cloth masks is being introduced in conjunction with maintaining a physical distance of at least 1.5 metres and strictly following hygiene measures such as hand washing, good cough etiquette, and decontamination of regularly used surfaces.
Medical face masks have been a vital part of COVID-19 prevention efforts in East Asian countries such as China, Taiwan, Hong Kong and South Korea.
In countries where medical face masks are preserved for healthcare workers or are scarce, fabric face masks provide a cost-effective alternative. These can be homemade and are reusable.
There has been a growing movement of homemade mask production. Factories have also repurposed to produce fabric face masks to support commercial and free distribution.
In South Africa wearing a cloth mask in public places is now mandatory. In our view, there is sufficient evidence to suggest if everyone wears a mask, droplet transmission from each person will reduce and minimise exposure.
Transmission
The early phases of the COVID-19 epidemic included an evolving understanding of the routes of transmission of the coronavirus. It is now well established that droplet transmission is of vital concern. In the case of the severe acute respiratory syndrome coronavirus in 2002, viral shedding via the respiratory tract happened mostly after people developed symptoms. But COVID-19 includes a pre-symptomatic phase where people can be infectious and still feel healthy and be unaware that they are infected. Mildly symptomatic and asymptomatic cases also occur.
Mandatory masking ensures that viral transmission by any potential carrier is markedly reduced. It emphasises the concept of “source control”, in other words controlling the amount of a pathogen that is present in the environment. This is well expressed through the slogan: “I protect you, you protect me”. This was popularised by the #masks4all initiative, started by a group of researchers and scientists to promote the scientific evidence showing that cloth masks limit the spread of SARS-CoV-2.
An additional benefit of the ubiquitous wearing of face masks is the reduced possibility that respiratory droplets will be released to settle on surfaces – or for smaller aerosolised particles to float in the air.
For those still in doubt, we have answered some key questions to address the biggest areas of controversy:
Why should I wear a cloth mask? To prevent potential transmission of the coronavirus that causes COVID-19 via respiratory droplets and particles released when you talk, laugh, sing, shout, cough or sneeze, or to prevent the potential inhalation virus laden particles. A cloth face mask also serves as barrier that prevents touch transfer from surfaces to your mouth and nose and a reminder not to touch other parts of your face – especially your eyes. In addition, a face mask reduces the extent to which droplets and particles end up on surfaces or float in the air.
When should I wear a cloth mask? As a general rule, any time that you are outside your home, and especially in close contact situations such as when using public transport, shopping, working, or in any crowded setting. If a person in your household is possibly infected with coronavirus, face masks must be used when in close proximity, in conjunction with separating living quarters. Helplines and healthcare providers are good places to go for additional steps to follow.
Can I make my cloth mask out of anything? The most effective approach is to use a thicker weave material such as cotton for the outer layer, and then to include at least two layers of softer material for comfort and additional barrier protection. Test the materials combined for breathability before sewing. There should be some resistance to airflow, but you should be able to breathe freely when using the completed mask. Fit is important to minimise air bypassing the cloth barrier via the sides. Materials used should be easily washable and heat tolerant for cleaning. Stretchy material should be avoided.
How do I wear the mask? Never share a mask with anyone and always use a mask that is freshly cleaned. Wash or sanitise your hands before putting on the mask and when removing. Ensure that it covers the area from the top of your nose to below your chin. When you remove the mask, move your hands forward so you can fold the front over itself. Hold on the sides and place in a safe area for cleaning.
How do I reuse a mask? A cloth mask can be washed in hot water with soap or washed in a washing machine. Iron or sun dry. You can also drop the mask into boiled water and leave to cool to a temperature that allows you to wash the mask with soap or washing detergent. Avoid harsh chemicals such as bleach as this will be toxic when wearing the mask. By having two masks available, you can wear one, and have one to wash.
Dr Warren Parker a public health communications specialist, and Dr Beth Engelbrecht from the Western Cape Department of Health contributed to this article.
WITS COVID-19 UPDATE 27 – FINAL YEAR MEDICAL STUDENTS RETURN TO CAMPUS
- Wits University
Final year medical students will return to Wits on Monday, 11 May 2020.
Following the directive issued by the Minister of Higher Education and Training on 30 April 2020, final year medical students will return to Wits on Monday, 11 May 2020. This will require a limited opening of the Wits Junction Residence Complex and the Faculty of Health Sciences building, as well as the clinical training platform in various hospitals.
The University has prepared for the return of 314 medical students in their final year of the MBBCh and GEMP programmes. 91 students from this group will be housed in the Wits Junction on a self-catering basis.
An additional 142 medical students on the Mandela Castro programme will also be returning to continue their clinical training in hospitals. These students will be housed, as usual, in the Witwaters Building and at various hospitals.
We have implemented the following safety measures in compliance with all regulations and protocols, and with the advice of experts:
Residences and related facilities, offices and teaching venues have been decontaminated, including surfaces, equipment and ventilation systems. This has been confirmed by Wits’ Occupational Health and Safety Director and his team.
Sanitisers have been installed at all entry points, as well as at the entrances of all buildings.
Buses have been decontaminated and screens have been installed to separate bus drivers from students. Bus drivers have been instructed to ensure that buses are no more than two thirds full when transporting students to hospitals, in line with transport regulations. Physical distancing must be maintained on buses and masks must be worn at all times.
All students and employees will be expected to complete a confidential screening questionnaire every day (via an app) before being allowed onto campus, in line with national protocols. Temperature screening may be undertaken at the gates if this becomes necessary for any reason.
Staff and students will be issued with the proper Personal Protective Equipment, including the appropriate masks for medical students. At least two cloth masks will be issued to all other staff and students, who will be responsible for ensuring that they wear a newly-washed mask every day. It is compulsory to wear masks at all times when in open spaces, whilst using University transport and in clinical settings.
Physical distancing and good hand hygiene (preferably by washing hands with soap and water for 20 seconds at a time and drying properly) is compulsory.
In order to ensure our collective wellbeing, students and staff members are required to adhere to the stringent measures outlined above and to report immediately any violations of protocol to the Office of the Dean of Health Sciences via david.gray@wits.ac.za. Anyone who does not adhere to these requirements may be escorted off the premises by Campus Protection Services.
We would also like to extend our appreciation to our returning students, and to all Wits’ staff members who have meticulously prepared f or the return of this cohort, and who will continue to support them in the months ahead. These include in particular staff members from the following departments: Student Affairs; Services; PIMD; ICT; Protection Services; OHS&E; Finance; Faculty of Health Sciences staff, and other supporting units.
Remember to wear your masks and to practice physical distancing and good hand hygiene.
Keep healthy and safe!
SENIOR EXECUTIVE TEAM
8 MAY 2020
Health and safety in the spotlight as South Africa’s miners go back to work
- Nancy Coulson and Nicola Christofides
Miners face cramped working conditions, transportation in packed cages, and a high incidence of other respiratory diseases, posing considerable risks.
South Africa was put under strict social and economic lockdown on 26 March. By the end of April the government announced that it was easing some of the restrictions. This included allowing certain key sectors to begin operations once again. One of them was mining.
Mining is an important contributor to the South African economy. It employs around 450,000 people and makes a direct contribution of 8.1% to GDP. Approximately 78% of these people work on gold, platinum and coal mines that are largely underground operations.
Under the regulations easing the lockdown, mining can resume operation at 50% capacity and must provide health and safety protection from COVID-19. But the government guidelines were not binding on employers.
This decision led a trade union, the Association of Mineworkers and Construction Union, to take a case to the country’s Labour Court. At issue was the adequacy of the voluntary guidance about the COVID-19 response to protect mineworker health.
The case challenged the preparedness of the sector to protect workers.
The threat posed by COVID-19 on mines is considerable. Working conditions underground are cramped, transportation is in packed cages, and there is a high incidence of respiratory diseases.
The union argued that the hazard posed by the pandemic was too substantial for voluntary guidance and that both the mineral resources minister and the chief inspector of mines had failed to institute the necessary mandatory measures under the country’s Mine Health and Safety Act.
The judge agreed. As a consequence, measures to address COVID-19 are now compulsory for all mines.
One aspect of the union’s argument for compulsory guidance was that worker health and safety representatives appointed under the Mine Health and Safety Act would be unable to hold the employer to account without enforceable standards. Research we have done shows that worker health and safety representatives on South African underground mines are indeed in a weak position. Even with enforceable standards they will face an uphill task.
Case study research we conducted on four underground mines revealed the important, but hugely compromised role of health and safety representatives in a health response.
Health and safety representatives
The powers of safety representatives are largely universal. They include representing workers on all matters related to health and safety, conducting inspections and withdrawing workers from a dangerous workplace. They have the right to training and to resources to support them in their role.
On a large underground mine with more than 1,000 employees there are between two and four full-time representatives per shaft and sometimes hundreds of workplace representatives – those who take on the role of representative alongside his or her job of employment.
These arrangements are subject to agreements signed between the employer and recognised trade unions at a mine site. These agreements typically cover the number and election of representatives and their training and resourcing. Representatives are elected by workers and while the employer must ensure their training and resourcing, there is no requirement for workplace representatives to be paid. Full-time representatives are paid by the employer and this resembles arrangements for shop stewards.
Consultation by the employer with autonomous employee representatives is a central tenet of the Mine Health and Safety Act.
Our research made three major observations about worker representatives when it comes to health issues.
Firstly, that representatives were engaged in activities to address the existing triple disease burden on mines: occupational (lung disease and noise induced hearing loss), communicable (HIV and tuberculosis) and noncommunicable (diabetes and hypertension) diseases.
Workplace representatives acted as frontline health workers responding to the ill-health and emotional problems of production workers. They advised and counselled workers, encouraged visits to the clinic, escorted workers to the surface should they fall unwell, and reorganised workloads in the production team when workers were upset, weak or tired.
Full-time representatives acted as the compassionate voice for workers. This involved, for example, escorting individual workers to face bullying supervisors to address health related problems.
Secondly, representatives took on the responsibilities of the employer too. Full-time representatives took daily instructions (including some about health) from safety management. Representatives conducted inspections, gave education talks and policed the behaviour of workers on behalf of the employer. They also engaged in inappropriate problem solving, such as encouraging workers to use a cloth as a dust mask in the absence of personal protective equipment.
Representatives were often left feeling they would get into trouble with the employer if something went wrong. Representatives who challenged the production imperative by withdrawing workers from a dangerous workplace felt unsupported by the employer. We found approximately 30% of mineworkers who had withdrawn from a workplace went back despite believing it was still dangerous. Workers had little confidence that their health and safety representative could get the workplace fixed.
Thirdly, representatives were dominated on a daily basis by the employer and faced retaliatory employer actions. Supervisors threatened representatives who exercised their powers or had them removed from a workplace. In some instances, they lost their jobs.
We found that worker representatives were not an autonomous voice for worker concerns and therefore could not hold the employer to account. Nor could representatives rely on trade union support. The employer actively discouraged their reporting into trade union branch structures.
Employer appointed service providers, rather than trade unions, provided training and delivered the accredited skills programme. Not one representative in our research knew their powers correctly under the law – even after training. Neither did they have instruments for routine tests, such as for dust, or access to the internet to support their role.
Dangers
For worker representatives to fulfil their role, mandatory standards for COVID-19 protection are a first step. But more needs to be done.
International evidence shows there are broad preconditions necessary to support the effectiveness of worker representation. These include trade union training and support for worker representatives; a supportive steer from the regulator, which could include dedicated guidance about the role and resourcing of worker representatives; and an appreciation by the employer of the autonomous role of representatives.
Mine health and safety has become more complex under COVID-19. A bold step to resource and equip health and safety representatives is now needed.
South Africa’s COVID-19 testing strategy needs urgent fixing: here’s how to do it
- Marc Mendelson and Shabir Madhi
Early reports by the National Health Laboratory Service indicated that it had the capacity to do 30,000 tests a day. But capability to do so has not materialise
The COVID-19 epidemic in South Africa is now in its exponential phase. Cases are rapidly increasing in many areas. This is most apparent in the Western Cape province, which could be due to higher rates of testing per capita, coupled with a more selective testing strategy than in other provinces.
The doubling time of mortality in the province’s Cape Town metro is now 8-9 days, indicating a rapid increase in the number of severe cases and deaths from COVID-19. Although the health system is better prepared as a result of the initial lockdown, major cracks are starting to show. This is causing a deterioration in clinical service which, if not stemmed, threatens the country’s response to the epidemic.
Globally, rates of testing for SARS-CoV-2 infection have varied between and within countries. For example, testing rates (per 1,000 people) range from 148 in Iceland to 0.76 in India. In South Africa, as of 3 May 2020, the testing rate was 4.5. The high demand globally for molecular assays (known as PCR) to identify infectious cases has led to a shortage of samples and kits required in laboratories.
In South Africa’s case, the rise in the number of cases in the Western Cape, and the pressure this is putting on laboratories charged with processing tests, is only the forerunner. Here, we explain what needs to be done, and why.
Turnaround time
Diagnosis of COVID-19 relies on a laboratory test that is simple, but laborious. The time taken from the sample being taken to communication of the result – the “turnaround time” – is influenced by a number of factors. These include the speed at which the sample reaches the lab, the lab’s capacity to run the test – access to reagents and test kits, number of analysis machines, availability of staff, errors leading to a need for re-testing – and the communication process.
Early reports by the National Health Laboratory Service indicated that it had the capacity to do 36,000 tests a day by the end of April 2020. But capability to do so has not materialised.
Currently, the number of tests received in laboratories exceeds their capacity to deliver results within 12-24 hours of sampling. In many parts of the country, turnaround time has increased from 24 hours to over 5-14 days. According to correspondence we have seen, some labs with the capacity to do 1,000 tests a day have a backlog of 10,000.
Why is “turnaround time” so critical?
South Africa’s ambitious community testing programme relies on identifying infected persons, isolating them, tracing their contacts, and isolating or quarantining them.
Identification of infectious cases – even if only a quarter of those who are infected are identified – coupled with adequate tracing of their contacts and ensuring isolation (of cases) and quarantine (for up to 14 days) of test-negative contacts, could assist in slowing the rate of community transmission of the virus.
This would mitigate the expected surge in severe COVID-19 cases occurring over a very short period of time. Healthcare facilities could be better equipped to deal with the expected surge of COVID-19 cases over the next 2-3 months.
But for such a strategy to be effective requires a clear line of sight in terms of efficiency of testing, isolation of cases as quickly as possible (within 12-24 hours of being tested), and effective and immediate tracing of their close contacts.
It is estimated that any single case will, on average, have 20 close contacts (probably higher in South Africa) who should be traced. These include any close contacts (someone who spends more than 15-30 minutes within 1.5 metres of the person) occurring from at least 2-3 days prior to symptom onset in the identified case, and up until the case has been isolated. Assuming that isolation occurs on the third day after symptoms appear, for each case there would be approximately 120 close contacts to be followed up.
For this strategy to assist with slowing the spread of the virus requires tracing (and physical contact for screening for symptoms) of approximately 80%. Although possibly achievable in the initial phase of the epidemic, it becomes an unrealistic goal to aspire to when identifying 400 “new cases” each day, as that would require tracking and physical tracing of approximately 5,200 contacts.
This is why the turnaround time matters. A delay means that the current “new” cases reported in South Africa reflect cases that were likely sampled approximately a week ago.
This points to the need to shift the focus of PCR testing to patients being admitted to the hospitals. This would inform the management of the patient and limit the likelihood of spread within hospitals.
But the turnaround time for this cannot be anything more than 12-24 hours if it is to achieve any of these goals of testing. When a person with COVID-19 is admitted to a hospital, it is critical that they do not infect others. We achieve this by triaging patients into those who are COVID-19 suspects (a “person under investigation”) and those who are not. We separate patients into different wards accordingly.
Slow turnaround time for tests means a delay in diagnosis. The longer the turnaround time, the worse it gets. As the epidemic accelerates in South Africa, the number of patients needing to be admitted to hospital as a “person under investigation” and subsequently COVID-19-confirmed cases rapidly rises, and the system becomes overwhelmed.
This is why we are arguing for a wholesale change to the current system.
How to fix the faults
We believe the following crucial steps need to be introduced as a matter of urgency.
Stop the testing and contact tracing components of the community surveillance programme, in favour of self-reporting of symptoms via an app-based programme on mobile phones. We believe there is sufficient mobile coverage and access to do this. This would allow monitoring of disease activity, and self-isolation of symptomatic people for 14 days on the probability of COVID-19 infection. If resources allow for testing to confirm negative status sooner than 14 days to accelerate early return to work, that should be considered, but not at the expense of undermining turnaround times in hospitalised patients.
Steps need to be taken to map the spread of SARS-CoV-2 in communities. This should be done by gathering evidence on the seroprevalence, which can be measured using rapid antibody blood tests to detect recent or past SARS-CoV-2 infection (but not whether currently infectious). Geospatial mapping of the epidemic could assist in a more measured and informed approach for developing district or regional strategies to reduce the rate of community transmission. It could also help inform anticipated demands on healthcare services.
Focus testing resources on specific groups of people for whom a rapid turnaround time result will effect significant change.
Allow rapid diagnosis of hospitalised people under investigation, which allows optimal case management of severe COVID-19, optimal infection prevention and control, and patient flow to enable hospitals to cope with the escalating numbers as we climb the exponential curve to the peak.
Rapidly isolate and quarantine symptomatic healthcare workers and their close contacts to limit hospital outbreaks.
Introduce high risk group surveillance and testing, including patients and staff at long-term care facilities.
Convene an intersectoral government task force to analyse the barriers to operational flow of the entire testing system and make recommendations for a new testing strategy.
Lockdown is riling black and white South Africans: could this be a reset moment?
- David Everatt
It is rare for a post-authoritarian society to get two chances to reconcile. This may be just that, for white South Africans in particular.
The South African government seems to have gone from an absence of data coupled to a firm but sensible strategy of lockdown to delay the pain of COVID-19, to a multitude of inputs and a seemingly cavalier attitude to the restrictions.
Academics and NGOs have done the same, focusing primarily on the economy and poor people in particular. Many others have followed, with data or models or both.
Something has changed – the government or citizens?
Capriciousness
It is remarkable how quickly South Africans have lost the sense of camaraderie and support for a strong leader, and begun to complain rather about crypto-fascist authoritarianism. This was exacerbated by government as it introduced a “Stage 4” that was meant to be lighter than “Stage 5”.
On 1 May, when the relaxed restrictions kicked in, the roads were full of runners, walkers, shufflers, cyclists in their spandex, and dogs of every type. As he faced a sea of (mainly) white faces jogging on Cape Town’s Promenade, Police Minister Bheki Cele threatened:
I saw this thing of running, I think we will be making some form of recommendation to the National Command Council about it.
I saw … people running in clubs, walking with their dogs and they were even swimming – something that is [criminalised] in the regulations…
And in case anyone was in doubt about who had power, he added: “we can forget about Level 3” because such terrible behaviour meant citizens did not “deserve” it.
It is that final throw-away line that grates. This is not for citizens to “earn” or “deserve” because they behave well, it is meant to be a science-driven risk-based analysis that determines stages 1-5. But now it smacks of capriciousness, with more than a hint of pay-back.
South Africans – regardless of race or class – picked this up as they watched Cooperative Governance Minister Nkosazana Dlamini-Zuma announce the reversal of a promise of tobacco sales being allowed under “Stage 4”, made earlier by President Ramaphosa. Similar to Cele telling them whether they “deserve” stage 3 or not.
Virtually all research into racial attitudes in South Africa has shown racial differentiation growing. This was most easily shown in the 2019 elections. These differences seem increasingly to be replaced by a shared hostility towards an ANC government that appears to be making rules up as they feel like it, and whose own ministers clearly feel above COVID-19 – and above citizens.
Throwback to an inglorious past
Are citizens protected by evidence-based interventions, or are they being jerked around by mean-spirited politicians?
If the country steps back, is there not something worth learning now, particularly for white South Africans?
Think about it. You can’t go to work or school or to the park unless government says you can. Your freedom of movement is severely limited. You’re told when you’re allowed out, and you are supposed to have a permit akin to a dompas (dumb pass), to prove you’re legally out. (The dompas was the demeaning identity document all black people were required to carry during apartheid rule, which controlled their movements.)
And the troops and police are there to ensure you obey, or beat the hell out of you. Your behaviours are deemed foreign, not normal. You can only enter certain shops, and only after you are sanitised (because you may be dirty or a vector of disease) and you can’t buy alcohol or cigarettes. And other than a small handful, your work is not essential and government will decide for you if you can work or not.
White South Africans right now have a rather comfortable, tiny insight into what life under apartheid was like. It can be a powerful moment to empathise with what it was like to be black under apartheid – and this time, blacks and whites are all being treated the same.
They are all irritated by a government that seems bent on exercising power in small, nasty ways. That’s why this can be a great moment, because black and white South Africans really are all in this together, and they all increasingly dislike their government together.
If white people can stop acting as if they are individually and personally being attacked, and understand the shared nature of both unhappiness and anger, there is real potential for some (much delayed) healing.
As the global economy tanks, whites with retirement policies and shares and businesses are being hit in the pocket. Society and the economy, they are told, are never going back to normal – they have to reset in different, as yet unknown ways.
Can they?
Never waste a good crisis
If South Africa has to reset, can its people – consciously and together – treat this as the real “miracle” moment? A lot of good work has been done since apartheid, which advantaged the white minority to the detriment of the black majority, ended in 1994. Millions of people now have clean water, water-borne sewerage, electricity, tarred roads, street lights and the like. Quite a few more have tertiary education, and some have wealth.
According to most studies, reconciliation has not fared well. Racism, racial redress and patronage have made short work of the noble goals of the early 1990s.
We should see the last 26 years as South Africans’ infrastructural investment for the real “new South Africa” to be able to emerge.
If we assume that the society matters more than simply repeating “it’s the economy, stupid!”, now is the chance to be different, and to reset to a new social reality. Wealth has been destroyed by COVID-19, and it has laid bare the lines of inequality for all to see. So, talk of a wealth tax sounds rational, not punitive, in the post-COVID-19 context.
South Africans can come out of lockdown as a more empathetic and united people – even if united in irritation or anger at a capricious government that seems to regard evidence-based decision-making as meaning regulations chop and change according to ministerial whim.
Can they use this moment to look beyond “race” and see a shared humanity?
It is rare that any post-authoritarian society gets two chances to reconcile. This may be just that, for white South Africans in particular.
What should South Africa’s coronavirus endgame look like? Here are some options
- Alex van den Heever, Imraan Valodia, Lucy Allais, Martin Veller and Willem Daniel Francois Venter
SA's response to the COVID-19 pandemic was one of 'intervene first and ask questions later'. Now is the time for government say what its strategic endgame is.
South Africa has aggressively intervened to contain the local SARS-CoV-2 viral epidemic. But it is far from clear which strategic outcome is being pursued. Is it following the lead of countries such as New Zealand or South Korea and trying to stop virus transmission altogether until a suitable vaccine becomes available? Or is it attempting to manage the infection rates so that extreme peaks in morbidity are prevented?
As the government’s strategy is not currently explicit, the intervention framework implemented so far appears consistent with a wide range of possible policy objectives. The rapid emergence of the pandemic defaulted policy to intervene first and ask questions later. But the dust is now settling, and the strategic endgame can and should be made transparent.
Any strategy requires a rational combination of what is known with what isn’t. What’s not known includes the possible outcomes of interventions, as well as contingencies that can materially influence the trajectory of the disease. Given the substantial uncertainties of disease elimination, South Africa should adopt at least a multi-year strategic perspective – that is the time until a vaccine or treatment is probable and has been implemented.
The strategy should, however, allow for the possibility that each month introduces more certainty about the success of public health interventions and the options for treatment and vaccines.
We discuss three possible approaches, and consider the efficacy of each.
What’s known, and what’s not known
The various options mapped out below take into account what is known, and what’s not known.
What’s known. First, the SARS-CoV-2 virus is highly infectious. In the absence of interventions it has an average reproduction rate (R or R0) every four days of roughly 2.5. Infections are also associated with levels of morbidity and mortality that make an active public health response necessary.
Second, no vaccine is available yet and no drug has been shown to prevent transmission of the virus.
Third, no virus-specific treatments exist to mitigate the current levels of morbidity.
Fourth, the complexity of the economic and social problems arising from general lockdowns means it is very difficult to rely on extended lockdowns without creating a new range of severe socio-economic problems.
Where does uncertainty lie?
First, the extent to which reliance can be placed on social distancing and lockdown strategies in South Africa’s high-density, poor and informal settlements is in question.
Second, South Africa appears unable to get testing to the levels necessary to successfully manage a health prevention strategy based on testing and contact tracing. This is true of a number of well-resourced countries too.
It is also unclear whether South Africa is able to ramp up testing, and associated isolation of those infected or their contacts, to the level needed to stay ahead of the epidemic during the course of 2020.
Third, it is unclear when a vaccine will become available. Even under ideal circumstances, it is likely that it will only be available for wider use in 2021. And even with the development of suitable vaccines, it may still take years to eliminate the virus.
Fourth, therapeutic options based on existing treatments, which could be available soon, are still speculative and unlikely to prove wholly successful.
Fifth, therapeutic options based on new technologies are unlikely to be available in South Africa until the latter part of 2021.
Strategic options
Option 1 is to target complete disease control within 2020, without waiting for a successful treatment or vaccine to be introduced. This would require that public health interventions achieve a sustained reproduction rate of the disease (R) below 1. This would require selective, targeted lockdowns, ongoing social distancing and high rates of population testing, tracing and quarantining.
Option 2 is to keep new infections relatively low, but accept that the epidemic will continue until a vaccine or some other treatment becomes available. This strategy would require keeping the R at around 1, by limiting daily, country-wide new infections to roughly 250 to 300. This approach is premised on the assumption that no public health approach, or other intervention, will be able to eliminate the epidemic in 2020, and also not completely in 2021. It assumes that a combination of treatment and vaccinations will eliminate the virus during the course of 2021.
Option 3 is to keep new infections sufficiently low that they prevent excessive morbidity at any point in time to avoid health services becoming overwhelmed, but sufficiently high as to achieve early herd immunity within, say, the next 18 months. While this approach assumes an average R of more than 1 for an initial period and roughly 1 thereafter, the daily levels of new infections would be higher than option 2, but should still be kept manageable using targeted public health interventions.
Process of elimination
Of the above, the third option – allowing infections to rise to achieve herd immunity – is ill-advised, at least for now. To achieve herd immunity over a period of just two years, assuming that only 60% of the population would need to have achieved immunity, would require roughly 51,000 new infections per day. At these levels it can be expected that more than 2,500 people will require hospitalisation each day and that approximately 500 will require intensive care, most of whom would die.
This option can also be rejected on rational grounds. If it is possible to maintain the R at about 1 over an extended period using public health interventions without undue economic hardship, it makes sense to manage a lower rather than a higher and more risky level of infections.
This leaves options 1 and 2. The choice comes down to what is achievable with South Africa’s public health and economic capacities and capabilities. Both options, however, must be compatible with the maintenance of a functioning economy.
A generalised lockdown is unlikely to succeed as a preventive option in the South African context. As a result much depends on whether more focused public health measures– such as testing and contact tracing, social distancing, employer health protocols, generalised requirements to wear masks and border management – are sufficient to hold R at 1 or below 1. If these interventions can’t be relied on, the outlook for South Africa would be bleak, as a runaway epidemic would be more, rather than less, probable. The de facto consequence would be option 3.
But it’s plausible that a strategy that is able to maintain a low level of daily new infections over a two-year period could hold out the opportunity for disease elimination if public health prevention improves over time.
For instance, while significant constraints exist to scale up testing in the short term, these can reasonably be expected to lift progressively over a 12-month period. Similarly, it is not unreasonable to expect the specificity and speed of contact tracing and quarantining to improve over time. It is also common sense for testing priority to be given to communities where transmission risks are highest – such as townships and informal settlements.
The direct costs of many of these interventions may appear large. But when compared to the indiscriminate impact of a general lockdown, the additional resources required pale into insignificance.
Conclusion
The current best option is for the government to pursue option 2 as a minimum strategic goal – keep new infections relatively low, but accept that the epidemic will continue until a vaccine or some other treatment becomes available to allow for societal immunity. With a continuous expansion of key public health interventions, such as testing, tracing and quarantining, this approach also offers some hope of achieving option 1 – to target complete disease control within 2020.
Keeping open the option of disease control through targeted public health measures within 2020 is plainly worthwhile, even if it is far from certain until treatment and vaccine options become more concrete.
Choices in a fog of uncertainty: lessons for coronavirus from climate change
- Robert (Bob) Scholes, Albertus J. Smit, Francois Alwyn Engelbrecht, Guy Franklin Midgley, Jennifer Fitchett, Neville Sweijd, Pedro M.S. Monteiro and Pravesh Debba
The science to policy process that was developed to guide climate mitigation decisions can be applied to the response to the COVID-19 pandemic.
Governments around the world, driven by the threat of overburdened health systems and mass mortality resulting from the COVID-19 pandemic, are being forced to make decisions that have enormous, long-lasting consequences for lives and economies. They are doing so without sufficient assurance that the choices they make are the best ones.
The fog of uncertainty can be partly lifted by better use of information that’s emerging around the world. But it will never completely clear.
The most difficult choices are those that have to be made before you know how they will work out.
The challenge of making high-consequence decisions based on imperfect knowledge is not unprecedented. For example, tough policies to mitigate climate change must be adopted long before the world crosses catastrophic thresholds. To guide these decisions, countries rely on imperfect models of the climate system, along with divergent and values-based assumptions about how the future could unfold.
Scientists and policymakers, working together over a period of three decades through the Intergovernmental Panel on Climate Change, have worked out how to guide decisions in the face of uncertainty in such a way that there is broad agreement, and which minimises regrets even if the future does not work out exactly as projected. Their approach has allowed scientists to remain providers of evidence, and politicians to focus on value-based choices.
The Paris Agreement to mitigate climate change, signed by 197 countries, was the result of a well-functioning science-policy interaction.
This experience can be applied to the response to the COVID-19 pandemic, without having to reinvent the process.
The best practice guidelines involve making decisions based on the best available information at the time, and progressively improving them in the light of experience and emerging new information. Secondly, they involve using a “multi-model approach” and an ensemble of results, rather than placing all bets on a single prediction. And finally, they use collectively agreed scenarios to explore the full range of options and outcomes.
Three-pronged approach
Decisions about containing COVID-19 are inevitably a balancing act between reducing the immediate loss of lives on the one hand, and protecting livelihoods that could be damaged as a result of the actions taken on the other. The models used to support the decisions must be similarly balanced. There is no point in having precise projections about the course of the pandemic, but only a vague idea of the impact on the economy.
At present, these different streams of information are not well integrated.
For the case of using mathematical models to help guide COVID-19 policies, we make the following suggestions based on our collective experience with scientific assessments.
Use what information is available, then adapt: The novelty of the disease means you start from knowing very little and taking guidance from experiences with similar diseases in the past. You work towards improving modelled projections, using information from a range of sources – from science to public health to the economy.
Nimble and efficient channels of communication ensure that the pace of modelling matches the urgency of the problem.
The multi-model approach: Using several different models rather than one relies on the same logic that tells you not to put all your savings into a single asset. The most robust approach is to build a portfolio, which is collectively stronger than just one, particularly if they are based on fundamentally different assumptions.
Typically, different models have different purposes, and some are stronger in some respects than others. Some models are good at short-term projections while others are better in the long term. Including more detail is necessary for some purposes, but a less detailed model may be sufficient, and more reliable, for more general policies.
This does not mean you should not winnow out models that are simply wrong. But to do so you need a well-structured, evidence-based test. The statistician George Box wisely commented that “all models are wrong, but some are useful”.
For modelling COVID-19 we would similarly encourage a diversity of models.
Scenarios: Some things cannot be predicted accurately, because they depend on chaotic physical processes, or behaviours that defy simple representation, such as human choices. For these issues you use scenarios. Scenarios allow the models to be stress-tested, by asking questions such as: What is the range of possible outcomes? How does my decision play out in the worst case, as well as in my preferred case?
The scenarios must be shared between models, or you are unable to tease apart differences in the way models work from differences in model drivers.
The scenarios need to be plausible, but must span a wide range of possibilities if they are not to lead to confirmation bias – our tendency to choose the outcomes that support our prejudices. It is important to include measurable indicators, so that you later know which scenario is playing out.
For COVID-19 we recommend exploring the model predictions over a range of agreed scenarios. For example, one scenario can impose strict lockdown and maintain it over several months. Another can progressively relax the restrictions. And both can be compared to a reference scenario where no policy action is taken.
When many models, several scenarios and uncertain data are used together, the result will be a wide range of predictions. The differences need to be evaluated so it’s clearer which findings have the most supporting evidence.
Public trust is key
The balancing act of managing COVID-19 requires public trust, which is fostered by an open, clear and credible process of decision-making. The framework we propose is focused on providing the information needed to make good decisions, but should not assume the right to make the decisions. For that purpose, people elect political leaders to represent their rights and values.
This approach has been successfully applied elsewhere, for instance in the protection of the ozone layer, and mobilising action to halt biodiversity loss. In South Africa, it recently aided sensible decisions regarding fracking in the Karoo.
Information pertaining to the screening of staff and students entering University campuses and premises.
Government Directives pertaining to Covid-19 obligate employers to implement a Covid-19 Screening Tool to ensure that employee / student health condition is monitored.
In view hereof,
Staff / students must use the Covid-19 Screening Tool on a daily basis to monitor whether they are showing any Covid-19 symptoms.
This must be done before staff / students leave their homes to come to Campus.
Assuming staff / students have completed the forms to indicate that they do not display any of the symptoms – including having not been exposed to or in contact with any individuals who may have been diagnosed, been in self-isolation or in quarantine for the past 14 days, and do not suffer from any other risk factors; please drop the completed form in dedicated boxes at the entrances.
Further notes regarding the Covid-19 Screening Tool:
Please conduct daily self-screening before leaving home / residence and before coming onto Campus. Follow the flow diagram should symptoms be experienced.
If any symptoms mentioned in questions A1 to A10 are experienced then don’t attempt to enter the University. Consult your Healthcare Worker to determine whether further testing / self-quarantine will be necessary. If cleared by your Healthcare Worker only then may you enter the University. If you reside on Campus and experience Covid-19 symptoms then please remain in your room and seek advice telephonically from relevant CHRL staff and/or your Healthcare worker.
If tested positive for Covid-19 (and, if you do not require hospitalisation) then self-isolate for 14 days. Follow your Healthcare Worker’s advice.
If you are not able to come to Campus due to experiencing Covid-19 type symptoms, or due to being tested for Covid-19 (or after being positively diagnosed) then urgently notify your Supervisor/ relevant Manager about your situation / absence.
If you answered “YES” to any of the questions in Section B1, B2, C1 and C2 (but have none of the usual Covid-19 symptoms mentioned in sections A1 to A10, then this does not mean that you will be refused entry onto Campus (but a decision may be necessary as to whether this requires further intervention).
If “YES” is answered for the questions in sections A1 to A10 then this does not mean that you definitely have Covid-19. This screening tool is used merely as a pro-active precautionary indicator to establish whether further tests should be carried out in order to make a definite diagnosis.
If you reside on Campus then please follow the CHRL protocols on notification / quarantining should you experience Covid-19 symptoms.
Nothing prevents a person that experiences any of the usual Covid-19 symptoms to immediately bring these to a Healthcare Workers attention at any time of day / night should these symptoms present themselves.
Service provider and contractor employees are expected to have a Screening process in place for their staff (preferably using the same standard of screening that Wits staff / students are using).
A flow diagram has also been developed and which explains the Covid-19 screening / testing / management process to be followed at Wits. This process flow must please be adhered to:
Covid-19 Update (28) - Wellness services for students and staff
- Wits University
A reminder to all students and staff about Wits' mental health and wellbeing services that are available to you during the Covid-19 pandemic and lockdown.
The majority of our staff and students have been home for 50 days now and given the many changes, it is expected that some individuals and families may be finding it difficult to deal with the disruption to normal life. We remain concerned about your well-being and want to remind you of a number of services available to staff and students during this period.
Help for students
The Wits Student Crisis Line is available 24/7/365 on 0800 111 331 to all Wits students who require counselling, including those feeling anxious or uncertain during the lockdown.
Students who require personal, career or life coaching counselling services can email the Counselling and Careers Development Unit (CCDU) via info.ccdu@wits.ac.zabetween 08:00 and 16:30 on weekdays. A professional team member will respond with assistance. Zoom sessions and some group sessions are also available, depending on the need.
The CCDU Lockdown Wellness Chronicles offers daily coping strategies that can be used by all. The site has daily prompts to help structure and regain control of life and also to prepare for normalcy. The May Motivation seriesis a useful resource to assist students. Visit the CCDU website for more information on various mental health and wellness topics.
The Campus Health and Wellness Centre is available to assist with primary healthcare and mental health enquires:
Primary healthcare enquiries – Call 0743077259 or 0824832251
Mental health enquiries – Call 0766093924
A satellite Campus Health and Wellness Office is open on the Wits Education Campus from 08:30 to 12:00 on weekdays, in order to assist the final year medical students who have returned to campus.
Help for staff and immediate family
The Wits Impil’enhle programme offers free services to staff and their immediate families who require counselling for stress, anxiety, abuse, trauma, parenting, relationship and marriage-related problems. They also offer legal and financial advice. This independent service is offered through Kaelo Lifestyle and is provided in all South African languages 24/7. Call 0861 635 766 OR dial *134*928 OR send a ‘Please call Me’ to 072 620 5699 OR Email asknelson@kaelo.co.za for assistance.
Gender-based harm
During this time of lockdown, we are aware that there are some people who will find themselves in spaces where they may not feel safe. The Gender Equity Office (GEO) can be reached via email on info.geo@wits.ac.za. Alternatively, call the national gender based violence command centre on 0800 428 428 or send a "Please Call Me" to *120*7867#. It is important to remember that should you require a restraining order, courts continue to operate for this purpose. The GEO is available to guide you through the process and prepare you for what to expect when you apply for the order.
Cyberbullying
Cyberbullying involves the use of the internet or technological devices to send, post text or images intended to hurt, embarrass, discriminate, threaten, torment, humiliate or intimidate an individual or a group of people. Cyberbullying and harassment may become more common as the digital sphere expands and technology advances. For confidential reporting, consultation and support, contact the Transformation and Employment Equity Office via Cecilia.Smith@wits.ac.za or Advocate Mahlako Neo on neo.mahlako1@wits.ac.za. The Anti-Discrimination Policy can be accessed viawww.wits.ac.za/transformationoffice.
Covid-19 resources
Read more about the coronavirus at www.sacoronavirus.co.za or call the emergency hotline on 0800 029 999. The WhatsApp support line is 0600 123456. The website of the National Institute for Communicable Diseases also hosts a wealth of information on the coronavirus. Visit www.nicd.ac.za for daily updates and more information.
Remember to always:
Wear a face mask in public areas,
Practice physical distancing,
Wash your hands for at least 20 seconds with soap and water (and dry it properly) or sanitise,
Take care of your families, friends and loved ones during these difficult times.
Senior Executive Team
15 May 2020
What South Africa needs to forge a resilient social compact for Covid-19
- Erin McCandless and Darlene Ajeet Miller
Ramaphosa's call for a new social compact will fall on deaf ears unless there are some fundamental changes to the way in which the pandemic is being managed.
South African President Cyril Ramaphosa has called for “a new social compact among all role players – business, labour, community and government – to restructure the economy and achieve inclusive growth”.
In South Africa, ‘social compact’ has often been used narrowly to describe pacts between stakeholders on specific sectoral issues. A resilient social compact, as we use the concept, requires a dynamic agreement between the state and society on how to live together, and how to address issues of power and resources.
For such an agreement to contribute to peace and societal well-being, it must be reflected in the mechanisms, policies and responses that uphold the agreement. This needs to be done in a way that’s flexible and responsive, especially in times of crisis.
This approach recasts the concept of social compact (or social contract) as a tool for addressing issues of conflict, crisis and transition. Research across nine countries, including in South Africa, found that social cohesion is a key driver. Social cohesion builds on the concept of social solidarity, which lies in areas of trust and respect, belonging and identity, and participation.
Its achievement also rests on progress by other drivers. These are inclusive political settlements addressing core issues dividing people, and institutions delivering fairly and effectively.
To move in the direction of a resilient social compact, Ramaphosa’s call will fall on deaf ears unless there are some fundamental changes to the way in which the pandemic is being managed.
Solidarity and cohesion
The first is that there needs to be a critical focus on how vulnerable groups are affected differently.
South Africa’s stark socio-economic inequalities – within and across racial groups – are core issues that continue to divide people. This is true economically as well as spatially, psychologically, socially and politically.
Lockdown restrictions, therefore, affect people differently. In townships – apartheid-era residential areas that are predominantly black – loss of work means loss of livelihoods with grave challenges accessing food, health and education. Suburbanites – who are mostly white – on the other hand, have tended to be more preoccupied by loss of freedoms related to jogging, dog-walking, and accessing liquor and cigarettes.
These differences demand, secondly, that greater attention be given to how policies are being implemented.
Addressing these issues could ensure that social cohesion and social solidarity are nurtured through this crisis.
People need to feel included and that they belong – and that policies and practices deliver on expectations and agreements. When this fails, and human rights are violated in the process, these bonds and relationships suffer. Trust in the state, its institutions and associated legitimacy needed for their functioning, falters.
Human rights abuses by the security forces in the wake of the lockdown have included shootings, baton and gun beatings, teargassing, humiliation, abusive language, water bombing, invasion of private backyards, and even death. This has occurred especially in townships.
The UN High Commissioner for Human Rights recently identified South Africa as among 15 countries where human rights violations associated with COVID-19 restrictions were most troubling.
What’s missing
In the current COVID-19 context we are seeing fissures that dangerously undermine the bonds and relationships between the state and citizens. These are common in fragile and transitional contexts.
Many security forces members are following on the path Ramaphosa set with his peaceful messaging to guide them in defending citizens against the pandemic.
These abuses echo the experiences of black South Africans under apartheid when obedience was secured with authoritarian rule and aggression.
In addition, developing a national COVID-19 response has brought glaring inequalities to the fore – and the country’s persistent racial geographies.
These too challenge the goal of achieving a resilient social compact.
Resentment among some township residents has grown, and various forms of civil disobedience have resulted. Vuyo Zungula, leader of the African Transformation Movement, one of the smaller parties represented in parliament, observed on his Twitter page:
Until I see Whites, Indians getting the same treatment for breaking the Lockdown rules I will view the SANDF and SAPS as the enemy of the people.
Way forward
If the lockdown is enforced through coercion rather than consent, and the dignity of citizens is not respected, a resilient social compact won’t ever be viewed as anything more than rhetoric.
COVID-19 presents profound challenges for citizens and the state. Building trust and cooperation, between state and society, and between social and stakeholder groups in society, is paramount.
What then is needed?
First, there needs to be vigilant government commitment against coercion. Swift action must be taken against abuses by the security sector. And there needs to be effective communication with those affected by the abuse. This should accompany strong assurances of accountability and justice, and upscaled training of the military and the police in crisis response functions.
Second, two-way communication channels that offer the means to build trust and legitimacy of government actions need to be established. These should focus on fostering innovative ways for citizens to access information and participate in crisis response strategies. This can occur through surveys, via radio and mobile applications, or radio call-in shows.
Township and suburban residents must take part in the security and other crisis response measures. Widely accessible and consistent messaging is needed, such as the township education undertaken by the C-19 People’s Coalition. The alliance brings together social movements, trade unions, and community organisations working to provide an effective, just and equitable response to the pandemic.
Its members distribute leaflets in Gauteng townships in local languages, as they demonstrate social distancing and the wearing of masks while they mobilise and strengthen networks of food production, distribution and consumption. These may well have benefits beyond the COVID-19 crisis.
Finally, social solidarity is forged when each segment of society works together for the greater social good. Such efforts are widespread in South Africa and around the world. These stories need to be shared with a view to strengthening longer-term transformation efforts in the country.
South Africa’s COVID-19 strategy needs updating: here’s why and how
- Imraan Valodia, Alex van den Heever, Lucy Allais,Martin Veller, Martin Veller and Willem Daniel Francois Venter
South Africa should base its COVID-19 mitigation strategy on the premise that the pandemic will last for two years unless a vaccine is developed before then.
Decision-making at the early stages of the SARS-CoV-2 pandemic (the coronavirus causing COVID-19) was constrained by a paucity of medical evidence and epidemiological data. Knowledge gained over the past two months can therefore inform the next phase of the strategy.
In the context of the initial uncertainty, South Africa’s early lockdown was prudent. It allowed time to prepare the health care system, to ramp up wide-spread testing and to introduce other measures to reduce transmission rates. Extending the lockdown is no longer required. It is also no longer reducing transmission rates and has become unaffordable.
Current evidence indicates that:
It is impossible to eliminate the virus and the spread will continue. Only a few countries have been able to minimise the rate of spread but they remain highly susceptible to repeated outbreaks.
The majority, approximately 70%, of people infected with SARS-CoV-2 are asymptomatic, or have a moderate, self-limiting illness (approximately 25%). The 5% who develop severe COVID-19, with the risk of dying, are usually older than 65 years (greater than 80%) or have underlying comorbidities (such as hypertension, diabetes and obesity).
Children under 18 years are generally spared from developing severe COVID-19 and contribute less than 1% of all COVID-19 deaths (none among the more than 30,000 COVID-19 deaths in Italy).
It is not likely that a vaccine will become available in the near future. Without this, control of the infection would require about 60% of the population to develop immunity. This will take time and while there is considerable uncertainty over the number of deaths that may occur from COVID-19 over the next two years. Current evidence suggests that it may be less than originally estimated.
An extended lockdown comes with substantial health costs. These include costs brought about by undermining public health initiatives such as immunising children against threatening diseases and in the impaired provision of health services to those living with comorbidities such as diabetes, tuberculosis (TB), HIV and hypertension. Indeed, there is evidence that currently the gains made over recent years in reducing the rates of, and deaths from TB are being reversed.
SARS-CoV-2 is highly infectious, with a reproduction rate every four days of roughly 2.5 at the onset of the outbreak. The reproduction rate measures the number of people to whom an infected person will pass on the virus. When South Africa introduced the lockdown, the reproduction rate was low relative to other countries. However, South Africa’s reproduction rate has remained above 1, even under a highly restrictive lockdown. Indications are it will remain above 1 at least for the foreseeable future.
The hard, extended lockdown has come at significant economic cost. While there is debate about the cost to date, with estimates from 5%-16% of GDP, economists agree that this has been significant.
The lockdown has also imposed social costs. For example, children are missing out on schooling. This is detrimental for their cognitive development and for many other reasons. Children are at risk of becoming malnourished due to missing out on school feeding schemes, as well as from the increasing number of families that are being pushed into poverty.
South Africa needs to accept that it is not on a unique trajectory. The virus cannot be eliminated. The country’s strategy needs to move away from a hard lockdown. In our view, South Africa should focus on using interventions aimed at slowing the virus’ transmission rate.
The success of these interventions depends on the buy-in and cooperation of citizens. The message to South Africa must be clear: It is not going to be spared deaths from COVID-19. But it is possible to prevent some of these through our own actions and by promoting strategic public health interventions. South Africa should plan to mitigate the effects of the pandemic using the above strategies for at least two years, or until a vaccine becomes available.
Areas of uncertainty
There are two important areas of additional uncertainty. The first is that it is too early to establish the effect of COVID-19 on people living with HIV. But emerging evidence appears to be reassuring. People living with HIV who are on antiretroviral treatment do not appear to be at an increased risk.
Secondly, South Africa is not achieving the testing levels or reporting speeds required to contain the spread through diagnosis and contact-tracing. This gets harder as infection rates rise. Without this, it is unlikely that the country will stay ahead of the epidemic.
South Africa’s strategic thinking should therefore be informed by the following:
The need to minimise infection in vulnerable, high-risk groups and, where possible, to minimise deaths from COVID-19. This requires clear communication on the actual threat of the virus, preventative strategies, and slowing the spread of the virus to levels that spare the healthcare system and the economy while preventing the economic effects themselves from causing death.
It is not possible to contain the spread through lockdowns, because of the economic cost and the fact that it is not possible to keep the reproduction rate at consistently low levels easing lockdown.
It is therefore vital that the country develops strategies to control the virus and simultaneously manage the health, social and economic implications without resorting to further lockdowns.
Economic strategy
We suggest that South Africa move rapidly to stage 2 lockdown and that a risk-assessed framework be adapted. We propose that such a framework permit all economic activity, except where there is a clear and material threat to public health. The other exception are activities that pose a high risk of transmission over a short period of time, for example mass gatherings or transmission hotspots.
The framework should specify, by exception, economic activity not allowed on public health grounds. This would see the reopening of critical areas of the economy coupled with current behavioural and societal mechanisms to slow viral spread.
Within this framework, we also suggest that:
Health of workers should be a high priority. Precautions with respect to the protection of healthcare workers and protocols in healthcare settings require careful attention.
Regulations should specify employer responsibilities to ensure that the opening up of the economy does not result in flareups of infections.
Retail opening hours be extended to reduce density and exposure to the virus, with early pensioner-only hours.
The frequency of public transport services be increased to enable movement subject to the adoption of health protocols. These protocols can be enhanced as necessary.
The hours of work for accessing public services be extended to make it possible for the population to access services in ways consistent with health protocols.
For now, international travel for leisure should not be allowed.
The health risks associated with this economic strategy should be premised on effective strategies to mitigate the rapid rate of transmission of the virus. This is best achieved by:
Reinforcing physical distance measures in settings where people have no option but to gather, and paying attention to ventilation. In the case of busses and taxis, windows should be opened to prevent prolonged contact with potentially contaminated air.
Reinforcing evidence-based public health measures like hand washing. This should include providing sanitation to all communities.
The continued use of face masks for all outside of the home. Reusable masks must be made available to all communities free of charge.
This list is not exhaustive but sets parameters which can guide an adaptation to level 2.
The ability of the country to avert the possible full impact of the virus will only succeed if all citizens of South Africa cooperate willingly with measures aimed at slowing the rate of transmission. If that does not happen, the full might of this virus will manifest itself sooner rather than later, irrespective of the level of official lockdown.
Why more must be done to fight bogus COVID-19 cure claims
- Chimaraoke Izugbara and Mary O. Obiyan
Authorities around the world can do more to ensure that correct information and messages on the pandemic reach everybody.
Fake and bogus cure claims are a longstanding, but neglected public health problem. Throughout recorded history, plagues have inspired anxiety and desperation. Time and again, this public nervousness has proved a fertile ground for false cures and claimants to thrive. In this sense, recent claims of COVID-19 cures and antidotes are no exception.
During the Spanish flu, cure claims generated a false sense of safety that drove hundreds to defy closures and isolation. In the US, scores of bogus remedies alleging to cure the flu were sold under upbeat labels that undermined preventive action. One ad boasted:
When Vick’s VapoRub is applied over the throat and chest, the medicated vapors loosen the phlegm, open the air passages and stimulate the mucus membrane to throw off the germs.
Fake and bogus cures caused the death of many as HIV swept around the world. In Nigeria, for instance, as early as the 1990s, Jeremiah Abalaka, a surgeon with fringe training in immunology, startled the world with his HIV cure claim. Many of the HIV patients who flocked to his private clinic reportedly died, including dozens of soldiers referred for treatment by the Nigerian government.
More recently, during both the Ebola and SARS epidemics, fake cure claims also circulated freely, with lethal consequences. For example, salt solution, snake venom, vitamin C, Nano Silver and some herbs were all touted as cures for Ebola. At least two people died in Nigeria and about 20 more were hospitalised after drinking excessive amounts of salt solution to prevent Ebola infection.
Sadly, history is repeating itself in the context of COVID-19. False claims range from US president Donald Trump’s touting of anti-malaria drug hydroxychloroquine as a miracle cure to Madagascar’s herbal “cure” promoted by President Andry Rajoelina.
In Ghana, a Pentecostal pastor launched and sold “Coronavirus Oil”, telling a packed church that it was effective against COVID-19. An American pastor also recently directed viewers to buy Optivida Silver Solution to prevent COVID-19. Its promoter had falsely claimed that the product was government-approved and has the ability to kill every pathogen it has ever been tested on, including SARS and HIV.
With growing global anxiety, many people are easy targets for cure scams and hucksters. Victims of fake cure claims are often among the world’s poorest and most vulnerable. Fighting these cure claims is integral to containing the COVID-19 pandemic.
Authorities across the world are working hard to ensure that correct information and messages on the pandemic reach everybody. But there is room to do more.
Why we must act now
Cure claims are dangerous. They delay treatment-seeking and promote reckless behaviour that may result in deaths. At least 300 Iranians have died from methanol poisoning after consuming alcohol to prevent COVID-19. Hours after Trump declared hydroxychloroquine as a miracle cure for COVID-19, people overdosed on it in Africa and Asia. In Arizona, a man died after reportedly treating himself with a COVID-19 home therapy derived from the same anti-malarial drug that the US president touted as a wonder drug.
Health literacy – the ability of patients to read, comprehend and act on medical instructions – remains weak in many contexts. Several millions of health-seekers around the world rely on informal or inexpert sources for their health information needs. Hard-to-reach and vulnerable groups and communities must be targeted through bespoke health promotion strategies.
Online and traditional media offer immense potential to intensify public health education. They must maintain vigilance on COVID-19 cure scams and claimants as they emerge in diverse forms and places. However, merely identifying bogus COVID-19 cure claims or alerting the public about them is no longer enough.
Targeted seizure and destruction of unproven cures can deliver important results. In 2015, a global crackdown by Interpol seized nearly 21 million fake and illegal drugs, including fake cancer “cures”.
Governments must also implement community health outreach programmes that communicate clearly and accurately. Such programmes should have fit-for-purpose feedback systems to enable lay persons in multiple contexts to raise concerns, ask questions and swiftly receive answers. One size will not fit all at this time. Part of the success recorded in Nigeria during the Ebola outbreak has been attributed to the use of different media, including government-sponsored TV and radio messages, town-criers, social media campaigns, and experts to communicate health information to its citizens.
Countries and national health bodies must integrate traditional healers, faith leaders and community principals in their COVID-19 response strategies. Several studies have documented proven strategies for effectively engaging lay and faith healers to offer correct support and information on epidemics. This is the time to bring these strategies to scale.
Robust mechanisms for holding scam COVID-19 cure claimants and hucksters accountable are also urgently needed. Currently, few countries have such mechanisms. But a good precedent exists in Australia, where a “healing church” that touted a bleach-based solution as a COVID-19 cure has been fined more than $150,000. Politicians and other thought leaders must also realise that their utterances and actions during this pandemic will have far-reaching health, social and economic consequences.
Why arguments against quantitative easing hold no water
- Chris Malikane
The Reserve Bank should be allowed to buy more government bonds and securities to support the liquidity of the banking system.
Some analysts, including myself, have argued that the SA Reserve Bank should have long started the local version of quantitative easing (QE), which involves the central bank buying long-term securities on a large scale.
In addition, and contrary to the Bank’s initial position, I have argued that the law allows it to directly finance the fiscal deficit, and it could refinance government debt to open fiscal space for an effective response, not just to Covid-19 but also to the underlying structural economic crisis.
I estimate that the limit imposed by the SA Reserve Bank Act implies that the Bank’s balance sheet could absorb at least R239bn worth of direct bond purchases from the government. This excludes loans and other advances the Bank could extend to development finance institutions and municipalities.
The limits in the act do not provide sufficient flexibility and space for the Bank to play its developmental role given the scale of the structural historical problems, which have not been adequately addressed for far too long. The finance minister should by now have tabled amendments to the act to lift those limits, with new provisions that would permit the Bank to broaden the types of securities it may acquire in response to the crisis.
There are, however, those who oppose these proposals. The first view is that QE is strictly applied when economies face deflation, which is an absolute fall in prices, and when short-term interest rates are at 0%. The argument is that in deflation people delay buying goods and services in anticipation of prices dropping. This and other forces, such as debt deflation, reinforce a fall in demand and drive the economy into a severe contraction. Because the short-term interest rate is impotent at 0%, the use of QE aims to raise inflation, to make people anticipate a rise in prices in future and buy goods and services now.
The second view holds that outright financing of fiscal deficits and refinancing of public debt by the Bank would undermine the central bank’s “hard-won central independence”, which would weaken its ability to meet its monetary policy mandate. The argument is also that money creation to finance deficits would cause inflation to breach the Bank’s target, in much the same way as QE.
The argument that direct financing of the government undermines central bank independence is not necessarily correct. First, whether central independence is undermined depends on how the interface between the central bank balance sheet and that of the government is designed, particularly the need for transparency, accountability and the specification of limits in the use of such financing mechanisms.
Second, if the monetary policy mandate of the central bank — the inflation or long-term interest rate target — provides an explicit overarching device to co-ordinate fiscal and monetary policies, the ability of the central bank to achieve its monetary mandate will not be jeopardised. In fact, it may be enhanced. Third, in this arrangement the Bank remains independent to choose whatever instrument it deems fit to pursue its mandate.
In a number of cases central banks that directly finance their governments exhibit a higher degree of independence than the Reserve Bank. The Bank of Thailand directly subscribed to a variety of government debt instruments, yet it scores substantially higher than the Reserve Bank when it comes to independence. The same is true for the Bank of Korea, which lends directly to its government. The central banks of Uganda, Nigeria and Malawi all score better than the Bank on independence, and directly purchase bonds and make advances to their governments. This is also the case with the Central Bank of Cuba, which exhibits more independence than SA’s central bank.
The argument that direct money financing of the government necessarily undermines “the hard-won independence” of the Bank is therefore not correct. It all depends on the institutional design, transparency and accountability in the interface between the Treasury and the central bank. The proposals for the Bank to adopt unconventional measures do not tamper with the requirements for transparency and accountability.
The second view maintains that short-term interest rates, those that are charged for lending for less than one year, should be 0% before QE can be applied. I have argued elsewhere that this view is erroneous for an emerging market. To have a stable exchange rate the short-term interest rate in an emerging market should equal the interest rate of an advanced economy plus a sovereign risk premium.
When the advanced economy hits a 0% lower bound, the emerging-market interest rate will equal the sovereign risk premium, which is not 0%. Therefore, while the advanced economy embarks on QE at a 0% interest rate, the emerging market does so at some positive rate equal to the sovereign risk premium. It is wrong to expect SA to hit 0% interest before QE can be pursued. By extension it is also incorrect to say the currency will automatically depreciate if QE is implemented. It depends on the specific aims and design of the QE.
A related argument against the QE proposal is that it is strictly for economies on the verge of a deflation. This is also not correct. When an advanced economy hits its inflation target, say 2%, the emerging market hits its own target of say 4.5%. Now if the advanced economy hits 0% inflation, the emerging market reaches 2.5% inflation. Therefore an inflation rate that is on, or below, the target and an interest rate that is at the sovereign risk premium are sufficient conditions for an emerging market to embark on QE. This is where SA is now.
To expect the emerging-market inflation rate to be on the verge of 0% before embarking on QE is to allow the unemployment rate to soar to high levels because demand would have to fall significantly to pull inflation down to zero, before aggressive measures to counter the downturn are implemented. Such a haemorrhage of the real economy would be made worse if inflation expectations are anchored, as they should be, at the target.
The Bank should not be shy to acquire more government bonds and other securities to support the liquidity of the banking system, even if the short-term interest rate is above 0%. The R11bn purchases of government bonds is a step in the correct direction, but it is sadly inadequate.
Because the banking system is increasingly facing defaults and high risk aversion, the Bank should be legally empowered to broaden the types of securities it could purchase from the entire financial system, to effectively secure financial stability and drive progressive structural change. The Bank should also explore more channels of credit transmission to the real sector, beyond the conventional banking channel, such as direct lending to development financial institutions, securitised commercial loans, acquisition of government-guaranteed securities and direct lending to government. All this should be done in a transparent and accountable manner, in much the same way as the budget process.
In short, a new financial architecture needs to be established that is informed by a vision and mission to address the historical and structural fault lines of SA society, beyond the pandemic.
Chris Malikane is Associate Professor in the School of Economics and Finance at Wits University. This article was first published in Business Day.
A new, fairer economy is possible, but that would mean sacrifice
- Imraan Valodia
That Covid-19, the lockdown and whatever will come after will have had a lasting and devastating impact on our economy seems indisputable.
Since it was first reported in Wuhan, China in December 2019, the SARS-CoV-2 virus and the resultant disease, Covid-19, has evolved from being a distant perceived threat to having the most devastating impact on the world economy of any single event since the Great Depression.
This has occurred in a matter of less than 6 months. Having declared a state of national disaster on 15 March 2020, President Ramaphosa announced on 23 March that South Africa would commence a three-week national lockdown starting at midnight on 26 March 2020.
The lockdown was then extended for a period of 2 weeks, and continues for the foreseeable future, albeit now in terms of the South African government’s risk-assessed phased approach.
The economic, health, social and political consequences of the pandemic have wreaked havoc on our lives and left us all permanently scarred.
The pandemic has exposed the deeply unequal world that we live in, and uncovered how vulnerable the economic situations of millions of our citizens really are.
It is ironic that it is not the working of the economy, but rather the shutting down of the economy, that has most starkly exposed our unequal world.
Those at the top own the most of everything
Two pieces of research on income and wealth, conducted by my colleagues Gabriel Espi and Aroop Chatterjee in the Southern Centre for Inequality Studies, highlight the extent of South Africa’s inequality.
If we divide South African households into five groups (quintiles), we can create a picture of income inequality and how different income groups have been able to live through the challenges of a lockdown.
On average, South African households in the poorest income quintile have a total monthly income of just R2600, which has to support, on average, 5 members of the breadwinner’s household.
About 18 million South Africans live in these households.
In contrast, the highest income quintile has an average income of R38 000, which has to support two household members. Some 7 million South Africans live in these households.
The data on the distribution of wealth is even worse.
The poorest 50% of South Africans have an average net wealth of negative R16 000.
That means their assets are less than their liabilities: they are deeply in debt.
By contrast, the richest 10% of South Africans have an average net wealth of R2.8 million per person. The top 1% of holders of wealth in South Africa have an average net wealth of R17.8 million per person.
The ability of these households to withstand the economic effects of a sustained lockdown is very different indeed.
For low-income households, closing off the taps that allow them to earn their meagre income has meant being plunged immediately into hunger and even deeper poverty.
With this income and wealth picture in mind, it is not at all surprising to see the shocking food queues that we have seen over the last five weeks.
Low-skilled and informal occupations are by far the hardest hit
Let us consider the world of work, in which the inequalities go much deeper. Andrew Kerr and Amy Thornton from the University of Cape Town have done some very interestingresearch that aims to examine who, notwithstanding the lockdown, is able to work and who is not.
They estimate that just over two million South Africans, who make up 13.8% of those who had employment pre-lockdown, are able to continue working from home for the same income they were earning before the lockdown.
It is hardly surprising these are mainly professionals and those with high levels of skill. For most low-skill occupations, outside of those who are essential workers, the lockdown has meant a dramatic fall in income.
That has affected 10.5 million workers - approximately 63% of the workforce.
Some of these workers are facing the prospect of long-term unemployment as large businesses consider shutting down permanently.
The effect of the lockdown has been particularly severe on one group of workers: the approximately 5 million workers who earn their livelihoods in the informal economy.
For this group, who rely on a functioning economy to earn a small amount of income from selling vegetables at a bus rank, preparing food for sale at the train station, or collecting waste for recycling, the lockdown has meant immediate poverty and hunger.
As my colleague at Wits University, Melanie Samson has shown,waste pickers, while clearly part of essential services, remain unseen by policymakers because they form part of the informal economy.
Formal sector waste services are deemed to be essential services and allowed to operate, but those who perform exactly the same services in the informal economy are not.
The double standard could not be more stark.
Until government relaxed the lockdown rules and allowed some informal trade to happen and announced a special Covid-19 grant for the unemployed and those working in the informal economy, the lockdown was placing informal workers in an impossible moral dilemma: abide by the lockdown regulations and starve, or break the rules and expose yourself and others to the risk of infection.
My colleagues at the African Centre for Migration and Society at Wits University havehighlightedthe fact that the percentage of foreign born migrant workers in the informal economy is twice as high as that of South Africans.
For most of these migrants, the lockdown means neither an income from informal work, nor a Covid-19 grant.
Gender Inequality
The gender inequalities in our society have also been starkly exposed. Besides the gender inequalities in employment, the lockdown has revealed the deeply unequal gender relations within households.
Ours is unfortunately a society with significant levels of gender-based violence. For many of our women and children, the lockdown has meant a dramatic increase in gender-based violence.
The Foundation for Human Rights reports that, during the first week of the lockdown, SAPS received more than 2333 complaints of gender-based violence - a 37% increase on the weekly average for 2019.
One of the most significant but unseen gender inequalities in our economy is the unequal value that society places on care work. Care work is undervalued mainly because the work is done largely by women.
This inequality is seen starkly in a comment by Matt Hancock, the UK Health Secretary (the equivalent of our Minister of Health). Responding to a question on the numbers of health workers that have died in the UK as a result of Covid-19, Hancock replied: “We’re seen very sadly four doctors die so far, and some nurses”.
Quite disgusting! While our Health Minister is doing a better job than Matt Hancock, our gender data on the unequal burden of care is not dissimilar to that in the UK.
According to our time use survey in 2010, women in South Africa spend 5.8 times more time doing unpaid care work than men do. It would be interesting to see how much more unequal this burden is during a lockdown.
Effects on the economy
That Covid-19, the lockdown and whatever will come after will have had a lasting and devastating impact on our economy seems indisputable.
Might it also provide the impetus for a new economy – one that is more equitable, more resilient and more sustainable?
President Ramaphosa has raised the idea of a new social compact to get us onto such a path.
As a hopeless optimistic, I do think that it is possible to gain consensus on such a social compact, and rebuild our economy as on that is more equal.
However, a key ingredient for a social compact is getting those who have a lot to give up some of their short term interests, in the long term interest of the entire society.
How does one convince people to give something up in an economy that is likely to contract by as much as 10 percent?
Professor Imraan Valodia is Dean of the Faculty of Commerce, Law and Management and Head of the Southern Centre for Inequality Studies at the University of the Witwatersrand. This article was first published on News24.
Wits' Covid-19 Standard Operating Procedures
- Wits University
The country remains in a level four lockdown, which means that only employees who render essential services are allowed to be on our campuses.
This may change in the coming weeks if restrictions are relaxed.
As and when employees are allowed to return to work, it will become imperative for all executives, managers, deans and heads of school to ensure that all employees, service providers, contractors and visitors comply with the Standard Operating Procedures. These documents elaborate on the processes to be followed regarding access to the University’s campuses, as well as the screening and testing procedures that need to be followed. These documents must be read in conjunction with the Human Resources Plan circulated two weeks ago.
The Screening Form will have to completed every day, before anyone can access the University’s campuses. The Form will be made available on the Wits website, and where possible should be downloaded and completed before employees, service providers, contractors or visitors arrive on campus. Where this is not possible, people will have to fill out a screening form at the University’s gates. A mobile application is being developed to eventually replace the hard copy forms.
All employees must abide by all the regulations stipulated in the documents above whilst on the University’s premises, with effect from today, 18 May 2020.
Should you have any questions pertaining to access, please direct them to Gary.Kruser@wits.ac.za. All issues pertaining to Occupational Health and Safety, should be directed to Jonathan.Devilliers@wits.ac.za.
Thank you
Zeblon Vilakazi
Vice-Principal and DVC: Research and Postgraduate Affairs
18 May 2020
GeneXpert testing platform for TB repurposed to accelerate testing for Covid-19
- Wits University
Efforts to test for Covid-19 in SA have been boosted through repurposing the Cepheid GeneXpert® Systems, originally designed to test for tuberculosis (TB).
The first batch of GeneXpert machines began testing for Covid-19 ahead of Freedom Day on 26 April 2020.
The combined efforts of joint staff in the Division of Haematology and Molecular Medicine at Wits University and the National Health Laboratory Service (NHLS), along with the National Department of Health (NDoH) has enabled the National Priority Programme (NPP) division to now also support Covid-19 testing in record time.
The NPP division enables the NDoH to provide increased access to patient testing and treatment – now also for Covid-19. Professor Wendy Stevens, Head of Haematology and Molecular Medicine in the School of Pathology at Wits leads the NPP division, which aims to provide affordable, accessible HIV and TB diagnostic services that yield accurate, reliable, relevant and timely results.
These services and results align with NDoH strategy and are based on current scientific knowledge and international norms. Through efficiently leveraging existing resources, including the GeneXpert platform, the NPP division can now also respond to the global Covid-19 pandemic.
There is no doubt that the GeneXpert System will make a massive difference in testing capacity, provided that there is constant access to reagents and the appropriate human resources support. The GeneXpert System is simple to run, with the bigger machines accepting up to 80 cartridges at a time.
It is forecasted that if all the Covid-19 testing sites are operational on a 24-hour basis, up to 15 000 additional tests can be conducted daily from these machines alone. The data collected from the testing sites will provide valuable insight into the spread of the virus and hopefully contribute to a greater understanding of it in the South African context.
Xpert diagnostics for Covid-19
The GeneXpert platform has been used extensively in South Africa to test for TB for almost a decade. The initial rollout took 18 months to complete. Now, with the Covid-19 pandemic, the NHLS has utilized its existing TB footprint and condensed the escalation of testing into just one month.
The NHLS has been responsible for the implementation and programmatic monitoring of TB through GeneXpert since 2011. Developed by American-based company Cepheid, these systems are distributed to 166 laboratories in South Africa, with more than 325 machines ranging in size and capacity, the smallest no bigger than a desktop computer. More than 17 million TB tests have been conducted to date – 1.7 million positive cases and more than 100 000 drug-resistant cases have been detected.
Thanks to the GeneXpert’s ability to test an array of assays (including HIV), GeneXpert instruments are now being used to test for the presence of Covid-19. Cepheid released their Xpert® Xpress SARS-CoV-2 cartridge on 21 March 2020, following emergency Federal Drug Administration approval, to support the scale-up of testing. Training material has been distributed to all users.
To detect Covid-19, the machines are loaded with the test cartridges containing a combination of a patient’s specimen (e.g., pharyngeal swab) and chemical reagents, thereby enabling detection of certain genetic material. Once a cartridge is loaded, it produces a result within 45 minutes.
Xpert project management
With experience gained in managing the GeneXpert Programme for TB testing since its inception, Ms Puleng Marokane, the GeneXpert Project Manager within the NPP division of the NHLS, has been tasked with ensuring the smooth rollout of Covid-19 testing nationwide.
Marokane explained that successful implementation of the system was only possible if all the parameters were in place. The system would have to be loaded with Covid-19-specific software, and cartridges validated to ensure they could produce the requisite results. Although laboratory technicians have used GeneXpert Systems before, it was important that they adapted to the new Covid-19 interface.
Online training in this regard focused mainly on the new cartridge, processing and result interpretation, whilst emphasising Good Clinical Laboratory Practice. This was guided by a standard operating procedure (SOP) developed by the NPP and used across all test sites.
“This was not an easy job [in lockdown]. We had to rely on everybody’s experience with GeneXpert to ensure they could load the software themselves. Our task then was to try to cover all nine provinces. We were hoping to implement testing in a phased manner, but because this is an emergency, it is not always possible,” said Marokane.
Once technicians had familiarized themselves with the system, they were able to begin the cartridge verification process. A limited number of reagents were ordered centrally and were sent through to specific sites. Verification panels were developed by SmartSpot®, a manufacturing company co-founded by Professor Stevens and Professor Lesley Scott in the School of Pathology at Wits, to aid with diagnostic testing.
Covid-19 sample verification was kept to a minimum due to a shortage of reagents – all that was required was to confirm the system could produce a positive or negative result. To date, eight of the testing sites have passed the verification process and have gone live for testing.
Testing and training in challenging times
Marokane and her team have worked tirelessly to ensure operational stability of the system. However, a project of this scope is not without challenges. South Africa’s national lockdown impedes the shipment of reagents, the vital component required to meet the kind of daily testing numbers the health ministry is hoping to achieve. At the time of writing, an additional 10 000 reagents were received from Cepheid. But with South African borders being closed indefinitely, access remains an issue.
Some staff members have expressed concern about their personal safety during the testing process. The NPP, through the NHLS, is working closely with safety departments: virtual training is being rolled out for NHLS staff; SOP material has been made available to advise laboratories on processing the test method, as well as sample disposal; and the appropriate Personal Protective Equipment (PPE) has been provided in line with government regulations.
“All that is left to do at this stage is to monitor the implementation processes. We want to ensure users are comfortable using the tests,” added Marokane.
Covid-19 Update (29) - Students to receive an additional 15GB of data for next 15 days
- Wits University
The four telecommunications companies agree to extend the provision of data to students for another 15 days.
Wits University has negotiated with the four telecommunications companies to extend the provision of data to students for another 15 days. This means that students whose numbers are registered on the self-service portal will automatically receive an additional 15GB of data (5GB daytime and 10GB night express) from 21 May 2020 until 5 June 2020 in order to continue with the academic programme online.
The University is in the process of establishing a long-term solution for staff and students from 6 June 2020 onwards.
Economic policy remains hotly contested in South Africa: this detailed history shows why
- Edward Webster
Book sheds new light on the evolution of the economic policy of the African National Congress, South Africa's governing party.
Economic inequality in post-apartheid South Africa has deepened. This is not what was expected. Firstly, the African National Congress (ANC) won an overwhelming victory in the 1994 elections and promised to significantly reduce inequality in the world’s most unequal country. Secondly, the country’s constitution, adopted in May 1996, foregrounds the promotion of social and economic rights.
This paradoxical outcome has led to a ferocious political-economic debate on the nature of South Africa’s transition to democracy.
On the other hand, there are those who argue that the ANC had no alternative to the Washington consensus approach to the economy in the 1990s. They say it was always a party of a mixed economy, the right to trade freely and the growth of a black business class.
Among the exponents of this view are Thabo Mbeki, the key figure in shaping ANC economic policy as deputy president from 1994 to 1999, and Trevor Manuel, finance minister at the time.
Simply put, the Mbeki camp maintains that a fundamental continuity exists in the economic and social policies developed after 1994. Critics say there has been a policy reversal in post-apartheid South Africa.
A new book, Shadow of Liberation, by Vishnu Padayachee and Robert Van Niekerk, respectively Distinguished Professor of Development Economics and Professor of Public Governance at the University of the Witwatersrand, challenges both approaches. It revisits how economic and social policies were made from the late 1980s to the mid-1990s. The authors draw on 35 in-depth interviews with participants in the policy process. This pool of original data is complemented by a rich archive of primary and secondary sources. Together, these data sets reveal a fascinating story about who shaped these policies and how.
The book is the first attempt to comprehensively document and interpret the origins and evolution of the ANC’s economic and social polices.
Evolution of ANC economic policy
The authors argue that the ANC lacked economic expertise – and spurned what little it had. In particular, it rejected the evidence-based analysis and recommendations of the MacroEconomic Research Group, which it had commissioned. They argue that it was less a case of the ANC “selling out” and more one of being outmanoeuvred. Policy makers were, Padayachee and Van Niekerk conclude (p. 135),
Intellectually seduced in comfortable surroundings and eventually outmanoeuvred by the well-resourced apartheid state and by international and local pro-market friendly actors.
The story of the evolution of the ANC’s economic policy is a complex one. The authors take us on a long journey that begins in the 1940s. The rest of the journey is spread over nine chapters. Chapter 2 shows how the party’s economic and social roots lie in social democratic policies. These ideals can be found in the bill of rights in African Claims, developed in 1943.
African Claims was a document with a recognisably social democratic impetus. It argued for state intervention to secure social rights to health, education and welfare for all. This was to be based on universal political and social citizenship. These aspirations can also be traced to what the authors call the “Keynesian, social democratic welfare state, based on the social rights of citizenship” in the Freedom Charter adopted in 1955 (p. 22).
The next chapter connects the past to the dawn of democracy and the formation of the ANC’s economic planning department. The authors argue this consisted of a small group – Trevor Manuel, Alec Erwin, Maria Ramos, Neil Morrison, Moss Ngoasheng, Leslie Maasdorp – who came to believe that there
was no alternative to neo-liberal globalisation (p. 67).
The pace quickens in chapters 4, 5 and 6 – the empirical heart of the book. The authors show how the ANC distanced itself from the post-Keynesian MacroEconomic Research Group in December 1993, and then abruptly dropped the popular “growth through redistribution” Reconstruction and Development Programme in April 1996.
At the centre of the book is a powerful critique, not only of the policy outcomes, but also of the way in which the policies were made. Yet the critiques sometimes feel incomplete.
There is a substantial body of literature on the “politics of economic reform” that could have been drawn on to deepen Padayachee and Van Niekerk’s argument that widespread consultation and negotiation is vital for successful economic reform. In fairness, the refusal to negotiate the Growth, Employment and Redistribution macroeconomic strategy for South Africa in the National Economic Development and Labour Council is rightly criticised and the authors show admirable awareness of the issue.
The late post-Keynesian American economist Hyman Minsky’s famous observation, made over 30 years ago and rightly quoted by the authors, makes the point:
Economic issues must become a serious public matter and the subject of debate if new directions are to be undertaken. Meaningful reforms cannot be put over by an advisory and administrative elite that is itself the architect of the existing situation (quoted on p. xi of the book under review).
Tragically, it is precisely what unfolded in South Africa in the 1990s.
Speaking to the present
Although the book examines events nearly three decades ago, it speaks to the present where the demand for rapid economic reform has become widespread.
The lesson I draw from the book is that economic reform cannot be undertaken by a small group of people. Instead, policies must be formulated and implemented through negotiation and consultation of a social compact beyond the state and parliament to include unions, employers and other interest groups.
Labour retains the power to block the imposition of economic reform – both at the national and workplace level. Any attempt to impose neo-liberal solutions unilaterally is likely to take the country down the path of ungovernability and civil war – it will ensure rather than avert chaos. If, at the same time, socialist solutions seem unfeasible, this conclusion points towards a class compromise between capital and the labouring poor: a Southern version of social democracy.
The insights in Shadow of Liberation complement this claim, while developing new interpretations based on evidence from face-to-face interviews with the key actors as well as new archival material. It is a necessary read for a new generation of policymakers as they confront the challenge of economic reform. Above all, this book is a major contribution to the growing body of literature on the appropriate policies required to reduce inequality in the global South.
Statement of Support for Professor Glenda Gray and the Principle of Academic Freedom of Speech.
Professor Glenda Gray, Full Professor in the Faculty of Health Sciences,has pioneered advances in preventing mother-to-child transmission of HIV, which has saved thousands of lives. She is an alumna of Wits Medical School and established the Wits Perinatal HIV Research Unitat Chris Hani Baragwanath Hospitalin 1996. She has been awareded South Africa's highest honor, theOrder of Mapungubwe(Silver); and in 2017 TIME Magazine named Professor Gray among the top 100 most influential people in the world.
She is an NRF A-rated scientist, CEO and President of the South African Medical Research Council (SAMRC) and involved in HIV vaccine research.
Statement of Support for Professor Glenda Gray and the Principle of Academic Freedom of Speech:
“As scientists, academics and policy experts, we are committed to being part of the complex policy response and debate on dealing with the epidemic of SARS-CoV-2 (the cause of COVID-19) in South Africa. We recognize that it is impossible to have perfected the response to the epidemic, but course correction should be rapid and not defensive. With that in mind, we condemn the specific threat made against Professor Glenda Gray for expressing her opinion in public, which is totally out of step with the public pronouncements made by the President, welcoming criticism. We uphold the right to academic freedom of speech, and call on the South African government to engage openly with alternate views, and for all of us to urgently work towards constructive solutions regarding policy, in the interests of the country"
Current signatures (alphabetic order): (note, this list was assembled on Saturday evening, and finalised at 6.45 pm; additional names may be added)
The Wits Senate Academic Freedom Committee (SAFC):
Associate Professor S Laryea (Chairperson)
Professor M Byrne (Senate representative)
Professor J Dugard (Senate Representative)
Dr B Johnson (Acting Director: Transformation Office)
Professor E Sideras-Haddad (Senate Representative)
Mr A MyIchreest (Legal Office Representative)
Professor R Osman (DVC: Academic and Vice-Principal)
Dr T Augustine (Academic Staff Member)
Adjunct Professor F Cachalia (Academic Staff Member)
Professor Cathi Albertyn, School of Law, University of the Witwatersrand
Professor Lucy Allais, Professor of Philosophy, University of the Witwatersrand, Henry Alison chair of the History of Philosophy, UCS
Professor Linda-Gail Bekker, Director, Desmond Tutu HIV Foundation, University of Cape Town
Dr Duanne Blaauw, School of Public Health, University of the Witwatersrand
Professor Keith Breckenridge, WISER, University of the Witwatersrand
Professor Catherine Burns, Associate Professor of Medical History; Adler Museum of Medicine; Faculty of Health Sciences, University of the Witwatersrand
Professor Nithaya Chetty, Dean, Faculty of Science, University of the Witwatersrand
Professor Usuf Chikte, Emeritus Professor, Department of Global Health, Stellenbosch University
Professor Jason Cohen, Deputy Dean, Faculty of Commerce, Law and Management, University of the Witwatersrand
Dr Francesca Conradie, Clinical HIV Research Unit, University of Witwatersrand
Dr Aslam Dasoo, Progressive Health Forum
Prof Joel Dave, Head of Division of Endocrinology, University of Cape Town
Professor Ames Dhai, Professor of Bioethics, University of Witwatersrand
Professor David Everatt, Wits School of Government, University of the Witwatersrand
Dr Dean Gopalan, President Critical Care Society of South Africa
Professor Adam Habib, Vice Chancellor, University of the Witwatersrand
Professor Shireen Hassim, WISER, University of the Witwatersrand
Professor Ian Jandrell, Dean, Faculty of Engineering the the Built Environment, University of the Witwatersrand
Professor Bavesh Kana, Personal Professor, Wits University
Professor Kathy Kahn, School of Public Health, University of the Witwatersrand
Professor Uma Kollamparambil, Head, School of Economics and Finance, University of the Witwatersrand
Professor Naomi Levitt, Emeritus Professor of Endocrinolgy, University of Cape Town
Professor Gary Maartens, Head of Clinical Pharmacology, University of Cape Town
Professor Shabir Madhi, Professor of Vaccinology and Director of the MRC Respiratory and Meningeal Pathogens Research Unit, University of the Witwatersrand
Dr Gloria Maimela, Director: Health Programmes, Wits Reproductive Health and HIV Institute, University of the Witwatersrand
Dr Moeketsi Mathe, private practice, lecturer, University of Witwatersrand
Professor Marc Mendelson, Head of Division of Infectious Diseases & HIV Medicine, University of Cape Town
Prof James McIntyre, School of Public Health & Family Medicine, University of Cape Town
Professor Shaheen Mehtar, Emeritus Professor, Stellenbosch University
Professor Mike Morris, Economics, University of Cape Town
Dr Jeremy Nel, Department of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand
Professor Ntobeko Ntusi, Head of Medicine, University of Cape Town
Dr Regina Osih, Senior Technical Expert, Aurum Institute
Prof Peter Raubenheimer Department of Medicine, University of Cape Town
Dr Haroun Rhemtula, Head of Clinical Unit and Head of Obstetrics, Department of Obstetrics and Gynaecology, CMJAH and University of the Witwatersrand
Professor Guy Richards, Emeritus Professor, University of the Witwatersrand
Mr Fana Sibanyoni, Chief Operations Officer, University of the Witwatersrand
Professor Mark Sonderup, Division of Hepatology, University of Cape Town
Professor Jantjie Taljaard, Head of Divison of Infectious Diseases, University of Stellenbosch
Professor Steven Tollman, School of Public Health, University of the Witwatersrand
Prof Imraan Valodia, Dean, Faculty of Commerce, Law and Management, University of the Witwatersrand
Professor Alex Van Den Heever, Chair in the field of Social Security at the Wits School of Governance
Professor Martin Veller, Dean, Faculty of Health Sciences, University of Witwatersrand
Professor Francois Venter, Ezintsha, sub-division of Wits Reproductive Health and HIV Institute, University of the Witwatersrand
Prof Zeblon Vilakazi, DVC Research, University of the Witwatersrand
Professor Jimmy Volmink, Dean Faculty of Health Sciences, Stellenbosch university
Professor Sean Wasserman, Infectious Diseases. Groote Schuur Hospital, University of Cape Town
Prof Nicola Wearne, Division of Nephrology, University of Cape Town
Professor Edward Webster, Southern Centre for Inequality Studies, University of the Witwatersrand
Professor Robin Wood, Director, Desmond Tutu HIV Centre, University of Cape Town
Dr Adrienne Wulfsohn, Emergency and Disaster Medicine, KZN
Covid-19 Update (30) - Wits Prepares for the return of some students
- Wits University
Final year students and other identified groups of students expected to return to campus from 8 June 2020.
Dear Colleagues and Students
We have spent almost two months in lockdown and we understand that the restrictions may be taking a toll on some students and staff members. If you do need help, please make use of the University’s health and wellness services available to staff and students.
On another note, President Cyril Ramaphosa announced last night that the entire country would be moving to level 3 restrictions. He said that all higher education institutions should have remote teaching and learning plans in place to ensure that all students had an equitable chance of completing the 2020 academic year. He added that all students who could study or work from home should do so. Finally, he confirmed that final year students and other groups of students would be allowed to return to public universities from June 2020, provided that all the requisite preparations were in place and that no more than one third of the total University community returned.
The University has developed a schedule for the planned return of students and staff at level three and subsequent levels. Senior executives and managers will refine the plan and will advise on Friday, which student groups should return to campus from 8 June 2020.
The next two weeks will be used to ensure that our campuses are prepared for the return of students and staff, and that all the requisite screening, cleaning, sanitising and personal protection equipment is in place before members of the community return to campus. Further details will follow later this week.
In the interim, keep learning and working from home.
Take care and keep well.
SENIOR EXECUTIVE TEAM
25 MAY 2020
Dubious remedies will not decolonise Africa
- William Gumede
So-called African solutions that are often uncritically accepted as ‘good’ do nothing for the continent
Many African governments, leaders and intellectuals’ misguided seeking refuge in quick fixes and conspiracy theories to deal with intractable problems have undermined development, good health and peace since end of official colonialism at the end of the Second World War.
It now undermines the fight against Covid-19 in Africa. The Covid-19 pandemic has now reached more than 100 000 confirmed cases in Africa, with more than 3100 confirmed deaths. While reporting statistics in Africa is often unreliable, it nevertheless appears that in Africa Covid-19 appears to be rising slower than elsewhere, taking 52 days to reach 10 000 confirmed Covid-19 cases, it took 11 days to increase from 30 000 to 50 000 cases, according to the World Health Organisation.
Some African leaders and intellectuals say Covid-19 is a Western or Chinese conspiracy, aimed to entrench their pharmaceutical or imperial interests in Africa.
Often diseases, development problems and violence are blamed mostly on outsiders – which leads to no or little decisive action to tackle diseases, development problems and violence; or the wrong solutions are embarked on. This is not to say that colonialism did not bring diseases, development problems and violence to Africa; or that former colonial powers do not meddle in the domestic affairs of African countries to the harm of the continent’s peoples.
Under the rubric of fighting decolonization, every African problem or solution to a problem is wrongly often positioned as either Western-originated, and therefore to be rejected; or African-originated and therefore to be embraced. Scientific and evidence-based solutions are then rejected as supposedly Western colonialism. Yet, science and evidence-based solutions are universal, meaning they are not restricted to Western countries alone, neither are they unAfrican.
At the same time dubious solutions are often embraced solely because they originated from within Africa. Many so-called misguided African solutions are therefore uncritically accepted as part of decolonization. Other ancient societies which suffered from colonialism or imperialism, just like Africa, such as China, Japan or Singapore, do not take the Africa approach to decolonization. Such countries take the best of their own and Western cultures and forge new solutions out of these; or they adapt appropriate solutions from outside for their own circumstances.
Madagascar’s President Andry Rajoelina has claimed to have discovered a cure for Covid-19. He has pushing what he calls Covid-Organics, an herbal drink, put together by the Malagasy Institute of Applied Research, which he says can cure Covid-19. The Madagascan government has given the drink to school children.
Rajoelina has provided no information about any clinical trials, tests or results of the efficacy of the drug beyond saying “all trials and tests have been conducted and its effectiveness in reducing and elimination of symptoms has been proven in the treatment of Covid-19 patients in Madagascar”. The Malagasy Institute of Applied Research look at the treatment of disease by African traditional practices, plants and animals.
Equatorial Guinea, Liberia and Tanzania have enthusiastically accepted batches of the herbal drink. Many African countries, leaders and intellectuals appear to have embraced the Madagascar drug as an indigenous “African solution”, as part of “decolonization”. Many have dismissed questions over the science of the drug as supposedly Western government, pharmaceutical and business interests against African “solutions”.
Rajoelina in an interview stated: “If it was a European country that had actually discovered this remedy, would there be so much doubt? I don't think so”. Stéphane Ralandison, Dean of the Toamasina School of Medicine in Madagascar has warned that the underlying research methods behind the Covid-Organics were “not fully scientific”. The World Health Organisation has said that: “Africans deserve to use medicines tested to the same standards as people in the rest of the world.”
Across Africa, in countries such as Uganda, the Democratic Republic of Congo (DRC) and Cameroon, other so-called traditional African potions are being touted as a cure-all for Covid-19. In the Democratic Republic of Congo one traditional leader has secured a following with his alleged cure of inhaling steam from a concoction of mango bark, ginger, papaya leaves and unknown plant. There have been deaths reported in the DRC as a direct result of people using such African potions as cures for Covid-19.
Uganda arrested Lazarus Kungu, an herbalist who claimed to have invented his own traditional plant-based remedy for Covid-19 for endangering public health. Tanzanian President John Magufuli has called for prayer in churches and mosques as a solution to tackle Covid-19.
The African Union has been predictably be quiet – its usual default position on contentious issues where it should actually take decisive leadership - on Madagascar’s and other untested African Covid-19 remedies and conspiracies.
During the explosion of the HIV/Aids virus, many African leaders, governments and intellectuals also blamed Western conspiracies for its spread on the continent. This delayed tackling the disease causing needless loss in lives. Then South African President Thabo Mbeki questioned the science used to treat the disease. The late South African Health Minister Manto Tshabalala Msimang preached the African potato, garlic and beetroot as remedies for HIV/Aids.
To deal with Covid-19, African countries must follow, what their peers in Asia, such as China, South Korea, Singapore and Taiwan has done, by making evidence-based policies guide their strategies to tackle the virus. These countries have done so without conspiracy theories, blaming outsiders or sought untested dubious “local” solutions – and they have been very successful as a result. Former colonial powers now look at lessons from these countries in how they have tackled Covid-19. Now, there is successful decolonisation in practice.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand; and author of South Africa in BRICS (Tafelberg)
Long-term Data Access for 2020 - Wits partners with Vodacom
- Wits University
New initiative provides students with data to access selected URLs through the Wits network.
Staff and students who provided valid Vodacom numbers to the University are receiving 10Gb daytime and 20Gb night-owl data-bundles per month for use on selected URLs accessed through the Wits network. This will continue on a rolling month-to-month basis. To use the data, staff and students must have provided the University with a valid Vodacom mobile number and installed the CISCO AnyConnect Mobile Client VPN app on their device.
Any queries or requests for assistance for existing staff and students should be directed toDataHelp@wits.ac.za.
Covid-19 Update (31) - The phased return of students and staff to campuses
- Wits University
Information regarding the staggered approach adopted for a phased return to ensure wellbeing and safety of students and staff.
The phased, coordinated and safe return of students and staff to the University from 8 June 2020 was deliberated on this week, following the announcement that South Africa would move to level 3 of the COVID-19 lockdown from June, which will allow for some groups of students and staff to return to campuses across the country.
The wellbeing and safety of our students and staff is paramount and it will take our collective effort, courage and determination to keep the coronavirus at bay. After consultation with the Deans, academics and student leaders, it was agreed that a staggered approach will be adopted with the first cohort of students returning from the 8th of June 2020, followed by a second cohort in mid-July.
The following student groups will return from the 8th of June 2020. The exact dates and schedules for each cohort will be communicated by faculties:
Faculty of Commerce, Law and Management
Certain courses in the Faculty’s executive education programme in the Wits Business School and Wits School of Governance will be offered on campus.
The Faculty will reintegrate a percentage of the student body in Phase 2 from July onwards, as and when appropriate. Further details will be communicated in due course.
Faculty of Engineering and the Built Environment
PhD and MSc students who require access to laboratories will return.
Selected graduating classes and progressing students (including third year students who need access to laboratories) will return.
Faculty of Health Sciences
Clinical students and students in their final year of study (MBBCh, GEMP and students on the Mandela-Castro programme) are already on campus.
Pre-final year students with a high clinical load will return.
Undergraduate students with clinical training needs and postgraduate students with laboratory-based research will return.
Faculty of Humanities
The Faculty will reintegrate a percentage of the student body as and when appropriate in Phase 2 from July onwards.
Faculty of Science
PhD and Research Masters Students will return.
Honours students who require access to laboratories will return.
A very careful selection of 3rd year students will return.
Residence students who do not live in an environment conducive to learning and who find it extremely difficult to study online
Students in this category will be brought back to residences incrementally, to enable them to continue with their studies online from their respective residences. As per regulations, not more than one third of Wits’ residences may be occupied at any given time. This means that the number of students who are able to return to residences are limited. The Dean of Students will communicate the process to be followed for the phased return of students in this category early next week.
Details of student groups that will return from July onwards will be communicated in the coming weeks. Please do not return to campus unless you have been given permission to return.
Level 3 lockdown: Implications for staff members
The phased reopening of our campuses will necessitate the return of some academic, professional and support staff to our campuses. A comprehensive workplace plan has been developed by the Senior Director: Human Resources, which includes guidelines for the preparation of the workplace before employees arrive, the responsibilities of managers, health and safety officers and employees before returning to work, whilst in the workplace, and processes to follow if issues arise.
The SET has also agreed to the following principles:
All academic, professional, administrative and support staff who can work from home, should continue to do so, and should only come onto campus if necessary;
Staff members who are required to be at work should report for duty (line managers will make this request to staff members);
Staff members over the age of 60 or those living with co-morbidities (see below) should stay at home;
All staff who are unable to work during this period, should, where possible, be redeployed to areas where they could make a contribution.
Staff members who have co-morbidities (like cancer, diabetes, asthma or other respiratory illnesses) should voluntarily declare these illnesses to their line manager or provide a valid doctor’s letter that indicates specifically why they cannot report for work. Where line managers believe that it is necessary, a second opinion may be obtained from selected healthcare practitioners based at the Wits Donald Gordon Medical Centre.
Line managers should work with health and safety officers, Services and HR to ensure that the following measures are in place:
Physical distancing of staff and students;
The adequate provision of sanitisers and/or soap and water;
The regular cleaning of venues and work spaces;
The provision of cloth masks (two per student and staff member) and other personal protective equipment for specialised areas; and
Protocols to prevent the spread of infection.
It is the responsibility of every staff member to ensure that the self-screening form (paper or online or via the app) is completed in full every morning. The paper-based screening form is being converted into a mobile application to reduce congestion at entry points. Details about the app will follow early next week.
Conclusion
Students and colleagues, we are living through a difficult period, but it is time for us to put our shoulder to the wheel and to move forward, in the interests of the broader Wits community. This is a true test of our Ubuntu - our personal actions, behaviours and choices impacts on those around us, and it is up to each and every one of us to act responsibly for the sake of our collective humanity.
Keep well and safe.
SENIOR EXECUTIVE TEAM
29 MAY 2020
The world is flat: Covid-19 becomes the driving force for 4IR
- Barry Dwolatzky and Mark Harris
The most profound change is the accelerated of way in which digital transformation and the Fourth Industrial Revolution have moved at warp speed.
In February 2020 the Presidential Commission on the 4th Industrial Revolution (4IR) finalised its recommendations. As it did so an unexpected and terrifying tsunami was gathering on the horizon. On 26 March South Africa went into a national lockdown in response to the Covid-19 pandemic.
It is still far too early to understand the ramifications of the pandemic on the country, our economy and institutions. However, one immediate and obvious consequence has been the rapid adoption of digital technology. This is driven by necessity as the world has been catapulted into rapid digital transformation.
Many people are discussing the “new normal” that will emerge beyond the current coronavirus emergency. There seems to be a consensus that we won’t simply return to our old ways of working, at least until a vaccine is available, but possibly forever. New standards for health and safety are emerging that will prioritise social and physical distancing. These standards will permanently influence the nature of the “workplace” and how work is done. What will the “new normal” look like? Has 4IR suddenly arrived?
Digital transformation inhibitors
Over recent years many digital transformation initiatives have failed, both in South Africa and internationally. In an article inForbesmagazine published on 30 September 2019,Blake Morgan wrotethat 70% of corporate digital transformations fail.
While each failed transformation initiative can be attributed to specific reasons, a common theme in almost all failed digital transformation projects is a lack of buy-in. Either executive support for the proposed initiative is insufficient or change management is unsuccessful. People have a natural propensity to resist change, and digital transformation usually involves a profound and significant change in how people are expected, or required, to behave.
In South Africa, the challenge of creating a new digital world is compounded by other inhibitors to the digital transformation such as poor connectivity, lack of digital literacy and a low level of access to suitable technology, such as smartphones.
Some examples of digital transformation in SA in response to Covid-19
Detailed case studies of how specific organisations and sectors in South Africa are responding to the pandemic are still to be written. We have, however, been collecting some of our own observations and those of others. We have used these to inform the comments that follow.
The sudden decision by the government to impose a general lockdown gave companies and institutions only three days to move to a work-from-home (WFH) policy. Different sectors dealt with this enormous challenge in different ways, some coping better than others
The health sector: Perhaps the most important example of digital adoption in the health sector has been the rapid adoption of basic tele-medicine methods. Health practitioners, including GPs, psychologists, biokineticists and pharmacists have started using tools such as WhatsApp, Zoom and various apps to engage with patients and clients. There has also been innovative use of data visualisation tools such as Google’s Data Studio to aggregate and present Covid-19 data in the form of dashboards.
Education:Although the issue of e-learning and distance education has been discussed in South Africa for decades, the sudden arrival of the lockdown caught most institutions completely unprepared. It is in this sector that the deep chasm of the digital divide has become most visible. Issues of connectivity (both the cost and availability of network connection) and access to technology and computer literacy have become critical factors. We have, however, seen rapid adoption of e-learning and distance education tools and methods.
Justice:Who would have imagined a few months ago that advocates would be arguing cases on Zoom to judges while they all sat in their studies at home? This is now happening in “virtual courtrooms” around South Africa. One of the professions most reluctant to embrace digital transformation before the lockdown has been transformed in the space of a few weeks.
We could list other sectors. Driven by necessity, individuals and institutions are willingly adopting digital technology in order to survive and continue operations. And – most importantly – the technology adopted has been existing applications that are readily available. This digital transformation has been achieved at a very low cost using technology that is free, some of it open source, and all of it easy to use.
Digital transformation in South Africa beyond the pandemic
It is our belief that the pandemic has removed some of the significant inhibitors to digital transformation in South Africa. These are:
Executive buy-in:With the arrival of Covid-19, executives who in the past were lukewarm to digital adoption now have evidence that digital technology actually works within the context of their organisation, and that it supports effective and better ways of working.
Policies and regulation:Both government and business are having to rewrite a variety of policies and regulations to accommodate the need for rapid change to cope with the changes we are experiencing.
Buy-in from staff and other stakeholders:Before the pandemic, many people working in organisations and people interacting with organisations might have been resistant to using digital technology. The pandemic has blown away many of these doubts and opened up people’s minds to different ways of working and interacting.
Concerns about cost and new technologies: A common preconception has been that digital transformation is expensive and requires the development of new customised digital solutions with a large price-tag. Many organisations have made effective use of available, low-cost (or free) solutions, most of it on the Cloud.
Concerns about skills:Another preconception is that digital transformation requires lengthy and expensive training of existing staff, or recruitment of new staff. During the Covid-19 crisis many people have rapidly and easily taken to working in a digital world.
Connectivity and access:While some short-term solutions have been found during the lockdown period, a great deal will need to be done in the future to remove the digital divide. Government, companies and other institutions have all come to realise the importance of having the entire population well connected.
Redefining a ‘job’
In the old style of working, a “job” is defined as supervised attendance at the workplace. Being employed means having a “job”, which means that one is paid to spend a certain number of hours each month at a place of work. This is usually understood as a specific physical space in an office provided by the employer. Measurements of an employee’s performance are usually relative to time spent at the workplace and managers track delivery through inspection. We might, for example, measure productivity as the output produced per time spent at the workplace.
WFH fundamentally changes the definition of a job. In the future, jobs will be deconstructed into a set of activities or tasks. In thinking about a “job” we will no longer see it as belonging to an individual. The tasks within a job might be done by different individuals, or might even be automated and done by robots. While there will still be tasks that require physical presence, this will likely be the focus of moves to drive automation. We’ll discuss this in more detail later.
A redefinition of the notion of a job brings into focus the issue of how work is measured and how it is managed. There will be a requirement for new tools and processes. These tools will be designed to give management oversight of tasks. The output of tasks will need to be monitored, measured and coordinated.
Human resource models will have to be re-examined
Contractual relationships that currently bind an individual having a job to a specific organisation will be replaced by tools that measure task outputs. Instead of me saying, “I have an employment contract with Company X that defines my job at Company X”, I will say: “I spend my day doing tasks of a certain type. I get rewarded for completing these tasks. Some of the tasks I do are for Company X.” This trend emerged several years ago under the definition of the “Gig Economy”,which is definedas an arrangement where organisations and independent workers engage via a digital platform in short-term work arrangements. The changes brought about by the Covid-19 pandemic will see this trend accelerate rapidly and will bring a larger variety of tasks into this mode of working.
Management philosophies will be dramatically impacted by new human capital data
Many of the changes brought about by remote working and a redefinition of the notions of “a job” and a “workplace” will increase the importance of data to manage the organisation. We are destined to see a transition from human-to-machine interaction to far more machine-to-machine (M2M) activity. This type of communication results in the generation and use of large amounts of data. Although this is not new, it will become far more pervasive.
Given the importance of data, all organisations will need to develop very clear strategies on the collection, storage, use and management of data. This is called “data governance” and it will become a central requirement in our new way of working.
Automation will become widespread
We have touched on automation in relation to redefining jobs and sequences of tasks, some of which might be automated, or performed by robots. Social distancing and the WFH will result in society adapting to working more interactively with chatbots, robots and other forms of automation. An important prerequisite for wide-scale automation is the availability of data. This seems set to become a reality, based partly on the increased use of M2M communication and the Internet of Things (IoT).
Covid-19 flattens the world
In his 2005 book “The World is Flat” Thomas L Friedman writes about small companies accessing advanced skill sets from around the world. If this is used correctly it will be one of the most powerful tools a company can have. It will allow small companies to compete globally and gain access to advanced skill sets (especially in areas such as engineering design) at a reduced cost for a temporary period of time. This allows small local companies to produce globally competitive products without the long-term expenses and risk of employing a large team. This can only be accomplished if done correctly.
In the post-Covid-19 “new-normal”, businesses that reject outsourcing will simply not scale at the same speed as the ones that do. For the first time, a piece of work done by an individual in South Africa vs someone outside of our country will only be differentiated by quality, speed and cost. While this might not be creating local employment, it does put South Africa in the position to start exporting technology globally, which will have a significant impact on the local economy.
Reflections on 4IR
While South Africa’s Presidential Commission on 4IR submitted its recommendations to government early this year, these will need to be rewritten in the light of Covid-19.
One of the key principles at the heart of the commission, and much of the discussion that has taken place around 4IR, is “technological determinism”, ie, technology drives change. The response to Covid-19 implies that rather than technological determinism we are seeing the opposite driver for change, namely “social determinism”. At the same time, core concepts such as the notion of “jobs” and “workplaces” are being redefined.
It has become critical that the Presidential Commission on 4IR should re-examine its recommendation from the perspective of social determinism and in the light of redefining some core concepts. While a new 4IR strategy will be required for the post-Covid-19 South Africa, it will need to take account of the many changes currently happening outside of any strategic framework.
Professor Barry Dwolatzky is Emeritus Professor at the University of the Witwatersrand and director of the Joburg Centre for Software Engineering. Mark Harris is CEO of Altron Nexus. This article first appeared in Daily Maverick/Business Maverick.
Stop random Covid-19 testing and sort out the backlog
- Marc Mendelson, Shabir Madhi, Jeremy Nel and Francois Venter
The testing backlog and proposed testing strategies outside hospital settings are threatening patient management and compromising health care workers’ safety.
The Covid-19 pandemic has created a national crisis in South Africa, requiring a State of Disaster to be enforced. As frontline clinicians and public health specialists at the forefront of this crisis, we signal an urgent need for a course correction of our testing strategy to focus it on saving lives and the integrity of the country’s health system. Acceleration of change must occur, and unnecessary testing for reasons outside of these goals must be stopped.
A medical test should only ever be performed if it will change management of an individual patient or inform a public health response. Early in South Africa’s SARS-CoV-2 epidemic, which has now resulted in 29,240 cases of Covid-19 (as of 29 May), testing for the virus served two main purposes – to triage patients and to trigger the contact tracing, quarantine and isolation cascade.
Recently, different ministries have announced generalised testing of employees returning to work (e.g. in the mines), and screening and testing of sportsmen before non-contact sporting events are allowed to restart under Level 3 restrictions. Unfortunately, these “regulations” are seemingly oblivious to realities of the national crisis facing South Africa’s capabilities to undertake Covid-19 testing.
The testing crisis in South Africa is due to internal planning issues by private and public laboratories, and a consequence of global shortage of testing kits. The number of testing kits available in South Africa within the National Health Laboratory Services (NHLS) is reportedly running dangerously low, and risk being exhausted within a matter of weeks if indiscriminate testing is not halted immediately.
Furthermore, the turnaround time (TAT) of getting results from the time of sampling is already exceeding 24 hours. Dr Kamy Chetty, CEO of the NHLS, indicated during the minister of health’s press conference on 29 May that a backlog of over 80,000 tests had built up nationwide. This is despite the valiant efforts of NHLS laboratory staff on the frontline. This translates into a TAT for a test of up to two weeks. In many instances, this renders testing a futile exercise, since by the time suspected cases tested in the community receive their results, they are less likely (if at all) to be infectious than when they presented for testing, and would have in the interim inadvertently continued spreading the virus. Consequently, a more pragmatic strategy would be the adoption of apps or web-based platforms that are widely and freely available, and that are able to screen for symptoms of Covid-19 and provide advice to the user. The same strategy was implemented in high-resource settings such as the UK at the time of the peak of the outbreak, when they too faced constraints with PCR testing.
The focus of the limited resources for Covid-19 testing available in South Africa – which is unlikely to change over the next few months – needs to be unconditionally reserved for where needs are the greatest, and that’s in our healthcare facilities.
In the hospital setting, the delayed TAT is impairing decision-making on the triage of patients and consequently negatively affecting the management of seriously ill Covid-19 and non-Covid patients and patient flow within the hospital. Consequently, more dedicated wards for suspected cases awaiting tests need to be opened.
Compounding this is the shortage of adequate personal protective equipment (PPE) for healthcare workers (HCWs), with higher levels of PPE (e.g. N95 respirators) being reserved for when managing suspected and confirmed Covid-19 cases and doing aerosol-generating procedures such as intubation. Consequently, not knowing the Covid-19 status of hospitalised patients within the shortest possible time likewise risks jeopardising the wellbeing of HCWs in these facilities.
Also, missing from rationality in the regulations for Covid-19 testing of returning employees or in the sporting environment, is the apparent failure to understand that for such a strategy to be of any use, it would require repeat testing every three to four days, as the risk for acquisition of the virus continues within and outside of workplaces as the outbreak continues its upward trajectory across the country.
This is compounded by the majority (50-80%) of individuals who are infected by SARS-CoV-2 being completely asymptomatic; hence, subsequent testing cannot be reserved for individuals with clinical symptoms of Covid-19 illness. Rather, the only pragmatic strategy available to workplaces and the return of sporting events is one that focuses on ensuring rigorous enforcement and adherence to non-pharmaceutical interventions; i.e. physical distancing, rigorous attention to hand hygiene, use of cloth masks in public, and a ban on mass gatherings (including within the social areas of workplaces).
The focus of the limited resources for Covid-19 testing available in South Africa – which is unlikely to change over the next few months – needs to be unconditionally reserved for where needs are the greatest, and that’s in our healthcare facilities.
We, and others, have repeatedly highlighted this in publications (The Conversation,SAMJ), within the advisory system of government and in public interviews. Despite the department of health taking steps to rectify this, acceleration of change is needed, and other government departments must retract regulations that will not significantly mitigate the risk of people becoming infected, but will only increase demand for testing and worsen the current testing crisis. Here is what needs to happen:
The backlog of tests must be dealt with. For the reasons outlined above, we see little point in testing any of the backlogged samples that were taken more than 48 hours previously. The backlog is such that rapid identification and separation of the mountain of tests is going to be a challenge. Realistically, those tested within 48 hours would get their result back between day 3-5, which may still influence management. As the laboratory test detects the virus’ genetic code, which begins to degrade in the days after the sample is taken, the heightened chance of a false negative result is too great, impairing interpretation. Hence, any test taken more than 48 hours previously – that is from a non-hospitalised person or any test from a hospitalised patient that is unable to be tested immediately – should be discarded. The person who was sampled, and the HCW who took the sample, should be informed with a clearly defined procedure to follow for different scenarios that the person may find themselves in at this new time point. Furthermore, we believe that all tests from the community screening programme (if identifiable) should be discarded, irrespective of sampling time, if from the country’s high prevalence areas where the ability to impact on contact tracing cascade has been lost.
The ‘tap’ regulating the flow of tests to the laboratory must be tightened, and indeed, turned off for certain testing indications. A prioritisation process for determining which persons will benefit from a test at this surge and mitigation stage of the epidemic (and the position we find ourselves in here and now as a country) must be accelerated, and focus on testing only those persons for whom it will change clinical management or protect the integrity of the health service. The process is already nearing completion, but rapid publication and communication to the public is now vital, so that everyone understands the reasons behind the new strategy of our public health response. Testing must focus squarely on hospitalised patients for the reasons given above, and on HCWs to ensure continued running of the health service in South Africa. Linking prioritisation groups to the realistic number of tests that can be performed each day allows us to optimise the testing strategy. Substitution of testing with already formulated screening apps or similar platforms that can impart advice and instruction, should be rapidly rolled out.
Regulations from government ministries outside the department of health that will not impact on mitigating the epidemic or have no scientific rationale, must be rescinded immediately. These include:
Department of Labour – the Minister of Employment and Labour is planning to amend workplace regulations to compel employers totest employeesand place them in quarantine if close contacts are infected. These tests would give a snapshot at one moment in time, but are meaningless as a once-off test, as explained above. The current department of labour regulations also state that employees that have been diagnosed with Covid-19 can only return to work once they have tested negative. This is not consistent with national guidelines or advice from the Ministerial Advisory Committee on Covid-19. The only workers for which a recommendation of testing is made to facilitate early return to work are HCWs who have a high-risk exposure to a confirmed Covid-19 patient, but who are asymptomatic themselves. This does not apply to any other worker.
Department of Sport, Arts and Culture. It is pointless to require that athletes and staff of clubs must undergoCovid-19 testing and quarantinepending results of the tests before resumption of activities during Level 3 lockdown. As for employees forced to be tested by the department of labour, these ‘snapshot’ tests will not significantly contribute to mitigating viral transmission or meaningfully address virus acquisition, and will detract from the critical focus of our testing strategy.
Our focus at this stage of the epidemic in South Africa demands that our sole attention must be on saving lives and the integrity of our health service through its workers. This can only be achieved through accelerated course correction of the testing platform, and elimination of unnecessary and wasteful testing countrywide.
Marc Mendelson is Professor of Infectious Diseases and Head of the Division of Infectious Diseases & HIV Medicine at Groote Schuur Hospital, University of Cape Town (UCT). Shabir A. Madhi is Professor of Vaccinology and Director of the MRC Respiratory and Meningeal Pathogens Research Unit,University of the Witwatersrand. Jeremy Nel is Head of Division of Infectious Diseases, Helen Joseph Hospital, University of the Witwatersrand Francois Venter is Professor of Medicine, Ezintsha, University of the Witwatersrand. This article was first published in Daily Maverick/Maverick Citizen.
Almost 16-million people allowed back to work
- David Francis, Kamal Ramburuth-Hurt and Imraan Valodia
New level 3 regulations mark an important strategic shift in the government’s approach to the coronavirus pandemic.
During the Covid-19 pandemic and response an important question from both a health and economic policy perspective is how many people are able to return to work as the lockdown is eased (and tightened). Policymakers will need to consider the likely implications for the spread of the virus.
In a recent working paper we estimated how many people would return to work, either at the workplace or at home, at the different levels of the lockdown, according to the five-level plan unveiled on April 26. Using a static analysis derived from industry subsectors matched to the five-level plan, we estimated that under level 5 of the original lockdown framework 40% of total employment was permitted, or 6.6-million workers. This rose to 55% (9.2-million) under level 4; 71% (11.8-million) under level 3; 94% (15.6-million) under level 2 and 100% under level 1. These figures are all benchmarked against employment levels in the fourth quarter of 2019, before any curbing of economic activity.
In the final regulations for level 3, which were published on May 28, there have been significant changes to the framework. The “new” level 3 allows all economic activity to resume, except for a small set of exceptions including restaurants, theatres, personal services and leisure air travel. This has significantly increased the number of people who are permitted to work under level 3.
According to the original strategy we calculated that 11.8-million workers would be permitted to return to work at level 3 of the lockdown. Under the new regulations an additional 3.97-million people will be permitted to return to work. The total number of those permitted to work under the new level 3 is about 15.8-million, slightly more than would have been permitted under the original level 2 regulations, and close to the total level of employment at the end of 2019, which was 16.6-million.
We estimate that the shift from level 4 to the new level 3 means the total number of people able to work increases from 9.2-million to 15.8-million. That means 95% of the employed workforce is permitted to return to work.
Some subsectors, such as in mining, were permitted to operate fully under the old framework and the changes will have little effect. But there are a few sectors where there has been a substantial increase in the number of workers permitted. One of these is the private households sector, a category that includes domestic workers. About 1-million more workers will be permitted to work under the revised level 3 regulations. Another large sector is manufacturing: under the previous level 3 a large portion of the sector was only permitted to operate at 50% capacity, but it is now permitted to operate fully. This permits about 300,000 more people to return to work.
This marks an important strategic shift in the government’s approach. The initial approach was to restrict all activity and then allow a set of special emergency sectors to operate. The new approach is the opposite: allow everything, except for a small set of restrictions. The new regulations are likely to be easier to regulate, are more transparent, and will result in better coherence between the health and economic strategies government is following.
The significance of this change is reflected in the large number of additional workers who are now permitted to return to work. The total change in permitted employment between level 4 and the new level 3 is 6.6-million people. Of course, in this analysis we are assuming that all workers who had jobs before the lockdown will have jobs to return to. Estimates of job losses run into the millions. It will take time to understand how many have been lost, where these losses have occurred, and whether they are permanent. We are also assuming that all of those who are able to work and have a job to return to will in fact return. This may well not be the case.
We expect a lot of statistical noise about this as we try to understand the full impact of the lockdown on unemployment and on how many workers may not be able to return to work because of concerns about comorbidities, Covid-19 infections and other perceived health risks. It also remains to be seen whether workers can be accommodated in a manner that is in line with best-practice health protocols.
David Francis is the Deputy Director, and Kamal Ramburuth-Hurt a researcher, at the Southern Centre for Inequality Studies at Wits University. Professor Imraan Valodia is Dean of the University’s Faculty of Commerce, Law and Management. This article was first published in Business Day.
Sub-Saharan Africa needs to plug local knowledge gap to up its anti-COVID-19 game
- Alex Ezeh and Sharon Fonn
Africa needs to be better prepared to deal with future pandemics; starting with a re-assessment of how countries invest in – and support – local research.
Africa remains one of the regions least affected by COVID-19, although evidence suggests it is an evolving and growing pandemic. It is now present in all African countries and territories.
From the start, the responses across many African countries have mirrored those of other countries where the pandemic has been more prevalent. These measures generally include the promotion of social distancing and personal hygiene, lockdown orders, and management of more severe cases in hospitals. Other responses, such as contact tracing, testing, and isolation of suspected cases, have been used less widely.
The implementation of lockdowns has created major challenges for governments and citizens alike. Local realities – such as urban slums – make the spread of the virus more likely and social distancing almost impossible. Lockdowns in these settings pose very high economic risks for the residents.
Given local conditions in many of Africa’s urban areas – including high density slums and informal settlements – lockdown strategies are proving to be unworkable.
Part of the disconnect between the current responses and the current realities of many Africans stems from the limited engagement between policy decision-makers and African institutions generating contextual knowledge. Some examples are the lack of an adequate notice period before lockdowns and the limited consideration given to the situation of slum residents.
The gaps in our current knowledge of the course of COVID-19 in Africa make things even more difficult.
We don’t know what accounts for the very low numbers of cases in most countries. Is it a reflection of very low testing capacity? Or rather, of Africa’s very young demographic profile? Or is it simply that we are in the early phase of the pandemic?
Each of these possible explanations will demand different policy responses.
Now more than ever, African governments need their scientists and their scientific institutions to provide insights and guidance. They are turning to these local institutions for help in managing their responses to the pandemic. Unfortunately, many years of neglect and limited investment have created capacitygaps. Where capacity does exist, it is being used, though it remains inadequate. The extent of this is being documented by a network of academics across the continent.
African scientists are not able to deliver what Africa needs because governments have starved their institutions of crucial funds for many years. The result is that governments are importing wholesale what is being done elsewhere.
What’s missing
Africa’s experiences in managing other recent and ongoing epidemics could be an advantage in responding to COVID-19. These epidemics include cholera, measles and viral haemorrhagic diseases like Ebola virus disease, yellow fever, dengue, Lassa fever, and Rift Valley fever. The potential is there, but strong research institutions and systems are needed to activate this advantage to inform timely local, national and global responses to the COVID-19 pandemic. These, unfortunately, remain underdeveloped. The use being made of the resources that doexist only underlines the need for the science and research systems in Africa to be strengthened.
For example, there has been a glaring lack of ongoing rigorous studies of the pandemic on the continent. Of the 2,032 clinical trials related to COVID-19 registered by 14 May this year, only 35 included study sites in Africa. Of these, 23 were in Egypt and only 12 included a site in a sub-Saharan African country. Seven of the 12 were internationally led multi-country studies. The remaining five were in Nigeria and South Africa.
Additionally, the 12 clinical trials involving a country in sub-Saharan Africa are extremely limited as most are looking at hydroxychloroquine, while another is looking at traditional medicine.
This pattern positions Africa to remain a consumer of knowledge and solutions produced elsewhere.
And, during this period of a global pandemic with critical shortages of life-saving resources, Africa is losing because it lacks the capacity to produce what it needs and what others may need.
What needs to be done
What key actions need to be taken?
The first lesson for Africa is that it cannot continue to depend on international and multinational agencies to determine the path it takes to development. We must reverse the limited investments in local and regional research institutions and universities. Countries must do more to attract their best minds, many of whom have been forced, over the years, to leave Africa.
As we look towards a post-COVID-19 world, investments in strengthening local and regional knowledge-based institutions will be key to enhancing the continent’s global relevance and competitiveness.
And we need to understand where we currently are in the course of the pandemic. This requires clarifying the drivers of current low levels of reported infections and deaths. Achieving this will require coordinated serological antibody surveys across countries with different epidemiological profiles of the pandemic. These surveys would be a game changer.
At the moment countries are only doing antigen tests. These tests are positive if a person is currently sick with the virus. Once the person is better, the test will again be negative. Antibodies, however, last longer in people who have contracted a virus and will be positive in asymptomatic people as well (it is not yet known for how long). An antibody survey would involve selecting a sample of people who are representative of the entire population and testing them. This will show how widespread the infection has been in a given population.
Such antibody surveys will show who has had the virus – and therefore has built antibodies (some kind of immunity) to it. This will be key to formulating appropriate context specific responses to the pandemic. And it would help us understand where a country’s responses to the pandemic have been appropriate.
These surveys could show us, for example, if the lockdown policies have been beneficial, or if there have been very widespread infections but with mild morbidity and very low mortality, perhaps due to the continent’s young age profile. This would mean the quarantines and lockdowns have come at a high price with less than anticipated benefits.
Combining such surveys with community studies that include verbal autopsies – interviewing people who were close to the person who died, and from this deciding the cause of death – could show if the lockdown is leading to increased mortality within communities that are not being captured in our accounting of COVID-19-related deaths.
Understanding the extent of the spread of COVID-19 within urban and rural Africa can also help with the adaptation of policy responses to a specific setting. This is urgently needed as many countries are in the middle of their rainy season when most villagers cultivate their farms. Disruptions in farming activities, coupled with the effects of climate change-related floods and an ongoing locust epidemic in East Africa, could spell an uncertain future for hundreds of millions of people as they begin to face massive food insecurity.
Evidence from such studies can help countries calibrate their national responses to the pandemic.
In the long term, we must be better prepared to deal with future pandemics, and that preparation needs to start with a re-assessment of how we invest in and support local research and service delivery institutions across Africa.
This article draws on contributions to Drexel University’s Webinar on “The Global Impact of Pandemics”; the African Development Bank’s Global Community of Practice Webinar on “Enhancing Resilience in African Economies: Macro-Economic Policy Responses to COVID-19 Pandemic in Africa”; and the Think-20 Engagement Group and Global Solutions Summit Panel on “The Social and Economic Implications of Covid-19 Pandemic and Beyond: Risks and Opportunities for the Global South”.
Pasha 66 - The Conversation Africa's podcast series focus on "Coronavirus conspiracy theories and myths".
The coronavirus was made in a laboratory in Wuhan, China.” “COVID-19 is not real and comes from 5G network towers.” “Drinking warm water with lemon juice will kill the coronavirus.” “The flu vaccination will mean I won’t get COVID-19.” These are all conspiracy theories and myths shared on social media platforms. And it’s time they were addressed.
In today’s episode of Pasha, Neelaveni Padayachee, a lecturer in the Department of Pharmacy and Pharmacology, and Lisa Claire du Toit, an associate professor, both at the University of the Witwatersrand, talk about false ideas surrounding the coronavirus.
Wits thanks SA Post Office for delivering laptops to students
- Wits University
SA Post Office enables online learning through the delivery of almost 5 000 laptops to Wits students across the country.
The Speed Services Courier Unit of the South African Post Office (SAPO) delivered almost 5 000 laptops to the homes of disadvantaged Wits students across South Africa – including in rural areas, thereby allowing these students to continue with their studies online.
The University suspended contact teaching due to the national COVID-19 lockdown and commenced with emergency remote teaching and learning on 20 April 2020. In its transition to online learning, Wits established a Mobile Computing Bank that granted qualifying students access to a mobile device for online learning purposes. A partnership with the SAPO ensured that students who needed mobile devices could continue learning during the lockdown. SAPO successfully delivered these devices to the homes of students.
SAPO Acting CEO, Ivumile Nongogo hailed the sterling service of the SAPO staff who ensured the seamless delivery of mobile devices to Wits students.
“I want to commend our drivers and other employees for their dedication during this time when regular transport connections were not available. This is another example of the role that the Post Office plays in making South Africa’s infrastructure work and bringing services to the people,” he said.
Professor Adam Habib, Wits Vice-Chancellor and Principal expressed his deep gratitude towards the SAPO.
“All devices were delivered promptly by SAPO employees to students at various locations across the country (including many rural areas), thus enabling the students to participate in the University’s online academic programme. This project is an exemplar of how public institutions can work together efficiently to achieve a common good that benefits society,” he said. “We are appreciative of the SAPO and its efficient delivery of services that has positively impacted on the lives of thousands of students.”
This mutually beneficial relationship has benefitted students, Wits and the SAPO and we look forward to partnering on similar projects in the future.
Covid-19 (Update 32) - Wits Screening APP goes live
-
Self-screening form on the app is for staff members with permits to be on campus, and students who have been invited to return to campus only.
The Wits Screening App (LogBox Patient Application) is now live and can be downloaded from the App Store or the Google Play Store.
Staff members with permits to be on campus, and students who have been invited to return to campus must COMPLETE THE SELF-SCREENING FORM ON THE APP EVERY DAY, BEFOREentering campus.
Download the Logbox Patient Application from the App Store or the Google Play Store.
You will receive a notice on your mobile phone that either clears you for entry or denies you entry to campus.
Show your clearance note to the security officers before entering campus.
For those staff members and students without smartphones or computers, hard copies of the screening form can be filled in and/or dropped off in boxes at the gates.
Pasha 66 - The Conversation Africa's podcast series focus on questions arising from the symptoms of people who have contracted the coronavirus.
COVID-19 is proving a hard medical nut to crack. Why are some people asymptomatic? Why do some people have different symptoms? Why are children hardly symptomatic and why do older people seem to be hit the hardest?
In today’s episode of Pasha Tom Boyles, an infectious diseases specialist at the University of the Witwatersrand, answers these, and other questions.
What sets good and bad leaders apart in the coronavirus era
- Lawrence Hamilton
It is no accident that those leaders who have responded worst to this crisis have been the main sources of countless conspiracy theories and misinformation.
Crises bring out the best and worst of politicians and populations. Folly, fear and fortitude are on display everywhere. In the main, democracies have fared better than non-democracies in handling the coronavirus pandemic.
But the record is very varied indeed. What explains this? What can be done about it?
Among democratic regimes, at the one extreme we have seen denialism, the denigration of scientific advice and an obsession with putting the economy before lives. This is especially evident in the United States and Brazil. At the other we have witnessed the organised, prudent, empathetic responses of countries such as South Korea, New Zealand, and Finland. South African president Cyril Ramaphosa initially did very well, but some subsequent decisions might damage his good record.
These two extremes of leadership style were evident even before COVID-19.
The USA and Brazilian responses to the pandemic, led by President Donald Trump and President Jair Bolsonaro, have been characterised by secretive, narcissistic, paranoid, hubristic and impulsive decision-making. These actions have endangered the lives and livelihoods of their residents, over which they have a duty of care.
The data bears this out well. Despite having arrived on their shores relatively late, the pandemic has ripped through their populations, with no sign of abating. They lead in infections and deaths.
At the other extreme, a common denominator has been a firm attempt by political leaders to “follow the science” and control the spread of the virus and fake news from the outset. A combination of transparency, prudence, empathy, timing and courage has produced excellent results in South Korea, New Zealand and Finland.
What becomes clear is that in these fast-moving and life-defining times in democracies a great deal depends on the quality of the elected leadership. Democracies that happen to have leaders who simultaneously engage empathetically with those they govern and are informed by good science are best able to deal with the crisis.
They gather clear-eyed knowledge of their countries’ particular circumstances, and display courage and timing in making critical and sometimes unpopular decisions. They are able to overcome many of the challenges that the pandemic throws up.
Democracy helps, but it is not the deciding factor. What matters most is what kind of leader is in place, where his or her priorities lie: the well-being of the populace or the interests of a small group.
Politicians judge best when they listen to their populations and learn from the science. That is why democracy is uniquely placed to engender good judgements, as the Indian economist Amartya Sen argued with regard to famines, and I have argued elsewhere.
Yet, it would be mistaken to think that democracy guarantees good judgement. If the purveyors of conspiracy theories and exemplars of prejudice are also your democratic leaders, democracy itself cannot resolve things. It only gives citizens the power to remove those leaders at the next election.
Bread, circuses and crises
In the current crisis, Ramaphosa has done a much better job than Trump and Bolsonaro.
Ramaphosa got off to a great start. He acted firmly, quickly, with clear justification and impressive results. South Africans have just emerged from one of the most severe lockdowns imposed anywhere in the world. This kept the infection rate nearly as low as that of South Korea, though it is now shooting up.
During this period, however, there have been at least two problematic decisions that undermine public trust and thus how people may behave.
The first is the decision to ban the sale of tobacco. Even if we could distinguish sharply between basic needs and other needs – something I dispute – the idea that addiction to smoking falls into the latter category, and that, along with the fact that COVID-19 is a respiratory disease, justifies the ban, is misguided. For an addict, the need for a cigarette may often trump even the need for vital nutrition.
The second is the decision to allow religious gatherings to resume under lockdown level 3. Having spent so long restricting gatherings, to now allow larger gatherings seems like folly. It is well known – cases abound from South Africa to South Korea – that, like funerals, large religious gatherings are super-spreading events.
Along with the ban on tobacco products and the incorrect assumption that the state could directly meet the basic nutritional needs of the population via the delivery of food parcels, the response to the religious lobby is reminiscent of Juvenal’s comment under imperial Rome some two thousand years ago that all the people really want is “bread and circuses”. This is not what people want or need. They require the power to express their actual needs and interests and the democratic means to ensure that government responds to these.
Ramaphosa’s good leadership has been undermined by a paternalistic attitude to people’s needs and seeming deference to South Africa’s powerful religious lobby.
Lessons to be learnt
Two things can be learnt from the varied responses to the coronavirus crisis.
First, we must use it to find a roadmap for how we can properly make the health and well-being of a state’s population the raison d’être of its government. The first thing to identify is that health is not the “absence of disease” but the status we each have when our ever-changing needs are optimally satisfied. For this, we need a politics that allows us to express and assess our needs, and determine who is best placed to represent us in responding to these needs, all in non-dominating conditions.
Second, given that it is no accident that those leaders who have responded worst to this crisis have also been the main sources of countless conspiracy theories and misinformation, we must learn to keep oligarchs away from political power. Under representative democracy, bar outright revolution, we do not have the power to affect the everyday decisions of our representatives, but we can keep those with exclusive social and economic interests out of positions of political power.
Climate change, biodiversity loss and other global ills share root causes
- Mary Scholes and Robert (Bob) Scholes
By identifying the roots of global ills there's an opportunity for coordinated action as countries lay new pathways for a post-Covid world.
The modern world seems to lurch from one crisis to another. What if that is because the crises have shared underlying causes, and therefore tackling them as if they were independent events is doomed to fail?
The issues of climate change and biodiversity are deeply intertwined. The United Nations Framework Convention on Climate Change and the Convention on Biological Diversity, the international treaties charged with solving two of the biggest problems of the 21st century, were both due to hold make-or-break meetings in 2020. COVID-19 – yet another crisis with strong connections to the other two – has forced the meetings to be postponed. The only positive result is that the delay provides an opportunity to better coordinate actions, in order to lead to better outcomes.
To mark World Environment Day on 5 June, the Commonwealth Academies released a statement on climate change, biodiversity and sustainable energy. The statement stressed the grave risks to people and nature of allowing the global climate to warm at its current rate and draws attention to the accelerating rate of biodiversity loss. It proposes that a rapid transition to predominantly renewable energy sources can help alleviate both issues. The statement calls for urgent leadership.
This article explains the logic behind that statement, linking three apparently different issues. By identifying the connections we reveal the opportunities for coordinated action and the pitfalls of continuing to pursue independent agendas.
Rapid species extinction
The world is in the throes of a “sixth extinction crisis” – an accelerating loss of species at a rate far more rapid than the evolution of new species. Such a loss was last seen sixty million years ago, when Earth collided with an asteroid. The result is the unravelling of the ecosystems which we depend on for our well-being.
For the past few centuries, the main cause of declining biological diversity has been habitat loss – the relentless replacement of natural ecosystems by croplands, cities and managed forest, to meet human demands for food, timber and raw materials. That process continues.
Apart from driving our co-inhabitants of the planet to extinction, land use change is the most important cause of climate change after the burning of fossil fuels. Human encroachment on nature is also the root cause of the emergence of novel zoonotic diseases such as COVID-19. So if we could stop deforestation, we would help solve three problems at the same time.
Climate change
But as we move into the middle part of the 21st century, the biggest future threat to plants and animals is climate change. Despite the undertaking by most of the countries of the world in Paris in 2015 to stabilise the global climate at safe levels by mid-century, the climate continues to warm at an accelerating rate.
As a result the climate comfort zones of millions of species are moving faster than they can keep up. Our main strategy thus far for conserving biodiversity – the creation of protected areas – is increasingly irrelevant. The single most important thing we can do to save nature (and ourselves) in the 21st century is to cap global warming at no more than 1.5℃. In other words, the fate of nature is being decided by the outcome of climate negotiations, not biodiversity discussions.
As South Africa learned the hard way, when we afforest ancient, species-rich grasslands with monocultures of alien trees, the rivers dry up and biodiversity is lost. There are potentially similar problems with simply replacing fossil fuels with bio energy crops. The vast areas required will either displace food crops or further encroach on natural habitats.
Energy generation
Renewable energy – particularly solar and wind power – offer far more sustainable futures. They are not without impacts on biodiversity, but the magnitude of those impacts is much less than the effects of climate change, driven by fossil fuels and land use change.
The remarkable worldwide reduction in atmospheric pollutants and the resurgence of nature while travel and economic activity were suspended under COVID-19 restrictions give us a glimpse of what we have lost and what we stand to gain.
Those effects will be short-lived, but they do show that when the world perceives a problem to be urgent and critically important, it can very quickly take actions previously said to be completely impossible. That is the lesson we need to apply to the much more life-threatening, and just as urgent, challenges of climate change and biodiversity loss.
Covid-19 update (33) - Secure gateway enables teaching and learning
- Wits University
Students and staff members who have not already done so, must complete the student survey or staff survey before 8pm on Thursday, 11 June 2020.
Wits University has partnered with Vodacom to implement a secure gateway, which enables staff and students to access teaching and learning resources.
This solution will provide staff and students with 10GB daytime and 20GB night-owl data bundles per month for use on selected URLs that can accessed through the Wits network for teaching and learning purposes. This is available on Vodacom SIM cards only.
A comprehensive set of Frequently Asked Questions can be downloaded, which explains how you can access the data: www.wits.ac.za/mywits/data-access/. You will have to download the CISCO VPN app and have a R5 Vodacom sim card to access the solution (the R5 will be refunded through airtime).
Students and staff members who have not already done so, must complete the student survey or staff survey before 8pm on Thursday, 11 June 2020 in order to inform the University of their Vodacom number or to advise if they do not want to receive the data.
Please direct all queries to DataHelp@wits.ac.za – the ICT team will respond within 24 hours.
Thank you.
SENIOR EXECUTIVE TEAM
10 JUNE 2020
South Africa needs a new governance model post-Covid-19
- William Gumede
South Africa’s governance model, the way the country is run, is broken.
Without a new governance model, South Africa will be unable to overcome the Covid-19 health, social and economic crises; and the country is likely to plunge into economic chaos, social breakdown and rolling violent unrest. To save South Africa from such a frightening fate, a new governance model is urgently needed.
Here’s 10 pillars that should be the foundations of a new post-Covid-19 governance model for South Africa.
Evidence-based policy must be a key pillar of the management strategy model of the country. This will make government policy more logical, credible and palatable, to wider constituencies. Over the past few years, government policy-making has often either been based on ideology, wishful thinking or being corrupted.
Merit must be principle of government operations. The talents of all South Africans, no matter their colour, ethnicity or political affiliation must be used to rebuild the economy.
Merit-based appointments to government positions and to structures that oversee Covid-19 economic restructuring are crucial. Crony, cadre and pork-barrel appointments to government structures has wreaked destruction since 1994, undermining public service delivery, wasting scarce public funds and destroying government’s credibility. Government contracts must be awarded based on merit, fairness and value for money.
Commonsense must drive government decisions, actions and policies. Many government policies, decisions and actions over the past years have made little rational sense. This definitely have to change.
There has to be greater accountability from elected and public representatives. There has to be consequences for wrongdoing. People must be hold accountable for wrongdoing. The culture impunity must come to an end.
Accountability strengthens the credibility of government, and importantly motivate citizens to willingly comply with government directives. If citizens perceive there a lack of accountability among elected and public representatives accountability, citizens readily defy government injunctions.
There has to be partnerships between the public, private sector, civil society and communities to reconstruct the post-Covid-19 economy. The private sector and civil society are not the enemies of government to be in mortal combat with as many ANC leaders may misguidedly belief.
It is also a fallacy to think as many ANC members or others do, that the state can go it alone. The state simply lacks the capacity, resources and ideas to execute economic policies on its own. Partnerships not only bring goodwill, they bring skills, resources and wider-buying for policies, decisions and delivery.
Government must govern honestly. Without honesty, there can be no trust, the glue of effective partnerships, citizen compliance and willingness to behave public-spiritedly. This includes government communicating honestly to citizens, beyond the traditional faceless press statements, doublespeak and gobblygook, is crucial rally citizens behind government initiatives.
Entrepreneurship has to be heart of post-Covid-19 economy reconstruction. Entrepreneurs create new industries, new jobs and new wealth. They increase the size of economies. They fuel economic growth. They inspire a virtual cycle of others trying their hand at starting new businesses, new developments and new initiatives too. In South Africa, entrepreneurship will have to be promoted across society - within the state, private sector, civil society and communities.
Corruption has to be tackled with greater seriousness. No successful posti-Covid—19 reconstruction is remotely possible with the government seen to tackling corruption, especially corrupt by untouchable politically connected ANC cadres, political capitalists and tenderpreneurs. Corruption that is not dealt destroys the credibility of government, trust and encourages corruption across society.
The rule of law is fundamental. The rule of law must apply to everyone equally. The rule of law cannot just be applied to ordinary citizens. The politically-connected cannot be exempted from the law as has been the case since the end of apartheid. Neither should there be untouchables, which appear to be above the law, such as minibus taxi drivers and bosses, gangsters and building hijackers.
The poor, vulnerable and marginalised must always be cared for, without this principle, there will be no post-Covid-19 economic reconstruction possible. The, country will go up in flames on the back of their. The Covid-19 crisis offers a fresh opportunity to fix South Africa’s broken governance model. Without fixing the broken governance model a new equitable, inclusive and peaceful society is not possible.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand; and author of Restless Nation: Making Sense of Troubled Times (Tafelberg)
This is an edited extract from the Academic Review Paper, “Priority Setting for Interventions in Pre-and Post-Pandemic Management: The Case of Covid-19, analysing Government’s Covid-19 response. The report was done in partnership with the South African Technology Network (SATN) and National Scientists and Organisations.
Does alcohol have an undisclosed African heritage?
- Neil Rusch
Until now the search for early evidence of alcohol has fixated on residue analysis.
Alcohol is the most widely used psychoactive substance in the world. But where was the first alcoholic beverage brewed and consumed?
The answer isn’t clear because traces of alcohol don’t preserve well in the archaeological record. Containers like skin bags and wooden vessels that were likely used to hold alcohol don’t survive indefinitely. This poses a problem because residue analysis relies on the preservation of containers and implements.
The earliest evidence of alcohol comes from starch granules, either wheat or barley, transformed by fermentation. These were found in Raqefet Cave in Israel and are dated to 13,000 years ago. Chemical traces of alcohol have been detected in containers from Neolithic China. These were used in the seventh millennium B.C.E for the storage and dispensing of a fermented drink made of rice, honey and fruit. Early evidence of wine has been found in Northern Iran and dated to the mid-sixth millennium B.C.E.
Where does the African continent fit into the story of alcohol? Until now the search for early evidence of alcohol has fixated on residue analysis. But I tried a different route – I looked at the role of honey, because honey and bee-related products were being used and consumed 40,000 years ago by people living in southern Africa.
First, I conducted a fermentation experiment in which alcohol is produced by combining honey, water and moerwortel (Glia prolifera).
The procedure and combination of ingredients follows an indigenous method, as was conveyed to the botanist Carl Thunberg by indigenous Khoe-San informants in the 18th century. Results of this experiment are contextualised using ethnohistorical and early traveller testimonies that suggest widespread use of honey-alcohol combined with plant material for psychotropic and medicinal purposes. This included kanna (Sceletium tortuosum), which produced a ‘spiked’ honey drink known as khadi.
Controlled fermentation may have emerged as early as the Middle Stone Age (which started about 280,000 years ago and ended between 50,000 and 25,000 years ago) together with manifestations of complex behaviour and mental processing that was cognisant and capable of using a suite of complementary botanical, technical and chemical methods for various applications. These included making arrow poison and the synthesis of compound materials for the manufacture of mastics, adhesives and pigment.
From this research I conclude that honey was the most likely catalyst that allowed controlled fermentation to commence at a very early date in Africa, with the weight of probability pointing to southern Africa.
The background
In my research, I’ve also provided an explanatory framework that encompasses a Middle Stone Age and deep-time perspective. This helps to explain the related themes of honey bees in southern San mythology, pictorial expression and fermentation practices.
Fragments of knowledge about honey fermentation are retained in ethnohistoric accounts and among communities that continue to use honey to make alcohol, to this day. The association between alcohol, honey and bees has pre-historical antecedents. We see this in the form of rock paintings that feature bee-related themes. Mythology, widespread among the San of southern Africa, considers bees, wax and honey to have magical qualities.
The cognitive requirements necessary to support an understanding of chemical and technical processes (such as fermentation) are manifested in the last 100,000 years in the Middle Stone Age in southern Africa. These processes include bow hunting, about 60,000 years ago; the use of ochre compound, interpreted as paint, around 100,000 years ago, and arrow poison, 24,000 years ago. Arrow poison was possibly used even earlier.
Intentionally controlled fermentation fits comfortably within these techno-behaviours but leaves no archaeological trace.
What we do have, though, is a parcel of beeswax. This tells us that honey and bee products were being used and consumed 40,000 years ago in southern Africa by people living at Border Cave, near the present Eswatini (Swaziland) border.
The Border Cave beeswax is an important biomarker: (1) it is the oldest known example of the use of beeswax anywhere; (2) it makes explicit the connection between honey, bees and plant poison.
From this information it is reasonable to infer that controlled fermentation arose on the African continent alongside bow hunting and the use of poison tipped arrows, some time between 60,000 and 24,000 years ago.
Within this time bracket, what is certain is that at 40,000 years ago early people were using and consuming bee products.
Does this mean that fermentation of honey-alcohol was attempted 40,000 years ago? We cannot know for sure. All we can say is that the conditions were highly conducive.
Ongoing questions
Honey is the most likely catalyst that allowed controlled fermentation to commence at a very early date in Africa, with the weight of probability pointing to southern Africa, given current evidence. And chemical analysis of the Border Cave beeswax provides added incentive for continuing investigation.
So you think investing in fever screening can curb the spread of COVID-19? Think again
- Andrea Fuller and Duncan Mitchell
Detecting fever requires measuring core body temperature. Screening measures the body's surface temperature.
As lockdowns are lifted, procedures are being put in place to reduce the spread of COVID-19. Along with physical distancing, hand sanitisation and wearing of masks, fever screening is increasingly being set up as a requirement before entry is allowed into hospitals, shops, workplaces and schools. But there are physiological and clinical reasons why fever screening simply won’t work.
Andrea Fuller and Duncan Mitchell explain why fever screening is unlikely to reduce the spread of the virus. Their arguments are based on an understanding of the physiology of fever, body temperature measurement, and fever prevalence in people who transmit COVID-19.
What happens to your body when you have a fever?
Fever is a temporary elevation of body core temperature. It is part of a defensive response to infection by a virus.
When you develop a fever, you feel cold, heat generation in your body increases (achieved by shivering) and heat loss decreases (achieved by seeking warmth, covering up and reducing the flow of warm blood to the skin). When a fever breaks, either naturally or because you have taken an antipyretic like paracetamol, you feel warm. Your reactions include increasing the flow of warm blood to the skin and sweating, which helps to bring the body’s core temperature back to normal.
What are the limitations to infrared thermometers or thermal cameras detecting fevers?
Detecting fever requires measuring body core temperature. To do that accurately, you need to put a thermometer into the body core. Temperature in the rectum and the mouth get close to body core temperature.
Needing to measure body core temperature raises the first problem with fever screening. Thermal cameras and infrared thermometers measure heat radiating from a surface – in other words surface temperature. They don’t measure body core temperature.
But the forehead skin or inner eye temperatures that infrared thermometers or thermal cameras usually measure in fever screening are not body core temperatures.
Human surface temperature is heavily influenced by environmental conditions. In cool environments, surface temperatures can be much lower than body core temperature. And doing exercise, or being exposed to the sun, can raise the temperature on our foreheads above body core temperature. Thermal cameras screen for high skin temperature. They can and do find high face temperatures that have nothing to do with infections. Those “false positives” waste time and money in unnecessary follow-up.
Another problem is that skin temperature does not rise during the developing phase of a fever. It falls, because warm blood is kept away from the skin. So your skin temperature changes in the opposite direction to your body core temperature.
Thermal cameras would declare you safe, because your skin temperature is low, but you could be in the most infectious phase of the fever. No surface temperature is a reliable indicator of fever.
Could better fever screening detect COVID-19?
Even if infrared thermometers could detect fever reliably, they could not detect COVID-19 reliably. Nor could any other thermometer. Patients with COVID-19 are not guaranteed to have a fever.
Recent research indicates that many people who test positive for COVID-19, and especially children, never have any detectable sign of illness, including fever.
To add to the problem, not all patients with symptoms will have a fever, at least on the basis of once-off measurement. Only 31% of patients presenting at New York State hospitals with COVID-19 had fevers.
So, in addition to not measuring body core temperature well, infrared thermometers are being used to find a high temperature that many people exposed to COVID-19 won’t have.
Has fever screening ever helped to prevent the spread of viruses?
Thermal cameras were introduced at airports at the outbreak of the 2002/3 Severe Acute Respiratory Syndrome (SARS) pandemic. They were widespread in airports during the 2009 Influenza A (H1N1) pandemic. But for medical and technological reasons they have failed to prevent the import of any virus causing respiratory disease. They have failed even in combination with other interventions like follow-up contact and health declaration questionnaires. For example, 930 people who presented as potentially infected candidates were picked out by thermal screening from over 9 million passengers entering Japan in 2009/2010. But not one case of H1N1 influenza was diagnosed.
The data from Ebola shows the same pattern. Not one case of Ebola virus infection was picked up in 166,242 airport passengers screened when entering and leaving Sierra Leone in the 2014/2016 outbreak.
In the case of COVID-19, CNN has reported that no cases were detected among the more than 30,000 passengers screened with thermal cameras at US airports by mid-February 2020 .
Some scientists have been forthright about the dubious value of fever screening, arguing that border screening for infectious diseases should not be continued.
Is there any place for fever screening?
Perhaps, there may be benefits.
Some people with viral infections who know they are sick attempt to conceal their illness. Travellers wanting to fly home are prone to do so. Others take antipyretic drugs, hoping to avoid triggering thermal cameras.
Though there still is no scientific evidence, researchers have suggested that the prospect of being caught by fever screening is a deterrent to such dishonesty.
But we do not believe that the potential benefit outweighs the negatives. Apart from fever screening being unreliable, infrared thermometry poses a risk to thermometer operators who are required to come up close to potentially infected persons. Successfully passing a fever screen can create a false sense of security. And the thermal cameras used for mass screening are costly. So are the personnel required for any fever screening.
Society is not ready to safely reopen schools and education centres
- C-19 People’s Coalition
Government is steaming ahead with the reopening of schools. This is an overly hasty, ill-considered step for a number of reasons.
The government plans for reopening schools are underway. But Covid-19 infections and deaths are rapidly increasing. Testing is still severely delayed, and effective tracking and tracing isn’t yet in place. In response to this, the government seems inclined tonarrowthe criteria for who gets tested even while pushing to reopen schools.
But we need all these public health measures to identify infection clusters and learn how reopening schools affects viral spread so we can respond appropriately. Announcing reopening dates before schools have all safety measures in place and before we are able to track and trace the pandemic is arbitrary, and premature. Any decision to reopen must follow the evidence of health and safety at schools and the societal state of spread/containment of the virus.
Some loud voices insist that children are at lower risk of suffering Covid-19 symptoms so schools must reopen immediately. But the evidence on how children transmit the virus is not yet clear in South Africa or internationally. We do not know how much children can infect adults, especially those who are elderly or at high risk. It is irresponsible to insist on using partial and conflicting evidence to make unqualified claims about the safety of opening schools.
Given this context, society is not yet ready to safely reopen ordinary schools, special schools, special care centres and early childhood development centres. The risks of school infections are especially high because:
Many schools lack sufficient water, toilets, soap, masks, textbooks and classrooms (and once these are supplied, schools need time to establish safe routines);
Budget cuts mean there are not enough teachers for physical distancing in schools;
Many teachers are at high risk because of their age and illness profiles, and there are insufficient measures in place to protect them; and
Learner transport is unsafe and too crowded.
Opening justly, not just opening
Our education system is unequal and unjust. The short-term plan must use this time of school closure to prepare and strengthen education, and contribute to the goals of a longer-term plan so that we have a unified education system that serves all our children justly, freely and equally. We have an unusual opportunity to address long-standing injustices. We should not waste it.
We must all think creatively, together, about how to educate each other in this time of crisis and how to use this time to bend schooling towards free, equal education for all. Education is wider than schooling: education is about learning to live together critically in the world as it is, struggling towards the better world we must build. This social learning must lie at the heart of our struggle against Covid-19, the social crisis it has intensified, and the unjust, unequal education system.
Who decides?
Schools and education centres are social resources and human communities for the public good. Millions of learners and caregivers, and hundreds of thousands of teachers and early childhood development (ECD) practitioners, are involved in education. The minister and education bureaucracy can’t unilaterally announce when it is safe to reopen. People themselves, in local school communities, must be integral to deciding democratically whether and when they are ready to reopen schools, in context, equitably and safely across society. People’s involvement must extend beyond “consulting” school governing bodies (SGBs).
In line with democratic principles, we demand that the national and provincial education departments make policymaking transparent and open to real public engagement:
Education departments must make public which experts they are drawing on, what research they are using to inform their decision-making and the minutes of all meetings;
They must recognise and seek out the invaluable contextual knowledge that teachers, support staff, learners and caregivers have: they are experts who know their own contexts best;
They must invite the public to participate directly in developing policy – not just inform them via National Education Collaboration Trust (NECT) representatives;
They must invite the public to guide budget priorities and monitor contractual deliverables and spending;
They must empower local school communities, including SGBs, parents, students, principals, teachers, civic bodies in local communities such as churches, welfare providers, sports and recreation clubs, and religious structures, to decide on whether schools should be reopened or not; and
If schools decide to open, they, in collaboration with local communities must be provided optimal sanitary resources by the provincial education departments and districts to secure safe, and healthy conditions of learning. School communities should be empowered to secure deep cleaning, sanitisation, safe distancing, and the delivery of water, food and health security.
Importantly, the national Department of Basic Education must develop clear roles and responsibilities, and hold provinces to account for failing to comply with its directives. This will reduce the petty power struggles and bickering over responsibilities which have made our schools a battleground for party politics, spreading confusion, and undermining coherent and realistic policymaking.
Prepare infrastructure and support teachers
Poor infrastructure and insufficient support for teachers are central obstacles to responding effectively to Covid-19. So the Department of Basic Education should work hand-in-hand with the public to pursue the following concrete measures, with all effort, immediately:
Ring-fence a portion of Covid-19 funds for preparing and strengthening the education system;
Work with the Department of Public Works to build and rehabilitate school infrastructure, and encourage the employment of local community members; and
Support and work with teachers to:
Identify teachers at risk and work with them to identify how they can safely participate in education: for example, by collectively developing open-access textbooks, storybooks, and learning aids
Identify young and unemployed teachers and integrate them into the education system on equal terms with public sector teachers
Identify all teachers employed by SGBs as their jobs are at risk: they must be formally employed by the state on equal terms with public sector teachers
Identify teachers who are teaching out of phase and out of subject, and work with them to reallocate them appropriately
Work with teachers to develop more creative physical distancing solutions, where schools decide with their learners and teachers how best to use their space and time equitably.
Work with teachers to build a realistic school calendar and timetable for learning that is structured around the pandemic instead of an artificially imposed “academic year”.
Support schools to serve communities
Communities have real, serious needs for nutrition and childcare, because the economy is forcing caregivers to risk their lives and return to work for others’ profits and to earn just enough to eat. We must address these needs by understanding and using schools as community resources while they are closed for formal teaching and learning. When teaching resumes, schools will have stronger relationships with their community and continue to build on these programmes.
To this end, the Department of Basic Education must work together with the Department of Social Development to recognise and strengthen the social role of schools in communities:
Use schools as nutrition centres for both children and adults: children need to eat to learn, but all people need nutrition to learn and live;
Use schools to distribute public health awareness literature;
Use schools to identify at-risk families and provide psychosocial support through social workers;
Use schools as spaces where other state support programmes can be supported and housed, such as SASSA grant disbursement; and
Use schools as tracking and testing spaces for specific areas surrounding the school.
Support schools for social learning
Government’s obsession with “saving” the academic year is unrealistic and unjust.
It is unrealistic because the government’s regulation that only 50% of learners can be at school at any time means that learners (outside of Grade 12) will be out of school half the time. Schools that reopen may need to reclose; many teachers and learners will spend time at home, in quarantine or isolating. Given this, it will be impossible to “complete” the CAPS curriculum on its own terms.
It is unjust because the curriculum has already been failing us, as struggles for free, decolonised education have articulated. The curriculum should define what people and communities believe is important for everyone to know and be able to do, and identify human knowledge and skills which should be accessible to all.
Moreover, education should enable and enrich life, learning, and life-making, together for all. It is not just about ensuring that the minority of learners who matriculate have a certificate for an inequitable and unjust job market.
The government’s insistence on “saving the curriculum academic year” prioritises saving face over supporting everyone to learn. Dropping the folly of trying to save the academic year will give the school system the flexibility to respond to the pandemic when, for example, infections increase exponentially, or when schools respond to the psychosocial, food and health needs of learners.
Together, we can build a just and emancipatory popular education using social learning. To do this, national and provincial education departments must work together with schools, families and communities to support learning.
First, learning happens at home and in the community as much as it happens in school. Education departments must support this learning through:
Asking caregivers how they cope during holidays and sharing this to guide childcare practice and policy;
Rolling out public mobile libraries to support reading at home;
Rolling out public toy libraries to support playing at home; and
Implementing realistic and practical distance learning initiatives accessible to all. Instead of the government’s unrealistic and inequitable emphasis on 4IR and online learning, we must use public and community radio and television for distance learning. Here, we can learn from what other countries are doing and have done. This should be complemented with the delivery of printed materials through schools.
Second, national and provincial education departments must pay special attention to children who have been unjustly excluded from the education system:
Hundreds of thousands of children with disabilities who are excluded from formal schooling;
Millions of children who are pushed out of schooling for socio-economic reasons and then blamed as “drop-outs”; and
One million undocumented children who were excluded until this year from accessing basic education.
Education departments must publicly acknowledge that the education system has failed these children, and openly ask for the public’s help to fundamentally transform the education system to ensure equitable and truly inclusive participation for all.
Strengthen education financing and governance
Over the medium term, the national Department of Basic Education must recognise that three issues are the key drivers of inequality and injustice in education: financing, school choice and decentralisation.
Financing
The national Department of Basic Education has a duty to:
Pressure Treasury to protect and increase the education budget over the next three years to reduce teacher-student ratios. The education budget must not be cut after years of decreasing real spending per learner. Education funding must be increased significantly to build a just, free, equal schooling system. And this must not be used as an excuse to cut funding for ECD and post-school education, or other social spending;
Pressure Treasury to prioritise education over non-social spending, such as the Security Cluster. Buying military-grade weapons for the police, who routinely kill people, is violently unjust when children don’t have toilets at school;
Revise the equitable share formula to allocate budget equitably and progressively across provinces, redressing long-standing inequities: the current formula, which only considers the number of learners in each province, doesn’t consider that education is more expensive to provide in the poorest provinces because larger distances and lower population densities increase costs;
To pressure other organs of state, such as SARS, to crack down on illicit financial outflows and tax evasion in order to improve public finances; and
To pressure other organs of state to revise tax laws to incorporate a wealth tax and strengthen a progressive income tax which better targets the upper bracket of earners.
We demand that government recognise that school spending is an investment in our people and our future, a public good, not a “cost” to be reduced no matter the consequences.
School choice
The national Department of Basic Education has a duty to:
Publicly acknowledge that policy enabled the creation of no-fee public schools, fee-paying public schools and private schools. This allows the middle class and rich to opt out of true public schooling and capture a disproportionate share of education spending. It must work with the public to develop a plan to reintegrate these schools back into a tuition-free public sector, in the same way that the Department of Health is working with the public to develop a National Health Insurance scheme to create a unified people’s health service. In the interim, it must place an absolute cap on school fees in public and private schools; and
Publicly consider how the policy of allowing teachers and learners to choose which schools to attend has fostered race and class segregation. The department must work with the public to demarketise schooling and implement the recommendations of the Hunter Report, which it ignored during the transition to democracy.
Decentralisation
The national Department of Basic Education has a duty to:
Publicly recognise that the creation of provinces was a key concession in the Codesa negotiations. The provinces have strong spatial and institutional overlaps with apartheid bureaucracies. This means that the anti-democratic ethos of apartheid institutions has manifested itself in many provinces – through white enclaves and ethnic provinces;
These provinces have a high level of autonomy over budgets and the hiring and firing of staff. It is difficult for either the national government or the public to hold them accountable. While recognising the entrenched political power of the provinces, the department must work with the public to address this fundamental driver of inequality; and
District and circuit structures need to be reorientated to serve schools by supporting teachers and learners, instead of imposing unrealistic plans on schools and pressuring them to comply.
Covid-19 has shown us how violently unequal our schools are. During the democratic transition, we had an opportunity to create a unified education system that serves all our children justly, freely and equally. We squandered that opportunity. Covid-19 has given us a precious second chance. For the sake of our children and those who have yet to come, we dare not squander it again.
Issued by the C19 People’s Coalition and its Education Working Group.
Signatories:
Adam Haupt – Centre for Film & Media Studies, UCT; Ally Cassiem, CALT, UJ; Anna James – ELRC, Rhodes University; Asanda Benya – Department of Sociology, UCT; Ashley Visagie – Bottomup; Aslam Fataar – Stellenbosch University; Azeem Badroodien – School of Education, UCT; Ben Verghese – UWC; Bonga Nzuza – Concerned Citizen; Britt Baatjes – Educationalist; Bruce Damons – Centre for the Community School, Nelson Mandela University; Carolyn McKinney – bua-lit Language and Literacy Collective; Clint Le Bruyns – Theology & Development Programme, UKZN, Underground Academy for Lifelong Learning; Dylan Valley – Centre for Film and Media Studies, UCT; Enver Motala – Centre for Education Rights and Transformation, University of Johannesburg; Fadia Gamieldien – Division of Occupational Therapy and CPMH, UCT; Fairuz Mullagee – UWC; Fathima Peerbhay -University of Western Cape; Fatima Gabru – Educator; Ganief Davids – Trustee Hidayatul Islam Primary School; Heila Lotz-Sisitka – Environmental Learning Research Centre, Rhodes University; Helene Rousseau – Bottomup; Ivor Baatjes – CIPSET, Nelson Mandela University; Jabu Bam – Centre for the Community School, Nelson Mandela University; Jane Keen – South African Education Project; Jane Quin – Education and Development, UKZN-P; Jon Fish Hodgson; Josh Miller – University of Cambridge; Kaathima Ebrahim; Kate Angier – School of Education, UCT; Kelly Gillespie – Department of Anthropology, UWC; Kharnita Mohamed – Department of Anthropology, UCT; Koni Benson – Department of History, University of the Western Cape; Kristen Abrahams – Division of Communication Sciences and Disorders, UCT; Leigh-Ann Naidoo – School of Education, UCT; Liz Blaiklock – concerned citizen; Lubna Nadvi – School of Social Sciences, UKZN; Lyndal Pottier – School of Education, UCT; Marcus Solomon – Children’s Resource Centre; Mejury Mushanguri – South African Education Project; Mellisa Francke – Division of Occupational Therapy, UCT; Mocke J van Veuren – University of the Witwatersrand (Film & TV); Moeneer Gamieldien – College of Cape Town; Mohamed Shahid Mathee – Religion Studies, UJ; Morné Steyn – Centre for Theatre, Dance and Performance Studies, UCT; Nadeema Musthan – Centre for the Community School, Nelson Mandela University; Najwa Norodien-Fataar – Cape Peninsula University of Technology; Nandi Msezane – Pan African Home Education Foundation; Natasha Vally – Department of Sociology, UCT; Nimi Hoffmann – Centre for International Education, University of Sussex; Polo Moji – Department of English Literature, UCT; Post School Education Alliance for Social Pedagogy; Pumeza Mahobe – South African Education Project; Rasigan Maharajh – Institute for Economic Research on Innovation, Tshwane University of Technology; Reza Khota – UWC; Robin Notshulwana – Nelson Mandela University; Roshan Galvaan – Division of Occupational Therapy, UCT; Rubina Setlhare – Educational Psychologist, UJ; Ruchi Chaturvedi – Department of Sociology, UCT; Saajidha Sader – School of Education, University of Kwazulu-Natal; Sadick Desai – eduACTION Community Education SA; Salim Vally – Centre for Education Rights and Transformation, University of Johannesburg; Sandra Jordaan – Department of Integrative Biomedical Sciences, UCT; Sara Black – Centre for Education Rights and Transformation, University of Johannesburg; Sarah Godsell – Social and Economic Sciences, Wits University; Sebolelo Mokapela – Department of Xhosa, UWC; Sinethemba Zungu – University of KwaZulu-Natal; Suren Pillay – UWC; Susan Gredley – University of the Western Cape; Susie Taylor-Alston – South African Education Project; Vanessa Japtha – Western Cape Forum for Intellectual Disability; Vanessa Pillay – Educator; and Xolisa Guzula – bua-lit Language and Literacy Collective.
Covid-19: The full economic impact will only be known later
- David Francis, Imraan Valodia and Kamal Ramburuth-Hurt
South Africa needs to focus urgently on how COVID-19 will reshape its labour market.
The full economic damage caused by COVID-19 and the lockdowns is uncertain. It will take several months, indeed years, to have a better understanding of where the damage has occurred and how severe it is. While the magnitudes are uncertain, it is already clear that we will see a sharp decline in incomes, rising unemployment, and widespread business closures.
South Africa, in particular, needs to keep a close eye on all aspects of the labour market so that policy responses can support those most in need. Recent work has highlighted the enormous impact of the COVID-19 pandemic and the lockdown on the lives of working people.
A focus on the labour market is particularly important given South Africa’s already high unemployment, and the inequality which is generated by the labour market. We highlight four areas of the labour market which will require scrutiny in the coming months: the informal economy; turbulence and job churn; increasing capital intensity; and gender and work.
Informal sector as a shock absorber?
Before the pandemic, South Africa had about 5 million people working in the informal economy. The orthodox view in development economics on the effect of economic crises is that informal employment acts as a shock absorber for the formal economy. When someone loses a formal job, they take up informal work. The argument is that there are no barriers to entry to informal work, so workers will simply move into this part of the economy and undertake some informal activity.
In South Africa, the evidence is that this is largely not the case. This is due to the very low absorption rate of labour of both the formal and informal sectors. Different to other developing countries, South Africa has both very high unemployment and relatively low informal employment. About 34% of workers in South Africa are informally employed, while the global average is more than 60%.
There is good reason to believe that the informal economy, rather than being a shock absorber, could well have proportionately larger employment losses in South Africa. For example, following the 2008 crisis, Professor Mike Rogan from Rhodes University found that both the formal and informal sectors contracted – the formal sector by 4%, the informal by 7%. This suggests that the informal economy does not necessarily absorb those who lose their formal jobs.
In the current crisis, this is exacerbated by the design of the lockdown and physical distancing protocols. These have had a particularly severe impact on the informal economy. Any economic policy responses must therefore take the informal economy into account, and provide support where possible.
Churn and capital intensification
The second area South Africa needs to focus on is which kind of jobs will be lost, who will be most affected, and where opportunities exist to create new employment. This requires looking deeper than the headline unemployment figures and into the nature of job changes. The economic shock from the pandemic and the lockdown will cause a reconfiguration in the labour market. Many people will lose jobs, but many will find new ones, too. This has been a common dynamic in labour markets since the industrial revolution. But the new jobs might pay less, or be more precarious, or more dangerous.
Given the structural nature of the shock, the changes to the labour market will not be random, and may affect certain groups more than others. Low to medium skilled workers are more likely to be employed in lower paying, more precarious forms of work. And there’s a concern that the sectors hardest hit will be those that employ a large proportion of women. Evidence from other countries suggests that, unlike in previous recessions where men lose proportionately more jobs, the current crisis is affecting women disproportionately.
The third important labour market issue to consider is capital intensity in the economy. In the production of goods and services, firms use a combination of labour, machinery and equipment (capital), land and entrepreneurship; the factors of production. The proportion of labour versus capital that firms in an economy use matters for job creation and unemployment. South Africa has seen a general trend toward capital intensive production. The country is likely to see an acceleration of this due to physical distancing requirements in offices and factories that will make automation more attractive for firms.
Physical capital, technology and labour can be combined in different proportions by a firm to increase or maintain the same amount of production. But in a country like South Africa, with very high unemployment, increasing capital intensity will further increase unemployment, and undermine the prospects of labour-intensive growth. This change will not be instantaneous. It’s more likely to unfold over the next months and years.
An increasing capital-to-labour ratio in production is an important consideration for two reasons. The first is its effect on unemployment. Secondly, a shift towards capital intensity will increase existing inequalities. One way this will occur is through the rising portion of value that is generated by capital that will be claimed by the relatively small number of owners of capital. This is a common driver of long-term inequality that persists if it is not countered by redistributive policies.
The fourth aspect is gender and work. Women in the South African labour market continue to suffer higher unemployment, lower wages, and more precarious working conditions. Indeed, women earn less than men, in general, even when they do the same job. In addition to the fact that evidence is pointing to the crisis affecting women disproportionately in the labour market, there is also uncertainty about how the lockdown has affected the distribution of unpaid work in the household – a burden which falls disproportionately and unfairly on women. It is critical that the country’s policy interventions are developed with these gender considerations in mind.
Need for new social compact
If the solidarity and social commitment to ending divisions in South African society is to be taken seriously beyond the pandemic, the manner in which these labour market trends will affect inequality must be considered. There is no natural mechanism or economic law that reduces inequality. Reducing it relies on policies of redistribution. This can happen either directly through structural changes leading to employment growth, higher wages or fiscally through taxation and expenditure. All of these require development policies that ensure the benefits of growth accrue disproportionately to low-income groups.
Given the conditions the world finds itself in, an increase in employment or wages is unlikely. In the case of South Africa, the country is also in a highly constrained fiscal position, which limits its ability to pursue redistributive policies.
In the medium to long term, South Africa will need a new social compact that ensures that the economic damage from COVID-19 is not borne disproportionately by the poor. Such a compact will have to address policies that raise the incomes of the poor – through the labour market and fiscal measures. South Africa needs to start an urgent conversation not only about the costs of COVID-19 but also about how the economy is likely to transform and who will benefit from that transformation.
SA needs to block transmission routes to get Covid-19 under control
- Alex van den Heever, Imraan Valodia, Lucy Allais, Martin Veller, Shabir Madhi and Willem Daniel Francois Venter
Testing and tracing has not been at a level needed to suppress the spread and must now focus on containing opportunities for super-spreading and transmissions.
As the lockdown is relaxed, South Africa’s focus should now be on how best to suppress the spread of the SARS-CoV-2 virus using other strategies. Policy should be informed by understanding the spread of the virus both in terms of the main mechanism of transmission (respiratory particles) as well as in terms of the connections that result in spread between communities. Crucially, not all spreaders are equal, and understanding this is important for policy.
South Africa introduced a lockdown early. It couldn’t afford, or adequately implement, a lockdown for long enough and effectively enough to contain the virus. Unfortunately, the country has also not been able to implement testing and tracing at a level needed to suppress the spread.
Nevertheless, the strategy did buy some time to prepare hospitals and the healthcare system. But if the country can’t contain the spread through lockdown or testing and tracing, this certainly does not mean that it should give up. Importantly, whether or not there is a lockdown, as long as people are conducting some economic activity, working in healthcare and other essential areas, and using transport to do so, there are routes of spread.
This means that, independent of lockdowns, the government needs to pay attention to limiting spread in these routes.
In this article we examine a way to think about successfully suppressing the epidemic with the tools that South Africa has available, by examining the main areas of transmission risk.
Features of SARS-CoV-2 transmission
Respiratory viruses spread rapidly as transmission occurs largely through the air. The reproduction rate (or R0) represents the average number of people an infected person will infect over a period of time. Importantly, the R0 figure is a crude average which in fact reflects a wide distribution of spreaders of the virus.
It turns out that much of the average is made up of a few super-spreading events and a majority of weak spreaders. Super-spreading can be tied to one-off events, such as a religious gathering, or a recurring high-risk setting – such as a call centre with many workers in an enclosed open plan setting. In the case of influenza, schools and universities are associated with super-spreading due to the frequent grouping of people into enclosed classrooms and canteens.
The importance of super-spreading events can be seen in the finding, in a still to be peer-reviewed article, that roughly 80% of COVID-19 infections are attributable to 20% of infected people. More interesting is a finding that roughly 70% of people with COVID-19 did not infect anyone else.
Understanding the importance of super-spreaders informs the potential effectiveness of physical distancing interventions – even in the absence of testing and tracing.
Social spaces that connect households
Given the way it spreads, the risk of exposure depends on:
In terms of transmission between groups it is worth differentiating between three levels of connection.
First there is the household level. Infected people within a household will tend to infect other family members living in close proximity.
Second, there are the social spaces that connect households within a community. A community refers to multiple households in close proximity to each other – such as in a district or town. Local shops, stores, local schools and restaurants create opportunities for transmission to occur between households within a community.
Third, there are the spaces that connect communities. These include places of employment, forms of bulk transport, major shopping centres, places of education, places of worship, theatres, healthcare providers, funeral gatherings, sports events, and any area where people from multiple communities are in close proximity.
The infectious disease spread between households and communities depends on two factors: first, the way in which the disease is transmitted between people; and second, the dynamics that connect people to each other. More distance naturally translates into no, or slower, transmission.
The distance is narrowed by social spaces that connect households and communities. Social spaces between households are responsible for transmission within a community. Social spaces between communities transmit an infectious disease between distant communities.
In theory, a strong generalised lockdown successfully implemented early enough could close both social spaces, restricting the further spread of the epidemic to that within the households. If these household members did not have contact with others, the disease would become extinct.
Where a generalised lockdown successfully closed the third-level social space, but left the second open, the spread would be affected by the number of communities with at least one household infected. In this scenario, the outbreak spreads through the connections between households within a community. However, the outbreaks would be quite localised. Communities with no infected households prior to the lockdown would not experience any outbreak.
Containment without preventive testing and tracing
Community-based testing and tracing can contain community-level outbreaks of COVID-19 relatively quickly – but only if the infection levels are relatively low and testing and tracing capabilities are highly responsive. This option has been taken off the table, given South Africa’s level of spread combined with insufficient rapid testing.
This means that the country’s strategy should focus on intensive management of the two levels of social space that connect households.
First, this means closing or heavily controlling the social spaces that provide opportunities for super-spreading and that are not essential for the economy and society. These include all large gatherings, such as funerals and church gatherings, particularly where these gatherings occur indoors in spaces with poor air circulation.
Second, it means the following general requirements for all spaces that are essential for the maintenance of the economy and society:
Masks to be worn by everyone.
Require physical distancing wherever possible. Staff who can work from home should be required to do so.
Introduce outside air into closed settings. Whenever people from different households are in a vehicle, open windows if possible.
Upgrade filters in air conditioning systems and only use air conditioning systems which extract rather than re-circulate air. Air flow from air conditioning systems and fans may also need to be modified.
Regularly clean high-contact surfaces.
Require that employers provide good quality protective equipment for staff in regular contact with clients.
Provide for on-site symptom screening for staff. Self-screening should also be enabled before coming to work. This should include a requirement to stay at home if any person in the household has symptoms and clear messaging about which symptoms these are.
Access to hand-washing facilities must be made available.
Where cases are detected at any social space, testing and contact-tracing can ensue (where resources allow), with the possibility of a temporary short-term closure where required to understand the outbreak.
This strategy requires clear, accurate public information messaging, co-operation from employers and employees, and buy-in from society.
Conclusion
These measures are unlikely to eliminate spread, but will contain opportunities for super-spreading and transmissions between communities and households.
South Africa has clearly struggled to manage the social spaces within and between high-density communities using a lockdown approach. Redirecting efforts to managing the high-risk social spaces between communities and households may go a long way towards lowering the maximum infection peaks and reducing the risk to society.
If infection levels decline sufficiently, current capabilities for testing and tracing could be sufficient for their strategic redirection toward prevention – particularly if all testing capabilities in government, universities and the private sector were mobilised as part of a single strategy.
The first Covid-19 vaccine trial in South Africa begins
- Wits University
The first participants in South Africa's first clinical trial for a vaccine against Covid-19 will be vaccinated this week.
The first clinical trial in South Africa and on the continent for a Covid-19 vaccine was announced today, 23 June 2020, at a virtual press conference hosted by the University of the Witwatersrand, Johannesburg (Wits).
To watch the full Zoom recording of the press conference, click here and enter the password: 5n?p3Z*?
In South Africa, at least 80,000 people have already been diagnosed with Covid-19 and more than 1,674 have died from Covid-19 since March, when the President declared a state of disaster and national lockdown.
By 17 June 2020, South Africa (population: 59 million) contributed to 30% of all diagnosed Covid-19 cases and 23% of all Covid-19 deaths on the African continent (population: 1.34 billion). These statistics emphasise the urgent need for prevention of Covid-19 on the continent.
Shabir Madhi, Professor of Vaccinology at Wits University and Director of the South Africa Medical Research Council (SAMRC) Vaccines and Infectious Diseases Analytics Research Unit (VIDA), leads the South African Ox1Cov-19 Vaccine VIDA-Trial.
Wits University is collaborating with the University of Oxford and the Oxford Jenner Institute on the South African trial.
“This is a landmark moment for South Africa and Africa at this stage of the Covid-19 pandemic. As we enter winter in South Africa and pressure increases on public hospitals, now more than ever we need a vaccine to prevent infection by Covid-19,” said Madhi at the launch of the South African Ox1Cov-19 Vaccine VIDA-Trial, which is being run at multiple sites in South Africa.
“We began screening participants for the South African Oxford 1 Covid-19 vaccine trial last week and the first participants will be vaccinated this week,” says Madhi, who is also the National Research Foundation/Department of Science and Innovation SARChI (South African Research Chairs Initiative) Chair in Vaccine Preventable Diseases, based at the University of the Witwatersrand.
Professor Zeblon Vilakazi, Vice Principal and Deputy Vice Chancellor: Research and Postgraduate Affairs at the Wits University, who facilitated the virtual press conference, said: “Wits University identified vaccinology as a key institutional flagship project in 2016. Vaccines are amongst the most powerful tools to mitigate life-threatening diseases. Without a vaccine against Covid-19, there will likely be ongoing contagion, causing severe illness and death. Wits is committed to developing a vaccine to save lives in collaboration with the University of Oxford.”
Prior to launch, the South African study was subject to rigorous review and has been approved by the South African Health Products Regulatory Authority (SAHPRA) and the Human Research Ethics Committee of the University of the Witwatersrand.
Furthermore, after eliciting and considering public comment, the Department of Agriculture, Forestry and Fisheries (DAFF) approved import of the investigational vaccine for use in the trial.
South African participation in international trials
The vaccine is already being evaluated in a large clinical trial in the UK where more than 4,000 participants have already been enrolled. In addition to the South African study, similar and related studies are about to start in Brazil. An even larger study of the same vaccine of up to 30,000 participants is planned in the USA.
“It is essential that vaccine studies are performed in southern hemisphere countries, including in the African region, concurrently with studies in northern hemisphere countries,” says Professor Helen Rees, Chair of SAHPRA and Executive Director of the Wits Reproductive Health and HIV Institute (Wits RHI).
“This allows evaluation of the efficacy and safety of candidate vaccines to be assessed in a global context, failing which the introduction of many life-saving vaccines into public immunization programmes for low-middle income countries frequently lags behind those in high-income countries.”
Rees also co-directs the Wits African Leadership in Vaccinology Excellence (ALIVE) flagship programme and is engaged in global discussions with Gavi, the Vaccine Alliance and the World Health Organization to ensure equitable access for all countries, including those in Africa, should a successful vaccine be developed.
About the South African vaccine on trial
The technical name of the vaccine is ChAdOx1 nCoV-19, as it is made from a virus called ChAdOx1, which is a weakened and non-replicating version of a common cold virus (adenovirus). The vaccine has been engineered to express the SARS-CoV-2 spike protein.
The vaccine was developed at the Oxford Jenner Institute and is currently on trial in the UK, where over 4,000 participants are already enrolled into the clinical trial and enrolment of an additional 10, 000 participants is planned.
The vaccine being used in the South African trial is the same as that being used in the UK and Brazil.
The vaccine was made by adding genetic material – called spike glycoprotein – that is expressed on the surface of SARS-CoV-2 to the ChAdOx1 virus.
This spike glycoprotein is usually found on the surface of the novel coronavirus and is what gives the coronavirus its distinct spiky appearance.
These spikes play an essential role in laying a path for infection by the coronavirus. The virus that causes Covid-19 uses this spike protein to bind to ACE2 receptors on human cells.
ACE2 is a protein on the surface of many cell types. It is an enzyme that generates small proteins that then go on to regulate functions in the cell. In this way, the virus gains entry to the cells in the human body and causes Covid-19 infection.
Researchers have shown that antibodies produced against sections of the spike protein after natural infection are able to neutralize (kill) the virus when tested in the laboratory.
By vaccinating volunteers with ChAdOx1 nCoV-19, scientists hope to make the human body recognise and develop an immune response (i.e., develop antibodies) to the spike glycoprotein that will help stop the SARS-CoV-2 virus from entering human cells and causing Covid-19.
Local application of a global response
In addition to the more than 4,000 people already vaccinated in the UK with the ChAdOx1 nCoV-19 vaccine, other vaccines made from the ChAdOx1 virus have also been given to more than 320 people to date. These vaccines have been shown to be safe and well-tolerated, although they can cause temporary side effects, such as a temperature, headache or a sore arm.
There are currently over 100 candidate Covid vaccines in development around the world and many of South Africa’s best vaccine research institutions will soon be involved in a range of vaccine studies evaluating other types of potential Covid vaccines.
“As the world rallies to find health solutions, a South African endeavour for the development of an effective Covid-19 vaccine is testament to our commitment of supporting healthcare innovation to save lives,” says Professor Glenda Gray, President and CEO of the South African Medical Research Council.
Dr Sandile Buthelezi, the Director General of Health in the National Department of Health, said: “The National Department of Health is excited at the launch of this vaccine trial, which will go a long way to cement South Africa's leadership in the scientific space. With Covid-19 infections increasing every day, the development of the vaccine will be the last solution in the long term, and we are fully behind the team leading this trial.”
Distance, Dose, Dispersion: Experts’ guide on Covid-19 risks in South Africa and how to manage them
- Lucy Allais, Shaheen Mehtar, Francois Venter, David Francis, Shabir Madhi, Alex van den Heever, Imraan Valodia and Martin Veller
Understand the three things that can make the most difference to easing the lockdown and reopening South Africa with the least risk.
Our lives have been turned upside down by the coronavirus pandemic and by the lockdown, and further confused by shifting information. You might be wondering about the role of masks, whether to wipe down your groceries, and if the lifting of lockdown means we can all relax now. You might have concerns about how you can safely travel to work, what steps to take as you reopen your business, whether to attend a religious gathering, or what to tell your grandmother about how to stay safe.
It has become clear that some countries in Asia and Europe rapidly contained their epidemics through simple and relatively easy behaviour changes, rather than relying on changes in immunity or prolonged lockdown strategies. Our aim here is to share some basic essentials about how to minimise risk. Nothing is risk-free (for example, we take risks getting into cars, buses or taxis). But we can manage risks, which requires understanding how they intersect and amplify each other. It turns out that with this new coronavirus, open windows, masks and physical distancing are more important than obsessive hand sanitising and temperature taking.
Understand that we may be in for a long haul, adjusting our lives for at least the next few years. Some of these changes may be permanent (and may be things we should have done anyway, for TB and seasonal ‘flu). We need to enable businesses to survive, our institutions to open as safely as possible, while we live our lives as naturally social animals.
We cannot be saved by government policy alone – the things we can all do are what will save South African lives. And those things are pretty simple.
Our Summary:
Do everything possibleOutdoors;
Open Windows;
wearMasks;
keep at least one metreDistance(two metres is better) from people,
Avoid Crowdedspaces,
beQuick.
What causes the problem?
The way the virus spreads is that when we cough, sneeze, talk, sing or simply breathe, we spray very small drops of moisture into the air; these are respiratory particles. If someone is infected, the live virus will be present in these particles. These particles in our breath can spray quite far (several metres). If there is poor ventilation and no air movement, they can hang around in the air. They can land on surfaces (where the virus may survive for some hours) and if you are close to someone they can land on your eyes, nose or mouth. Most people who become infected get the coronavirus by direct contact with an infected person. It is also possible, but less common, to be infected from touching your mouth, nose or eyes when your hands have the virus on them from touching a surface.
What is the impact of the three Ds?
Distance:The further away you are from someone who is infected, the less likely you are to be infected by them or to breathe in particles they have breathed out.
Dose:To become infectedyou need to have contact with a minimum dose, which takes time and exposure to people with the virus.Thelongeryou are exposed to an infectious person, themore peopleyou are exposed to, and thefewer barriers(like cloth masks) between you, the more likely you are to be exposed to the virus. People who have symptoms or are about to develop symptoms, including mild illness, are generally more infectious – i.e., are able to produce larger doses of infected respiratory particles.
Dispersion:Because smaller particles hang around in the air, themovementof air makes a really big difference. The particles disperse quickly if you are outside, particularly if there is a breeze or wind. We also know that sunlight breaks down the virus. Small, enclosed spaces with closed windows are high risk, especially when they are crowded.
The three Ds interact! If you are outdoors, at least one metre (but preferably two metres) apart from others, for less than 10 minutes, your risk of becoming infected is incredibly low. On the other hand, if you are stuck in a room with closed windows, with someone with symptoms, your risk of getting the disease increases, whether or not you wear a cloth mask. Large known outbreaks have arisen in indoor functions in churches, weddings, music events, and restaurants or bars: places where a crowd of people are indoors, close together and talking and singing for hours.
Businesses, factories, workers and families urgently need to pay attention to the interaction of the three Ds. Physical distancing is very effective when outdoors or for short encounters (10 minutes); once you are in a closed space, its effectiveness dramatically diminishes.Masks and two metres distance are not enough if you are with people in an unventilated space all day.Evaluate your office, place of worship, business, planned funeral or other event in terms of the intersection of the three Ds.
What can we do?
Physical distance:This is your major defence from infection. The good news is that although the virus spreads easily, short periods of contact will not get you infected. Passing someone in a supermarket, paying for your groceries, brushing past a runner in a park is no problem. But sitting in a taxi with closed windows, being alongside a sick co-worker at a work station, or singing in a packed church, is.
Go for outdoors and open all windows:Outside air is your best friend, and we may all have to start dressing more warmly in winter as many activities move outdoors and windows stay open.Open windows whenever possible on public transport, in shops or at work.Unfortunately, the interaction of the three Ds means that taxi rides of more than 15 minutes are risky, even if everyone is wearing a mask –unless the windows are open.
Businesses, factories, offices – look at your windows and work out how to get air flow. Open all windows and utilise outside space. Restaurants, bars and shebeens should consider outdoor seating wherever possible. Streets with a number of restaurants should inquire into closing the street a few evenings a week, or every day, and putting tables and chairs outside.
Socialise outside if you can, keeping a two-metre distance. An outside braai or picnic is much safer than visiting someone in their house. Avoid visiting people or being visited inside homes for more than a few minutes. Have work meetings outdoors, if possible. If you want to have a gathering, such as a religious gathering or funeral, do it outside if you can. An outside shebeen, with physical distancing, is far safer than an indoor shebeen with masks and obsessive hand washing. Outdoor sport is very low risk, unless involving close prolonged contact. (Even outdoors, don’t talk to someone up close for long; maintain distance.)
Wear masks:There is now lots of evidence on the effectiveness of wearing cloth masks in the community. A cloth mask traps the virus-containing respiratory particles during breathing, coughing or talking, and helps prevent them from moving away from the mask-wearer. (But why has mask advice changed? *See our comment at the end.) People who have very mild symptoms or are about to develop symptoms can spread the virus – this means that each of us might spread the virus unknowingly. If everyone wears a mask the amount of virus in the air is much reduced: we all protect each other. Therefore youshould always wear a mask whenever you are close to people other than those in your household, especially indoors. It is also vital that you wear your mask correctly – it must cover from the bridge of your nose to over your chin at all times. Wash your mask daily with soap or detergent.
Offices, factories, banks, shops, malls, government services – any indoor space where people come into contact – must require everyone to wear masks. Employers should distribute reusable cloth masks to employees. Reusable cloth masks should be distributed in communities where people can’t afford them.
As important as masks are, in an indoor space they are not a substitute for ventilation and distancing – you need all three.
Work in homes:If you work in someone’s home (domestic workers, plumbers, etc) or someone comes in to work in your home, insist on windows being open and don’t be in rooms at the same time as them for long. Wear a cloth mask, carry and use your own hand sanitiser, and keep your distance.
Soap and surfaces:The virus is incredibly fragile, and washing your hands with any soap for 20 seconds kills the virus. Make soap and water (or hand sanitisers with an alcohol solution of at least 70 percent) as widely available as possible at workplaces, malls, shops, transport and offices. Soap works much better than alcohol-based sanitiser, is cheaper, and will result in less cracked hands. Invest in mobile handwashing stations in areas with a high concentration of people, like hospitals and clinics.
It is unclear how likely you are to contract the virus from surfaces, but it is wise to clean commonly touched workspaces and public areas often. Minimise touching and wipe down frequently touched surfaces – like door handles, lift buttons, railings, credit card machines. The virus dies quickly on surfaces; in laboratories it has been found in low doses beyond 24 hours on plastic and steel (but not on porous surfaces such as park benches, or grass). Whether this is enough virus to infect you is unknown, but surface transmission is very unlikely to be the major way you will be infected. Washing your clothes after going out, or washing your car, and wiping all your groceries is not necessary; just wash your hands and keep surfaces around you clean and dry.
If there is an outbreak in a venue, or an employee tests positive, wiping surfaces down with soap and water, followed by bleach, or other common disinfectants, is very effective in removing any viral particles that may still be present. And if you can leave the venue open and ventilated for 24 hours, this should be enough. There is no need for special chemicals, or “deep cleansing” or “fogging” or “disinfection tunnels”; they are no more effective than soap and water, and are associated with other health risks, including making asthma, eye and skin conditions worse. There is no need to shut down a facility for days; once surfaces have been cleaned, dried and disinfected, and spaces ventilated, work can continue.
Gloves are unnecessary for most people: you still need to wash them so you may as well just wash your hands. The one exception may be someone who handles lots of items – like a dishwasher or a cashier, where exposure may be higher (and they must wash their hands after taking the gloves off).
Air-conditioning:Employers, businesses, restaurants, offices: understand your air-conditioning system. A system that recirculates air is very risky, and has been linked to several call centre and restaurant outbreaks. You are essentially guaranteeing that everyone breathes everyone else’s air. On the other hand, an air-conditioning system that extracts air and brings in air from outside makes an indoor space safer. But simply opening windows, where possible, especially if combined with use of a fan, may be more effective if it increases the movement of air. If well ventilated, a room can be safe in minutes, even if someone is coughing and highly infectious.
Hours:All shops and businesses that can extend opening hours to reduce crowding should do so. Limit the number of people in shops. Lines on the floor to signal distancing requirements have been very successful. Consider discounts for coming in at unpopular hours. All shops should consider having a pensioner-only (or also people with a health-risk note) hour at the beginning of the day. Older people, and people with diabetes, hypertension, HIV, cancer and obesity may be more at risk (we are still learning about the extent of risk), and enabling them to shop when it is least crowded, and when other people have not yet been into the shop, helps protect them. Consider leaving hotel rooms empty and ventilated for a day after someone leaves, and ask guests to open the windows when they leave, to protect cleaning staff. Factories, mines, offices and other workplaces should consider staggering work hours or days so that not every employee comes in at the same time or on the same day. Take turns in lifts (and always wear cloth masks). Tea and break rooms must be well ventilated and break times staggered to reduce crowding.
Family:We are social creatures; we need human contact. Many extended families have regular get-togethers. Unfortunately, if you are indoors with people who don’t live in the same home, you are seriously increasing the risk of spread to your family. Even if you know who each person has been in contact with in the past two weeks (and you may not), one person who was exposed in a shop or transport or work, who is not yet showing symptoms, can expose a whole extended family, who can then expose everyone they work with. A high percentage of people are infected in their own homes and take the virus to work. In China, many infections occurred in the home, so homes with vulnerable members in them should consider wearing masks at home. Meet outdoors wherever possible.
We know that children are much less likely to be infected with the virus and even when infected have no or mild symptoms. Going to school is unlikely to be dangerous for them (though schools have to think about protecting teachers). Children are probably also less likely to pass it on others. But, sadly, you still may want to hold off from children hugging vulnerable grandparents for a while. One of the hardest parts of the lockdown has been stopping children from playing together. There is no easy answer here. From current knowledge it seems that there is likely to be some risk, and children’s behaviour when they are together is a challenge to all three Ds. If children play together, encourage outdoors, masks or face shields and lots of handwashing (before, during and after). Consider who they come into contact with at home (an elderly grandparent, someone with diabetes) when deciding about play arrangements. Perhaps discourage hugging and kissing.
Personal risk factors:People of all ages and levels of health have become very ill and have died of Covid-19. But we know that some people are at much higher risk than others. The most significant risk factors for being badly affected are older age (especially over 65), diabetes, hypertension, HIV, uncontrolled asthma and obesity. If you or your family member has one of these factors, consider getting someone less vulnerable to do the shopping, consider going to shops at opening time, before anyone else has been in them. Vulnerable people should avoid taxis, trains, buses and gatherings if they can.
Protect others:Stay home if you have any of these symptoms: a fever, a cough, body aches, difficulty breathing, loss of sense of smell or taste. Encourage workers to stay home if they have these symptoms. When you are not at home, wear a cloth mask to protect others, especially indoors. Wearing a cloth mask protects other people – and they protect you.
When should you test?Getting a PCR test for coronavirus is less useful than many people think. A test that comes back negative doesnotmean you don’t have the virus; it has a very high “false-negative” rate – almost a third of tests. Unless you need hospital care (in which case you will be tested), the test won’t affect how you look after yourself, and if you have symptoms you should isolate anyway as you may be infected.
How should you isolate?If you have symptoms or have been in close contact with someone who has tested positive, try to self-quarantine. Once you understand the three Ds, self-quarantining is not difficult to understand. If living with people, try to spend time in a room on your own or spend time outdoors. Try to avoid communal spaces wherever possible; when you can’t avoid using these (the kitchen or bathroom), try to spend as little time as possible, wipe surfaces, wear cloth masks, and open windows.
Public toilets:There is some evidence that flushing a toilet sprays particles in the air which can have the virus in them. Tell customers, employees, and passengers on planes to put toilet seats down before flushing. Consider adding signs in all public restrooms with this message.
What about thermometers?Thermometers, especially the “point at your forehead” or oral ones, are actually very poor at telling your temperature, and may falsely create the impression that an infected person is not infectious. At a business or venue entrance they require close contact with the person with the thermometer. A person who has a fever from Covid-19 is likely to have other symptoms, so a simple symptom check is all you need.
Can you fly?Planes have very good air-circulation systems with particle filters that remove the virus from the air, which means that they are very low risk during the flight. But be careful of surfaces, and on short trips avoid the toilet if you can. You are far more likely to contract the virus in the airport while queuing, or waiting in a lounge or restaurant, than on the plane.
Communicate:Have clear communication about how to manage risk at work. Managers and policy advisers should realise that although policies need to be clear and not too complicated, at the same time advice that is nuanced but actually doable has better results than advice that is very simple but unrealistic in practice. Compare telling people they can prevent HIV bynever having sexrather than by giving information about safe sex practices. The former is simpler but does not result in HIV prevention; it may be true but it doesn’t help because it is not realistic. Businesses should anticipate they might have to shut down for a day and openly communicate.
No shaming:Don’t judge or stigmatise people with Covid-19. Getting infected does not mean they were careless or have bad hygiene. Anyone can get infected, millions of people worldwide have been, and in South Africa, for every case diagnosed there are likely to be 10 others who have it but have not been tested, and may not have symptoms; it may be you. A workplace may have an outbreak despite taking all necessary measures. There is no need to shout at people exercising outdoors without a mask but at a distance, or in the park with their family; they are not going to infect you. Be kind.
Take it seriously: Covid-19 is real!If we all act together and help each other, we can dramatically limit spread, reduce deaths and protect our hospitals. Remember that anyone can get Covid-19 and become very sick. Those who were seriously ill can take a long time to fully recover. Even if you are not high-risk for severe illness, your actions create risks for others. Covid-19 is spreading rapidly in South Africa and this is the time for more, not less, vigilance.
This is in our hands:Covid-19 is here to stay for a while and is rapidly spreading; but we need to live, to see each other and to work. South Africa had an early and strict lockdown, but we always knew we couldn’t do this for long. The easing of the lockdown does not mean the threat of infection has decreased. In fact, the opposite is true. We must not give up on containing spread: there is a lot practically that we as individuals, commuters, workers, managers and trades unions can do to protect ourselves and each other as South Africa reopens.
Why has information on masks changed?Early on we were advised not to wear masks, now we’re told everyone should wear masks – what gives? Three things. First, as this new pandemic hit, there was a worldwide shortage of masks that healthcare and other emergency workers needed. It was more important for them than for the rest of us to get the masks, as they are more exposed, and also expose more people. Second, we were told initially that masks are more important for sick people than for protecting those not infected. This hasn’t changed, but what has changed is understanding how much spread could be caused by people who have mild symptoms or do not yet have symptoms. This means that everyone is potentially a sick person who is spreading, and if we all wear masks we limit spread. Third, the world is learning fast about this new disease: more information is emerging all the time about how much of an impact universal mask-wearing can have on reducing spread.
Lucy Allais is Professor of Philosophy, University of the Witwatersrand and UCSD, Director, Wits Centre for Ethics. Shaheen Mehtar, Professor of Infection control, Stellenbosch university. Willem Daniel Francois Venter, Ezintsha, Faculty of Health Sciences, University of the Witwatersrand, University of the Witwatersrand. David Francis, Deputy Director, Southern Centre for Inequality Studies, University of the Witwatersrand. Shabir Madhi, incoming Dean of the Faculty of Health Sciences, Professor of Vaccinology and Director of the MRC Respiratory and Meningeal Pathogens Research Unit, University of the Witwatersrand. Alex van den Heever, Chair of Social Security Systems Administration and Management Studies, Adjunct Professor in the School of Governance, University of the Witwatersrand. Imraan Valodia, Dean of the Faculty of Commerce, Law and Management, and Head of the Southern Centre for Inequality Studies, University of the Witwatersrand. Martin Veller, outgoing Dean of the Faculty of Health Sciences, Professor of Surgery, University of the Witwatersrand.
This piece has been produced by an interdisciplinary group of academics working on Covid-19 and responses to it. The technical input is provided by members with medical expertise and has also been fact-checked by a number of other medical professionals, in accordance with the latest science.
SA's budget for COVID-19 fails to pave way for more equal society
- David Francis and Imraan Valodia
The budget is one of the key tools that government has to effect meaningful change.
The COVID-19 pandemic has not only generated a far-reaching social and economic crisis in South Africa, but is also exposing two major fault lines in the society.
First, the pandemic has starkly exposed the country’s high levels of inequality. Every way in which South Africa is unequal has been exacerbated by the pandemic. Those with high-paying office jobs have largely been able to work and earn an income from their homes. Those in low-paying, precarious work have lost their jobs and income, or have been forced out to work. These same workers have to risk infection on public transport and in crowded shops. Children at private schools continue learning online, while the vast majority of learners in the public system have not had any schooling for almost three months.
Second, the pandemic has exposed the deep gender inequalities in the country. Not only has South Africa continued to experience the most abhorrent forms of gender-based violence under the lockdown, but the pandemic has also exposed the deep gender-based inequality in both paid and unpaid work. Women are having to bear a disproportionate responsibility for unpaid care work, while at the same time bearing a heavy burden for job and income losses in both the formal and informal economies.
Any economic policy proposals from government would have to address these inequalities if the country were to emerge from the pandemic with a more equal and fair society, and a more resilient economy. The budget is one of the key tools that government has to effect meaningful change, though it can’t address all these problems on its own. Of course, the rebuilding is a long-term process, but the budget is a key starting point.
In many of its pronouncements on managing the economic fallout from the pandemic, the government has emphasised its intention to forge a new economic growth path that would address the high levels of inequality in South Africa. Indeed, in a recent speech President Cyril Ramaphosa outlined his vision for a new economy thus:
We must transform and restructure. We are operating under an economy both colonial and racist. We need a reset of the economy for inclusive growth. We need an economy that responds to poverty. We can’t countenance 10 million people out of work.
How does the supplementary budget announced by Finance Minister Tito Mboweni move South Africa towards this objective? And what can be learnt from the budget about government’s plans to seriously work towards such a new economy?
To be fair, it is not the sole job of the finance minister to address inequality. However, the budget of the government, which is his responsibility, should provide a strategic financial framework for prioritising the key objectives of government. Sadly, we are of the view that there is very little in the budget he set out this week that creates a pathway to a better, more equal economy.
Balancing competing imperatives
We don’t deny that the financial and fiscal challenges which face South Africa are immense. There are no simple solutions. However, the budget needs to balance competing and sometimes incompatible imperatives:
spending which protects and assists the poor and vulnerable;
financial management which allows the country to raise debt affordably and repay it sustainably; and
spending which promotes equitable growth.
In addition, the budget should indicate how the fiscal consolidation plan will address the major inequalities in the country. It should also show how the adjustment will affect the country’s ability to address key social and economic challenges, in both the short and the long term.
First, the narrower measure of the budget deficit for 2020/21 has, as a result of COVID-19, shifted from 6.8% of the gross domestic product (GDP) to 14.6% of GDP. Government had, in the original 2020/21 budget, projected its revenue for the fiscal year to be R1.398 trillion. As a result of the shutdown and lower economic growth, government now expects revenue to be R1.099 trillion – a shortfall of almost R300 billion. Expenditure, on the other hand, which was initially projected at R1.766 trillion, is now projected to be R1.809 trillion – an increase of about R44 billion. The net result is that the deficit, originally expected to be R368 billion, is now estimated to be R709 billion.
Second, within the current fiscal year, government has cut R101 billion from various budget lines, and reallocated R145 billion worth of expenditure for COVID-19 measures – hence the R44 billion of net additional expenditure.
Third and most strikingly, government plans to have a primary budget surplus (that is, the difference between revenue and expenditure before debt payments) by 2023/24, in order to deal with its growing debt.
This raises two important questions. The first is why it is necessary at all to have a primary surplus in the budget. An obsession with balanced budgets dates back to the Thatcher/Reagan era of the 1980s. But there are many compelling arguments for why it is not necessary for a government ever to run a balanced budget. The austerity measures required to balance a budget can inflict permanent economic damage on the poorest and most vulnerable citizens, and deepen inequality.
Second, how will this surplus will be achieved, and at what cost, to whom? The indications are that the budget will be balanced through significant cuts in expenditure (rather than rapid revenue growth), projected at R230 billion in 2021/22 and 2022/23, and even further in 2023/24. Unfortunately, we are not provided with details on where these cuts in expenditure will occur. But there is little doubt that they will disproportionately affect those dependent on state services.
There is little in the 2020 adjustment budget to suggest that the government is serious about building a fairer economy which addresses the already high levels of inequality. Essentially, we have been told to wait until the October mid-term budget, and the 2021 annual budget, to see the detail about how the government will achieve its goals.
The fallout
On the basis of what has been said (and not said) in the supplementary budget, we can expect inequality to rise significantly. Government expenditure is progressive and significantly reduces the levels of inequality in our society. Cutting expenditure at the magnitude planned will certainly lead to higher levels of inequality. Moreover, because of the nature of social spending, the impact of spending cuts will fall disproportionately on women.
There are two very worrying aspects of the desire to run a budget surplus. The first is that spending cuts required to achieve it are extreme, and contrary to the expansionary fiscal policy being adopted by many countries around the world. The second is that there is little information in the adjustment budget about who will bear the brunt of these cuts. This matters for inequality.
If government is serious about addressing inequality and building a less unequal economy, what should the budget do? Inequality cannot be addressed without an active economic strategy that:
There is, unfortunately, very little in this supplementary budget to suggest that government has an economic strategy to lower inequality in South Africa.
More money for COVID-19 but SA lacks a spending strategy
- Alex van den Heever
South Africa's public health system has been allocated R21.5 billion more to fight the Covid-19 pandemic but there's no strategy to guide how it should be used.
The supplementary budget tabled last week by South Africa’s finance minister, Tito Mboweni, whose primary objective was to make more money available for the fight against the COVID-19 pandemic, sheds no light on the relative prioritisation of prevention over treatment for COVID-19.
The required health system response to COVID 19 broadly falls into these two areas: prevention and treatment. The two are closely interlinked. And there are severe shortcomings in both.
On the prevention side, interventions include social distancing as well as rapid testing, contact tracing and quarantining. These require massive upscaling to have a preventive effect.
Prevention also involves public health interventions separating infected from uninfected people.
For its part, treatment requires that health services address the needs of COVID-19 patients while at the same time protecting health service workers and non-COVID-19 patients from undiagnosed patients presenting for non-COVID conditions.
But for this to happen there has to be rapid turnaround of test results. In the absence of this, all patients awaiting results need to be treated as potentially COVID positive. This, in turn, requires staff to have full personal protective equipment when treating all patients. But public sector facilities aren’t able to reliably provide personal protective equipment.
COVID-19 patients also need expensive hospital-based care together with oxygen, ventilators (when oxygen proves insufficient on its own) as well as a variety of medications. Using private sector inpatient data from the Hospital Association of South Africa, the distribution is: general ward (64.2%), high care (15.7%) and intensive care units (20%).
The supplementary budget announced by the minister of finance makes provision for an additional R21.5 billion for health to be split between the provinces, which will get most, and the national department of health. The problem is that, though money has been made available, there’s no associated strategy that sets out how it will be spent. This is a major omission that suggests the funds will not have any meaningful impact.
Missing strategies
The number of cases has been rising steadily in South Africa since around 22 April 2020. The lockdown was implemented on 27 March 2020 to stop the epidemic until such time as alternative prevention strategies could be put in place and to ready health services. Neither objective was achieved. Not only did the lockdown not stop new infections, as has been achieved elsewhere, but testing and tracing at scale was not implemented by the end of April as promised, and health services are in no position to cope with an uncontained outbreak.
During April, May and early June 2020 the Western Cape experienced increasing new cases relative to all the other provinces. During the course of June the outbreak appears to have peaked due to interventions targeted at hotspots (Figure 1).
Over the same period the Eastern Cape and Gauteng provinces have seen a spike in new infections (Figure 1). Inpatient numbers and expected deaths have not yet caught up with these steep increases. But the impact on services is likely to rise steeply.
Gauteng is fairly well-resourced in critical care beds (2,690 with only 819 in the public sector), when both the public and private sectors are aggregated. But the Eastern Cape is far behind (400, with only 241 in the public sector) (Table 1).
Source: Daily data provided by the National Institute of Communicable Diseases (NICD)
Given what lies ahead, how will the supplementary budget help?
Of the additional R21.5 billion made available for health, R16 billion will be transferred to provinces as an adjustment to the provincial equitable share allocation (formula-based and allocated at the discretion of the province). The remaining R5.544 billion is allocated to the National Department of Health.
The biggest problem is that these allocations are not connected to any strategy. The budget documents state broadly that the funds are meant to support testing, community health workers, expanding hospital capacity for critical care and field hospitals, PPE, oxygen, ventilators and new staff.
A number of immediate concerns therefore arise.
First, the R16 billion is a general augmentation of provincial health budgets. It gives no consideration to differences in the provincial COVID-19 disease trajectory or likely impacts on services.
Second, it is unclear how testing and tracing infrastructure is to be expanded. For example, does it include funding university and private sector laboratories?
Third, no clarity is provided on how the R5.544 billion is to be spent by national government.
What this means is that funding is likely to be allocated inefficiently. Some provinces won’t get what they need while others will waste allocations on less important functions. Because the funds aren’t earmarked, provinces can also choose not to allocate them for COVID-19 health interventions.
Another major gap is that the budget doesn’t offer any strategy or strategic targets when it comes to testing. Provincial governments will have to fund testing out of their existing budgets for the remainder of the year. This could, based on my own estimates, range from R3 billion (15,000 tests per day) to R8 billion (40,000 tests per day).
Provinces also need to fund quarantine sites and additional hospital beds. No strategy on either is outlined.
Overflow requirements for beds in the private sector are priced at R16,000 per day for critical care. Given that an overflow requirement introduces a demand-driven element into the budget process, significant contingent fiscal risks arise.
Again, however, no strategy is outlined.
South Africa only has critical care bed capacity for the remainder of the financial year of around 468,433 bed days (account has been taken of existing occupancy), of which 90,400 bed days (16.3%) are in the public sector. However, if the epidemic trajectory continues as at present, COVID-specific critical care bed need may be as high as 2.9 million bed days over the period July to December 2020.
As this would exceed both the financial and human resources of both the public and private systems, prevention strategies would need to be substantially more effective than at present.
It would therefore have made more sense to clarify the strategy. This would logically require flexibility in the budget process to enable prioritisation between prevention strategies and differential provincial treatment needs.
The increase in the equitable share allocation by R16 billion has, however, removed any flexibility for national government to shift funds to the highest strategic priorities by province. The remaining national allocations appear insufficient to fine tune prevention strategies or to augment provinces in greater relative need for hospital beds.
Source: Compiled by the author from various sources including the Department of Health and the Hospital Association of South Africa.
Now what?
The relative prioritisation of prevention over treatment for COVID-19 is neither explicit in government’s COVID-19 strategy documents, nor determinable from resource allocations in the supplementary budget. While this distinction may appear unimportant, disease prevention can only succeed if resourced at sufficient scale to avoid the catastrophic demand for critical care services for which no preparation will be sufficient.
Consistent with the handling of the pandemic to date, however, there is no evidence of a strategy. The supplementary budget for health is merely further evidence of this.
Ideological responses, traditional economic theory won't lift SA out out of Covid-19 slump
- William Gumede
South Africa will have to prioritise new business, employment and growth based on the current and new domestic and global needs unleashed by Covid-19.
Given the cataclysmic nature of the Covid-19 economic crisis, conventional economic responses - of pursuing counter-cyclical fiscal policy, which is increasing public spending and cutting taxes, to stimulate the economy, employment and growth - on their own, will not do as solutions for South Africa.
Ideological responses or wishful thinking will also not do.
The government will need an integrated economic stimulus response, which should focus on rebuilding neglected public and social infrastructure – housing, education, water, transport and technology; while at the same time focusing on saving current critical businesses, jobs and opportunities, and creating new businesses, job creation initiatives and economic diversification.
An integrated response must also include overcoming the social impact of Covid-19, ranging from gender-based violence, mental illness, to a rise in crime. The backbone of an integrated economic response would therefore be based on building value chains that will produce the infrastructure, skills and material to deal with all these problems in an integrated way.
Such an integrated economic strategy must focus on both on Covid-19 relief, as well as post-Covid-19 economic reconstruction – both at the same time. A new integrated Covid-19 response strategy should carefully select the strategic sectors to be expanded or newly created, to diversify the economy, and which new technologies will help South Africa benefit from the Covid-19 acceleration in the digital economy.
Here are at least 12 pillars for an integrated Covid-19 economic recovery plan.
The first pillar would be to support current industries and create new ones, through expanding neglected public services in the areas which have increased the spread and impact of Covid-19. South Africa has large informal settlements, dilapidated township and rural housing – where no social distancing is possible. This is an opportunity to use a giant rollout of new housing to sustain existing construction-related businesses and create new ones,as well as jobs and growth.
The second pillar should be to foster a housing material manufacturing sector, where all the inputs, equipment and material that go into construction would be manufactured. New mass post-Covid-19 skills training for the poorly skilled would then be built around such a sector.
Crumbling water and sanitation infrastructure in the townships, informal settlements and rural areas will fan the Covid-19 spread. The third pillar would be expanding water and sanitation across the country, with similarly, a manufacturing arm which would build the inputs, material and equipment for the rebuilding of a water and sanitation sector.
South Africa’s public education system is falling apart – whether it is the poor quality of education itself, or school infrastructure such as classrooms, equipment and toilets. Human development is going to be essential, both to reskill those losing jobs because of Covid-19, and those who were jobless before the virus. However, the skills development should focus on training relevant people to operate in the post-Covid-19 economy.
Rebuild health infrastructure, food production chain
The fourth pillar of a Covid-19 integrated economic, social and health strategy should be the upgrading the public education system – again linked to construction manufacturing, aimed at boosting current businesses, creating new ones and expanding skills.
Covid-19 has exposed South Africa’s ailing health system. The fifth pillar should be rebuilding health infrastructure, and equipment and skills should be a crucial part of an integrated economic plan. South Africa imports most of its health equipment, personal protective equipment (PPE) and medicines from abroad. This is the moment to build a health-related manufacturing sector which could not only supply local needs, but also African and developing countries' needs. A mass health manufacturing skills development programme would then focus on fostering the skills needed for such a new expanded health manufacturing sector.
Covid-19 has battered South Africa’s food production chain. Producing food for the country, but also for the world, should be the sixth pillar of an integrated response. It should focus on expanding existing viable commercial farming, fostering new commercial farming and upscaling informal farming to produce the products the country and the world needs. A core component would be to build the agricultural manufacturing sector to produce the inputs, equipment and building material. Agricultural skills development should be linked to these areas.
Congested, dilapidated and outdated public transport - with minibus taxies, trains and metered taxies - has made it impossible to practise social distancing – and is helping along the rapid spread of the virus. Covid-19 is the moment to restructure the public transport economy, infrastructure and culture. As a seventh pillar, government will have to garner the political courage to transition South Africa from the death-trap minibus taxis to safer, cleaner and integrated transport – and link a skills development programme around these.
South Africa will have to prioritise new business, employment and growth based on the current and new domestic and global needs unleashed by Covid-19.
Covid-19 will accelerate the inevitable expansion of the digital economy, with many companies and people shifting online more quickly than before the virus. The new needs - ranging from working from home, to less to face-to-face interactive manufacturing and services, to online education - brought on by Covid-19 bring opportunities for new businesses to be created to meet these needs.
As an eightth pillar, Covid-19 provides the opportunity for South Africa to leapfrog into the digital economy. Increasing infrastructure and access to cheaper, faster internet and new technologies is a crucial for South Africa to benefit from the expansion of the digital economy. A Covid-19 strategy will bring South Africa’s businesses, public schools and homes into the digital economy. This means that there has to be dramatic expansion of the digital economy's manufacturing sector that should produce the materials, products and new mass digital skills.
The ninth pillar, is the opportunity to foster a green economy manufacturing hub in South Africa to provide new solar, wind and other sustainable energy sources. The inputs, materials and infrastructure must be produced here. A mass skills development programme should be launched alogside this to provide the skills for such a new manufacturing sector. Covid-19 provides an opportunity to create a recycling manufacturing economy, in the way China, Denmark and Sweden have done, where waste is reproduced as either inputs for others or as new products or to produce energy.
Most South Africans eke out a living in the informal economy, travel in informal transport and live in informal housing. This has also increased the spread of Covid-19. The 10th pillar should be to formalise the informal economy, travel and housing. A core element of an expansion of post-Covid-19 manufacturing sectors should be around formalising these sectors. Similarly, mass skills development programmes must also be centred on these areas.
Fiscal and monetary policy reforms crucial
The 11th pillar should be to boost the civil society organisation sector to secure existing jobs and create new ones. Civil society groups should help co-deliver public and basic services in communities – from combating gangsterism, combating gender-based violence and fostering community police partnerships to keep crime down.
Fiscal and monetary policy reforms are a crucial 12th pillar. Fiscal policy must have a programme of payment and tax holidays, easier finance, low-interest loans and softer collateral requirements for business and private individuals from private and public institutions. The Covid-19 social grant should be extended beyond the Covid-19 period. However, social grants could be linked to training and community work in critical areas, such as crime prevention, cleaning and volunteering. Monetary policy must be aimed at continuing to push for policy rate cuts as far as prudently possible, and injecting liquidity into the financial system.
In all these integrated economic recovery initiatives, government should strike partnerships with the private sector to initiate business recovery and creation. Alternatively, to partner and enter into public and private partnerships according to sound business principles set by private sector players who know their industries, not bureaucrats.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand; and author of South Africa in BRICS (Tafelberg This is an edited extract from an address “Building a post-Covid-19 Economy based on the Freedom Charter”, at the Webinar: “Fighting for Freedom: The Charter 65 Years On” organised by the Human Sciences Research Council, 25 June 2020. This extract appeared on News24.
Lockdowns and freedoms
- William Gumede
SA had to have a hard lockdown because we don’t trust our government. Little since has made us change our minds.
Whether countries implement lockdowns which significantly limit freedoms; or ones that try to retain as many freedoms as possible during their lockdowns depend on whether they have pre-existing open democratic cultures, higher levels of trust in government and whether citizens have greater self-responsibility.
The severity of Covid-19, justify restrictions on certain rights resulting from the imposition of quarantine, limiting freedom of movement, increased surveillance and the use of technology to track the movements of people. However, the challenge for many countries has been to balance these limitations of freedoms with maintaining basic human rights, freedom of expression and not impinging on individual dignity.
Countries can generally be divided in three groups in the way in which they responded to the Covid-19 pandemic. Some countries have opted for hard lockdowns with strict rules, limits to freedoms and movements. Such countries include South Africa, Panama and Thailand. In Panama men and women were designated different days to go on essential shopping. Like South Africa, Thailand banned sales of alcohol and imposed curfews.
Some governments, such as Hungary, Thailand and Ghana that implemented hard lockdowns have been accused of using Covid-19 to give themselves unlimited powers.
A second group of countries have had softer lockdowns, leaving it up to their citizens to take individual responsibility to practice social distancing, clean health hygiene practices and stay at home. These countries did not have the harsh lockdown restrictions, but placed the responsibility largely on their individual citizens to behave responsibly. These countries include Singapore, South Korea, Germany and many Northern European countries.
A third group of countries, such as Brazil, Belarus and Tanzania initially appeared not to have taken Covid-19 seriously. In response to why the country was not taking precautions against Covid-19, Belarusian President Aleksandr Lukashenko said: “it (Covid-19) happens.” Tanzanian President John Magufuli said workers must continue working and citizens must pray in churches and mosques, claiming the virus could not harm the “faithful”. The World Health Organisation lashed out at Tanzania for its refusal to introduce stringent measures to slow the spread of the virus.
With exceptions, the hard lockdowns have been mostly in countries that are either autocratic, non-democracies or poor quality democracies. In many of these societies, governments and leaders only know to tackle crises in hard-fisted ways. Alternatively, governments and leaders are not trusted by citizens, either because they are not accountable, corrupt or have not delivered public services before the lockdowns. Not trusting their governments, citizens do not follow government issued rules. Governments therefore use force to compel citizens to comply.
The South African government does not have the trust of many citizens, because of years of corruption, inefficiencies and lack of accountability. This means that many citizens would not have taken the government’s injunctions to self-regulate seriously. This is why in a sense the government had no option but to go for the hard lockdown.
Countries that have implemented soft lockdowns, such as Singapore, South Korea and Germany are higher trust societies. Citizens there have more confidence in their governments, because of their greater accountability, less corruption and better record of delivering effective public services. In these countries governments put the onus on citizens to adhere to lockdowns rules.
New Zealand is a democratic country that implemented a hard lockdown. However, New Zealand emphasised individual freedoms, common sense and still heavily relied on citizens taking self-responsibility. This was possible because citizens in New Zealand had a high trust in their government – and therefore high levels of public cooperation, because of government accountability, lack of corruption and effective public service delivery.
Having implemented hard lockdowns under the circumstances of distrust in government, it is important that the South African government ensure greater inclusivity in decision-making structures, such as the National Command Council, overseeing the Covid-19 response. Evidence-based decisions are crucial. Decisions must be explained, communicated transparently and must make rational sense. As a case in point, there has been very little rational explanation from government why tobacco and alcohol could not be sold during level 5 and 4 lockdowns and why e-commerce was not allowed.
There has to be greater oversight of government’s emergency powers under lockdowns by democratic institutions. So far, there has been little parliamentary oversight or even debate of the Disaster Management Act or the declared state of emergency, which gives the government extensive powers. Opposition parties should hold government accountable in Parliament. They have not done so.
Freedom of expression is crucial in hard lockdowns. Yet, it appeared that some ANC leaders believed that criticism of government actions are not permissible under Covid-19. This is off course not the case. A typical example has been the over the top criticism by Health Minister Zweli Mkhize of South African Medical Research Council president Glenda Gray she said that there were no cases of child malnutrition at Chris Hani Baragwanath Hospital until the lockdown.
Similarly, despite of public criticisms of the heavy-handedness of the South African National Defence Force’s enforcement of the lockdown, some ANC members of Parliament’s Joint Standing Committee on Defence, which is supposed to oversee the defence force praised the SANDF’s actions as “simple measures to discipline community members”.
The courts have an important role to play to curb government excess. It is important that citizens use the courts to hold government accountable if other official oversight institutions do not so. The family of an Alexandra township man, Collins Khosa, who died after allegedly been assaulted by soldiers during the lockdown enforcement in the township, went directly to the Constitutional Court to hold government accountable, have the soldiers involved fired and to seek compensation for his death.
But ombudsman offices, such as the Military Ombudsman, the police watchdog, the Independent Police Investigative Directorate (Ipid), and Chapter Nine institutions, such as the Gender and Equality Commission, should play a more pro-active role in holding security forces accountable during the lockdowns.
Citizens, civil society and the media should monitor and hold government accountable. Citizens must expose official wrongdoing whether on social media, protesting or seeking redress in the courts. With exceptions, countries which have allowed more freedoms during Covid-19 lockdowns, such as Singapore, South Korea and New Zealand, have in general had better health and economic outcomes.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand; and author of South Africa in BRICS (Tafelberg). The article first appeared in Times Select.
SA faces devastating multiple social impact
- William Gumede
Government urgently needs an integrated Covid-19 response to deal with mental illness, violence and crime.
South Africa urgently needs to put in place mechanisms not only to deal with the devastating social impact of Covid-19, whether from the trauma from the economic fallout from the virus, the mass loss of human lives and the effect of “cabin fever” from the lockdowns.
Record numbers of people will suffer from post-traumatic stress disorder (PTSD cases), the combination of stress, anxiety and depression that develops in some people who have experienced a terrifying event. It is very likely that the incidents of suicides are likely to jump, in a country with already high suicide rates. South Africa has the eighth highest rate of suicide in the world, with around eight thousand people committing suicide every year, meaning it is the third biggest cause of unnatural death after homicide and unintentional reasons.
Mental illness are likely to increase because of the financial stress, anxiety and self-isolation. The reality of possible illness or death surrounding us – and the possibility of becoming a victim can cause profound anxiety, depression and unease. The last World Health Organisation mental health survey of South Africa estimated that 30% of South Africans will suffer from a mental disorder over the course of their lifetime. It is very likely that Covid-19 pandemic will increase these figures.
Violence, whether in families, on the roads, workplaces, educational institutions and in communities are going is likely to rise. There has been a terrifying rise in domestic violence and abuse against women and children. There will be a rise in marriage breakdowns. Drug and alcohol abuse will soar. Familicide, murder-suicide or murder in which a person kills multiple close family, whether spouses, children and relatives are likely to increase also.
Crime levels in South Africa is likely to increase to even higher levels, whether robbery, housebreaking and cash-in-transit heists. The prolonged lockdown, with many young people in townships and informal settlements being idle, may see an increase in teenage pregnancies, not unlike the spike seen in the 1980s State of Emergencies. The disruption in the school year, may also mean that many in public schools will drop out of the schooling system, in ways black youth dropped out of school during the 1980s State of Emergencies. South Africa may see another Lost Generation of public school dropouts, unless there is an urgent intervention by government, civil society and communities.
As Covid-19 rages, many South Africans with other illnesses are either not seeking medical help; or not getting attention – as the hospitals are turned into Covid-19 treatment theatres. This means that many South Africans may die of non-Covid-19 related causes. Unless government get food to the needy and to schoolchildren large numbers may die from starvation, malnutrition and related illnesses.
Gangsterism is already on the rise. In the despair because of lack of income, food and government failure, ganglords in many townships have now become the providers of food, money and help to the needy. There is likely going to be a rise in corruption too.
If the state fails to deliver an effective Covid-19 strategy, there will be a rise in violent social protests. Populism will rise – as opportunists will try to exploit hardships for self-enrichment. There are likely going to be a rise in tribalism also, as people seek refuge in tribal solidarity, to, given a failing state, to deal with their hardships. There are likely going to be a rise in blaming outsiders. This means we will see a rise in xenophobia too. Racial tensions may rise, and with it incidents of racism and accusations of racism rising too.
Government urgently needs an integrated Covid-19 response which must include plans to overcome the potentially devastating multiple social impact of Covid-19. Covid-19 business, unemployment and basic income grants must reach the needy in time. The Covid-19 social grant should be extended beyond the Covid-19 period. Social grants could be linked to training, civic work in critical areas such as crime prevention, supporting vulnerable families and children and community cleaning.
The army may have to remain in townships for some time beyond the Covid-19 pandemic to tackle crime, violence and social breakdown.
Government, business and individuals must behave honestly during this crisis and beyond. All South Africans must support individuals not on racial solidarity, but on honesty, values and competence. We need new levels of civic solidarity, which goes across race, class and political party. Individuals will have to reach out to vulnerable neighbours, friends and family, to provide support, connection and companionship. Schools, religious and community organisations must reach to vulnerable members, individuals and groups.
Those who can should prioritise self-wellness, self-care and healthy living. Companies will have to invest in employee wellness as the fear, anxiety and powerlessness associated with Covid-19 and the lockdown “cabin fever”, cause symptoms similar to post-traumatic stress syndrome in many, which could potentially undermine employee productivity.
Civil society is going to be crucial in softening the social impact of Covid-19. Currently, no provision has been made in the government’s Covid-19 emergency stimulus or by private sector solidarity funds to support non-profit civil society organisations, which includes charities, community-based organisations and civil movements.
Civil society groups should help co-deliver public and basic services in communities – from tackling gangsterism, combating gender-based violence and fostering community-building programmes to keep crime down and supporting the vulnerable.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand; and author of Restless Nation: Making Sense of Troubled Times (Tafelberg). This article was published in the Sunday Times.
COVID-19 vaccine trial in South Africa: everything you need to know
- Shabir Madhi
Not enough clinical research is being done in Africa. This has repercussions for when interventions become available and effective in high income countries.
There isn’t enough clinical research being done in Africa. Less than 2.5% of all clinical trials in the world are done on the continent. This is why South Africa’s involvement in one of the COVID-19 vaccine trials is so important. The country’s effort is being led by Professor Shabir Madhi. The Conversation Africa’s health and medicine editor Ina Skosana spoke to him about the process, and what can be expected. This is an edited version of a podcast [which you can listen to here Pasha 71: COVID-19 vaccine trial in South Africa explained]:
How does the trial work?
The study that we embarked on in South Africa is for a vaccine that was developed by the Jenner Institute at the University of Oxford. It’s what is known as a non-replicating vector base COVID-19 vaccine.
The study came about when I reached out to the principal investigator at the University of Oxford whom I’ve known for over 20 years to find out if there was any interest on their part to include South Africa as part of the clinical development plan of the vaccine. The short answer was yes, provided we conducted the study on our own, including raising the funding to conduct the study.
The agreement with Oxford University preceded a subsequent agreement that they’ve entered into with AstraZeneca, the pharmaceutical company responsible for the further clinical development of the vaccine and future manufacturing. Pre-clinical studies of this vaccine candidate, including in non-human primates, have demonstrated initial evidence of the safety of this vaccine, as well as its ability to protect against COVID-19 disease.
Why South Africa?
The main reason is that the legacy of vaccines shows that they don’t necessarily work similarly across different populations. So if we want to be one of the early adopters, in terms of implementing vaccination against COVID-19 as part of our immunisation programme, we really need to generate data applicable to the local context.
A number of past vaccines have been shown to be highly efficacious in high income settings. But when they’ve gone on to be evaluated in low and middle income settings, they were found to be much less efficacious and, at times, not efficacious at all.
So if we want to make informed decisions at an early stage about whether these vaccines are going to be of benefit to people in South Africa, it’s critical that we undertake the clinical evaluation during the start of the entire programme, rather than at the latter stage. Waiting for results to come in from other studies would just lead to a lag in terms of the timing when vaccines would be introduced in South Africa as well as other low and middle income countries.
This has been the experience for many other life saving vaccines where it has taken between five and 20 years between their availability in high income countries and low middle income countries.
How are participants chosen for the trial?
Participation is completely voluntary.
Participants typically come to inquire about the study at clinics. We sit down with them and explain what the study is all about. What are the criteria for joining, what the expectations are of the volunteers because the study has quite intense expectations in terms of being able to come for regular visits. And they obviously need to be agreeable that when they do participate in the study, if they do develop signs and symptoms suggestive of COVID-19, that they would come forward to be investigated. This is critical for us to be able to determine whether this vaccine protects against COVID-19.
In addition, we would do some blood tests which ensures that they don’t have any sort of medical conditions that we would want to exclude.
If they’re found to be eligible, we randomly allocate them to one of two groups. Half will receive the vaccine, and the other half a control substance, which in our case, is a placebo. This is important for two reasons. The first is that it allows us to provide robust data in terms of the safety profile of the vaccine. And the control group enables us to determine whether the vaccine actually does have any impact in protecting against COVID-19.
Is there any reason people should be sceptical of the trial?
The short answer is no. The narratives that Africans are being used as guinea pigs is fundamentally incorrect. Rather a case of us wanting to generate robust scientific data to be able to make informed decisions about whether those vaccines actually do protect South Africans – and possibly Africans more generally – against developing COVID-19.
What are the next steps?
Right now we busy enrolling into the clinical trial. We’ve just reached the 200 mark out of the 2000 participants that we plan to enrol. We expect to have completed enrollment of all the volunteers over the next three to four weeks.
After that we will keep in touch with all of the participants at least every two weeks, including weekly SMS messages to determine whether or not experiencing any signs or symptoms of COVID-19. And if they are they will be asked to come in to be investigated to determine whether they are infected or not.
The endgame of the study is twofold. One is obviously to evaluate the safety of the vaccine, which is something that is ongoing almost on a daily basis.
The second part is that once we have about 42 individuals that have developed COVID-19 at least about a month after they’ve received the first dose of either the vaccine or the placebo we will then be able to do an analysis to determine whether the vaccine actually does protect against COVID-19. Specifically we will be testing if the vaccine efficacy is at least 60%; that is by being vaccinated your risk for developing COVID-19 will be reduced by at least 60% if not more.
We anticipate that we will probably be able to provide an answer as to whether this vaccine works and protects against COVID-19 by the end of November this year. In the worst case scenario it might take us a bit longer probably into the second quarter of next year.
What about managing expectations?
It’s very exciting to be involved in the sort of clinical development of the vaccine. But we need to be guarded in terms of our expectations as to what the result will be.
The fact that we’re embarking on a clinical trial doesn’t mean that we’re going to have a vaccine that’s going to protect against COVID-19.
Only about 10% of vaccines that go into clinical trials are eventually licensed for use. Right now there’ are approximately 200 vaccines that are being developed for COVID-19. It would be a huge accomplishment if, over the next 12 to 18 months, we are successful showing that even one out of every 20 (5%) of the vaccines that go into human studies are safe and provide some protection against COVID-19.
So even though there’s a huge amount of work taking place around vaccines, at least for the next 12 months the only tools that we’ve got available to us to try to protect people is adherence to physical distancing, the wearing of face masks in public spaces, avoiding mass gatherings, and making sure that you’re in adequately ventilated settings when in public spaces.
Anyone living in South Africa who is interested in participating in the study can e-mail vidacov19@rmpru.co.za for more information.
As we enter the second phase of reopening, it will be necessary for more academic, professional and support staff to return to work on our campuses. A comprehensive workplace plan has been shared with managers. It includes guidelines on the preparation of the workplace before employees arrive; the responsibilities of managers, health and safety officers and employees before returning to work; rules for staff whilst at work; and a protocol to follow when infections are reported.
The SET agreed to the following principles:
All academic, professional and administrative staff who can work from home, should continue to do so, and should only come onto campus if necessary;
Staff members who have to deliver essential services that cannot be conducted remotely or from home, are required to report for duty if requested to do so by their line managers. Staff members without an official permit will not be allowed onto Wits’ campuses;
Staff members over the age of 60 or those living with co-morbidities should stay at home where possible;
All staff who are unable to work during this period, should, where possible, be redeployed to areas where they can make a contribution.
Staff members who have co-morbidities (like cancer, diabetes, asthma or other respiratory illnesses) should voluntarily declare these illnesses to their line manager or provide a valid doctor’s letter that indicates specifically why they cannot report for work. Where line managers believe that it is necessary, a second opinion may be obtained from selected healthcare practitioners based at the Wits Donald Gordon Medical Centre.
Workplace preparation
Line managers should work with health and safety officers, the Services Department and Human Resources personnel to ensure that the following measures are in place:
The physical distancing of staff and students;
The adequate provision of sanitisers and/or soap and water;
The regular cleaning of venues and work spaces;
The provision of cloth masks (two per staff member) and other personal protective equipment for specialised areas; and
Protocols to prevent the spread of infection.
It is the responsibility of every staff member reporting for duty on campus to complete the self-screening process via the Wits LogBox Screening Appevery day BEFORE entering Wits’ premises.
The form includes a checklist for managers to follow as soon as they are made aware that a staff member has been diagnosed with Covid-19. Amongst other aspects, the checklist places the responsibility on managers to report all cases to the relevant OHS&E and HR representatives (for reporting and management purposes); to Protection Services (in order to block access to campuses); to Services (in order to arrange for the cleaning of possible contaminated areas); and to the Campus Health and Wellness Centre (to follow up on the infected person). Line managers (with the help of the OHS&E Directorate) also need to conduct an investigation in order to try to establish the cause of the infection, to determine whether protective measures are adequate as per regulatory requirements, and whether any other persons could potentially have been exposed. The results of the investigation may make it necessary for the Department/School/University’s risk assessment processes and procedures to be reviewed.
As at 3 July 2020, the total number of employees positively diagnosed with Covid-19 is 15. No fatalities have been reported. The University is investigating each reported case. All infected persons are self-isolating and as at 3 July 2020, none have reported being hospitalised due to COVID-19 complications.
The Covid-19 pandemic will be with us for the next few months at least, possibly longer. We know that this pandemic is taking a toll on many. We are with you – we are all facing this scourge together, and it will take our collective care, strength, commitment and humanity to keep this pandemic at bay. Your individual ideas and comments on what else we can do for the Wits community are welcome – please send them to vco.news@wits.ac.za. They will be collated and passed on to the Senior Executive Team for consideration at our next meeting.
SENIOR EXECUTIVE TEAM
3 JULY 2020
Covid-19 Update (36): It's in our hands
- VCO News
Witsies, please take care, adhere to social distancing and follow Covid-19 protocols.
Thank you for all that you have done in recent months – we know that it has been an incredibly difficult time for many of you. As infections in the province rise, we urge you to take care of yourself, and to look after your colleagues and loved ones. Let us continue to work coherently and to act responsibly in the best interests of all members of the Wits community.
Number of infections
There are 40 staff members who have reported testing positive for COVID-19 over the past three weeks (22 June to 10 July 2020), many of whom have been working from home. Sixteen students have also tested positive during this period. All affected staff members and students are self-isolating, in line with the University’s COVID-19 protocols.
The passing away of a staff member
Mr Stanley Nkanyangi, a Supervisor in the Parking Office, passed away this week. At this stage we are still unsure of the cause of his death. Please take a moment to remember him and all those who have passed away.
Our responsibility
We are all responsible for taking care of ourselves and others in our community. With the permission and support of your line manager, if you are able to work from home, please continue to do so. However, if you are required to report for duty on campus, please follow the University’s approved COVID-19 protocols.
To protect yourself and others, always do the following:
Complete the daily screening process via the Wits App BEFORE entering campuses,
Wash your hands regularly with soap and water for at least 20 seconds and dry properly,
Wear your mask over your nose and mouth (or the appropriate PPE in specialised areas) at all times,
Stay at least 1.5 metres from any other person,
Sneeze or cough into your elbow, and
Follow all COVID-19 University protocols and rules.
Our actions today will impact on our collective futures tomorrow. Let us take the necessary precautions to ensure that we do our best to protect our colleagues, students, friends and other members of our community.
We are in this together.
Keep safe.
SENIOR EXECUTIVE TEAM
10 JULY 2020
Wits University senior clinicians volunteer for Covid-19 vaccine trial
- Wits University
Senior clinicians in the Faculty of Health Sciences at Wits University have volunteered to participate in South Africa’s first Covid-19 vaccine trial.
Volunteers were screened on Friday, 10 July and those found eligible to participate in the trail were vaccinated on Tuesday, 14 July at the Soweto trial site in Johannesburg.
According to Wits Professor of Vaccinology, Shabir Madhi, who leads the South African Covid-19 vaccine trial, the legacy of vaccines shows that they don’t necessarily work similarly across different populations.
“We really need to generate data applicable to the local context. A number of past vaccines have been shown to be highly effective in high-income settings, but when evaluated in low- and middle-income settings [like South Africa], the vaccines were found to be much less effective and, at times, not effective at all,” says Madhi.
Dr June Fabian, nephrologist and Research Director at the Wits Donald Gordon Medical Centre, explained her motivation for volunteering for the trial: “For me it’s about supporting local scientists to do world-class science. I think it’s amazing that South Africa is a Covid-19 vaccine trial site and to be a part of that is very exciting. We must support each other as a Wits community and we must support our colleagues.” Fabian was one of the scientists involved in the world's first intentional HIV positive liver transplant in 2018.
Leading HIV clinician, Professor Francois Venter, Divisional Director of Ezintsha at Wits University, said of his participation in the trial: “This collection of Wits Faculty, between them, have first-authored some of the highest-impact medical articles on pandemics. It’s important to demonstrate how urgent and safe these [Covid-19 vaccine] studies are, and I have enough confidence in the science to put myself on the line.”
Dean of the Faculty of Health Sciences at Wits and Professor of Surgery, Martin Veller, said of his vaccination this morning: “The coronavirus pandemic has caused massive disruption in the world to public health and economies. As a consequence, a vaccine is probably the only way to manage in the medium term. We need to get a trial done quickly. Anyone who can enroll, and especially we in the healthcare fraternity who understand the risks, should.”
Veller added that he feels strongly that Africa needs to be involved in vaccine development so there is a moral obligation for the continent to be able to access the vaccine once it becomes available.
Some in the healthcare fraternity are represented by the Progressive Health Forum (PHF), a national advocacy network of health professionals, activists and experts. Dr Aslam K. A. Dasoo, convener of the PHF and a trial volunteer, says that this vaccine trial is part of a multi-centre global effort to meet the greatest threat to humanity in living memory.
“Knowing that a vaccine is the best possible means of mitigating the global impact of the pandemic makes it a great privilege for me to participate in this study. For those who have expressed anxiety at the trial being conducted here, my enrolment, together with other doctors and medical scientists, should provide comfort that the trial is safe. More importantly, it is a signal that South Africa is not only at the forefront of this scientific effort, but also makes it more likely that the people of our continent will benefit from a future vaccine,” says Dasoo.
If you would like to volunteer to participate in South Africa’s first Covid-19 vaccine trial, email vidacov19@rmpru.co.za for information or call 072 055 1249 (Soweto area) / 074 800 7772 (Tshwane area) / 064 850 0744 (Hillbrow area).
Madhi said: “If we want to make informed decisions at an early stage about whether these vaccines are going to benefit people in South Africa, it’s critical that we undertake the clinical evaluation during the start of the entire programme, rather than at the latter stage. Waiting for results to come in from other studies would just lead to a lag in terms of the timing when vaccines would be introduced in South Africa as well as other low- and middle-income countries.”
Madhi assumes the role of Dean of the Faculty of Health Sciences at Wits in January 2021 after Veller retires.
How to protect yourself against increased cyber threats
- WitsICT
With the onset of the Coronavirus/Covid-19 pandemic, working and studying remotely have increased the risk of cybercrime.
This Cybercrime Survival Guide unpacks the potential cyber risks you may face and provide you with non-technical advice to protect yourself online. It offers valuable tips for cloud users, personal computers and mobile devices to ensure that your information is kept safe. [Download the Cybercrime Survival Guide.]
The Wits community should take note of these guidelines to protect themselves online, and observe the following:
Windows 7 and Windows 10
Microsoft no longer supports Windows 7 (that includes security upgrades and updates); and it is vital that users upgrade to Windows 10.
Windows updates need to be installed regularly. Microsoft releases patches every second Tuesday of the month.
You must have Antivirus software installed on your devices, there are both free and paid versions. Make sure these have the latest pattern files and updates.
Browsing the internet, purchasing online, checking email and using social media
Think before you send an email, search or post. Keep personal information limited and professional.
Practice safe browsing. Only browse and visit websites that are safe and that you trust the source. Do not browse unknown websites and be wary of the links that you click on.
Be careful of what you download. Cyber criminals often trick users into downloading malware programs or apps that carry viruses or try to steal information. These programs are disguised as an app or can be anything from a popular game to traffic or weather reporting. Don't download apps that look suspicious or come from a site you do not trust. Verify that a website is legitimate.
Choose strong passwords. Any password that is used needs to be complex. When entering the password on a site, make sure the website is using HTTPS.
Make online purchases from secure sites only. When providing credit card or bank account information, make sure the website is using secure, encrypted connections, i.e. they use HTTPS.
Be careful what you post online, especially on social media platforms. Think before you post. The Internet does not have a ‘delete key’. Comments, images, information stay online.
Be careful who you meet and chat with online. People you meet online are not always who they claim to be. It's easy to set up fake social profiles and con users. Be cautious and sensible in online activity.
Clicking on links in emails: Do not click on links in emails. If you need to click on a link, verify it has been sent from someone you trust, and also verify that the link is hosted on a trusted server.
Opening documents sent in emails: If an email contains a document and you need to open it, verify that the email was sent from someone you trust. Make sure your PDF reader and Office suite are up to date. Often cyber-attacks come via documents in emails using vulnerabilities in PDF readers and Office documents.
Be mindful of public Wi-Fi networks. Limit the use of these networks to basic browsing only.
Covid-19: Women are bearing more costs and receiving fewer benefits
- Nic Spaull, Daniela Casale and Dorrit Posel
Even though women have suffered two thirds of the job losses since February, men have received two thirds of Covid-19 grants (65%).
On 15 July we released theresultsof the largest non-medical Covid-19 research project in South Africa: the National Income Dynamics Study (NIDS) Coronavirus Rapid Mobile Survey (CRAM). It shows that three million jobs were lost during the first stage of the lockdown, and of those, two million (66%) were accounted for by women, and in particular poor women. This is a very concerning finding since there are large knock-on effects of this income loss for women and for the children who live in their households, especially when the woman is the sole breadwinner.
Perhaps unsurprisingly, given that initial job losses were so large and concentrated among women, we see unprecedented levels of household vulnerability, with half of all respondents (47%) saying that their household ran out of money to buy food in April and one in five (22%) reporting that someone in their household went hungry in the last seven days. Child hunger has at least doubled since 2018 with one in seven (15%) reporting that a child went hungry in the last week because there was no money for food.
What makes these results all the more devastating is that women are not receiving the new R350 Covid-19 grant at the same rate as men.
In a presentation to Nedlac on 30 June, Sassa reports that of the 3.25 million Covid-19 grants paid out up until the end of June, only 1.15 million were paid out to women. Put differently, two thirds of Covid-19 grants (65%) were paid to men even though women suffered two thirds of the job losses.
One potential reason is that people who receive other grants are ineligible for the new Covid-19 grant. For example, many women receive the Child Support Grant which has now been topped up by R500 per caregiver (notenotper child). Yet, this grant is primarily for the benefit of the child rather than the caregiver. The implication is that women who have lost their jobs are being disadvantaged because they have children.
This policy response assumes that those who receive the CSG were not personally dependent on their employment or earnings to make ends meet. It is a mistake to think that those who receive grants are somehow “immune” from job losses since they already have a grant.
Gabrielle Wills’ analysis of the General Household Survey of 2018 shows that 63% of grant-receiving households report receiving some income from employment or business, and only 42% said that grants were their “mainsource of income”. In other words, even grant recipients depend heavily on earnings from employment. And this is not surprising, since the CSG is not sufficient to lift a child above the poverty line, let alone children and their caregiver.
Because the top-up paid for the CSG is constant, regardless of the number of children the caregiver is responsible for, the extra support is often spread very thin, and in a sense is regressive – the more children you have the less there is to go around.
Let’s take the example of a mother living with two children who has lost her job and has no other income support. Her household of three would have to live on R1,380 a month (i.e. the R440 CSG per child plus the R500 top-up). This amounts to R460 per person, which is below StatsSA’s “food poverty line” of R578 a month.
And, of course, this minimum subsistence amount does not take into account the cost of rent, fuel, electricity, clothing and other essentials. Add to this rising food prices during the lockdown, and the loss of the one meal a day through the school-feeding scheme that 9 million children relied on to meet their minimum caloric needs, and it is easy to see how quickly families can fall into destitution.
The Covid-19 grant was designed to protect those who have suffered job loss and the income they were relying on. These grants should be provided regardless of whether a CSG is being received on behalf of a child.
Why so many women are not receiving the Covid-19 grant is not clear at the moment, and Sassa should investigate this urgently. The exclusionary criterion which prevents concurrent grant-holding is likely to be a key factor. It may also dissuade women from applying in the first place. What is clear is that half as many women as men are receiving these grants and yet twice as many have lost their jobs.
This is deeply troubling and requires immediate attention.
Nic Spaull is a Senior Researcher at RESEP in the Economics Department at Stellenbosch University; Daniela Casaleis an associate professor in the School of Economics & Finance at Wits University; Dorrit Posel is Helen Suzman chair and a distinguished professor in the School of Economics & Finance at Wits University. They are also part of the Nids-Cram consortium of researchers, visithttp://www.cramsurvey.org
Opposition parties struggle with how to play a Covid-19 role
- William Gumede
South Africa’s opposition parties appear to be confused, chasing shadows or paralysed by the enormity of the Covid-19 crisis.
Opposition parties, are supposed to hold government accountable, offer new ideas on post-Covid-19 economic, political and social reconstruction and act in such a way the public would perceive them to be able to do a better job if they would have been in government. Yet, South Africa’s opposition parties appear to struggle to come to terms over what role they should play in the pandemic engulfing South Africa.
Some opposition parties, such as the Inkatha Freedom Party, United Democratic Movement and the GOOD party appear to have entirely disappeared from the public scene in the aftermath of Covid-19 crisis.
At the beginning of the Covid-19 outbreak the opposition parties started well-enough. Outside parliament the 14 opposition parties issued a joint declaration: “The 14 political parties in our Parliament are standing together, across party political divides, to fight this disease together. We hereby demonstrate practically that we are united as the leaders of our nation to overcome this global crisis facing our country and our people”.
Opposition parties even made innovative proposals then. For example opposition parties proposed that government gave an Unemployment Insurance Fund (UIF) contribution holiday to employers, allow for Value Added Tax (VAT) refunds and for government to encourage business to propose payment holidays on property loans, business loans and vehicle loans. After that things went peer-shaped for the opposition.
The Economic Freedom Fighters since have supported Madagascar’s untested herbal drink as an “African solution” “cure” for Covid-19. The World Health Organisation has rejected the herbal drink saying ordinary Africans also deserve medicines which have been clinically tested, just like communities in Western or other developing countries.
EFF leader Julius Malema have also been touting African herbs including the herb commonly known as Umhlonyana in isiZulu, Lengana in Sesotho, Wilde Als in Afrikaans and Artemisia or African Wormwood in English. “Let’s start bottling it nicely because the only thing that we buy from these people is their fancy packaging”, Malema said.
Separately, Malema said South Africans must be defy moving the lockdown to level 3 on 1 June, saying if the EFF was in power, it would keep the lockdown at level 5, even if it means collapsing the economy. “If this white economy collapses, let it collapse”, he said, as if the economy is only made up of white participants, and as if only white, not black people will suffer if the economy collapses.
Economic Freedom Fighters MP Mbuyiseni Ndlozi saw a conspiracy in US billionaire Bill Gates offering to help African countries amid the coronavirus outbreak, rather than embracing help to stem the rising Covid-19 tide from overwhelming South African and African health and economic systems.
Ndlozi tweeted: “Nothing qualifies the university drop out Bill Gates to lead debates on vaccines & medical responses to #covid_19 except that he holds shares in BIG pharmaceutical companies. It’s a FACT that Gates is an under educated computer nerd who dropped out of university to become rich!”
The Democratic Alliance attacked Trade and Industry Minister Ebrahim Patel for gazetting a list of clothing and related products that could be for sale in retail stores during level 4 lockdown as “frankly mad and seem more at place during the 1980s under the Soviet Union than they do in a democracy like SA”.
Patel defended the clothing regulations saying they were requested by industry bodies and was aimed at pushing SA-made products to boost the local manufacturing and retail sector. The clothing industry bodies supported Patel. The National Clothing Retail Federation (NCRF), the industry body which include Mr Price, Pick n Pay clothing and Queenspark, and the Apparel and Textiles Association of SA (Atasa) supported the gazetted regulations for their potential “to ensure a form of social and economic recovery by many distressed companies in the sector”.
In holding government accountable, the opposition, should try to articulate realistic alternative policies for governing the country, which means they have to promote the interests of, and be relevant to the wider population. Off course, an opposition party, may decide it wants to remain small, and would rather just play a minimal watchdog role and only focus on the interests of a small core constituency, or alternatively just criticise government for the sake of it, just to get attention, with no intentions of wanting to be taken seriously as a possible government-in waiting.
Nevertheless, the opposition should ensure the sitting government make decisions in a transparent, rational and fair way. And get government to explain the reasons for coming to certain decisions. As a case in point, there has been very little rational explanation from government why tobacco and alcohol could not be sold during level 5 and 4 lockdowns and why e-commerce was not allowed.
Currently there has been no parliamentary oversight or even debate of the Disaster Management Act or the declared state of emergency, which gives the government extensive powers, nevertheless, opposition parties can still do so in parliament. They have not done so.
The DA and the Freedom Plus (FF+) did say they were planning to go to court to challenge the constitutionality of some lockdown regulations.
The government has reopened schools, yet with no readiness plan, given that social distance in public transport and schools are almost impossible, that many public schools do not have basic amenities such as working toilets and that pupils, if infected, will in turn infect vulnerable family members at home.
Mmusi Maimane’s One South Africa movement had petitioned the Constitutional Court to challenge government’s decision to reopen schools, but the court dismissed the application.
The opposition should hold government accountable to ensuring that human rights, freedom of expression and equal treatment is respected during the implementation of the lockdown. They must make certain that food gets to the poor on time; that the unemployed can access Covid-19 social grant quickly and easily without red tape; that distress businesses can get help quickly and fairly from the R500bn Covid-19 fund.
They should insist civil society organisations to get funding from the R500bn Covid-19 fund, which is not currently the case. They should safeguard against corruption, mismanagement and waste of Covid-19 funding; and watch over Covid-19 funding to ensure it is given to struggling businesses based on merit, fairness and common sense.
They should push for government to partner with civil society and business to deliver public services during Covid-19 crisis; and to advocate for the public and private health sector partner to share resources, expertise and services to combat Covid-19, which is not currently the case.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand; and author of Restless Nation: Making Sense of Troubled Times (Tafelberg). This article was first published in the Daily Dispatch.
Africa’s research capacity is growing. That’s good news for pandemic response efforts
- Sam Kinyanjui and Sharon Fonn
Investments are starting to help grow the African continent's science preparedness.
The COVID-19 pandemic has put global emergency preparedness under sharp scrutiny. It’s also placed national health systems’ capacity to predict and respond to major emergencies under the microscope.
Much of the response to the pandemic is focused on testing, case management and control measures such as personal hygiene, quarantine and social distancing. But in most African countries, these measures are not backed by reliable context-specific data. Instead, depend largely on epidemic curves from China and Europe; these appear to differ from those in sub-Saharan Africa.
Governments and other stakeholders are desperate for accurate, real-time data on the pandemic’s progress to inform intervention strategies. The scarcity of medical and laboratory resources because of increased global demand, along with international travel restrictions, has also forced countries to look inwards. African countries, for instance, are seeking local innovations and adaptations in COVID-19 testing options and interventions, as well as personal protective equipment.
All of this has turned attention to the contribution that local researchers can make in responding to the pandemic. This centres on the concept of science preparedness. Some commentators define science preparedness as
a collaborative effort to establish and sustain a scientific research framework that can inform and enable emergency planners, responders and the whole community to better prepare for, respond to, and recover from major public health emergencies and disasters.
Many countries in sub-Saharan Africa have low research capacities. This has led to some anxiety and fear about the ability of the research community to provide scientific backup to COVID-19 response. However, the last decade or so has seen a significant increase in funding for research capacity in Africa. But has this investment impacted on the continent’s science preparedness?
We set out to address this question by reflecting on how research expertise, infrastructure and resources established under one of the largest networks for research capacity building in Africa has been mobilised for pandemic response. Four months into the pandemic, we surveyed members of a massive African coalition. This revealed just how extensively the continent’s researchers have mobilised their expertise and resources towards the COVID-19 response.
At the forefront
The African Research Coalition for Health (ARCH) is an umbrella network of 11 African-led consortia largely funded by the DELTAS-Scheme of the African Academy of Science. It covers 54 African research institutions and universities across 17 Sub-Saharan countries. The coalition aims to build high-quality research capacity across the continent.
By the end of 2021, ARCH will have supported training for more than 1000 high-quality PhD and postdoctoral researchers. The numbers will be similar for Master’s training and graduate research internships, across most spheres of health research.
Responding to our survey, many ARCH partner institutions indicated that they were among the first COVID-19 testing and diagnostics training nodes in their respective countries. Beyond testing, the institutions have also deployed their surveillance systems. And they’ve used their expertise in epidemiology, modelling and pathogen sequencing to help. A significant proportion of this expertise was developed under the ARCH framework.
Many ARCH-trained researchers are currently launching immunology and pathogenesis studies to inform COVID-19 drug and vaccine development. Clinical trials capacity in Sub-Saharan Africa is limited. But ARCH has supported the development of some of the best capacity for trials in the region. At least four consortia are preparing to support clinical trials for COVID-19 vaccines and drugs.
The global response to COVID-19 requires a multi-sectoral, multi-agency approach. More than 30 ARCH-affiliated scientists and training fellows have been formally appointed to their respective national COVID-19 response teams. They are advising on all elements of the pandemic, including aspects like mental health. This builds on the links that ARCH consortia have established with their local state health agencies.
Several ARCH ethics researchers have also been involved in developing guidelines for expedited ethics review and approval for COVID-19 studies.
Prolific African researchers
The results of our study suggest that investment in research capacity building is paying dividends in sub-Saharan Africa.
ARCH’s model is underpinned by a theory of change that encompasses four domains of scientific leadership. These are research training; scientific excellence; scientific citizenship and research management. The coalition also strongly emphasises retaining and nurturing researchers beyond training.
This broad view of research capacity building has generated a cohort of prolific African researchers. Many of them lead their own research programmes. They are also fostering strong collaborations between the consortia and local ministries of health and other key health stakeholders to translate and implement research output.
All of this is illustrated by the fact that when COVID-19 reached Africa, the consortia were able to rapidly deploy and redirect their expertise, research resources, infrastructures and links with health agencies to support the response.
Work to be done
This isn’t to suggest the continent’s research capacity is fully developed. Much work remains to be done. The number of African researchers still falls far short of critical mass. Many countries are still excluded from coalitions like ARCH because their governments and other research funders will not invest. The pandemic is an opportunity for African governments to seriously reflect on their efforts to build science capacity.
It’s also important to point out that despite the expertise, infrastructure and resources that ARCH and other African institutions have mobilised for COVID-19 responses, critical gaps remain in Africa’s science preparedness.
Many institutions are hamstrung by an inability to procure key reagents, goods and services for laboratory and field-based research for COVID-19 and other diseases due to lockdown and travel restrictions. Such issues highlight the urgent need to strengthen institutional and national business continuity plans for research during major crises.
South Africans aren’t wearing masks or keeping their distance. This needs to change
- Laura Rossouw and Carmen S. Christian
Changing social norms in a short amount of time is difficult, and a one-size-fits all policy is unlikely to have the desired effect.
In countries like South Africa that face severe resource shortages, the burden of fighting COVID-19 falls heavily on citizens to change their behaviour and follow preventative measures. These include avoiding mass gatherings, physical distancing and wearing masks.
But a crucial determinant of whether people will change their behaviour includes having access to credible health information that’s trusted and that people can adopt. Inadequate sources of information carry a number of risks. One of the biggest is that people who don’t have credible information will be more exposed to the virus because they are less likely to abide by these behaviour changes. The second risk is that people don’t fully perceive the danger of COVID-19 or its negative outcomes.
This is often the case with preventative health interventions: they require individuals to make an investment in their health prior to being sick. For example, a person has to wear masks even though they are healthy.
Unfortunately, high-impact behaviour change is not happening fast enough in South Africa. Our research found that most people – 91% of those surveyed – reported that they had changed their behaviour since the start of the pandemic. But most of these efforts were on lower-impact strategies, such as washing their hands and cleaning surfaces.
Of those who changed their behaviour, the focus was less on high-impact strategies like wearing masks (53%), avoiding people by either staying at home or not attending large gatherings or avoiding big groups (58%), and physical distancing (25%).
The ‘why’ question answered
The survey was based on the nationally representative National Income Dynamics Study (NIDS) – Coronavirus Rapid Mobile Survey. In this survey, 7000 South Africans are telephoned every month and asked a range of questions about their income and employment, their household welfare, receipt of grants, and about their knowledge and behaviour related to COVID-19. Because the same people are contacted every month, researchers can track how their personal and household circumstances change over time.
The first survey showed that there is inadequate knowledge of COVID-19 symptoms among South Africans. For instance, only 11% of those surveyed were able to list tiredness as a symptom, and only 6% could list all three of the most common COVID-19 symptoms – coughing, fever and tiredness.
And 8% of people surveyed were not able to list any symptoms at all.
This is worrying. The country’s current public health approach relies on society to monitor their symptoms in order to know when to isolate or seek additional care.
The infectious nature of COVID-19 means that behaviour changes are required to change the trajectory of the disease. For instance, universal masking of at least 80% is required to flatten the infection curve. The paucity of COVID-19 symptom knowledge implies that South Africans may be unable to self-screen and self-isolate should they become infected. The joint failure on these two fronts may impede the containment of the virus.
The question of where people got their information was also revealing. Almost four in five of those involved in the survey said they relied on news media for their trusted source of COVID-19-related information. Only 14% said they relied on government sources and 11% on health workers.
The study found that those who relied on the government and health workers had more accurate knowledge of symptoms and were more likely to abide by high-impact preventative strategies.
Next steps
There is a clear responsibility placed on South Africans to adopt and adhere to high-impact preventative behaviours, remain vigilant and make daily sacrifices. This commitment requires serious societal buy-in.
So, how should the government go about encouraging this, given that current messaging and law enforcement efforts aren’t getting people to change their behaviour sufficiently?
We recommend that positive behaviour change should be encouraged by using clear, concise and consistent communication. And high-impact preventative measures such as mask wearing and physical distancing should be prioritised relative to lower-impact interventions (like surface cleaning and hand washing) when communicating about preventative measures.
There’s also a problem with reach: messages from the government aren’t reaching the population. Given that people are predominantly using news media, government sources should use these avenues more effectively to distribute centralised messaging.
Finally, given the long term behaviour changes required from South Africans, it may be more effective to create an enabling rather than a punitive environment to encourage the adoption of high-impact preventative strategies. This could include the free provision of masks, restructuring the delivery of services to encourage physical distancing (for example, home delivery of medication and telehealth) and empowering community champions, organisations and leaders to encourage these behaviours.
Changing social norms in a short amount of time is difficult, and a one-size-fits all policy is unlikely to have the desired effect. These changes require messaging that is context specific and which resonates strongly with its targeted audience.
Wits experts to speak at international symposium on climate and environmental factors in COVID-19
- Wits University
Symposium coincides with the publication of their article on environmental drivers and the potential seasonality of COVID-19.
Three Wits experts in climate change have been invited to deliver presentations at the World Meteorological Organization (WMO) virtual global symposium that will review the relationship between weather, climate and environmental factors and the spread of COVID-19.
Professors Bob Scholes and Francois Engelbrecht of the Global Change Institute and Professor Jennifer Fitchett from the School of Geography, Archaeology and Environmental Studies, will be part of the panel of experts that will be taking part in the symposium jointly hosted by the WMO and international science partners.
Scholes and Engelbrecht will be presenting on simulations of COVID-19 in South Africa under seasonality, while Fitchett will discuss early research on COVID-19 and climate co-present a poster on ways on improving the stability of projections from models.
Fitchett, Engelbrect and Scholes are also co-authors of an academic article entitled Winter is Coming: A southern Hemisphere Perspective of the Environmental Drivers of SARS-CoV-2 and the Potential Seasonality of COVID-19, published in International Journal of Environmental Research and Public Health. This work is part of their involvement in the COVID-19 Environmental Reference Group (CERG) formed under the auspices of the Department of Science and Innovation.
The coronavirus pandemic continues to spread globally, within a wide range of climates and seasonal and environmental settings.
Environmental conditionsare not the principle drivers of the first wave of the pandemic. Nonetheless, questions remain as to whether factors such as temperature, humidity, air quality and ultraviolet light influence the spread of the SARS-CoV-2 virus and the disease (COVID-19) that it causes.
“It is critical to understand whether meteorological, climatological and environmental factors promote the spread of the disease either outdoors or indoors. This is a pertinent scientific question that is the subject of numerous studies,” said Professor Jürg Luterbacher, WMO Chief Scientist and Director of Science and Innovation.
“COVID-19 is likely to be prevalent beyond the initial pandemic phase for several years. Better understanding of whether it will be influenced by seasonal environmental and weather conditions, as is the case with many other respiratory viruses and diseases, will help inform public health policy and management of the disease in the coming months and years,” said Dr Joy Shumake-Guillemot of the WMO/World Health Organization Joint Climate and Health Office.
The disease originally manifested in the Northern Hemisphere in early to mid-winter, in places with temperate climates, and spread east and west in an initially quite narrow climate band. This could reflect a climate sensitivity, but could just as plausibly reflect trade and human movement patterns.
Some countries currently facing the highest COVID-19 burdens are located in the tropics and subtropics. But there are also increasing case counts in some Southern Hemisphere countries as they move into winter. Whether this is a meteorologically driven phenomenon is yet to be determined.
Similarly, there are concerns about a resurgence in the next Northern Hemisphere winter, but these speculations are based largely on experience with other respiratory diseases which peak in winter and not on firm knowledge of COVID-19 climate sensitivities.
The e-symposium aims to create a forum to review and discuss existing studies in order to inform the state of knowledge that already exists and provide guidance for future research, according to Professor Ben Zaitchik, John Hopkins University and chair of the symposium’s scientific committee.
The symposium was initiated by a team of researchers from Johns Hopkins University, WMO and ACCESS programme in South Africa, and co-hosted by a wide range of scientific partners including the American Geophysical Union (AGU), U.S. National Oceanic and Atmospheric Administration, World Council Research Programme, SENAHMI Peru, International Science Council, Elsevier, FutureEarth, GeoHealth Community of Practice, the Japan Agency for Marine-Earth Science and Technology and the Pacific Science Association .
More than 450 participants will consider some 100 contributions on the topic from researchers from around 20 countries. There will be several keynote presentations, and panels and breakout sessions on understanding dynamics, forecasts and projections, and actionable information.
There will be a concluding statement on the outcomes and the future of research on this aspect of the COVID-19 pandemic. Symposium proceedings will be published by Elselvier OneHealth journal.
The outcomes of the conference will also support the work of a newly established WMO Research Board Task Team on COVID-19 and climate and environmental factors, which will provide official scientific direction on the topic through 2021.
Wits students dominate global supercomputing competition
- Wits University
Despite Covid-19, Wits students won second place with their applications to aide analysis of Covid-19 data in the competition held online for the first time.
Students in the School of Computer Science and Applied Mathematics (CSAM) and the School of Electrical and Information Engineering (EIE), nabbed a well-deserved second place at the 2020 final leg of the International Supercomputing Competition (ISC) Student Cluster Competition.
The Student Cluster Competition is open to all students in South Africa, and to students from universities globally.
The international finals have on average 82 university students from 11 countries competing to reign as world supercomputing champions. Since its inception seven years ago, South African students have dominated the ISC Student Cluster Competition and made it onto the podium in every single leg of the competition.
Here is a brief look at Wits’ track record:
First place awards: 2013, 2014, 2016 and 2019
Second place awards: 2015, 2017, and 2020
Third place awards: 2018
With this heavy legacy to live up to, the Wits teams prepared to dominate in the 2019 leg of the Student Cluster Competition.
The teams consisted of four undergraduate students from the Computer Science and Applied Mathematics (CSAM) and one student from the School of Electrical and Information Engineering (EIE) who spent endless hours in a specially prepared venue provided by TW Kambule Mathematical Sciences Laboratories.
These hard-working students paved the way to the regional finals and were tasked with designing a low budget cluster with a R190 000 budget constrain.
In true Wits fashion the students overcame all obstacles before them and won the regional competitions thrusting them further into the final leg of the country wide competition.
December 2019 saw Wits earn first place by completely dominating the competition and earning a spot in the 2020 final leg of the International Supercomputing Competition (ISC) 2020 Student Cluster Competition.
With the team having earned the right to represent South Africa on the world stage, the Witsies dominated the Centre for High Performance Computing’s (CHPC) national team. However, due to the Covid-19 pandemic the competition could no longer be held in Germany and the international finals were moved online.
The rules of the international leg need each participating country to have 6 members and 2 reserve members. The South African team consisted of:
Michael Beukman (CSAM-Wits)
Guy Axelrod (CSAM-Wits)
Victoria Bench (EE-Wits)
Donald Alungile Tshangela (CSAM-Wits)
Sivenathi Madlokazi (CSAM-Wits)
Mikhail Vink (UWC)
With reserves:
Stephanie Agenbag (UWC)
Kalreen Govender (UKZN)
Moving online meant all the work that went into preparing a cluster for the finals had to be shelved and the team had to adapt to a new focus on a display of skills using the same resources as everyone else.
The virtual stage was prepared and the tasks were given: students had to optimise resource heavy applications that aided with analysis of Covid-19 data in real time and the effects of global warming around the world (Tinker HP and Elmer/Ice respectively).
To make the competition even more exciting the judges threw in two additional challenges to see if the students could adapt to the field’s ever-changing terrain, an advanced coding challenge and the creation of an Artificial Intelligence.
Thanks to the many hours of training with Avraham Bank (teaching and training coach) and the coordination of Brian Maistry (MSS HPC and Cybersecurity coordinator) the Wits students managed to secure a second place finish.
The team acknowledges the support and contribution of the Mathematical Sciences Support team, HoS Professor Raseelo Moitsheki, Dell , CHPC and the Texas Advanced Computing Centre.
Covid-19 Expert Advice #1: How long should I isolate or quarantine for?
- The Scientists Collective
This is the first of a series of expert advisories on how to respond to Covid-19 which will be published from time to time by Maverick Citizen.
This series is co-written by some of South Africa’s leading medical scientists and academics, including some members of the Ministerial Advisory Committee (MAC) on Covid-19. Although not written for or on behalf of the MAC, much of whose important advice is being lost in the corridors of government, it is intended to provide practical life-saving advice based on the best emerging knowledge and evidence of Covid-19.
We are learning all the time, so it is highly likely that advice will change as we learn more about the virus, so keep an eye on any new recommendations. However, the basic principles explained in this series will stand and help inform your decisions.
“If I have Covid-19, how long should I stay away from work and self-isolate from other people?”
“If I have been in contact with someone who has Covid-19, for how long should I quarantine?”
“What should we advise workers, employers and their household contacts?”
It sometimes appears that the public is being given conflicting advice in media interviews, slide sets from the Department of Health that circulate over social media, and differences with guidelines from WHO and other countries. This has led to uncertainty and confusion for the public, employers and healthcare workers about how long we mustisolate or quarantinein relation to Covid-19.
We are a group of clinicians, scientists, and other professionals, many of us Ministerial Advisory Committee members, who are unpacking guidelines to help the public, workplaces, employers and unions, as well as government departments to support a balanced return to relatively normal life as fast as possible while keeping people safe. We have tried to align to guidelines and simplify wherever possible. The scientific references we have relied on are listed at the bottom of this article.
It is highly likely that people reading this will need to isolate or quarantine themselves in the coming months, possibly multiple times, so it is worth trying to understand the reasons for doing so.
Keep in mind:SARS-CoV-2 is the virus,Covid-19 is the disease it causes.
First, the difference between isolation and quarantine, as used here:
Isolationmeans that after you develop symptoms of Covid-19 and/or test positive for the SARS-CoV-2 virus, you need to stay apart from others so as to not spread the virus to them. This includes asymptomatic people who have a positive test.
Quarantinemeans that after you have had a high-risk exposure to Covid-19 (ie, close and prolonged (more than 15 minutes) contact without prevention strategies (eg, wearing of face masks or good ventilation), you need to stop being in contact with people and stay apart. This is in case you have contracted Covid-19 from your initial exposure.
Practically speaking,both isolation and quarantine means separating yourself from others. The difference in how long you need to separate yourself is based on the science.
To summarise the recommendations:
You shouldisolatefor 10 days after the start of suggestive symptoms(unless hospitalised, see below)or testing positive, andquarantinefor 14 days if you are exposed to a high-risk situation.
There is no need for you to test if you are asymptomatic (unless you are being screened as a frontline healthcare worker).
There is also no need to test or retest at the end of quarantine or isolation periods.
Do not rely on a negative test result to say you are safe, especially if you may expose vulnerable people, like the elderly or people with chronic medical conditions or cancer.
Bothisolateandquarantinemean stay at home; get someone else to shop for you if you can; try to keep away from people you live with and avoid all people in case you infect them. Open windows and wear a mask when you can’t avoid being in a space that others will use.
Obviously, quarantine transforms into isolation if you get symptoms. For practical purposes, they mean similar practical steps – stay away from people as best you can!
The 10 and 14 days advice above is a safe and very conservative recommendation, particularly in the case of the isolation guidelines. However, none of these rules are failproof and they may change as new information becomes available. As your best defence, you should continue to:
practise physical distancing
wear of a mask (covering both your mouth AND nose)
avoid crowds
wash hands frequently
wipe surfaces clean.
“Exposures” vary wildly and need some common-sense assessments. We present some case studies at the end, to help understand how much these can vary.
What is the reasoning behind the timelines?
Infection from SARS-CoV-2 starts with exposure to a person who is infectious. If you get infected, there is a period of a few days, called theincubation period(usually 2-4 days, but can be longer) in which you do not show any symptoms. After a few days of symptoms, you become less infectious, and (unless you were very seriously ill) 10 days after symptoms started you are very unlikely to be infectious (even if you still have some symptoms or test positive on the PCR tests, which shows dead virus).
There is greater confidence in the science allowing us to relax the previously used 14-day timeline for de-isolation. For people who do not require admission to hospital, the virus will not grow after nine days from the onset of symptoms, making it very unlikely that it will be able to infect anyone beyond this point. This is why staying away from people for 10 days protects them. The added four days for the 14-day quarantine period includes the incubation time. So, there’s generally no point in repeating tests in people who have had a positive test and are isolating.
In people who don’t have any symptoms and test positive, it is harder to know when infection started. In this scenario we recommend (to keep things simple) 10 days for such people (“asymptomatic infections”).However, please don’t test if you don’t have symptoms! You are wasting precious resources.
Another complication is that very ill people may be infectious for longer, so for them we start measuring once they are well on the road to recovery and off oxygen support. For everyone else, the start of symptoms is fine.
It is useful to start thinking of a clock (a calendar or diary is useful) – and these possible scenarios that will help guide 99% of your decisions:
I am ill with symptoms that may be SARS-CoV-2 (cough, fever, sore throat, loss of smell/taste, etc –see here).
The 10-day clockfor isolationstarts from the day symptoms started.
I am ill with symptoms that may be SARS-CoV-2 and tested positive on day 4 of symptoms. When will I be able to de-isolate?
The 10-day clock still starts from the day symptoms started.
I have no symptoms but I got a test and the result came back positive 3-days later. When will I be able to de-isolate?
Theisolation clockstarts from when you had the test, not when you got the result.
I have been exposed to someone who has tested positive or has been diagnosed with Covid-19, or I was in a high-risk situation (see below) and I am worried.How long should Iquarantinefor?
The 14-day clock starts from the last exposure.
Coming out of isolation or quarantine does not require a test unless you are a frontline healthcare worker (see below). Above all, if you do decide to rely on a test performed in private (the public sector does not perform tests for this reason), then pleasedo not rely on a negative testto say that you are to interact with vulnerable people like the elderly or people with chronic medical conditions or cancer.
The test for SARS-CoV-2, which causes Covid-19
The diagnostic test we use for acute infection with SARS-CoV-2 identifies the genetic material of the virus and is termed a PCR (polymerase chain reaction) test. What we can learn from the commonly available PCR test is surprisingly complicated to interpret. Sadly, it means that we should not rely too heavily on the results because:
If the result isnegative, you can still have the virus – it may be too early or too late (and you are no longer infectious) to detect the virusORthe sample has technical issues when being processed.
If the result ispositive, it means you ARE infected, but confusingly, may not tell if you are infectious or not – as the test detects only one bit of virus (its genetic material), it doesn’t tell us whether that genetic material is sitting within a fully competent virus able to infect other people, or just left-over bits from being killed by our immune system. Indeed, towards the end of symptoms, virus present on PCR testing can’t be transmitted (“replication incompetent’’).
This sounds confusing (and it is), but it is important to understand that a negative test is not the best basis for deciding to isolate or not, or for ending isolation or quarantine.
The SARS-CoV-2 PCR test has been recommended in the past to know you are “safe’’ to return to work (including recommendations in government department guidelines) or to see your elderly parents. As you can tell from the above, this is not a good way to assess your risk, particularly since it can take several days to get test results, is expensive and ultimately proves unreliable if negative.Many countries have started to remove the recommendation for a negative test, appreciating how limited its practical use is.
As presented above, a time-based de-isolation period is much more practical and reliable.
Another testing option involving serology (an antibody-based test) looks at the immune response to the virus rather than the virus itself. The problem here is that it takes days or even weeks to become positive. Furthermore, we do not yet know whether you get effective immunity (protection) after infection with this virus. Immunity may be possible in ways other than with antibodies, but there may be other parts of the human immune response that are important that we are not looking at. Additionally, protection from reinfection after you have had Covid-19 may be partial, temporary or zero – we do not yet know.
At present, this serology test has no role outside of research or surveillance settings. Talk of an ‘’immunity passport’’ is dangerous, in the absence of any reliable test (many appear to become negative again a few months after infection) or clarity whether immunity is even possible (the South African authorities are evaluating these tests).
Immunity
Sadly, we do not yet know whether you get effective immunity from infection with this virus. So, whether you have been diagnosed before, or think you may have had Covid-19 previously, it does not help make isolation or quarantine decisions. This may change,but for now rather think of yourself as having no immunity to a future infection from a previous proven or suspected infection. As mentioned, serology tests are under evaluation, and should not be used to assess your own immunity. The rule is: the clock operates for everyone, irrespective of whether you have had Covid-19 previously.
What is a high-risk exposure?
Hopefully you know this by now, but for the purposes of understanding what constitutes exposure, we need to understand that SARS-CoV-2 is thought to be spread primarily through respiratory particles which are in the air we breathe, or which can land on our eyes, nose and mouth, when we are close to someone who is infected, for prolonged periods (more than 15 minutes), or in front of them (face to face and less than 1-2metres).
The respiratory particles can be transmitted from an infected person who talks, sings, coughs or simply breathes. Barriers such as masks can stop these particles from moving away from a person who has Covid-19, and wind removes them quickly, meaning that being outdoors or in a well-ventilated space, with people wearing masks, is much safer, while being with people indoors or in a vehicle, with closed windows, not wearing masks, all dramatically increase risks. Air-conditioning systems that recirculate air also recirculate infectious particles, making them risky.
Open windows and natural ventilation is best.
An easy way to think about this is to imagine yourself not wearing a mask in a closed room with someone else for 15 minutes. That is considered a significant amount of time in contact with the virus and constitutes a high-risk exposure. If you and the other person are wearing masks, it buys you more time. If the windows and doors are open, it buys you a lot more time. If the person is coughing, talking a lot or singing, these actions significantly increase your risk and cut down the time required for you to contract the virus.
It is possible to get infected in less time than 15 minutes, but is very unlikely. Youwill nothave a significant exposure paying for your groceries, brushing past a runner who is not wearing a mask, or at an outdoor braai or picnic where everyone is standing more than 1m apart between each person.
Youwillbe exposed if you are inside a taxi with closed windows, in an indoor place of worship that is crowded (less than 1m) and where people are singing, in a workplace that has poor ventilation or heaters on, or in a nightclub, for longer than 15 minutes with someone who is infected, and all the more if not wearing a mask.
Why do exposed health workers get different advice?
Health workers are in a difficult position – their work places them in a very high-risk scenario; they are absolutely essential to providing uninterrupted services, particularly in a pandemic; but they also have access to personal protective equipment, which gives some protection from infection, and also reduces the likelihood of them of infecting their patients.
Having them off for 14 days each time after a high-risk exposure would be catastrophic for the health system. As a result, obtaining a PCR test result is prioritised for healthcare workers, despite all its weaknesses. The recommendation here aims to balance all known factors.
Current Department of Health guidelines require health workers who remain asymptomatic seven days after a high-risk exposure to have a PCR test on day eight, which if negative, allows an immediate return to work. We believe that a balance of the science, the pressure on the health workforce, and the safety aspect could allow this to be dropped to a test five days after exposure with return to work if negative, so long as they are extra careful regarding the use of medical-level protective equipment at work.
Common scenarios that people face every day
Finally, here are some common scenarios relating to timing of isolation and quarantine that we encounter day-to-day. All are real cases and the persons involved have given us their consent to use them.
SCENARIO 1
Someone with no symptoms goes to a drive-through testing station. The result is positive. How long do they have to isolate themselves for?
Recommendation
First of all, please stop testing if you do not have symptoms! As explained above, it does not help with decision making. But now we have the test, 10 days from the date of the test.
SCENARIO 2
A woman tests positive after she starts coughing. She self-isolates for 10 days, but on the 10th day her husband, who lives with her, also tests positive. When can she go back to work?
Recommendation
It is likely that she passed the virus to her husband some days before, and that she is now recovering. She can go back to work.
He should isolate and must observe the 10-day isolation from the start of his symptoms (or the day of his test if he has had no symptoms).
The test on him, especially as it probably took a few days to come back, adds almost no value here – he could have quarantined for 14 days from the last close contact with his wife, if she was isolated from everyone except him.
SCENARIO 3
A family of six, with one elderly person, one diabetic, and two children (one aged four, one six), are informed that their domestic worker, with whom they had close contact, is ill in hospital and tested positive for Covid-19. The family enters quarantine but the 6-year-old gets sick and gets tested positive. What should the family do?
Recommendation
The key question here is, how do you protect vulnerable members of the family from a member who is infectious to them? Isolation within family units is often difficult, especially with young children who may not understand physical distancing.
It seems the most effective way to deal with this is to either:
Ideally, quarantine the elderly and diabetic family members (higher-risk persons) elsewhere;
Distance them within the household as much as possible – stay in one room, open lots of windows, and wear masks).
Common spaces such as kitchens and bathrooms should be ventilated as much as possible; wait for some time (30 minutes with lots of windows open) after an infectious person has used these areas, and wipe surfaces.
Flush the toilet with the lid down.
If symptoms develop, watch them closely – any difficulty in breathing should trigger a trip to the hospital.
SCENARIO 4
A couple living with a 2-year-old child all have symptoms and test positive over a period of a week. One partner and the child get better, but the remaining partner has persistent symptoms. The well partner needs assistance with childcare from her elderly parents – when can the two parents leave the house safely?
Recommendation
The 10-day rule above applies.
Even the partner with symptoms (as long as improving) could de-isolate after this period.
But be aware that being elderly is high risk (as is diabetes, hypertension, obesity and HIV, as well as other chronic conditions), and being as careful as practical around the elderly parents seems sensible.
SCENARIO 5
A domestic worker is involved in looking after an elderly man with Covid-19. How long should she quarantine for?
Recommendation
14 days from her last close contact.
SCENARIO 6
Someone at work tests positive. When should the employer test everyone?
Recommendation
Don’t test ANYONE. Assess people’s exposure to the case, and, if significant (see above), quarantine them for 14 days. If not, carry on with the usual precautions.
We have found the first cases are often the wake-up call in the workplace you need, sadly, for employees and managers to take this seriously (tea rooms are notorious for people to relax their guard).
Use the opportunity this case affords to ensure strong adherence to interventions that we know work – physical distancing in the workplace, universal masking, proper hand hygiene, regular cleaning of routinely used surfaces, and checking for symptoms on a daily basis with employees staying home and seeking medical advice, if symptoms develop.
SCENARIO 7
Someone is returning from the US, how long should they quarantine for?
Recommendation
Current SA guidelines forcibly quarantine people for 14 days on return from international flights. This was based on when our epidemic was largely linked to people infected in other countries. It does not make sense now we have such widespread infection.
Air travel in general appears relatively safe, and it is unclear whether local and international travel risks are different (coming from a low-risk area may be safer than coming from an area in SA where the pandemic is raging). These guidelines need updating – but if you want to be supersafe, treat the travel as an exposure and quarantine for 14 days.
*The Scientists Collective:Dr Nomathemba Chandiwana, Professor Francois Venter, Dr Joana Woods, Dr Bronwyn Bosch, Mohammed Majam, all at Ezintsha, University of the Witwatersrand; Dr Jeremy Nel, University of the Witwatersrand, Professor Marc Mendelson, University of Cape Town; Prof Shaheen Mehtar, University of Stellenbosch, Dr Elijah Nkosi, Dr Morgan Chetty, both family doctors; Professor Yunus Moosa, University of Kwa-Zulu Natal; Professor Shabir Madhi, Respiratory and Meningeal Pathogens Research Unit, University of the Witwatersrand; Dr Halima Dawood, University of Kwa-Zulu Natal; Dr Lucille Blumberg, National Institutes of Communicable Diseases; Professor Lucy Allais, Department of Philosophy, Wits Centre for Ethics, University of the Witwatersrand; Professor Glenda Gray, South African Medical Research Council; Professor Andy Gray, Division of Pharmacology, Discipline of Pharmaceutical Sciences, University of KwaZulu-Natal; Dr Angelique Coetzee, South African Medical Association.
The advisory above has taken account of the following published studies:
Wolfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Muller MA, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020.
Liu Y, Yan LM, Wan L, Xiang TX, Le A, Liu JM, et al. Viral dynamics in mild and severe cases of Covid-19. Lancet Infect Dis. 2020;20(6):656-7.
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with Covid-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054-62.
Xu K, Chen Y, Yuan J, Yi P, Ding C, Wu W, et al. Factors associated with prolonged viral RNA shedding in patients with Covid-19. Clin Infect Dis. 2020.
Bullard J, Dust K, Funk D, Strong JE, Alexander D, Garnett L, et al. Predicting infectious SARS-CoV-2 from diagnostic samples. Clin Infect Dis. 2020.
Arons MM, Hatfield KM, Reddy SC, Kimball A, James A, Jacobs JR, et al. Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility. N Engl J Med. 2020;382(22):2081-90.
Lui G, Ling L, Lai CK, Tso EY, Fung KS, Chan V, et al. Viral dynamics of SARS-CoV-2 across a spectrum of disease severity in Covid-19. J Infect. 2020.
Covid-19 Expert Advice #2: Practical guidance on disinfecting
- The Scientists Collective
This is the second of a series of Expert Advisories on how to respond to Covid-19 which will be published from time to time by Maverick Citizen.
This series is co-written by some of South Africa’s leading medical scientists and academics, including some members of the Ministerial Advisory Committee (MAC) on Covid-19. Although not written for or on behalf of the MAC, much of whose important advice is being lost in the corridors of government, it is intended to provide practical life-saving advice based on the best emerging knowledge and evidence of Covid-19.
We are learning all the time, so it is highly likely that advice will change as we learn more about the virus, so keep an eye on any new recommendations. However, the basic principles explained in this series will stand and help inform your decisions.
These are some of the common questions we hear:
“How do I make my workplace or school Covid-19 free after someone tests positive?”
“Should I disinfect my groceries?”
“Should my school use disinfection tunnels? What should I disinfect after my child returns from school?”
“Must I wipe my shoes and wash my clothes after going outside?”
“What should I wipe down when I get in a taxi?”
Fear of contracting Covid-19 has been exploited by companies marketing unnecessary and even dangerous disinfection methods for surfaces, buildings and humans. Even government departments and officials have implemented spraying of outdoor spaces such as in taxi ranks and open streets. This display, often involving suited sprayers, has been called “hygiene theatre”, and can be alarming. At best, these systems are unnecessary and expensive; at worst, they are harmful to human health, the ecosystem and environment, and are ineffective in Covid-19 control.
Here, we try to give clear and practical advice, based on the latest evidence, that allows you to be as safe as possible. More detailed references are listed at the end if you need more guidance.
First, some basics:
The risk of being infected by the virus from touching surfaces is still not fully understood. Scientists believe it contributes less to your risk than being exposed to other humans in crowded environments. Physical distancing, ventilation, wearing masks, hand-washing, isolating if symptomatic, and being outdoors as much as possible (which is highly effective at diluting the virus) when you interact with others, are where you should focus energy – seehere.
The virus is very fragile. It does not need strong, dangerous chemicals to kill it – simple exposure to soap and water (for 20 seconds) breaks down the virus membrane very effectively, and kills it. In addition, sunlight and heat can kill this virus – which means if you must socialise, do so outdoors.
There is NO role for “fogging”, “disinfection tunnels”, spraying or “deep cleaning” for Covid-19. These are heavyweight options we occasionally use for other bugs (we don’t use tunnels anywhere!), and in very specific situations, but not for this virus.
Many people have seen studies showing that the virus can live on surfaces like metal and plastic for a long time. However, these studies used large amounts of virus (the equivalent of someone coughing on a surface repeatedly at close range), and even then, it has not been established that the virus can infect you via this route. However, scientists think it is probably a route of spread by touching your face after touching a surface, and is less than with respiratory transmission.
All this being said, it seems sensible to avoid or clean surfaces that may be contaminated (and there are lots of other bugs that can be transmitted this way, so this could have other benefits, and does no harm).
For surfaces you should be suspicious of – high-touch ones like door handles, rails, lift buttons, counters, common work tables – wipe away dirt first, then apply a soapy water mix, which “cleans and disinfects”, and allow 20 seconds for the virus to be killed. It is important to wipe away dirt, especially organic matter, as it inactivates soap’s action.
Avoid using shared utensils or cutlery, or anything else, without wiping them down with soap and water first. Wipe your cell phone down every so often, and try not to share. Make it easy to throw away used tissues, paper towels and other waste into a bin.
Note that our advice relates to SARS-CoV-2, the virus that causes Covid-19. Other bugs have different approaches when on a surface, and often need more effort.
There is a host of terms in the infection control field, including decontamination, disinfection, detergent, antiseptic, and cleaning, some of which we have listed at the end if you are interested, but they can be confusing, and it’s unnecessary for understanding how to keep yourself safe from SARS-CoV-2.
So, it is not that hard, and being sensible goes a long way: In summary, wipe away dirt before applying with a soapy water mix (“clean and disinfect”), to surfaces you are suspicious of – high-touch ones like door handles, rails, lift buttons, counters, common work tables – and allow 20 seconds for the viral membrane to dissolve. It is important to wipe away dirt, especially organic matter, as it inactivates soap’s action.
Which soap should I use?
Any hand soap and nearly all kitchen detergents will do an effective job. If the soap makes oil dissolve – whether on your hands, on your dishes, on the floor – it will dissolve the oil-based membrane around the virus, if in contact with it for 20 seconds or more. The recommendation for hand-washing and for surfaces is the same – give the soap enough time to work.
While alcohol-based sanitisers (at least 70% alcohol content) are more convenient (because they dry quickly on your hands)they are actually less efficient than soap and water at killing the virus.So don’t waste them on surfaces unless you want rapid drying, and only use them on your hands if you can’t access soap and water, and only if any obvious dirt is removed and your hands are dry. Soap and water, other alcohol-based solutions, and diluted chlorine and hydrogen peroxide-based liquids are effective for wiping down surfaces. Spray onto a cloth first then wipe.
How often should you clean?
Just be sensible – this depends on how busy the area is. Of course, you want to clean things more often if there is a lot of people traffic, someone in the area is coughing and sneezing, or where people are singing, shouting or talking, or in a high-risk area like a health facility. A taxi would benefit from wipe downs of seats and handles between trips (and ensuring everyone’s hands are sanitised), a shopping counter or credit card machine every so often. For anything left unused overnight, cleaning is not necessary at all.
Otherwise, routine daily cleaning can proceed as usual. Remember “cleaning” means using a detergent and water, and mechanical action. Disinfection is killing the microbe, but only works after cleaning has taken place because many disinfectants get inactivated in the presence of organic matter.
How extensively should you clean?
As above, it is unclear whether anything except the most frequently touched areas are risky (and even then, we are not 100% sure, but it seems sensible to be cautious). Simply allowing time and air movement to dry and dilute the virus out will naturally disinfect rooms,so there is no need for “misting” or “fogging” (which often uses dangerous chemicals).Wipe the common surfaces with soap and water, open all windows, and let nature take care of the rest.
There is no reason to “deep clean” or shut down buildings,especially where windows can be opened. If you want to err on the side of caution, wipe down surfaces, open the windows, and leave for two to three hours, although even this is almost certainly unnecessary.
Practically, what should happen at my gym, school, mall or place of employment?
Most important is to open windows and doors, add a fan if you don’t have windows on two sides, avoid crowding, wear masks, encourage sick people not to come to work, and send sick people home immediately – seeherefor symptoms. Then, encourage hand washing or sanitising (so as to limit contamination of the commonly touched surfaces), supported by having sanitising stations wherever possible. Physical distancing remains important and regularly cleaned perspex screens may be useful at reception counters or between desks.
Next, identify common-touch areas (and consider highlighting them with signs, to prompt people to not use them unnecessarily), and identify them for regular wipe-downs; in very high traffic areas, half-hourly may be needed, but less often is probably fine in most cases. Occasionally, it may be wise to wipe after every use – in the case of gym equipment, for instance.
Once an area is left overnight, it is very unlikely to have sufficient virus on any surface to infect anyone. Ensure that cleaning staff have access to gloves and masks as some disinfectants can be toxic to the skin. Be considerate of waste workers and waste pickers, and secure higher-risk waste, like tissues, in closed bags.
Laundry is a common question
As above, the amount of virus on clothing is extremely unlikely to be significant, unless the person wearing them has the virus (and even then, it’s unclear this will allow transmission) or someone near you has been singing, talking or coughing for more than a few minutes (which should never happen, if you do effective physical distancing). Even if contaminated, leaving laundry overnight, or washing (the dilution, detergent and heat of laundering will take care of the virus; cold-water laundering less so, but still very effective with soap) will solve this, but is an overreaction and unnecessary. The likelihood of Covid-19 being spread on shoes, as with laundry, is very low; if you have crawling kids, maybe put them somewhere safe.
Masks need a special mention
They are warm and moist all day, and you may unknowingly have the virus and be coating it all day long. This may be the one place to err on the side of caution, and launder daily. Always wash your hands after handling your mask and try keeping it on one particular spot (again minimising any potential risk of transmission to surfaces if you are shedding Covid-19 virus). Like with other clothes, have several, so some are being washed, or kept in convenient places.
The cause ofrisk in public toiletsis probably poor ventilation more than contaminated surfaces, so again, opening windows is probably the most important. Encouraging soap and water within public toilets is relatively easy, and closing the lid before flushing (to avoid generating an aerosol; there is some concern that faeces may be infectious) may reduce the need for wiping down surrounding surfaces.
Again: no fogging, misting or deep cleaning is required.The chemicals usually used with these cause skin and lung reactions, and are no more effective than soap and water for this virus.
Gloves are unnecessary for prevention of transmission, also need regular washing as per your hands, and may give you false reassurance – rather focus on getting soap and water on your hands regularly.
Fancy equipment, like UV lights, can be expensive and can harm your eyes; they may have a role in health facilities in special situations, but really have no role outside of these. Remember that sunlight is an excellent source of free UV light.
“How do I make my workplace Covid-19 free?”
Get the basics right – physical distancing, open windows and doors, masks, hand-washing are most important. Wipe common-use surfaces regularly. Encourage ill employees with Covid-19 symptoms to immediately go home and isolate – seehere.
“Should I disinfect my groceries?”
The amount of virus, even if contaminated, is unlikely to pose any threat. If you’re worried, sanitise your hands before and after handling the groceries, rather than wiping down each item. Leaving groceries overnight will likely disinfect them automatically anyway.
“Should my school use disinfection tunnels? What should I disinfect after my child returns from school?”
Disinfection tunnels may harm your child (or you for that matter), and should not be installed anywhere. For school bags, laundry and textbooks – see above, but again very unlikely to be a source of infection. Rather focus energy on educating the child regarding the basics about viral transmission.
“Must I wipe my shoes and wash my clothes after going outside?”
Unless someone was coughing on you, or singing or talking for prolonged periods, no. And you probably have a far, far greater risk of having breathed in droplets at the time, rather than getting it later from your clothes.
“What should I wipe down when I get in a taxi?”
Masks and open windows, and trying your best to distance yourself are your primary defence here. Sanitise your hands on getting in or out, and try not to touch common surfaces.
Definitions
A few essential definitions are shown below to clarify concepts and misuse of frequently used words, sometimes interchangeably, without a clear understanding of the meaning.
Antiseptic:a substance that prevents or stops the growth or action of microorganisms by inhibiting their activity or by destroying them. The term is used especially forpreparations applied topically to living tissuesuch as 70% propyl, isopropyl and ethyl alcohol (ethanol) with 2% emollient, povidone iodine (no longer recommended) and chlorhexidine 2-4%.
Cleaning:the physical or mechanical removal of foreign material (e.g., dust, soil) and organic material (e.g., blood, secretions, excretions, microorganisms). Cleaning physically, generally removes rather than kills microorganisms. It is accomplished with water, detergents and mechanical action.
Contact time:the time that a disinfectant must be in contact with a surface or device to ensure that appropriate disinfection has occurred. For most disinfectants, the surface should remain wet for the required contact time.For SARS-CoV-2, it takes 20 seconds to dissolve the membrane.
Contamination:the presence of any potentially infectious agent on items such as environmental surfaces, clothing, bedding, surgical instruments or dressings, or other inanimate articles or substances including water, medications and food.
Detergent:a synthetic cleansing agent that can emulsify and suspend oil. Contains surfactant or a mixture of surfactants with cleaning properties in dilute solutions to lower surface tension and aid in the removal of organic soil and oils, fats and greases.Effective against coronaviruses.
Decontamination:a process for rendering medical or other devices safe for reuse on the same or another patient. It includes thorough cleaning, and disinfection or sterilisation depending on the device’s heat tolerance.Disinfection is a part of decontaminationand these two terms should not be used interchangeably.
Disinfection:athermal or chemical processfor inactivating microorganisms on inanimate objects.
High-level disinfection:kills all microorganisms, with the exception of small numbers of bacterial spores. Used for endoscopes and heat-labile equipment.
Mid-level disinfection (also intermediate-level disinfection):kills inactivated vegetative bacteria, including mycobacteria, most viruses, and most fungi, but might not kill bacterial spores. Used for large areas of contamination such as blood spills.
Low-level disinfection:inactivates most vegetative bacteria, some fungi, and some virusesincluding enveloped viruses, in a practical contact time, but does not kill more hardy viruses (e.g. non-enveloped), bacterial genus (e.g. mycobacteria), or bacterial spores. Used for surface disinfection after cleaning.Effective against coronaviruses.
Disinfectants:Chemical compounds that inactivate (i.e. kill) pathogens and other microbes and fall into one of three categories based on chemical formulation: low-level, mid-level and high-level.Disinfectants are applied only to inanimate objects.All organic material and soil must be removed by a cleaning product before application of disinfectants. Some products combine a cleaner with a disinfectant.
Fogging:(fumigation, misting) Dispersing a liquid chemical disinfectant to disinfect environmental surfacesin an enclosed space.Fogging is sometimes indicated after an infectious patient with a highly resistant pathogen (e.g.C difficile),has been discharged and terminal cleaning has been completed. Fogging is to be carried out in a completely empty room with no humans, furniture or obstruction. The room is ready for use after a couple of hours, depending on the contact time.NOT recommended for coronaviruses.
Healthcare areas (also known as patient care areas):patient zones and the surrounding healthcare environment within inpatient (e.g. general wards, specialised wards, patient rooms) and outpatient settings (e.g. examination areas, patient toilets). This area should remain as clean and dry as possible.
Routine cleaning:the regular cleaning (and disinfection, when indicated) of the patient area to remove organic material, minimise microbial contamination and provide a visually clean environment. The frequency of cleaning is determined by indication, butshould be at least once a dayin the absence of an outbreak.
Terminal (discharge) cleaning: (deep cleaning)cleaning and disinfection after the patient is discharged or transferred, and includes the entire healthcare area.This does not apply to an office area or a gym or school or other work space, where deep cleaning has no place.The removal of organic material and significant reduction and elimination of microbial contamination to ensure that there is no transfer of microorganisms to the next patient.The room can be occupied as soon as terminal cleaning is completed and ready to accept the next patient.
Authors: Prof Shaheen Mehtar, University of Stellenbosch; Dr Nomathemba Chandiwana, Prof Francois Venter, Dr Bronwyn Bosch, Celicia Serenata, Dr Esther Bhaskar, Dr Joana Woods all at Ezintsha, University of the Witwatersrand; Prof Wolfgang Preiser, University of Stellenbosch; Prof Lucy Allais, Department of Philosophy, Wits Centre for Ethics, University of the Witwatersrand; Prof James McIntyre, Anova Health Institute; Professor Shabir Madhi, Respiratory and Meningeal Pathogens Research Unit, University of the Witwatersrand; Dr Aslam Dasu, Progressive Health Forum; Prof Lucille Blumberg, National Institute of Communicable Diseases (NICD); Dr Jeremy Nel, University of the Witwatersrand, Prof Marc Mendelson, University of Cape Town; Dr Elijah Nkosi, Prof Morgan Chetty, both family doctors; Andy Gray, Division of Pharmacology, Discipline of Pharmaceutical Sciences, University of KwaZulu-Natal; Prof Yunus Moosa, University of Kwa-Zulu Natal; Prof Eric Decloedt, Division of Clinical Pharmacology, Stellenbosch University; Prof Jantjie Taljaard, University of Stellenbosch
References used in this advisory:
MMWR/ April 24, 2020/ Vol 69/ No 16. US Department of Health and Human Services/ CDC
WHO. Cleaning and disinfection of environmental surfaces in the context of Covid-19 Interim guidance 15 May 2020. WHO/2019-nCoV/Disinfection/2020.1
PAHO. The use of tunnels and other technologies for disinfection of humans using chemical aspersion or UV-C light PAHO/CDE/CE/Covid-19/20-0012
AFRICA CDC, AND PREVENTION AND THE INFECTION CONTROL AFRICA NETWORK. Position statement. The use of disinfection tunnels and disinfection spraying of humans. May 2020
NDOH. Covid-19 disease: Infection Prevention and Control Guidelines, version 2, May 2020
WHO (2019)Implementation manualto prevent and control the spread of carbapenem-resistant organisms at the national and health care facility level
Guidelineson Core Components in Infection Prevention and Control, WHO, 2016.
NDOH. Covid-19 Disease: Infection Prevention and Control Guidelines Version 2 May 2020
Covid-19 NATIONAL PUBLIC HYGIENE STRATEGY AND IMPLEMENTATION PLAN (draft) Version 2- May 2020
Goldman E. Exaggerated risk of transmission of Covid-19 by fomites [published correction appears in Lancet Infect Dis. 2020 Jul 30;:]. Lancet Infect Dis. 2020;20(8):892-893. doi:10.1016/S1473-3099(20)30561-2
Covid-19 Expert Advice #3: Testing for Covid-19? All you need to know about antibody tests
- The Scientists Collective
The third in a series of expert advisories on how to respond to Covid-19 which will be published from time to time by Maverick Citizen.
This series is co-written by some of South Africa’s leading medical scientists and academics, including some members of the Ministerial Advisory Committee (MAC) on Covid-19. Although not written for or on behalf of the MAC, much of whose important advice is being lost in the corridors of government, it is intended to provide practical life-saving advice based on the best emerging knowledge and evidence of Covid-19. We are learning all the time, and it is highly likely that advice will change as we learn more about the virus, so keep an eye on any new recommendations. However, the basic principles explained in this series will stand and help inform your decisions.
These are some of the common questions we hear:
“Should I ask for a Covid-19 antibody test?”
“What is the difference between an antibody test and a PCR test?”
“Should I have a rapid diagnostic test?”
“If I have antibodies, does that mean I am safe from getting Covid-19 again, and do I still need to wear a mask, socially distance and take other precautions against Covid-19?”
South Africa has seen a flurry of controversies about the possible role and place for antibody tests – also referred to as “serology” tests – in managing Covid-19. Some have argued that antibody tests are themissing weapon, while others have countered that they provide little to no real-timevalueor are a “blunt stick”, offering false hope. Here, we try to help you unpack what is going on, when antibody tests might be helpful to you, your doctors, scientists and policy leaders in South Africa’s response to Covid-19… and when they won’t be of help.
The bottom line:
“Should I ask for a Covid-19 antibody test?”
Sorry, no, don’t use antibody tests, not yet at any rate. It becomes positive too late after getting sick to really be useful, and even the “it’s nice to know I was infected’’ is limited as the test becomes negative quite quickly. Better tests, and combinations with other tests may make them more useful with time, but some of the limitations are unlikely to be overcome ever.
They have a place in research studies, but don’t waste your money for now.
Some basic facts about antibodies:
Antibodies are proteins that are produced by the human immune system in response to an infecting pathogen, in this case, the coronavirus SARS-CoV-2, the cause of Covid-19. Their job, along with other parts of the immune system, is to identify coronavirus and get rid of it from the body. Antibody tests detect the presence of these antibodies in our blood (or less commonly, other body fluids).
The production and appearance of antibodies is the end product of a complex process involving many cells, signals and messages of our immune system that takes time to develop after coronavirus infection occurs. Therefore, when the virus first infects us and causes many of the symptoms that we now recognise in the first 7-10 days, antibodies are nowhere to be seen.
There are two main antibody types which appear and disappear at different time points:
IgM antibodiesstart to appear first, usually ~7-10 days after infection with coronavirus and disappear again after weeks to months;
IgG antibodiesappear second, usually ~2 weeks after infection with coronavirus, and usually persist for longer, in some infections, lifelong.
This is important because some antibody tests look for both IgM and IgG antibodies in blood, and will, therefore, be positive earlier than those antibody tests that just look for IgG antibodies. So, which test and the timing of that test is important in understanding a result.
Antibodies do their job by binding to specific parts of the virus. Some of these parts are critical for the virus to cause the damage it does and therefore by binding such a specific, important part of the virus, those antibodies will neutralise the virus’ damaging effects.
We call these “neutralising antibodies” and if they are present, it tells us firstly that the person has had coronavirus infection previously (they wouldn’t have been produced if the person hadn’t been infected in the first place), and it indicates that if that person was to encounter coronavirus again, if those antibodies were still there, then a level of protection is likely. These neutralising antibodies are what we hope will be generated when we vaccinate people against Covid-19. If they are, then that vaccine will have induced “protective immunity” in that person.
Other antibodies recognise and bind to proteins of the virus which are not critical for it to do its worst and these antibodies do not generally neutralise the virus, and are therefore referred to as “non-neutralising antibodies”. Their presence merely tells us that the person was infected previously with the coronavirus, but doesn’t tell us if they will have any level of protection should re-infection occur.
“Can the Covid-19 antibody test tell me that the symptoms I have now are caused by Covid-19?”
We have already seen that antibodies only start to appear in blood after the first week of infection, and only meaningfully from ~10-14 days. The symptoms that we get with Covid-19 – fever, cough, shortness of breath, sore throat, loss of taste and/or smell, fatigue, muscle pains etc – generally only occur during the first week to 10 days, ie, when antibodies aren’t around yet, so in this case, an antibody test is of no use to you.
The test you need in this setting is called a PCR that is able to flag the coronavirus itself in a sample taken from your nose. We know that the presence of symptoms correlates with presence of the coronavirus which are at its highest levels during the symptomatic period.
This is the test you need if you need to diagnose acute Covid-19 infection.
There is one known exception to the rule that antibody tests are no use for diagnosing Covid-19 during the acute infection. Very rarely, children may have a form of Covid-19 called “multisystem inflammatory syndrome in children” (MIS-C), during which PCR is negative but specific antibodies may be positive. We are still trying to understand why this is so.
“Can the Covid-19 antibody test tell me whether I have had Covid-19 in the past?”
Unfortunately, the answer is “maybe”. Think of it like this – for the antibody test to be positive a certain amount (level) of them needs to be present in blood. That amount depends on two main things:
How strong your antibody response is: We know that the level of antibody response you make is dependent not only on you as an individual (everyone is slightly different), but also on how severely you had Covid-19. The people who have the highest levels of antibody, and therefore most likely to test positive, are those who have had the most severe illness. Therefore, people with Covid-19 who have pneumonia and are admitted to hospital will generally have higher antibody levels in blood than someone who had mild symptoms treated at home, who in turn would have higher antibody levels that someone who had no symptoms at all, ie, asymptomatic (about 30-40% of infected with coronavirus). So people who have had asymptomatic infection or very mild Covid-19 may not mount a great enough antibody response for the test to register as positive.
At what time point the blood was taken for the antibody test:As we have seen above, antibodies only start to appear in blood after symptoms are getting better, so if you take the test too soon, then they may not be at a high enough level to register as positive. In addition, the information that we currently have on how long antibodies to coronavirus last in the blood only goes up to six weeks, and we think thereafter, they may wane. Hence, we can’t say with any certainty at this point whether or not the symptoms someone had over a month ago are due to Covid-19.
“But if my test result comes back positive, surely that tells me that I definitely had Covid-19 and that would help?"
Again, the somewhat disappointing answer is “no”, sorry. It is possible to have a “false positive” result, which means that the antibody that is being picked up by the test is one that looks very much like the SARS-CoV-2 but isn’t that virus. An example of such a “cross-reaction” would be to one of the four other coronaviruses that are known to be a cause of the common cold.
Hence, a positive antibody test result does not reliably prove prior SARS-CoV-2 infection.
“If I have a positive antibody test, does that mean I am protected from getting Covid-19 again?”
Once again, the answer to this is a cautious “maybe”.
Remember our earlier discussion about neutralising and non-neutralising antibodies? If the antibody test that you take is designed to pick up neutralising antibodies (the best ones are against the “spike protein” and the “receptor-binding domain”) which we know are protective, then if you have a positive test, as long as those antibodies remain in your blood, we think that you will have good protection. However, we have also just discussed the fact that antibody levels might decline over time, so that as they wane, you may lose that protection.
However, if the antibody test picks up non-neutralising antibodies, then having a positive test tells you nothing about whether you have protection or not.
Saying this, a further layer of complexity is brought in as we now understand that antibodies are not the only part of the immune system that could protect us against repeated coronavirus infection. Some of those cells, which form part of our complex immune system – T cells – are implicated in protection. What this means is that if you have had Covid-19 diagnosed by a PCR test when you were sick, but your antibody test later on is negative, you may still be protected. Sadly, there is still much to learn.
“If I have a positive antibody test, do I still need to wear a mask, socially distance and take other precautions against Covid-19?”
Absolutely!
For all the reasons we’ve discussed, at the current time with the tests we have, a positive antibody test result must not be misinterpreted as proof of immunity. Do not reduce or abandon protective measures – you may not be protected yourself and it is possible (however, unlikely from our current experience) that you can become infected again, and infect others!
“So is there anything that antibody tests could be used to help us with the pandemic?”
With all the caveats around tests being falsely negative if antibody levels have dropped or if the response of our immune system was too low in the first place, antibody tests may give us useful information about the level of coronavirus infection at a population level. We call these “seroepidemiology” studies (“sero” – indicating the sample comes from blood, and “epidemiology” being the study and analysis of distribution of a disease).
Seroepidemiology studies can be undertaken across the entire country, in certain provinces or districts, or certain groups at high risk of infection, eg, hospital patients and staff, residents and staff of old age homes, prison inmates and staff etc. The information that they give us can be even more useful if we repeat the studies at future time points which gives us trends over time. Another use would be for community surveillance, eg, looking at settings where infections have occurred recently, to evaluate “hotspots” of coronavirus transmission, and to help reconstruct chains of transmission within the community or specific groups.
Antibody tests are an important tool in understanding whether the vaccines that the world (South Africa included) is developing against the Covid-19 work. After we vaccinate someone, we wait and test for an antibody response (especially the production of neutralising antibodies) over many time points. This tells us whether the vaccine induces protective immunity, ie, whether it works, and for how long and at what level those antibodies stay in the blood.
Ideally, what we want to see are high levels of neutralising antibodies that remain over time. Lifelong would be first prize!
“What’s this rapid diagnostic test (RDT) I’ve been hearing about? Is that an antibody test and is it any better than antibody tests that have to be performed in a laboratory?”
The use of the term “rapid” in this context indicates that the result is available sooner than those that have to be sent off to a laboratory, as most often, RDTs are performed at the point-of-care, ie, at your doctor’s clinic or by you in your own home.
The same problems and restrictions in interpreting RDTs for antibodies apply as for laboratory tests. RDTs do not pick up antibody levels in blood sooner or more reliably. In fact, most of the RDTs that have been produced so far seem to perform worse than laboratory-based tests, ie, thesensitivity(ability to pick up the antibodies) of the test is lower.
However, while we are on the topic of increasing the speed of tests to give us an answer, future diagnostic developments may well see faster diagnostic tests targeting the virus itself. New versions of tests similar to PCR (some are in use in other countries but very expensive and with doubtful reliability) or for viral protein (antigen). Antigen tests, (not to be confused with antibody tests!) in common with the PCR, detect coronavirus in samples from the airways so they can diagnose acute infection. They can be simple to perform and cheap but sensitivity remains an issue, which is problematic for a diagnostic test.
“What should I do while waiting for the test results?"
If you are ill with fever, cough, etc – isolate yourself!
Our expert advice is based on what is known about the topic currently and is largely aligned with national policies. We will have to watch the rapidly growing body of data to update it should significant new findings emerge.
Professor Lucille Blumberg, National Institutes of Communicable Diseases; Professor Diana Hardie, University of Cape Town/NHLS Groote Schuur; Professor Marc Mendelson, University of Cape Town; Professor Shaheen Mehtar, University of Stellenbosch / Infection Control Africa Network (ICAN); Professor Wolfgang Preiser, University of Stellenbosch / NHLS Tygerberg; Professor Wendy Stevens, University of Cape Town/NHLS Priority Programmes; Professor Francois Venter, Ezintsha, University of the Witwatersrand.
Accounting, governance and integrated thinking
- School of Accountancy
Special Report by the Wits School of Accounting on how companies should manage the Covid-19 pandemic.
Companies are faced with unprecedented challenges to their business models, governance systems and financial viability.
According to Mervyn King, Honorary Professor at Wits, not since the emergence of democracy in the early 1990s have we seen anything close to the levels of economic, political and social uncertainty being faced by organisations, their employees and society in general.
This is not the first time that the world has been threatened by dangerous diseases. The archaeological evidence points to numerous outbreaks in the ancient world.
The Black Death claimed millions of lives in Medieval Europe. The Great Plagues of Marseille (1720s) and Russia (1770s), the Philadelphia Yellow Fever (1790s) and American Polio Epidemic (1910s) have been well documented. Spanish influenza is thought to have killed up to 500 million people in the early 20th century while, since its discovery in the 1980s, HIV continues to pose a severe health threat, especially in the developing world.
‘Fortunately, the fatality rate for Covid-19 is relatively low, but the impact which it has had on the health care system, the global economy and individual families is astounding. It is the most recent global health disaster in living memory and a stark reminder that we cannot continue with an attitude of “business as usual”,’ King says.
While governments enforce lockdowns and scientists grapple with the development of a vaccine, the business community must mobilise to accelerate progress on achieving the sustainable development goals outlined by the United Nations.
“Covid-19 has confirmed the vulnerability of business models grounded in a short-term pursuit of financial gain. An integrated thinking mindset is required to balance economic, environmental, and social imperatives for the benefit of an organisation and its stakeholders - not only the providers of financial capital,” King adds.
This report provides some interesting ideas to help companies with the application of integratedthinking. It touches on important areas on which those charged with an organisation’s governance should be focused. These include technical issues related to financial statements, assurance engagements and tax relief.
A brief and easy-to-understand explanation of integrated thinking is also provided with recommendations for boards of directors.
Pandemic underscores burden women carry doing paid and unpaid reproductive labour
- Odile Mackett
Women’s extended working days have become normalised, despite the adverse effects on their progression within the labour market and general well-being.
Debates about women’s unpaid reproductive labour have been going on since the first woman received cash for her services. Reproductive labour includes cooking, cleaning, and caring for the elderly, the sick and children.
It’s important to make the distinction between paid and unpaid reproductive labour. Paid reproductive labour is performed in exchange for money or a wage. Unpaid reproductive labour is done for free, and usually for the household in which the individual lives.
This reproductive work has traditionally been undervalued by both formal and informal institutions in societies, whether paid or unpaid.
As paid reproductive workers, women often find themselves in occupations that are highly feminised. These are jobs which consist of a large percentage of female workers, such as work in domestic service, health care or clerical work. This is either because those are the only types of jobs available to them or because their ‘skill set’ is said to be conducive for that type of labour. These types of occupations also tend to be lower paid and more insecure than other occupations.
As unpaid reproductive work, on the other hand, the work of women has gone widely unnoticed and is excluded from things such as the calculation of a country’s gross domestic product (GDP). Even though the calculation of GDP is said to consider goods produced within the home, quantifying the value of goods produced for use within the home is still a challenge for statisticians.
The production of goods and services within the home has typically been carried out by women, as girls and boys are socialised about their respective roles within the household from a young age. As women entered formal paid employment, many thought (as per the prescriptions of traditional economic theory) that the reproductive labour burden would equalise between men and women. But this didn’t happen.
The gap between men and women in paid and unpaid work remains vast, and women who are in paid jobs often still perform these duties in addition to their wage labour. Women are estimated to spend up to five hours a day more on unpaid reproductive labour than men. To cope with these responsibilities, these tasks have increasingly become ‘outsourced’ to people who live outside the household. Examples are employing a domestic worker to clean, employing a nanny to care for children, or ordering take-aways rather than cooking in the home.
Even where these tasks are performed outside the home, women may be left to pay for them or ‘manage’ the employees who perform them.
Women’s extended working days have thus become normalised, despite the adverse effects this has on women’s progression within the labour market and their general well-being.
The COVID-19 pandemic has forced a fresh look at this state of affairs. It has shone a light on the impact that poverty, inequality and unemployment have on people every day. This includes the hardships women face and the burden placed on them to manage responsibilities on a daily basis.
Drivers
Some of the reasons women have been adversely affected by the current pandemic include the fact that health workers and other essential service workers are disproportionately female. In addition, women are more likely to be employed in insecure jobs.
An underestimated problem is the fact that the institutions to which women traditionally outsourced their domestic duties have been closed down to prevent the spread of the coronavirus for extended periods. Domestic workers and nannies have been sent home, and schools, restaurants and fast food outlets have been closed.
As a result, all these services have had to be performed within the household.
This has worsened existing inequalities between men and women. In countries like the UK and the US, women have started spending more time than men on childcare and home schooling, but have also been more likely to lose their jobs as a result of business closures.
In South Africa, more than half of women reported that they were temporarily absent from work during the lockdown. Men have not been as severely affected. Women have also been more likely to lose their jobs than men. The loss was more likely if the individual had lower levels of education or was employed in the informal sector.
In addition, a greater percentage of women compared to men reported living with at least one child, and women also tended to have more children in the household compared to men. This has resulted in more time spent on childcare, whether they remained in employment or not.
This pandemic has thus highlighted how important the work of women is to the ongoing functioning of our society. Women are currently saddled with the ongoing education of the future workforce of the country while schools gradually reopen. They are also more likely to be doing the cooking, cleaning and caring in the home. Or they are managing whoever is being paid to do it instead.
This again highlights the need for governments to take a gendered approach in policy deliberations for relief during and after the pandemic. Numerous recommendations have been made including the provision of basic social protection to informal sector workers – many of whom are women – and ensuring women are adequately represented in discussions related to relief measures.
Now is the time to lay a firmer school maths foundation
- Craig Pournara and Lynn Bowie
Covid-19's lockdown leads maths scores particularly being badly affected but a return to core concepts could be the answer to a pre-pandemic problem.
In South Africa, when Grade 9 learners return to school after the COVID-19 closures, they will have a maximum of 76 teaching days left in 2020. But given the safety requirements and the limited infrastructure in most schools, it’s highly unlikely that they will be able to attend school every day. This means the average Grade 9 learner in 2020 is likely to have less than half of a normal year’s time in class.
While learners in schools for the middle class and independent schools have had access to online learning, learners in schools for the poor and working class have had no such access. And this is unlikely to change in the near future.
There is evidence that, in mathematics, learners in less well-resourced schools are four years behind their counterparts in well-resourced schools by the end of Grade 9. It is therefore likely that most Grade 9 learners will fall further behind in 2020.
This situation needs urgent attention. It is time to think beyond 2020, and to treat 2020 and 2021 as a continuous learning opportunity. It’s also time to be more strategic about what is taught. In the COVID-19 discussions on schooling there has been too little focus on what learners will learn – whether at school or at home.
Indications from research conducted after the Pakistan earthquakes of 2005 showed that, although learners in the affected areas had only a three-month break from school, four years after the earthquake they were 1.5 years behind their peers. In South Africa, most Grade 9 learners will have been at home for about five months due to the COVID-19 pandemic before they return to school.
A curriculum that does not adapt to learners’ levels may leave them further and further behind. The need to prevent this has led to calls to “build back better” after the COVID-19 pandemic. Evidence suggests that the way to do this is to focus on core concepts and identify what learners need to know but may have missed or forgotten.
The legacy
After Grade 9, South African learners must choose between Mathematics and Mathematical Literacy for the remaining three years of secondary school. Mathematics is essential for entrance into science-based programmes in universities, but the majority of learners lack the knowledge to cope with Mathematics from Grade 10 onwards.
For example, in the Annual National Assessments for Mathematics, administered from 2012 to 2014, the average mark each year for Grade 9 was less than 14%. Similarly, in the Trends in International Mathematics and Science Study assessments in 2015, only one third of South African Grade 9 learners achieved at the minimal level in mathematics. A recent study of Grade 9 and 10 learner performance on negative number, basic algebra and functions yielded an average score of 28.3%. Clearly Grade 9 performance is far below desired levels.
Add to this situation the impact of the COVID-19 pandemic. In most state schools, Grade 9s are scheduled to return to class on 24 August 2020. Research indicates that long breaks from school lead to learning loss, with maths scores being particularly badly affected. And these breaks have a greater negative impact on learners from lower socioeconomic groups.
A US model based on studies of the known effects of long breaks suggests that learners in the US could end the school year with only 37%-50% of the average gains they would have made in a normal school year in mathematics.
What’s needed
We suggest the solution to the pandemic interruption of learning is to identify a limited number of core concepts and skills for Grades 8 and 9 that will provide a strong foundation for further mathematics.
This involves, firstly, a carefully designed curriculum to address learners’ difficulties, starting with whole number, fractions, negative number, introductory algebra, linear patterns and functions.
Secondly, teachers need a range of supportive materials – not just fixed lesson plans. It should be clear what must be done face-to-face and what can be done alone at home without technology. Teacher materials should help to identify gaps in learners’ knowledge and to provide guidance for re-teaching what learners have missed.
Thirdly, tests should focus on revealing what learners understand and what they are battling with, instead of putting pressure on them to “pass” a certain level.
Encouragingly, recently released documents (S2 and S3 of 2020) from the Department of Basic Education are promoting these principles. These documents emphasise the need for teachers to work with learners where they are, to take time to remediate when learners don’t understand and to assess only what has been taught.
This is arguably the most forward-thinking policy produced by the department in recent years. What it lacks is a carefully considered implementation plan, informed by the realities on the ground, to identify the core mathematics content for learners, and a teaching and learning pathway for what remains of 2020 and into 2021.
In the short term, if learners are able to master the content we have identified, they may well end 2020 with more mathematical knowledge than they would have gained ordinarily.
COVID-19 could be the unexpected catalyst that makes the education system accountable to learners and their learning. But we need to get Grade 8 and 9 learners back to learning as soon as possible. It is crucial that they are not neglected because of an overwhelming focus on Grade 12.
Three South African vice-chancellors paint a post-COVID picture for universities.
Across the world, the higher education sector is changing because of the COVID-19 pandemic. The Conversation Africa’s Nontobeko Mtshali asked vice-chancellors from three South African universities to share their insights about what these changes could mean for the country’s higher education landscape.
Questions and answers
What long-lasting changes to South Africa’s higher education sector has the pandemic brought? And how will these affect the way universities deliver teaching and research?
Mamokgethi Phakeng, University of Cape Town: University teaching will draw from various methods that range between fully face-to-face and fully online. Long before COVID-19, the University of Cape Town recognised the need to prepare students for a digitally mediated world. For example, by the beginning of this year about 60% of UCT lecturers had chosen to record their lectures.
COVID-19 fast-tracked this process as we launched emergency remote teaching.
Many of our academics say they will never again teach in the same way as before. The new way puts the needs of students with barriers to learning at the forefront. It helps us design good learning experiences and reconsider methods of assessment. Students can revisit online course material, ask questions and get personal support, in and out-of-normal teaching hours. It’s especially helpful to students who are second-language English speakers or who have a disability.
Lecturers have found how easy it is to engage with students in a WhatsApp group. There are challenges, of course, such as how we can conduct assessment for some invigilated exams, and in data access and electricity provision for some students at home. We are surveying students and academics to monitor their experiences and review lessons for the future.
Tawana Kupe, University of Pretoria: The reliance on face-to-face or contact teaching was under question because of the rise of digital technologies that were slowly disrupting it. For a number of reasons, higher education institutions were taking their time. Some lacked capital. There was also the issue of students’ lack of access.
A return to purely contact learning is not going to be possible. People have experienced something that seems more relevant to a future marked by increasing digitisation. Universities will now need more resources allowing them to move with greater speed in changing to hybrid or blended teaching and learning. When it comes to research, the use of simulations will increase, as will the use of technologies that can gather research data.
Adam Habib, University of the Witwatersrand: I believe we are going to see a stronger shift to a blended learning model. Anecdotal evidence is showing that our students are performing better in the online environment than face-to-face. This suggests we need to re-imagine how we test and assess our students’ capabilities. Obviously certain degrees still require face-to-face learning but this can also be re-imagined.
The shift to online also means we are going to see the digital divide in our country grow sharper unless we are able to develop public-private partnerships to assist. Government will also need to adjust its thinking about how we achieve this financially and in terms of curriculum changes.
Do universities have the human and financial capacity to respond to these long lasting changes?
Mamokgethi Phakeng: New ways of teaching can release human capacity by allowing lecturers to manage their course loads more easily. And if they make it possible to increase the number of students who can enrol in certain courses, then they could bring more income to the institution, to help finance human capacity or infrastructure development.
Of course, there will always be courses that require students to work collaboratively, or to have access to labs, and those courses remain available. Other universities are now beginning to use the extensive resources we’ve developed under Creative Commons licences, to benefit the sector during the pandemic.
Tawana Kupe: Most universities do not have the human and financial capacity to respond to these changes given that they have not been adequately funded for decades. Many face an existential crisis if governments do not include them in the stimulus packages meant to reverse the impact of COVID-19.
The training of staff who manage the information technology infrastructure and academic staff who teach and do research is critical for a successful transition from contact teaching to hybrid teaching. Innovative and creative ways to fund the transitions will have to be developed. They should include partnerships and collaborations among universities and with governments, the private sector and international donors.
Adam Habib: Many academics and professional staff have been able to adjust fairly quickly to the new online mode of teaching. This has been under discussion for some time now. I do not believe we will have a human capacity issue. The real issue will remain how to finance higher education. There is going to be a significant financial challenge both as a result of subsidy cuts (given state finances) and the inability of students to pay fees (because of the economic crisis).
In South Africa, we will also see a growing “missing middle” cohort as a result of job losses. Providing financial support to these students is going to be more important now than ever.
Are South African universities unique in facing these long lasting changes? What can they learn from other universities?
Mamokgethi Phakeng: Universities around the world are re-examining how they teach, do research and serve their students, staff and alumni.
Digital technology has opened up ways for people and institutions around the world to discuss and collaborate on problems that are universal. COVID-19 is demonstrating that across the globe we are facing the same problems, so we need to work together to find solutions.
Tawana Kupe: No, South African universities are not unique. What South African universities can learn is how to navigate changes in modes of teaching, learning and research from those universities that are ahead in adopting hybrid or blended modes.
Adam Habib: South African universities have similar problems to other institutions across the world. The big distinction with South Africa is that we are undertaking these activities in the midst of deep inequalities.
This means that we have much to teach the world on how to engage in blended learning in unequal contexts and how to assist poor people in this regard.
Wits University begins its second Covid-19 vaccine trial in South Africa
- Wits University
Wits is the lead institution in South Africa for a second Covid-19 vaccine trial and will begin screening participants for the NVX-CoV2373 trial today.
The Phase 2 trial in South Africa will evaluate if the nanoparticle S-protein, in the Covid-19 vaccine known as NVX-CoV2373, protects against Covid-19 disease in adults aged 18-64-years-old.
NVX-CoV2373 is produced by the biotech company, Novavax (Maryland, U.S.A). Novavax is a late-stage biotechnology company that develops next-generation vaccines for serious infectious diseases.
Wits Professor of Vaccinology, Shabir Madhi will lead the Novavax clinical trial in South Africa after having engaged personally with Novavax to motivate for clinical development of the vaccine to be undertaken in this country.
Madhi, who is the Executive Director of the South African Medical Research Council Vaccines and Infectious Diseases Analytics Research Unit (VIDA) at Wits and the Faculty of Health Sciences Dean-elect, also leads the South African Ox1Cov-19 Vaccine VIDA-Trial launched on 23 June, in association with University of Oxford and the Jenner Institute.
The Novavax vaccine in the South African trial leverages technology used successfully to develop vaccines against influenza (flu) virus and experimental vaccines against Ebola and Respiratory Syncytial Virus (RSV).
Madhi previously collaborated with Novavax as a lead investigator on the RSV vaccine for pregnant women, which aimed to prevent the most common cause of pneumonia in babies.
About the Novavax vaccine: NVX-CoV2373
The Novavax vaccine candidate is called NVX-CoV2373. This vaccine candidate is engineered from the genetic sequence of SARS‑CoV‑2, the virus that causes Covid-19 disease.
In preclinical studies, NVX‑CoV2373 demonstrated the elicitation of antibodies that block the binding of spike protein to receptors targeted by the virus – this is a critical aspect for effective vaccine protection.
Studies of this Novavax vaccine in non-human primates have shown protection against SARS-Cov-2 infection in upper airways (nasal passages) as well as protection against lower airway (lung) disease.
Safety and immunogenicity [the ability of a foreign substance, such as an antigen, to provoke an immune response] data from part 1 of the Novavax Phase 1/2 randomized, observer-blinded, placebo-controlled trial of its Covid‑19 vaccine with and without Matrix‑M™ adjuvant in healthy adults 18-59-years-old, conducted in Australia, have been submitted to the U.S. Food and Drug Administration and an independent safety monitoring committee.
In this Phase 1 clinical trial, NVX-CoV2373 was generally well-tolerated and elicited robust antibody responses numerically superior to that seen in human convalescent sera. The data have been submitted for peer-review to a scientific journal and are available online.
Why South Africa?
“The major motivation for Covid-19 vaccines being evaluated at an early stage in South Africa is to generate evidence in the African context on how well these vaccines work in settings such as our own,” says Madhi.
“This would enable informed decision-making when advocating for the adoption of this [NVX-CoV2373 vaccine candidate] or other Covid-19 vaccines in African countries, once they are shown to be safe and effective.
Participating in the clinical development of these vaccines at the outset will assist in advocating for South Africans to be amongst the first in line to access these life-saving vaccines, once they become available.”
The South African NVX-CoV2373 trial
The screening of volunteers for the South African Novavax Covid-19 vaccine trial begins on Monday, 17 August.
The Phase 2 NVX-CoV2373 study in South Africa will enroll up to 2 904 volunteers aged 18-64-years-old. The trial will evaluate the vaccine candidate’s safety, immunogenicity, and efficacy [protection against Covid-19].
The randomized, observer-blinded, placebo-controlled Phase 2 clinical trial in South Africa will include two cohorts:
One cohort will evaluate the efficacy, safety and immunogenicity of NVX-CoV2373 in approximately 2,650 healthy, HIV-negative adults.
The second cohort will evaluate the safety and immunogenicity of NVX-CoV2373 in approximately 240 medically stable, HIV-positive adults.
“This important Phase 2 clinical trial will not only provide additional data on safety and immunogenicity of NVX-CoV2373, it also has the potential to provide an early indication of efficacy, as South Africa is experiencing a surge of Covid-19,” said Stanley C. Erck, President and CEO of Novavax.
The Bill & Melinda Gates Foundation awarded Novavax a $15 million grant towards the Covid-19 vaccine effficacy trial in South Africa.
The South African study is part of a larger, global clinical programme to evaluate NVX-CoV2373, including larger Phase 3 studies with approximately 30 000 participants, to be launched throughout the world.
Covid-19 Update 42 - The phased return of students and staff to campuses
- VCO News
Wits’ protocols remain in place, and only students and staff with the requisite permits and permissions will be allowed entry to campuses.
Over the weekend President Cyril Ramaphosa announced that South Africa would be moving to a level 2 lockdown from midnight, on 17 August 2020 (tonight), but warned that whilst we are making progress in reducing infections, we still need to be cautious, and to work remotely as far as possible. He also indicated that the country has the fifth-highest number of infections globally, and that there is a chance of a resurgence of the disease.
In his weekly newsletter, he added: “We now need to manage this risk and ensure that the gains we have made thus far in containing the pandemic’s spread are not reversed. The greatest threat to the health of our nation right now is complacency.”
Phased return of students and staff
In the wake of the President’s announcement and other government directives, including the prohibition of gatherings of more than 50 people, the prevention of international travel, and the need to maintain social distancing, the University is carefully planning for the phased return of specific cohorts of students and staff to our campuses over a period of time. Other considerations, including our infrastructure, residence and services capabilities, will inform the phased reopening plan.
It is envisaged that we will continue with an expanded hybrid model (contact and online teaching). Faculties, Schools and Divisions are currently determining exactly which cohort of students and staff will be required to return, and by when. This will be shared with the University community within the next ten days, along with the recalibrated 2020 almanac. For now, the academic programme continues as is.
No room for complacency
Whilst lockdown restrictions may be relaxed, the coronavirus will still be with us for many months to come. Wits’ protocols remain in place, and only students and staff with the requisite permits and permissions will be allowed entry to campuses.
Remember to always:
complete the online screening every day via the Wits Screening App before entering campus,
wear a cloth mask over your face and nose (and the relevant PPE in special contexts),
avoid touching your eyes, nose and mouth,
practise physical distancing from others,
wash your hands regularly for at least 20 seconds, and dry them properly,
Covid 19: Scientific excellence will help explore new frontiers
- Robin Drennan, Joao Rodrigues, Garth Stevens & Imraan Valodia
When university resources are scarce, building and sustaining equitable research excellence should be paramount.
In the midst of the Covid-19 pandemic, the emergence of successful solutions to the unprecedented levels of uncertainty and disequilibrium created in our society and in our economy, will depend largely on our ability to harness capabilities in scientific research – be that in the traditional sciences, the health sciences or the social and economic sciences.
It is scientific research in its broadest possible sense that can help to explore the new frontiers of vaccinology to counter the impact of the virus, to consider how best to stimulate an ailing economy, and how to manage the deep psychosocial effects and pre-existing social ills that Covid-19 has both caused and exposed.
Moreover, as the digital transformation gathers pace, our ability to remain within global science networks will be more critical than ever before. If we are to succeed as a society we need science and scientific research, and we need it to be robustly engaged with, interrogated, questioned, applied and embedded in social life. For this, we need to be constantly thinking about how we nurture both an enabling environment and a new layer of critical and creative thinkers of tomorrow, who will drive such scientific research and knowledge production. And, as our fiscal consolidation takes effect, and resources become more and more constrained, the efficiency with which we use scarce funding for science is more imperative than ever.
The key actor in our scientific community is the higher education sector. A large proportion of university-based research, and indeed some of the most cutting edge thinking, is conducted by postgraduate students under the supervision and in collaboration with academic staff. Research and critical thinking skills are acquired and honed in the cut and thrust of practice under the close and supportive watch of, and in partnerships with, academic staff. In addition, this is a site where emerging scholars are exposed to processes of quality assurance, peer review, critique and the social value of research – all of which contribute to research and human capacity development, high-quality research, and the possibilities of science and knowledge acting in the service of the public good.
Unfortunately, the National Research Foundation (NRF), the primary funding agency of the National Department of Science and Innovation (the DSI), has recently shifted the emphasis of its programme for the financial support of postgraduate students, having “phased out…the grant-holder linked modalities of funding postgraduate students in 2020” (NRF (HCD), 2020). “Grant-holder” linked bursaries are the bursaries that academic staff, who have been awarded an NRF research grant, can award to their students to support the research. However, from 2021 onwards this collaborative, capacitating and supportive method used by the NRF since its inception in 1998 for funding the student-staff research partnership, has effectively been moth-balled.
This action poses two important constraints on the research and postgraduate student training. First, it closes off the space for field development and advancement by academic staff who would normally have used this mechanism to identify promising students to work alongside them and to grow both the human capacities and expertise, as well as a specific field of inquiry.
If we sacrifice equity for quality research, we run the risk of reproducing skewed forms of knowledge production and institutional capacities. If we disinvest from productive sites of research and knowledge generation, simply to enact seemingly new distributional regimes, we do not attenuate the skills differentials that exist across institutions in South Africa and we undermine existing research strengths.
Second, and perhaps more worrying from a capacitation and transformation perspective, is the separation of the funding of the operating costs for the research and the bursary costs for the student. The net effect of this separation is that it is likely to weaken institutional and postgraduate capacity for innovative research that requires funding, even though it may seemingly broaden access. Separating these costs structures is perhaps courting failure for the postgraduate research capacitation pipeline and will have significant ramifications for research development in South Africa in the long term.
Clearly, transformation is an important social imperative and principle that must drive corrective action to attend to historical inequities, and is vital for the future of South Africa. Our society grapples with the challenges of quality and equity on a daily basis, but it is important that addressing these issues does not become a binary choice or a trade-off between the two principles. Indeed, these two principles of equity and quality are integral, and we should insist on both being pursued simultaneously.
If we sacrifice equity for quality research, we run the risk of reproducing skewed forms of knowledge production and institutional capacities. If we disinvest from productive sites of research and knowledge generation, simply to enact seemingly new distributional regimes, we do not attenuate the skills differentials that exist across institutions in South Africa and we undermine existing research strengths. We have to recognise that the 26 universities in South Africa are differentiated, even if this is not specifically by design today. Indeed, the Executive Summary of the National Development Plan notes that the “performance of existing [higher education] institutions ranges from world-class to mediocre”. With the necessary resources we could raise the standard of all our institutions, but in a constrained fiscal environment, we must utilise the limited resources prudently and in ways that play to existing research expertise and address issues of equity.
The requirements that all prospective students, for example, apply online and are treated entirely equally in their applications, is at face value a given tenet of transformation practice, but may have unintended and perverse consequences if considered purely on its own.
Students receiving bursaries to pursue research training at universities that are not research-intensive may be limited in their own development, and this does not in and of itself address the skills challenges at historically under-resourced universities. What is perhaps required is a different compact – a new set of knowledge and institutional architectures where funding agencies such as the NRF open access through its transformation lenses, but also simultaneously encourage partnerships between institutions that are more research-intensive and those who are historically under-resourced. In this model, students from all institutions would benefit from the funding allocations, but inter-institutional arrangements where research-intensive universities are coupled with institutions that have been historically under-resourced should be encouraged to develop excellence across an unevenly differentiated system.
During these times of reduced funding due to the demands of the Covid-19 pandemic, it is crucial that our limited resources are used as judiciously and efficiently as possible. Any funding strategy should take into account equity, existing research and knowledge infrastructures that we could optimise even further, capacitating an unevenly differentiated higher education sector, and encourage innovations to the local and global challenges that science, research and knowledge production could be responsive to.
Robin Drennan is the Director of Research, Joao Rodrigues is the Acting Deputy Vice-Chancellor: Research, Garth Stevens is the Dean of the Faculty of Humanities and Imraan Valodia is the Dean of Faculty of Commerce, Law and Management. All of them at the University of the Witwatersrand. This article was first published in Daily Maverick/Maverick Citizen.
Study on SARS-CoV-2 transmission by asymptomatic people in rural and urban SA
- Wits University
How many people in one household contract SARS-CoV-2, transmit it without having symptoms, and how does this virus interact with other pathogens in the home?
A new study aims to find out how many people in individual households in rural and urban South Africa become infected with SARS-CoV-2, how asymptomatic [producing or showning no symptoms] people transmit this virus, and how this virus interacts with other pathogens.
SARS-CoV-2 is the virus that causes coronavirus disease (Covid-19).
Professor Cheryl Cohen, Principal Investigator of the study, known as the PHIRST-C study, says, “The study will help answer vital questions about how common asymptomatic infection is and how people who are infected with SARS-CoV-2, but who remain asymptomatic, transmit the virus compared to those who do have symptoms. The study will also examine the role of children in virus transmission, which will be important as the schools reopen.”
Cohen is a Professor of Epidemiology in the Wits School of Public Health and Head of the Centre for Respiratory Disease and Meningitis (CRDM) at the National Institute for Communicable Diseases (NICD) in the National Health Laboratory Service (NHLS) in South Africa.
Infection insights in rural South Africa
The Mpumalanga component of the study draws participants from communities that form part of the Agincourt Health and Socio-Demographic Surveillance System site platform of the South African Medical Research Council-Wits Rural Public Health and Health Transitions Research Unit (Agincourt).
Agincourt is a major research endeavor within Wits University’s rural campus in Bushbuckridge, which has run longitudinal studies, intervention trials and health systems research in this community for over 25 years.
Professor Kathleen Kahn runs the PHIRST-C study in Agincourt, says, “Meeting the challenge of Covid-19 in rural South Africa is critical to the national response, now more than ever as the pandemic approaches its rural peak. Doing so effectively demands a deep understanding of how virus transmission differs among rural families and communities – exactly what PHIRST-C is designed to achieve.”
How viruses collide
The PHIRST-C study builds on a cohort monitored from 2016 to 2018, which estimated the burden and household transmission of Respiratory Syncytial Virus (RSV) and influenza (flu).
RSV causes respiratory tract infections and this this virus is a major cause of lower respiratory tract infections and hospitalisation of children during infancy and childhood.
Dr Neil Martinson, Chief Executive Director in the Wits Perinatal HIV Research Unit (PHRU) at Baragwanath Hospital, is the Principal Investigator of the PHIRST-C study in Jouberton Township, says, "Obtaining more information from settings outside of large metropolitan areas is important. This study will provide more understanding of the impact and transmission of COVID in peripheral townships where health services, including COVID testing sites, are not as available as in large cities; where household members are less likely to be employed; and where they are less likely to be able to safely self-isolate or self-quarantine.”
About the PHIRST-C SARS-CoV-2 study
In the PHIRST-C study: SARS-CoV-2 community burden and transmission in two South African communities, participants will be tested twice weekly until the end of 2020 to determine whether or not they become infected with SARS-CoV-2.
Participants will also be asked about the presence of Covid-19 symptoms at each visit and two different methods will be used to estimate the burden of infection: PCR tests and sero-surveys.
Polymerase chain reaction (PCR) tests are used to detect the presence of viral genetic material directly, rather than the presence of the body's immune response, or antibodies.
Sero-surveys investigate the presence of antibodies, which are evidence of an immune response to the infection. It is unclear for COVID to what extent these antibodies “resist” infection. Researchers will thus also use this methodology to estimate the burden of SARS-CoV-2 in these communities.
The PHIRST-C study will also conduct testing for RSV and flu to help understand the interaction of these viruses, should they circulate in communities at the same time.
Understanding viral re-infection and interaction
By analysing blood samples for antibodies to SARS-CoV-2 as evidence of recent or past infection (sero-prevalence), the study will add to global knowledge of the body’s immune responses to SARS-CoV-2 infection and reveal the factors that influence the duration of protection against repeated infection.
The serial serology testing planned will answer important questions related to the immune response to SARS-CoV-2 and the duration of the immune response.
Professor Lynn Morris, interim Executive Director of the NICD and a Research Professor at Wits University, says, “Serology results from this study may help to answer some outstanding questions related to Covid-19 immunity, for example, the level of antibodies needed to provide protection against re-infection as well as the rate of asymptomatic infection in South Africa.”
The results of the PHIRST-C study will help the South African Department of Health and the global community to better understand the transmission dynamics of SARS-CoV-2, of asymptomatic infection prevalence, and the transmission from asymptomatic infection.
The PHIRST-C study is a collaboration between the CRDM of the NICD and NHLS in partnership with Agincourt and the PHRU at Chris Hani Baragwanath Hospital. The U.S. Centers for Disease Control and Prevention (CDC) fund the study.
When conducting research in communities, the research teams abide by strict hygiene and safety protocols as instituted by the National Department of Health and governed by global best practices in ethics and public health.
Appoint a war Cabinet now to tackle Covid-19 crises
- William Gumede
SA should fire the current Cabinet and set up a national “emergency” one with the best talents in the country prevent it from plunging down the cliff.
This is the biggest crisis of our generation, and the way we deal with it will determine whether the economy will continue to spin into freefall, political instability surges and social order breaks down. Unless we change the Cabinet leadership course now, we will have no country left, either for ourselves, our children and the generations to come.
A “war”, “emergency” or rather Covid-19 Cabinet would be an executive committee to specifically manage the combined financial, social and health crises unleashed by Covid-19. Its main objective would be to bring together all South Africa’s skills, resources and institutions behind the single purpose of overcoming the economy, social and health impact of Covid-19.
Typically, such “war” Cabinets are small in size, maximum eight people for nimble decision-making. It cannot be as unwieldingly large as the current Cabinet, rank one of the largest Cabinets when compared to those of our better performing peer country competitors.
Such a “war” Cabinet would be dissolved once the Covid-19 storm subsides. The extraordinary crises that Covid-19 unleashed, means that current institutions will have to be adapted, and quickly so, to deal with the changing needs of society, economy and government.
This current Cabinet in its structure, the people and the laborious way it conducts its business is simply not equipped to tackle this massive crisis. It should be abandoned, if at least temporary until the crisis is passed. Some of the current ministers, if they are to be retained, presumably for political reasons, rather than competence, should be limited to overseeing the administrative running of their departments.
The Covid-19 crisis is unprecedented in South African history. The often repeated saying by government leaders that we have defeated apartheid and therefore we will defeat Covid-19, is not just being silly, it is underestimating the crisis and it leads to the current frightening complacency at the highest levels of government.
The Covid-19 financial, social and health crises can only be defeated with a clear plan, the best people to manage it and mobilizing all the country’s resources.
A “war” Cabinet should include the best professionals, industry leaders and figures from opposition parties with proven expertise, capabilities and acumen. They should not only consist of members of the ANC, but be drawn from opposition parties and those without any particular party affiliation.
The current Cabinet is not fit for purpose to deal with the crisis South Africa finds itself in. With the current Cabinet in charge of managing this once-in-century crisis, South Africa is likely to fail miserably. Now more than ever, expertise, new ideas and fresh energy is needed to guide South Africa.
The leadership of the public administration which steers public service delivery during “peace” time lacks the capacity, ideas and talent to lead the Covid-19 delivery effort. In “peace” times the public service has failed spectacularly to do the most basic functions; to expect the public service to deliver in Covid-19 times is a fallacy.
Mike Mlengana summed up the appalling state of the public service, when resigned a few weeks ago as Director General of the Department of Agriculture, Land Reform and Rural Development. Mlengana could have been speaking for the entire public sector when said that he quitted because his department was characterised by “large-scale and widespread inefficiencies at all levels”, and that “current structures and human capital are not geared for effective implementation”, and that there is an “absolute lack of delivery knowledge and work ethic”.
The capacity, resources and talents of the public sector, private sector and civil society will have to be combined to tackle Covid-19. It is certainly delusional for the government leaders to still carry on as if this inefficient public sector can on its own navigate the country successfully through this terrifying Covid-19 crisis.
A new “war” Cabinet would not only oversee the government’s Covid-19 response, but also coordinate the project management of the joint efforts of the public sector, private sector and civil society. To deal with the lack of public sector capacity, the private sector and civil society could each be assigned to delivery specific services, which is the state is either incapable of doing or doing ineffectively.
South Africa is faced with extraordinary crises, demanding extraordinary measures, one of these is to bring the best talents to head the structures that oversee the recovery effort, and pooling all the country’s institutions, talents and resources, behind the single purpose of overcoming the multiple Covid-19 crises.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand; and author of Restless Nation: Making Sense of Troubled Times (Tafelberg). The article was first published in the Sunday Times.
How lockdown has affected the health of South Africa's poor
- Chijioke Nwosu and Adeola Oyenubi
Poor populations bore a disproportionately higher burden of poor health.
The COVID-19 pandemic has wreaked substantial damage on human lives and the economy in South Africa. But the impact of the measures used to combat the pandemic, such as lockdowns, have not been even. The pandemic has likely worsened the income inequalities that characterise the country’s economy.
Vulnerable populations such as low income earners in informal and precarious employment have been most affected by job losses and the resulting income loss. Moreover, while COVID-19 has affected every facet of people’s lives, it is essentially a health problem. The loss of jobs and income is likely to result in reduced ability to access healthcare and a nutritious diet. This, in turn, will negatively impact on people’s health.
We recently conducted a study to estimate how closely health was related to income, in the context of COVID-19 in South Africa. We used data from the National Income Dynamics Study-Coronavirus Rapid Mobile Survey, a nationally representative survey collected in May/June 2020.
The survey collected information on health, income and other relevant factors during the higher levels of the lockdown. We compared these findings to data collected from the same individuals in 2017.
We found that poor populations bore a disproportionately higher burden of poor health. This was the case in both 2017 and the COVID-19 period. A remarkable finding was that income-related health inequality in the COVID-19 period was about six times that obtained in 2017. This shows that income had a much stronger relationship with health during the COVID-19 crisis than before.
Explaining the inequalities
To measure health inequalities related to income, we used a statistical measure known as the concentration index. The key factors that predicted the observed income-related health inequalities in the COVID-19 era were race, hunger, and income. Each of these factors worsened income-related health inequalities.
Race affected the inequalities in two ways: Africans were more likely to be poor and report being in poor health compared to their white counterparts. The same was true of hunger. On the other hand, income worsened health inequalities through the richer being less likely to be in poor health.
The impact of race on health outcomes, especially in this period, corroborates prior evidence in South Africa and elsewhere. Black people are among the worst affected by the COVID-19 epidemic in South Africa. One of the avenues through which this occurs is higher exposure to hazardous jobs such as working as cleaners or in fumigation of contaminated areas.
The relative disadvantage of historically disadvantaged racial groups to pandemics is well known – especially in the present situation. For instance, African Americans have disproportionately high infection and mortality rates due to COVID-19 in the United States.
Similarly, limited access to quality healthcare can contribute to race-based health inequalities. South Africa’s health system is deeply segmented. It consists of a well-resourced private sector – mostly funded by expensive medical aid scheme membership – and an overburdened public sector which caters for the majority poor masses (mostly Africans). It is estimated that only 10% of Africans belonged to medical aid schemes compared to 73% of whites in 2018.
This two-tier system is in dire need of reform if the country is to tackle health inequalities. Hopefully the country’s move to universal health coverage as envisaged in the proposed National Health Insurance Scheme will mitigate these inequalities and inequities.
The second factor was hunger. Its strong contribution to health inequalities is disturbing, especially given the rights-based approach to food security enshrined in the South African Constitution. The state hasn’t been able to fulfil its constitutional role of ensuring that all South African residents have enough food to enjoy a dignified life. This was especially true during the period of the COVID-19 epidemic.
As we found in this study, hunger not only adversely affects people’s dignity; it also widens the health disparity between the rich and the poor. This is particularly worrying given the high prevalence of hunger during this epidemic. It has become absolutely necessary to protect the health of the poor in South Africa. That is why anti-hunger policies such as the National School Nutrition Programme are even more relevant now.
The final factor contributing to widening health inequalities was income inequality. As earlier indicated, COVID-19 disproportionately affected the poor through a higher likelihood of them losing their jobs, among other things. A higher probability of job loss among already economically compromised individuals and households would not only exacerbate income inequality, but is likely to contribute to worsening health outcomes among the poor given their further limited ability to meet basic needs like food and medication.
Therefore, measures to save the livelihoods of the poor must be sustained during the crisis and beyond.
Way forward
Our paper underscores the fact that the poor bear a disproportionate burden of poor health and that income-related health inequalities seem to have gotten worse in the COVID-19 era.
We believe that this pandemic and the associated lockdown reinforced existing inequalities in South Africa. These were exacerbated by massive job cuts and a depressed labour market.
Policies that address race-based disadvantage – such as universal health coverage as well as anti-hunger measures are urgently needed to mitigate health disparities in the COVID-19 era and beyond.
South Africa’s second COVID-19 vaccine trial explained
- Wits University
Pasha 78: Listen to Professor Shabir Madhi, explaining how the new vaccine trial will work
Trials have begun in South Africa for a second COVID-19 vaccine study. The hope is that at least one of the vaccines being trialled will show promise and play a role in eliminating the SARS-CoV-2 coronavirus.
In this episode of Pasha, Shabir Madhi, professor of vaccinology and Director of the MRC Respiratory and Meningeal Pathogens Research Unit at the University of the Witwatersrand, explains why there are multiple vaccine studies under way, the differences between them, how this second South African trial works and when the results might be known.
The coronavirus is a moment to be humble and realise our finitude in a wondrous and infinite natural order.
Covid-19 pushed an already weak and crisis-ridden global economy over the edge. Massive value has been erased from crashing stock market prices. Many commentators have talked about the return of economic conditions similar to the great financial crash of 2007-2009.
The most powerful countries in the world, from China to the US, ground to a halt and the South African economy followed suit as citizens hunkered down in lockdown. Governments across the world have, to different degrees, seized the challenge to protect their populations, at least that is what it seems given the people-centred rhetoric.
Climate of carbon capitalism
The geo-politics of Covid-19 engulfing the entire globalised world in its rapid spread is also a shot across the bow of carbon capitalism.
Elite consumption of exotic animals in Wuhan, China unleashed the swift and lethal revenge of nature. These injustices are not new for climate justice politics as elite use and consumption of fossil fuels is linked directly to extreme weather shocks such as heatwaves, droughts, floods and cyclones, for instance, which impact those who most vulnerable the hardest.
Yet there is no consequence for those responsible and the fossil fuel industry, carbon addicted states and wealthy carbon-based consumers continue on as though climate science does not exist.
‘Black Swan’ event?
In the business world, Covid-19 tends to be reduced to being considered a Black Swan event. A sudden or unforeseen happening with great consequence that is rationalised after the fact. The idea was initially popularised by Nassim Nicholas Taleb’s five volumes on uncertainty, including the famous Black Swan.
While business risk analyses missed the likelihood of a Covid-19 pandemic, its occurrence cannot be explained as a Black Swan event.
Equally the worsening climate crisis and its global shocks are not Black Swans. They are dangerous systemic crisis tendencies produced by a hard-wired logic based on the duality of capitalism versus nature. Science has provided us with understandings and warnings, and yet the global capitalist system persists in driving us towards harm and destruction.
End the war on nature
The climate crisis is worsening with a lack of will to phase out fossil fuels and decarbonise.
We are facing a 1.5°C increase in planetary temperature most likely in the next five years, which will be accompanied by intensifying climate shocks. These crises will become interconnected, cascade into each other and push our socio-ecological orders towards collapse.
There are three considerations to address the imbalances, with each being critical if we are to enable nature to reverse climate damage that we as humans have caused.
First, in the South African context, the country will need an eco-justice stimulus package to tackle the impacts of Covid-19, the economic crisis and worsening climate crisis. South Africa’sClimate Justice Charteris a crucial point of departure in this regard.
Second, a war approach to Covid-19 is based on dangerous philosophical foundations. It continues the anthropocentric conquest of nature which is central to capitalist thinking.
Killing Covid-19 from this war-based framework is about us being the dominant species as we attempt to demonstrate superiority to the forces of nature. This is really a conceit which fails to understand that nature has been and will always be more powerful than us.
With Covid-19 we are really trying to mitigate the revenge blow from nature. It’s a moment to be humble and realise our finitude in a wondrous and infinite natural order. We are just one little part of a vast and delicate web of life.
As such, ending Covid-19 should be about ending the war with nature. This includes ending wet markets for exotic animals, ending globalised industrial agriculture and rapidly phasing out fossil fuels.
Third, the war on Covid-19 keeps us bound up in an ethical knot and derives from deeply oppressive ways of thinking. Violence whether colonial, imperial, patriarchal, racist or ecocidal is not what the world needs.
Ultimately Covid-19 has achieved what over 20 years of UN climate negotiations have failed to secure. What is required is a world led by those who place profit above human and non-human life is placing us all in jeopardy. Complex and holistic systems thinking that is grounded in an ethics of care, rather than war, has to prevail.
This article was written by Professor Vishwas Satgar. Professor Vishwas Satgar is an Associate Professor of International Relations at Wits University. He edits the Democratic Marxism series, is the principal investigator for Emancipatory Futures Studies and has been an activist for four decades. He is the co-founder of the South African Food Sovereignty Campaign, Climate Justice Charter process and Chairs the Board of the Co-operative and Policy Alternative Center (COPAC).
The full article captured in this excerpt was first published in the Daily Maverick.
Post-Covid Africa will have to save itself. It is a terrifying task
- William Gumede
African countries, with their lack of quality leaders, weak states and little fiscal reserves face economic, political and social disorder.
It is very likely that many African countries will increase debt, unemployment and social disorder. Many countries may reverse back to the terrifying instability of the 1970s, when African countries were characteristics by economic stagnation, social unrests and coups.
The countries that have more successfully dealt with Covid-19, such as South Korea, Singapore and New Zealand had at least three things in common: quality leadership, capable states and substantial financial reserves following pre-Covid19 prudent management of their country finances.
African countries are unlikely to get the substantial global financial, medical and technical support they received during past epidemics. In previous health epidemics in Africa, such as HIV/Aids, Ebola and cholera, industrial countries provided substantial financial, medical and equipment support.
Industrial countries have had to roll out large bailouts packages to tackle the financial crises fuelled by Covid-19, which will put pressure on their public finances for years. They will have very little remaining to provide the kind of financial support to African countries they had previously provided to Africans in previous health epidemics.
With Covid-19 impacting industrial countries also, they have not only sealed their borders to prevent the virus from spreading, they have also refocused their resources for domestic purposes to combat their own Covid-19 crises.
Some industrial countries producing critical medicines, equipment and food stopped these vital items from being exported to poorer countries, for local use instead. This deprived many African countries of similar support they received from Western countries during previous epidemics.
The European Union imposed temporary restrictions on the export of medical protective equipment from within the bloc to outside countries.
The US was accused by German biopharmaceutical firm CureVac of wanting to procure a coronavirus vaccine the company was developing exclusively for the US. German ministers reacted with anger to the US offer. India curbed exports of basic medicines, such as painkillers, for use for its own citizens.
Global trade wars preceded the Covid-19 outbreak, with the US battling China; and Russia and Saudi Arabia embroiled in an oil price war. In June 2020, the US threatened the EU with stricter tariffs. Tensions have escalated between China and India over disputed border territory in the Himalayas. India is putting restrictions on Chinese trade, businesses and interests in India.
Based on the nationalistic behaviour of many countries during the Covid-19 crisis, it is very likely that industrial countries that will successfully manufacture a Covid-19 vaccine, will prioritise their populations first, before they provide it to other countries.
Nationalism have risen across the globe with industrial countries becoming less altruistic, increasingly focusing on their own interests.
In previous African epidemics, multilateral organisations, such as the World Health Organisation was crucial in mobilising resources, expertise and funding for African countries. However, the rising nationalism preceding Covid-19, and countries’ sealing of borders and stockpiling their resources for almost solely for domestic efforts to combat the virus, has played out at multilateral organisations too.
Prior to Covid-19, the US and Israel withdrew funding from certain multilateral organisations. The US formally withdrew from the United Nations Educational, Scientific and Cultural Organisation (UNESCO) in 2019, accusing the organisation of anti-Israel bias. UNESCO has criticised the Israel’s occupation of East Jerusalem and granted Palestine full membership in 2011. The US withdrew its funding from UNESCO.
US President Donald Trump in June 2020 said he would formally withdraw the US from the World Health Organisation, accusing it of being under control of China. The US withdrawal from the WHO means there is less resources, to support African countries struggling with Covid-19, as they did when these countries battled previous epidemics.
Many African countries have undermined their own Covid-19 recoveries by blaming conspiracies for the spread of the virus, and therefore not acting decisively, using untested quack treatments under the guise of “traditional” African media and local “solutions” and shutting out the WHO from helping them.
The International Monetary Fund have estimated that some African economies could contract as much as 8%. The World Bank reported that up to 30million people are at risk of extreme poverty in Sub-Saharan Africa because of Covid-19. The exports of Africa’s commodities have declined following contractions in industrial economies which imports the continent’s commodities. African countries have experience large revenue losses. The already poor capacity of many African governments have been severely undermined during Covid-19, many governments unable to deliver essential services.
Africa’s tourism, hospital, media and transport sectors have been badly hit across the continent, with businesses closures, job losses and investments put on halt. The African Development Bank in a research note said that Africa’s tourist-dependent economies will decline up 10%. The economies of its oil exporters will decline up to 4%. The economies of oil exporters were already batters following the fall in oil prices in the oil price war between Russia and Saudi Arabia. Covid-19 have seen further oil production cuts.
Hunger, starvation and food shortages will continue as local and global food production and imports decline because logistical networks and supply chains are disrupted. Africa imports 85% of its food.
The IMF estimates that Africa will need US$110bn (R1.85trillion) in new funding in 2020 to tackled the socio-economic impact of the pandemic. The IMF has provided Covi-19 support to many African countries in the form of emergency loans and debt-service relief initiatives. The IMF has distributed US$10.1bn to 29 SubSaharan African countries in emergency lending or in augmentation of existing lending.
The IMF has given debt-service relief for 21 sub-Saharan African countries for an initial six-month phase ending mid-October 2020. The IMF has also provided a debt service suspension for highly indebted African countries as part of an initiative started by the Group of 20 leading economies that waived up to $U14bn in payments for poor, most of them African. Nevertheless, Covid-19 will increase African debt levels.
During Covid-19 countries sealed their borders to contain the spread of the virus. Given the new rise in nationalism in industrial countries, it is very likely that many industrial countries will keep the same Covid-19 border restrictions even when the virus is eventually contained, to keep out economic migrants from poorer African countries. This means that many struggling Africans that would try to seek new livelihoods in industrial countries will now be stuck in their own impoverished countries. Angry, impoverished and jobless Africans, with little alternatives, will become mass power kegs easily ignited.
Many African countries have also autocratic measures to enforce compliance to Covid-19 measures. The hard-handed measures have prompted anger, protests and defiance from citizens against leaders and governments – which may continue as socio-economic conditions worsen in the aftermath of Covid-19. Many African countries may see rising coups in which autocratic governments are ousted violently.
Others will see a rise in terrorist attacks, as terror movements see an opportunity in the rising poverty, collapse in public service delivery and popular anger against autocratic governments to recruit members, serve as alternative service providers and to unleash terror campaigns. Africa may see devastating food riots.
It will be crucial that African civil society be included in Covid-19 funding from multilateral organisations such the World Bank and IMF.
Furthermore, these multilateral organisations must put democracy conditions to their Covid-19 funding, such as compelling countries receive in the funding to govern honestly, respect human rights and uphold freedom of expression. African media, civil society organisations and watchdog organisations must ensure that Covid-19 related funding is used honestly, prudently and equitably.
African governments will have to govern more honestly, inclusively and caringly. African countries will have to muster the political will to genuinely formed an free trade area, trade more with each other and use their own country resources, skills, business and civil society capacity better.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand; and author of South Africa in BRICS (Tafelberg). This article was first published in Times Select.
GCRO map shows more women get Covid-19 in Gauteng
- GCRO
More women (56%) than men are testing positive for COVID-19 in Gauteng.
This August 2020 Map of the Month of the Gauteng City-Region Observatory (GCRO) sis presented as astory mapand draws on the infection data from the Gauteng Department of Health (6 March - 7 August 2020) and GCRO’sMarch 2020 COVID-19 vulnerability indicesbased on Quality of Life V (2017/18) survey data, to understand the ways in which women may be more vulnerable than men to COVID-19.
The GCRO also explore some of the implications for this gender bias in the number of positive cases.
Level two will allow more staff and students to return to campus. Faculties will invite carefully selected cohorts of students to return.
Dear Members of the Wits Community
We have reached level 2 of the national lockdown and although infection rates are declining, the virus is still circulating. Please continue to observe all COVID-19 protocols (social distancing, wear a mask, no large gatherings and sanitise or wash your hands regularly and properly).
This week, Dr Blade Nzimande, the Minister of Higher Education and Training in a speech stipulated that universities are allowed to bring back up to two thirds of staff and students to campuses. In light of this announcement, the Senior Executive Team has agreed to allow more students and staff to return, as per the University’s phased reopening plan.
Implications for Students
In keeping with the new regulations and to ensure that we comply with the health and safety protocols set out in the amended Disaster Management Act and Regulations, some faculties will invite carefully selected cohorts of students to return to campus, to participate in a combination of contact and online teaching and learning programmes. Please check your student emails regularly for communication from your faculty. Should you not be invited to return to campus, please continue with online learning from home.
The resumption of some services will commence in a phased in manner, in line with the University’s return to campus plans.
Students who are unable to study from home for various reasons may be brought back to residences on social justice grounds. The Dean of Student Affairs is managing this process carefully, as only two thirds of Wits’ residences are allowed to be occupied, with the requisite social distancing and other protocols in place. Applications from students who applied to return are being carefully considered given the limited number of beds available and in compliance with health and safety protocols. Invitations to return will be issued during the course of next week.
Implications for Staff
Employees, in consultation with their line managers, will continue to work from home where appropriate, and will return to campus if they are requested to do so by their line manager.
Third and Fourth Teaching Blocks (including Faculty specific requirements which may mean curriculum covered in shorter or more extended period / mid-term break / field trips /study break / boot camps and labs)*
13 Jul-23 Oct
77 Days
Study Break / Extended teaching period in Science / Field trips / Boot camps
26 Oct-30 Oct
5 Days
Assessment period 1 **
Assessment period 1 Science only
02 Nov-27 Nov
09 Nov-27 Nov
20 Days
15 Days
Vacation
16 Dec
* Academic calendar may be extended to allow for faculty specific additional teaching period as well as academic support for those cohorts of students identified by faculties so that they are eligible to be assessed in assessment period 2
** Sit down and online assessments (to be determined by faculty)
2021 Term Dates (including conclusion of 2020 academic calendar)
The complete 2021 Almanac will be published in the coming weeks.
Activity
Date
Number of weekdays
Assessment period 2 (will include supplementary and deferred assessments)
11-25 Jan
11 Days
New and returning postgraduate student registration and orientation
15-19 Feb
5 Days
Term starts for new and returning postgraduate students
22 Feb
Returning undergraduate students registration
22-27 Feb
6 Days
Welcome Day
28 Feb
First year online and one-stop-shop registration and orientation
01 -05 Mar
5 Days
Term starts for undergraduate returning and first year students
08 Mar
Notes:
The Faculty of Health Sciences’ term dates differ from those of the University and they may commence with lectures as early as the first working day in January.
Consult the University’s website for more detailed information about dates of registration for different cohorts of students.
Number of COVID-19 infections
Two staff members and ten students reported testing positive for COVID-19 during the past week. These include staff members who are working from home. Affected staff members and students are self-isolating in line with government directives and University protocols.
of infections
21 – 28 August 2020
22 June – 28 August
Staff
2
98
Students
10
177
The data provided in the table is based on the number of infections reported to the OHSE Office and the Campus Health and Wellness Centre.
It is with sadness that we announce the passing of two staff members this week – Ms Gugulethu Khumalo, an employee in the Faculty of Engineering and the Built Environment, and Ms Simangele Betty Nzima from the Services Department.
Ms Khumalo joined Wits in 2019 and assumed responsibility for all faculty-related academic administration for the School of Mining Engineering. She was well-known for her methodical approach to her work and her excellent organisational skills. Her integrity earned her the trust of her colleagues in a very short time and they recall how easily she integrated into the Wits environment. Prior to joining Wits, she worked at the University of Johannesburg in various positions.
Ms Nzima served Wits since 2014 and worked at the Wits Junction Residence Complex for almost six years until her untimely death. She was passionate about her duties and often assumed a motherly role as she cared for her colleagues and students. She enjoyed working as part of a team, was high-spirited and joyful, and enjoyed listening to ballads and gospel music. She is survived by her three sons and her extended family.
We extend our condolences to the family and friends of these colleagues. May they rest in peace.
SENIOR EXECUTIVE TEAM
28 AUGUST 2020
Covid-19 Update 45: Policies and Protocols - All you need to know
- Wits University
All staff and students are reminded of the approved Wits Covid-19 policy, Emergency Response Plan and other associated protocols.
Dear Colleagues and Students
We hope that you are well and healthy, and enjoying the return of the warm weather. As we prepare for the phased return of selected cohorts of students (as invited by faculties or the Dean of Students) and some employees (as requested by line managers), it is important for all members of the Wits community to be aware of Wits’ latest COVID-19 policies and protocols as explained below.
Please remember that you should only return to campus if you receive an invitation and permit from your faculty or line manager. In the case of residences, the Office of the Dean of Students will issue invitations and permits for some students to return in this phase, in line with government regulations. If you do not receive an invitation to return to residence by Sunday evening, please continue with the academic programme online from home. Your name will remain on a waiting list and you will be notified as soon as space becomes available, or when the next phase commences.
COVID-19 Infections
Two staff members and four students reported testing positive for COVID-19 during the past week. These include staff members who are working from home. This is out of a population of approximately 5 500 permanent staff and 37 500 students. Affected staff members and students are self-isolating in line with government directives and University protocols.
No of infections
28 Aug – 3 Sept 2020
Total Infections
Staff
2
100
Students
4
181
The passing of Mr Themba Tshabalala
We lost another long-standing member of the Wits community this week. We learnt earlier this week about the passing of Mr Themba Tshabalala, a Library Assistant at the Commerce Library. He will be sorely missed by all who interacted with him in the libraries and the greater Wits community. Mr Tshabalala has served Wits for over 22 years in various capacities. He joined the Wits Health Sciences Library in 1996 and was appointed as an Administrative Assistant in the Library’s Finance and Administration Department in 1999, before taking up the post of Library Assistant in the Commerce Library in 2011. On behalf of the Wits community, we extend our heartfelt condolences to his friends and family, and those who knew him well. May he rest in peace.
SENIOR EXECUTIVE TEAM
4 SEPTEMBER 2020
WITS’ COVID-19 POLICIES AND PROTOCOLS
The Occupational Health, Safety and Environmental Management Directorate (OHS&E) would like to remind all staff and students of the approved Wits COVID-19 policy, Emergency Response Plan and other associated protocols.
1. Risk assessment
All managers, Heads of Schools (HoS), Section 16.2 Assignees, Directors and Supervisors (as appropriate) must complete a COVID-19 risk assessment for their respective School or entity and implement the necessary risk mitigation measures before the return of staff and students to their respective entities. A copy of the risk assessment must be sent to the School or Unit’s respective OHS&E Officer. Guidelines to carry out the risk assessment are available from the OHS&E Directorate.
2. Relevant Forms
A Reporting Form for Employees must be completed for every staff member that contracts COVID-19, irrespective of whether the employee is working from home or on campus. The completed form must be sent to Jo-Anne Zastrau via Dept-OHS-Admin@wits.ac.za. This form has prompts indicating which other University entities should be notified.
A Reporting Form for Students must be completed for every student that contracts COVID-19. This form can also be obtained from Anna.Moloi@wits.ac.za from the Campus Health and Wellness Centre and must be returned to her once completed.
Line Managers and/or Supervisors are expected to investigate an infection incident involving an employee or student from their respective entity if the infected person was on the University’s premises 10 days prior to being positively diagnosed. The infected person's HoS, Section 16.2 Assignee, Director or Supervisor must, during such an investigation, attempt to ascertain whether contraction of the virus arose out of or in the course of employment or during student activities while on the University's precincts. They must complete the COVID-19 Investigation Form and send a copy of the completed form to the relevant OHS&E Officer. The form also includes prompts indicating which other University entities should be notified.
If an infected employee was on campus within a period of 10 days prior to being positively diagnosed and if there is evidence to suggest that the employee contracted COVID-19 arising out of and in the course of employment, then the infected person's HoS, Director, Supervisor or Section 16.2 assignee must fill in a WCL1 form and any other documents and send these to Ntabiseng.Nzimande@wits.ac.za and copy Dept-OHS-Admin@wits.ac.za so that the infection can be formally reported to the Compensation Commissioner.
3. Reporting Infections
In order to manage infections, maintain record-keeping and fulfil all University and legislative and regulatory requirements, certain entities at the University must be informed about staff and student COVID-19 infections. These persons or entities may include, but are not limited to:
The Line Manager or Supervisor must immediately be notified by the employee or student to enable the notification of other University entities and to investigate infection incidents;
The Line Manager or Supervisor will inform the Human Resources Officer, Manager or Course Co-ordinator of the entity in which the person is employed or studies (to assist with leave of absence arrangements and follow up);
In the case of student infections, the Campus Health and Wellness Centre (CHWC) is to be notified by the Line Manager or Supervisor and/or the infected person in order to facilitate isolation arrangements if necessary, to record the infection and to follow-up with the infected person, as well as to provide information about isolation and quarantining. Student infections must be reported using the student reporting form and must be sent to CHWC via Anna.Moloi@wits.ac.za
In the case of staff infections, the OHS&E Directorate is to be notified by the Line Manager or Supervisor and/or the infected person using the employee reporting form. The OHS&E Directorate records infections in a central register and uses the information to report work-related infections to the relevant authorities (such as the Department of Employment and Labour, insurers and the Compensation Commissioner).
Campus Protection Services is to be notified by the Line Manager or Supervisor and the CHWC to ensure that adequate access controls are implemented (i.e. CPS temporarily blocks the infected person's access card while the person completes the obligatory isolation or quarantine period and the card remains blocked until the recovered persons comply with the requirements to be permitted to return to campus);
Course coordinators in Schools (such as in the Faculty of Health Sciences) should be informed to facilitate the learning and/or tracking and isolation arrangements of infected and/or affected students;
For students and staff in residences, Residence Managers should be notified in order for isolation or quarantine arrangements to be made.
Cleaning services should be contacted in all instances where buildings and/or sections within buildings may potentially have been contaminated by an infected person and/or persons experiencing COVID-19 symptoms. The Services Directorate has a cleaning plan that can be obtained from the Director: Services by emailing Israel.Mogomotsi@wits.ac.za.
4. Confidentiality
The above designated individuals and those who may be designated to manage operations and who have access to information about an infected person, must keep such information confidential.
5. COVID-19 Symptoms
In the event that a person on campus experiences COVID-19 symptoms, this information must also be disclosed to the relevant Line Manager, Supervisor, Course Coordinator, the Campus Health and Wellness Centre, Residence Manager or Campus Protection Services either by the affected employee or student or by any person observing such symptoms (this requirement is not only confined to positively diagnosed persons). The person must be isolated and the protocol for the management of COVID-19 events must be followed. A copy of this protocol can be obtained from Jo-Anne Zastrau by emailing Dept-OHS-Admin@wits.ac.za.
6. Contact tracing
In the event that an infected or suspected infected person may have been in close contact with other persons on campus, then efforts will be made by the University to trace or determine (with the assistance of the infected individual) whether any other persons were potentially exposed. It will be expected that the relevant entity or School in which such an infected person functions will assist in the tracing process. The University will contact any affected employee or student and inform them of the potential exposure so that they may take the necessary precautionary measures. The name of the employee or student that is suspected to be infected with the virus must not be disclosed.
7. Return to Campus Readiness Plan
The Human Resources team have developed a comprehensive Return to Campus Readiness Plan, which can be obtained from the Senior Director: Human Resources via Kgomotso.Kasonkola@wits.ac.za.
8. Wits COVID-19 webpage
An informative COVID-19 webpage reflects Wits’ protocols as well as other useful COVID-19 information and resources. Please read and share this content as appropriate.
9. COVID-19 Emergency Response Plan
The latest version of the Wits COVID-19 Emergency Response Plan is available online and all entities must be aware of the content of this document.
Symposium to focus on key challenges in dealing with a delayed but explosive unfolding of Covid-19 in parts of Africa.
The purpose of the symposium, held from 1 – 4 September 2020, was to identify best practice solutions in respect of:
gaining of public trust in adhering to the health imperatives of social distancing and the use of approved therapies and vaccines to manage and contain outbreaks;
the dynamic and most-effective use of testing, tracing and isolation as public health tools during a pandemic; and
the scaling up of SARS_COV2 vaccine acquisition and distribution platforms that will serve all African countries for mass immunization.
The online symposium was hosted by Columbia University, the University of the Witwatersrand and Africa CDC, in collaboration with the Daily Maverick. Here follows post-symposium articles from a host of experts from Wits and its partners:
Why Africa needs to be involved in the development of Covid-19 vaccines
- Shabir A Madhi
Understanding the epidemiology of Covid-19 and moving forward would be critical to determining policy on the need to adopt interventions.
The Covid-19 pandemic continues to exact a toll on the health front, with about 25.5 million cases and 851,000 deaths documented as of 1 September 2020. Soberingly, this count represents only a conservative estimate of the number of people who have been infected by SARS-CoV-2 and who have died of Covid-19.
Central to this undercount has been the limited capabilities and capacity even in high-income countries to undertake adequate testing of suspected cases with symptoms suggestive of Covid-19, which is further exacerbated by the majority of adults (40%-60%) and children under 18 years (80%) likely to be asymptomatic. Consequently, even in the US, the country with the highest number of reported cases (6.03 million) and deaths (183,500), and where the testing rate is about 253 per 1,000 population, modelling suggests that the actual number of infections may be threefold to twelvefold higher in different states than has been documented.
In Africa, the capabilities to test for SARS-CoV-2 infection is severely constrained because of limited laboratory capacity. Despite the Africa Centres for Disease Control and Prevention indicating that about 43 sub-Saharan African countries have the ability to test for Covid-19, these are generally only available at a single central laboratory. Consequently, such testing facilities would be of limited value in quantifying the burden of Covid-19 in many of these sub-Saharan African countries. Furthermore, the limited test capabilities is compounded by the high costs of such tests, and the global shortage of SARS-CoV-2 testing materials – which is even more challenging to overcome in Africa, which is almost completely dependent on the import of the required reagents for Covid-19 testing.
South Africa, despite having the highest testing rate for Covid-19 in sub-Saharan Africa (62 per 1,000 population), nevertheless, lags behind the testing rate of many high-income countries (>150 per 1,000). Also, the positivity rate for tests conducted in South Africa was ~27% at the peak of the pandemic, and although declining to 13% in the past week, it still remains higher than the 5% threshold suggestive of adequacy in testing rates and control of virus transmission. Consequently, despite ~54% (680,000) of the 1.253-million Covid-19 cases reported in Africa being documented in South Africa, this itself probably represents a gross underestimate (possibly sevenfold to tenfold) of SARS-CoV-2 infections that have occurred in South Africa.
Characterising the burden of Covid-19, and any other disease, is more than an academic exercise. Understanding the epidemiology of Covid-19 currently and moving forward, would be critical to determining policy on the need to adopt interventions, including the Covid-19 vaccines that are being developed.
This underestimate in Covid-19 cases (and, by extrapolation, reported deaths) due to limited testing capacity is further highlighted by the disconnect between Nigeria and South Africa, both of which were ranked to be among the highest risk of Covid-19 outbreaks in Africa due to their global interconnectivity. In contrast to South Africa (population 59 million), Nigeria has a population size that is 3.3-fold greater (195 million), but has reported less than one-tenth (n=54,250) the number of Covid-19 cases compared to South Africa, and only 1,023 Covid-19 deaths. The testing rate for Covid-19 in Nigeria (1.95 per 1,000 population) is, however, 32-fold lower than in South Africa. Consequently, the burden of Covid-19 in Nigeria is likely to be even more grossly underestimated than in South Africa, and unfortunately the same would apply for most other sub-Saharan African countries where testing rates have generally been under 10 per 1,000 population.
Sero-epidemiological surveillance (testing for antibodies to SARS-CoV-2 to determine if infections may have taken place at least three weeks before) are about to be launched in South Africa, and would better quantify the proportion of the population likely to have been infected. Similarly, such sero-epidemiological studies could assist in characterising the extent of SARS-CoV-2 infection that has occurred in other African countries, in the absence of being able to test in any meaningful manner for quantification of active Covid-19 case detection. Such surveillance, coupled with epidemiological characterisation of excess mortality due to “natural causes” (assuming adequacy of vital registration data systems) over and above that anticipated for the period when the pandemic occurred, could assist in quantifying the burden of Covid-19 suffered in Africa. However, this is often only measurable after the pandemic has passed, as occurred for the swine flu pandemic in 2009.
Characterising the burden of Covid-19, and any other disease, is more than an academic exercise. Understanding the epidemiology of Covid-19 currently and moving forward, would be critical to determining policy on the need to adopt interventions, including the Covid-19 vaccines that are being developed. Mischaracterisation of the burden of Covid-19 in sub-Saharan Africa, particularly underestimating it due to lack of testing capacity, could paradoxically lead to African countries being compromised in advocating for and obtaining early and timeous access to safe and effective Covid-19 vaccines.
The lack of robust epidemiological data, largely due to inadequate health care and laboratory testing capacity in low-middle income countries (LMIC), has often contributed to a 10 to 20-year lag in the introduction of life-saving childhood vaccines into their public immunisation programmes relative to its availability in high-income countries. Examples of this include vaccines such asHaemophilus influenzae type bconjugate vaccine and pneumococcal conjugate vaccine, which protect against the leading causes of meningitis (brain infection) and pneumonia (lung infection) in children under five years of age. In the absence of immunisation, the bacteria targeted by these two vaccines caused more than one million childhood deaths annually, >95% of which occurred in LMIC (including approximately 50% in Africa which constitutes less than one-fifth of the global under-five childhood population).
The costs of these vaccines, and supply chain constraints contribute to the lag in introduction of these life-saving vaccines into LMIC public immunisation programs. However, often the lack of local epidemiological data to quantify the burden of disease and absence of local vaccine effectiveness studies from the region, has served as an excuse by governments not to mobilise resources for the introduction of these life-saving vaccines into their public immunisation programmes. Unfortunately, gathering local epidemiological data and undertaking vaccine effectiveness studies only after the vaccines have been licensed in high-income countries, inadvertently leads to millions of preventable deaths occurring while such evidence is generated.
Similarly, largely driven by paucity of laboratory testing capacity during the 2009 swine flu pandemic caused by the H1N1pdm2009 virus, there was a complete mischaracterisation of the burden of swine flu suffered in LMIC until after the pandemic. Notably, LMIC in the WHO African and south Asian countries reported the least number of swine flu cases during the pandemic, yet subsequently modelling estimated that 51% of all deaths due to the swine flu occurred in south Asia and Africa.
The global death toll from the swine flu pandemic included an estimated 201,200 respiratory deaths (range 105,700-395,600), and 83,300 cardiovascular deaths (46,000-179,900). Notably, there was also a flurry of activity to develop a vaccine against the swine flu virus during the pandemic, albeit using more tried and tested approaches leveraging on experiences with manufacture of seasonal influenza viruses. All the research on swine flu vaccine, including clinical phase I-IV studies, were undertaken exclusively in high-income countries, with no studies in Africa or south Asia. Consequently, despite a swine flu vaccine being developed during the course of the pandemic, following which it was deployed in many high-income countries, its availability in South Africa (which was the first in sub-Saharan Africa to gain access to the vaccine) only transpired after the pandemic had ended.
Of the 26 Covid-19 vaccines currently in human trials (many of which have multiple studies in different countries), only two are being conducted in Africa. This is consistent with the legacy of clinical trials more generally, where less than 5% of all clinical trials are done in Africa, despite it constituting 18% (1.3 billion people) of the global population.
Although not the only factor, the lack of involvement by African scientists in the development of the swine flu vaccine either by design (not their own, other than perhaps lack of initiative) or due to capability constraints, together with limited epidemiological studies quantifying the burden of swine flu in sub-Saharan Africa, diminished their ability to advocate for early access to the vaccine. This was compounded by vaccine manufacturers prioritising supply of the limited available doses of vaccine to high-income countries, where the licensure of the vaccine would have occurred immediately post-development.
Unfortunately, Africa remains almost totally dependent on vaccine developers and manufacturers in other continents for access to vaccines. Other than limited ability to produce yellow fever vaccine in Senegal, and limited manufacturing capacity of basic childhood vaccines in two north African countries, no vaccine manufacturing capacity exists on the continent. Furthermore, there has not been any discovery of a new vaccine that has been led by African scientists, largely a consequence of the systematic under-investment on the part of governments and the private sector in the field of research and development.
This, unfortunately places Africa at an immediate disadvantage in accessing vaccines, and perpetuates its dependency on non-African countries. This, despite political talk about Africa needing to prioritise vaccine-manufacturing capabilities, with very little progress having occurred since the adoption by the Ministerial Conference on Immunization in Africa in February 2016 of a resolution to promote and invest in regional capacity for the development and production of vaccines. In the absence of a strategic private-academia-public partnership, coupled with the ongoing brain drain of African scientists to higher-income countries where they are able to form part of teams geared toward vaccine discovery at its different stages of development, this situation is unlikely to change. Also, aspiring for a sudden break from the past and expecting manufacturing facilities to be set up in Africa within a 6-12 months framework to have an impact on the Covid-19 pandemic, is unlikely to yield any measurable success.
Fortunately, African scientists have been more involved in collaborating with international institutions in the clinical evaluation of vaccines, albeit in many sub-Saharan African countries, often under the leadership of investigators from high-income country institutions. Nevertheless, the infrastructure and local expertise does exist in at least a few sub-Saharan African countries for local scientists to assume a leading role in the clinical development and evaluation of Covid-19 vaccines. There has been some muted protest about vaccine trials being conducted in Africa under the notion that Africans are being used as “guinea pigs”. However, the reality is there is no rush on the part of vaccine developers (either from the private sector or academia) to conduct studies in Africa.
Of the 26 Covid-19 vaccines currently in human trials (many of which have multiple studies in different countries), only two are being conducted in Africa. This is consistent with the legacy of clinical trials more generally, where less than 5% of all clinical trials are done in Africa, despite it constituting 18% (1.3 billion people) of the global population.
The emergent vaccine-nationalism in many high-income countries, pre-ordering at premium prices vaccines that are yet to be licensed and suggesting regulations to restrict the export of Covid-19 vaccines manufactured in those countries, is a further challenge to ensuring an equitable and timeous distribution of Covid-19 vaccines especially to LMIC.
Notably, both of the Covid-19 vaccine studies in Africa are occurring in South Africa, following the initiative of local investigators to advocate and convince the vaccine developers to, at the least, provide the vaccine for such studies to be undertaken here, while in parallel being responsible for mobilising the resources to do so. The reasons for the paucity of Covid-19 vaccine studies in Africa are multifactorial, including cumbersome regulatory pathways that need to be navigated to get approvals to conduct such studies.
Furthermore, the harsh reality is that there is little interest on the part of manufacturers to undertake such studies on the continent which is unlikely to be a major market for the vaccine. Consequently, unless African scientists are proactive in engaging with the vaccine manufacturers, together with other stakeholders such as the WHO, the continent risks once again lagging behind by a number of years before it will be able to successfully advocate for timeous access to Covid-19 vaccines once these are licensed.
Although being involved in the clinical development of the Covid-19 vaccine pipeline does not necessarily guarantee immediate access to the vaccine for South Africa (or other African countries) should it be shown to be effective; it nevertheless generates evidence of the likely public health impact of these vaccines in our own context sooner than later. This could assist in disrupting the legacy of delaying the introduction of life-saving vaccines into Africa due to the lack of local evidence. Furthermore, it does place moral and ethical pressure on the vaccine manufacturers to prioritise the country for vaccine supply, should the studies contribute to the eventual licensure of the vaccine. Notably, for both of the Covid-19 vaccines currently being evaluated in South Africa, the Bill & Melinda Gates Foundation is funding Serum Institute of India, to develop manufacturing facilities to produce these vaccines, to accelerate timeous access to these Covid-19 vaccines to LMIC should the clinical trials confirm their safety and efficacy.
The emergent vaccine-nationalism in many high-income countries, pre-ordering at premium prices vaccines that are yet to be licensed and suggesting regulations to restrict the export of Covid-19 vaccines manufactured in those countries, is a further challenge to ensuring an equitable and timeous distribution of Covid-19 vaccines especially to LMIC.
To mitigate this, the Covid-19 Vaccines Global Access (Covax) Facility, which is co-led by the WHO, the Coalition for Epidemic Preparedness Innovations and Gavi, provides a possible pathway in assisting especially LMIC to gaining timeous access to Covid-19 vaccines. This will at least aim at providing access to sufficient numbers of Covid-19 vaccine doses to target populations at high risk of Covid-19 and frontline healthcare workers.
However, for countries such as South Africa to benefit from this initiative requires clear planning and commitment on the part of the government to provide the funds upfront to procure Covid-19 vaccines through the advanced market commitment model that is envisioned by COVAX. Delaying in doing so, unfortunately diminishes the country’s prospects of gaining early and timeous access to safe and effective Covid-19 vaccines. Also, not gearing up plans to access Covid-19 vaccines now is something that the country can ill afford, considering the health, economic and societal repercussions that the pandemic has already inflicted on South Africans and probably similarly elsewhere in sub-Saharan Africa.
Shabir Madhi is Professor of Vaccinology at Wits University. Daily Maverickis a media partner for the “Meeting the Challenge of Covid-19 in Africa” conference held virtually from 1-4 September and co-hosted by the Universities of Columbia and the Witwatersrand. This article is based on a keynote address made at the symposium.
Solid, altruistic global leadership is the only way to face future crises and win
- Martin Veller and Ames Dhai
Covid-19 has taught us that investing in health security research, preparedness and responsiveness, nationally, regionally and globally, is critical.
For this to work and to beat similar crises in future, effective, credible, altruistic political leadership at all levels of society is needed.
The world as we know it has changed, forever. The Covid-19 pandemic has achieved what a few outspoken voices had predicted. The emergence of the SARS-Cov-2 virus has affected every person in a multitude of ways, from restricting movement and changing interaction with others, to many losing their livelihoods and large numbers becoming infected and many of those infected, dying – more than 800,000 deaths have already been ascribed to the virus and evidence suggests that this is a substantial underestimation (in South Africa, the current level of excess deaths is three times higher than the number of deaths that can be ascribed to Covid-19).
It is, therefore, obvious that this pandemic is not just like any influenza epidemic (the 2009-2010 swine flu pandemic caused 300,000 deaths). On the other hand, fortunately, the lethality of this virus is modest when compared with the Spanish influenza pandemic of a century ago that cost between 20 million and 50 million lives and the more recent West African Ebola outbreak, where 11,000 deaths occurred among the 28,000 infected (a 40% case-fatality rate).
What is patently clear, is that such events, whether they are caused by natural evolution of an infective agent or are human-made, will recur. During this week’s virtual symposium organised by the Africa Centres for Disease Control and Prevention, Columbia University and the University of the Witwatersrand, titled Meeting the Challenge of Covid-19 in Africa, the key messages were:
That the world can overcome such threats if all nations and societies work in solidarity.
That tried-and-tested public health principles are effective. These primarily consist of using testing, tracing and isolation to reduce the rate of infections until vaccine-based prevention becomes available. Other methods to reduce the virus in circulation are also essential. In the case of droplet/airborne viral spread, this means limiting the movement of people, wearing facemasks, interpersonal distancing, enhancing dispersion of the virus by good ventilation and reducing the rate of transmission from hand to face by promoting effective and regular hand-washing.
That the only manner in which the SARS-Cov-2 virus will be relegated to becoming a seasonal, nuisance virus will be the development of effective population-wide immunity. To prevent undue mortality, this requires the development of effective, widely available vaccines.
That the world and every nation must be prepared and appropriately capacitated to prevent such threats from occurring, and if this fails, to thwart such events developing by rapidly implementing the public health interventions listed above.
That threats of this nature have lasting effects not only on the wellbeing of people and the world’s economy, but also on the world’s sustainability. The consequences are long-lasting and cures, if they exist, take time and large amounts of money to develop. Furthermore, the focus on the acute problem invariably has other downstream costs in disrupted health systems and economies.
Mechanisms to prevent and manage pandemics are, therefore, essential. This requires that all countries have an effective public health system that is well run, and is adequately and consistently resourced. These entities must be in the position to rapidly deploy, using the most up-to-date, evidence-based health interventions and technologies. Their ability to advise the decision-makers and the populace must be unrestrained and protected from political interference. Importantly, the most effective tool available to these agencies is their communication about preventive public health measures, the importance of societal solidarity and the value of vaccination. Such messaging must be trusted by everyone in society and it is mandatory that this has political ownership in the highest office.
This requires that governance at all levels of society is ethical, strong, thoughtful and accountable. Such servant leadership is not only essential to ensure the level of international collaboration needed to allow for an effective global response, but more importantly is the quintessential element in implementing the local interventions, which at times may be harsh and unpopular. Trusted management, based on transparent decision-making, using the best scientific evidence available at the time and subsequent quality trustworthy communications are much more likely to reduce the rate of spread of the virus. Without trust, no measure will be implementable, no matter how effective the local enforcement agencies are, particularly in societies that are deprived or under threat.
That trusted leadership works in reducing the number of SARS-Cov-2 infections and minimises Covid-19 mortality has been clearly demonstrated in a number of countries. On the other hand, where trust in leadership is patchy or does not exist, high infection rates occur. Similarly, when political leadership has been in solidarity with neighbouring nations, regional outcomes appear to be better. As the Covid-19 pandemic has again shown, the biosphere has no borders. This also means that with the possibility of Covid-19 vaccines being available in the near future, immunisation equity will be central to global health security. In contrast, vaccine “nationalism” will impede the development of global immunity and global distributive justice.
As we have seen, human tragedy from rapidly spreading infectious outbreaks is profound, with extensive health, economic and social consequences causing monumental human suffering. The painful statistic of lives lost is only the first measure of impact. Covid-19, like the 1918 Spanish flu, has underscored how vulnerable the world is. Therefore, investing in health security research, preparedness and responsiveness, nationally, regionally and globally, is critical, even when no imminent crisis is apparent. So what does this boil down to? That the management of any pandemic, which arguably is the biggest threat to the wellbeing and survival of humanity, requires effective, credible, altruistic political leadership at all levels of society. Above all, this leadership must be worthy of the trust placed in it. Anything less is paid for with lives, mostly by those who carry the burden of inequity and disadvantage.
Martin Veller is Dean of the Faculty of Health Sciences at the University of the Witwatersrand andAmes Dhai a Visiting Professor of Bioethics at the Wits School of Clinical Medicine and Specialist Ethicist at the Office of the President and CEO of the South African Medical Research Council. This article was first published in the Daily Maverick/Maverick Citizen.
The claim that SA’s economy has declined by 51% is a misrepresentation of the facts
- Imraan Valodia
South Africa’s Gross Domestic Product has not halved as reported by several publications and commentators over the past 24 hours.
Statistics South Africa (StatsSA) released the eagerly awaited Gross Domestic Product (GDP)estimatefor the second quarter of 2020 on Tuesday. In its ownsummary report, and in numerous press reports, the following is said: “South Africa’s gross domestic product (GDP) decreased by 51% in the second quarter of 2020 owing to the impact of Covid-19 lockdown restrictions since the end of March 2020.
Based on this report, a number of publications and commentators reported that South Africa’s GDP has halved as a result of Covid-19 (see this,for example).
So, let’s put some facts on the table before getting into the technical issues. We can safely say the following:
Covid-19 and the associated lockdown has had a devastating impact on the economy and the recovery process will be very tough.
While the impact across the globe has been uneven, South Africa is not alone, and is one of many countries where the impact has been severe.
The real number to focus on is the fall in the GDP between the first quarter of 2020 and the second quarter of 2020. Our lockdown was announced on 23 March and began on 26 March 2020 so, give or take a few days, the first quarter is pre-Covid-19, and the second quarter is post-Covid-19 and the lockdown period. In truth, the effect of Covid-19 began much earlier, with people changing travel plans, shortages of some personal protective equipment (PPE) and so on but, for simplicity, let’s ignore the effects prior to the announcement of the lockdown.
South Africa’s GDP in the second quarter, compared to the first quarter, did not fall by 51%. It fell by 16.4%.
While it is technically correct to say that, on an annualised, seasonally adjusted basis, GDP in the second quarter fell by 51%, in our current context, this is a highly misleading statistic. StatsSA should have published the report with the following health warning: “Before quoting this report, please take the time to understand the concept of an annualised quarterly GDP estimate. Oh, and please do think for a minute.”
So, how do we make sense of all of this?
In a normal world, for most economic data, including GDP data, we like to have the data annualised. This is mainly because annualised data allows us to compare data that is collected over different periods of time. This is clearly the case for GDP data.
StatsSA reports our quarterly GDP data on an annualised basis, as it did with the data released on 8 September 2020. In essence, the annualised data assumes that the quarterly trend of GDP would grow or shrink as if that rate of change is sustained over a period of 12 months. Since GDP growth compounds on itself, the calculation is a little more complex than multiplying by four (because we have four quarters). The data is then adjusted for seasonal patterns – hence, the annualised seasonally adjusted GDP growth rate. Ordinarily, from one quarter to the next, GDP data does not fluctuate dramatically, so the annualised data is a useful approach, and we can compare GDP growth rates in this annualised fashion.
However, in instances where the quarterly data may fluctuate in a dramatic fashion, as has been the case with the Covid-19 and the lockdown, this calculation, to annualise the estimate, is highly misleading, because it assumes that the economic effects of a lockdown will continue as it did for the second quarter, for four consecutive quarters. As Stuart Theobald has very usefully pointed out, the 51% fall is a result of compounding the quarterly 16.4% fall (in other words, -16.4 x -16.4 x -16.4 x -16.4). We know for certain that, while the third quarter data will not be good news, it will not be a fall of 16.4%, since the lockdown has eased. Moreover, since we will now be calculating the change between quarter three and quarter two, our comparator will not be quarter one data, but quarter two data, which is lower than quarter one data.
If you think this is all academic, think about what you would say if the quarter one and quarter two data were inverted – that is, if the economy grew in the same manner, rather than declined. The quarter on quarter growth rate would be about 20%, but the annualised growth rate would be over 100%! Correctly, if this were to occur and President Cyril Ramaphosa were to claim to be our economic messiah, we would accuse him of manipulating the facts. What is good for the goose must be good for the gander – the claim that South Africa’s economy has declined by 51% is a misrepresentation of the facts.
Of course, this is not in any way to suggest that we are not in a parlous economic state. Our economy has shrunk by 16.4% between March and June 2020 – that is a massive fall in GDP. Covid-19 and the lockdown has had a devastating impact on our economy. As a nation, over the period, we have lost R512-billion! It will take many years to recover from this. But, anyone who tells you that our economy has halved is misleading the public. The best estimates we have suggest that GDP for 2020, compared to 2019, will fall somewhere between 8% (the SA Reserve Bank estimate) and 10.4% (Intellidex’s estimate). Certainly not 51%!
Imraan Valodia is the Dean, Faculty of Commerce, Law and Management and Director of the Southern Centre for Inequality Studies, University of the Witwatersrand. This article was first published in Daily Maverick/Business Maverick.
Wits, GCRO, IBM and Gauteng Province opens Covid-19 dashboard to public
- Solomon Assefa and Zeblon Vilakazi
The Gauteng Province has been using data and cloud technologies to monitor and respond to Covid-19, and now they are sharing access with the public.
As of20 August 2020 the Gauteng Province in South Africa has 33% of the national cases for COVID-19 with 202,000 confirmed cases — and the numbers continue to rise.
To address this challenge, the Gauteng Province has been using a visual analytics platform developed by IBM Research Africa in collaboration with the University of the Witwatersrand (Wits University) and the Gauteng City-Region Observatory (GCRO). The dashboard visualizes anonymous data from multiple sources, including the University of Pretoria and GCRO, to help officials create policy based on data-driven decisions and to help the public understand their risk when they leave home.
The dashboard was designed to address three key questions for policy makers:
Where are the current hot spots of infection?
What are the predictions for the spread of the virus?
What are the risk factors that make certain communities more susceptible than others?
For example, using the dashboard we can see that the initial locations of the pandemic hot spots were in and around Sandton as business travellers returned from overseas. In April the virus began to spread to other districts in the province, and thereafter we can see that the hotspots have appeared in the Joburg CBD, Tembisa and Soweto. Such insights can help officials decide where health workers are needed and the type of intervention strategy.
Mduduzi Mbada, Head: Policy Research & Advisory Services Unit, Office of The Premier, Gauteng Province recorded a video for the Think Summit stating: “We believe this pioneering initiative will help us win the fight on flattening the curve, but also to build a strong public health system and bring back the economy because of the impact of COVID-19.”
In addition to data visualization, the dashboard also has a “what-if” prediction engine developed by epidemiologists and data scientists at Wits University. The engine provides predictions for different lockdown levels for non-pharmaceutical intervention control strategies. Highly sophisticated data analytics such as these can give officials the appropriate instruments of estimating how many beds and ventilators will be needed at the peak of the wave based on level of alert.
Policy makers can see the expected usage of hospital beds and the different kinds of health care setting using data from the Gauteng Province. Thanks to inputs from the Gauteng Province Department of Health, the dashboard gives a detailed account of the needs of the province as a function of time and location.
Starting today the platform isnow available for free to the public via the IBM Cloud. Using the latest Chrome or Firefox web-browsers anyone can access the dashboard to learn:
How many active cases are there in my neighbourhood?
When is the predicted peak for my neighbourhood?
Are the number of cases rising or falling in the area of my local supermarket?
“I am thrilled to see a U.S. company like IBM collaborate with Wits University to assist with the public-health response in the battle to defeat the COVID-19 pandemic. This is a best practice on how society benefits when government, academic and business collaborate. The All-of-America response reflects the generosity of American spirit and the importance of our partnership with South Africa in the long-run,” said Lana Marks, U.S. Ambassador to South Africa.
The research behind the predictive engine has been submitted for peer-review and is currently available in themedRxivoffers the following conclusion:
While lockdown measures have been successful in curbing the spread, ourstudy indicates that removing them too swiftly will result in the resurgenceof the spread within one to two months. Reducing the stringency index by 10will delay reaching the apex by about 6 months, where reducing it by 20 willdelay by only four. This indicates that post-lockdown measures should be stagedand the reduction of the stringency index should be slow.
Wits University pauses Oxford Covid-19 vaccine trial as part of standard regulatory procedure
- Wits University
Wits University will pause the Covid-19 vaccine trial it is running with the University of Oxford following a medical event in a volunteer in the UK.
The Ox1nCov19 trial, led in South Africa by Professor Shabir Madhi, Executive Director of the Vaccines and Infectious Diseases Analytics Research Unit (VIDA), will be paused as part of standard regulatory procedure designed to uphold the safety of participants.
Following a medical event experienced by a participant involved in the study of the ChAdOx1-CoV19 vaccine in the UK, the independent Data and Safety Monitoring Committee (DSMC) has recommended that all studies which they are overseeing pause further vaccination. This will allow the DSMC to undertake a thorough review of the case in the UK.
The details of the medical event that the participant in the UK experienced may not be divulged as this contravenes patient confidentiality.
Because the South African study is overseen by the same safety committee, all sites in the country have paused further vaccination.
“South African trial volunteers who are scheduled to receive either a first or second dose of the vaccine have been notified and we are in regular communication with them as to when vaccination will resume. This decision will be based on the DSMC’s recommendation. Ensuring the safety of all our study participants is our highest priority,” says Madhi.
“Pausing vaccination to review safety is evidence of the application of sound clinical practice and demonstrates the rigour of the independent oversight process under which this trial is being conducted. Assessing the safety of the vaccine is the reason why studies such as these are essential in South Africa, before there is widespread use of the vaccine.”
A spokesperson at the University of Oxford, which leads the trial in the UK and where a participant experienced the medical event, said:
“As part of the ongoing randomised controlled global trials of the coronavirus vaccine, our standard review process triggered a study pause to vaccination to allow review of safety data. This is a routine action which has to happen whenever there is a potentially unexplained illness in one of the studies, while it is investigated, ensuring we maintain the integrity of the trials. In large trials illnesses will happen by chance but must be independently reviewed to check this carefully. We are committed to the safety of our participants and the highest standards of conduct in our studies.”
About the South African Ox1nCov19 vaccine trial
Wits University announced South Africa and Africa’s first Covid-19 vaccine trial, the so-called ‘Oxford trial’, on 23 June 2020.
In South Africa, the study aims to enroll up to 2020 participants at up to seven sites in Gauteng and the Western Cape provinces.
In Gauteng, the sites are in Hillbrow, Soweto, and Tshwane.
In the Western Cape, the sites are in Cape Town and Stellenbosch.
The trial tests if the vaccine known as ChAdOx1 nCoV-19 is safe and able to protect people from developing Covid-19 illness.
The trial will also provide valuable information on whether the body generates good immune responses against the virus.
All South African trial volunteers have provided written informed consent to participate in the trial.
Participant safety a priority
Although the development of this vaccine is on accelerated timeline to address an unprecedented pandemic, the clinical development of the vaccine has built-in reviews processed by the independent international DSMC, as well as regulatory oversight locally by the South African Health Products Regulatory Authority (SAPHRA) and the University of the Witwatersrand Human Research Ethics Committee. The vaccine will only be licensed for use after adequate studies have been undertaken to confirm its safety and effectiveness.
Status of the South African Ox1nCov19 vaccine trial
The enrolment statistics of this trial as at 9 September 2020 are as follows:
2 886 volunteers screened
1 814 of required 2020 enrolled
1800 out of 1970 (91%) enrolled are HIV negative
14 out of 50 (28%) enrolled are HIV positive
About the ChAdOx1 nCoV-19 vaccine
The technical name of the vaccine is ChAdOx1 nCoV-19 because it made from a virus called ChAdOx1, which is a weakened and non-replicating version of a common cold virus (adenovirus).
The vaccine has been engineered to express the SARS-CoV-2 spike protein.
The vaccine was made by adding genetic material – called spike glycoprotein – that is expressed on the surface of SARS-CoV-2 to the ChAdOx1 virus.
This spike glycoprotein is usually found on the surface of the novel coronavirus and is what gives the coronavirus its distinct spiky appearance.
These spikes play an essential role in laying a path for infection by the coronavirus. The virus that causes Covid-19 uses this spike protein to bind to ACE2 receptors on human cells.
ACE2 is a protein on the surface of many cell types. It is an enzyme that generates small proteins that then go on to regulate functions in the cell. In this way, the virus gains entry to the cells in the human body and causes Covid-19 infection.
Researchers have shown that antibodies produced against sections of the spike protein after natural infection are able to neutralize (kill) the virus when tested in the laboratory.
By vaccinating volunteers with ChAdOx1 nCoV-19, scientists hope to make the human body recognise and develop an immune response (i.e., develop antibodies) to the spike glycoprotein that will help stop the SARS-CoV-2 virus from entering human cells and causing Covid-19.
A new app helps COVID-19 frontline workers with mental health
- Ashraf Coovadia and Shaegan Irusen
Pasha 80: Fighting the coronavirus can put severe strain on a person’s mental health.
Frontline workers in healthcare constantly have to deal with challenges of life and death importance. With this in mind, a team of researchers and health experts in South Africa developed an app to help healthcare professionals cope with anxiety and stress. The app connects healthcare workers to information, resources and each other. It recognises the importance of holistic protection.
In today’s episode of Pasha, Professor Ashraf Coovadia and Dr Shaegan Irusen, paediatric specialists at the University of the Witwatersrand, explain how the app works. They emphasise the importance of connecting with people and feeling more in control over an evolving situation.
Why halting the COVID-19 vaccine trial is part of the process
- Shabir Madhi
The experience of the Oxford vaccine and the measures put into place are not unusual. Many phase one and phase two clinical trials have holding rules.
This week the University of Oxford and Astra Zeneca temporarily postponed further vaccination in clinical trials of the COVID-19 candidate vaccine, AZD1222, after one of the participants fell ill. There are more than 15,000 participants already enrolled across multiple studies of the vaccine in several countries around the world, including 1,800 in South Africa. The Conversation Africa’s health and medicine editor, Ina Skosana, asked Professor Shabir Madhi, who is leading the South African leg of the trial, what these developments mean for the search for a vaccine.
Why was the trial suspended?
Pausing enrolment into a clinical trial is not unusual or unique to the COVID-19 vaccine. It happens often in the early phases of clinical development of investigational vaccines and other therapeutics, when there’s uncertainty as to the safety profile. For a COVID-19 vaccine to be licensed and recommended for use, it must be proven to be safe.
The decision to suspend trials came after one of the study participants in the United Kingdom experienced a medical event. The recommendation was made by the data and safety monitoring committee, which is independent of the investigators, and based on the stringent protocol criteria under which these studies are being conducted. The committee wanted to interrogate this particular medical event in more detail to determine whether it might be related to the participant having received the COVID-19 vaccine that is being evaluated.
In the clinical studies, participants receive either a placebo or control-vaccine, or the COVID-19 vaccine. The data and safety monitoring committee will be able to determine which of these the participant was allocated to. The committee – made up of clinicians, epidemiologists, and vaccinologists from the UK, as well as South Africa – will determine if this particular event might biologically be related to the participant having been vaccinated with the COVID-19 vaccine, or if there is another explanation for the event.
What are the next steps?
For the trial, the next step is for the data and safety monitoring committee to conclude whether this medical event might be related to vaccination.
The committee would also consider the severity of the episode. Even if the event were related to vaccination, the committee would need to judge the risk benefit profile of having other participants continue receiving the vaccine.
Many of the participants enrolled in South Africa have already started to receive the second dose of the vaccine or placebo. But we’ve suspended vaccination for those who were scheduled for a second dose. We’ll wait for the committee’s findings and recommendation as to whether and when vaccination can be re-initiated.
This interruption in completing enrolment into the study, as well as delays in administering the second dose at the scheduled time, is unfortunate. But it is necessary because the safety of the participants is of paramount concern to us. Should the data and safety monitoring committee allow the study to continue, it will likely set back the completion of the study by the equivalent of the period during which the study has been paused. But this interruption is unlikely to affect the integrity of the findings of the study.
What would it take for the trial to resume?
The decision to resume a study depends on the data and safety monitoring committee’s assessment. The committee has the prerogative to pronounce on this and, to a large extent, the investigators need to adhere to the committee’s recommendation.
We’ll also need the data and safety monitoring committee’s recommendations to be communicated to the local regulatory authorities. In South Africa this would include the University for the Witwatersrand and University of Cape Town Ethics Committees and the South African Health and Related Products Regulatory Authority. They will be engaged prior to further vaccination of study participants taking place in South Africa.
Only after that is done will we resume vaccination of participants. Those who are already enrolled into the study will continue with their routine scheduled visits, and will continue to be evaluated for COVID-19.
What also happens in studies of this nature is that if more participants experience medical events similar to those that resulted in the hold on further vaccination, those cases will also be reviewed by the data and safety committee in real time.
What about the other COVID-19 vaccine trials taking place in South Africa?
The Oxford vaccine is a different vaccine construct than the other vaccine that is being evaluated in South Africa. It’s a vector based vaccine, which is a different technology than that used for the vaccine developed by Novavax, which is the other vaccine being evaluated in South Africa. The Novavax vaccine is based on a more traditional approach of using only a protein (the spike protein) of the virus. These vaccines may also induce different immune responses.
There are a number of other vaccines also in clinical evaluation in other countries. Enrolment into those studies continues. Each of these studies has its own data and safety monitoring committee, which monitors – in real time – any serious adverse events that might be occurring. It’s a safeguard that is put into place to ensure the safety of participants. This is of paramount importance to the investigators as well as to the companies that are developing these vaccines.
So what were’re experiencing with the Oxford vaccine and the measures put into place is not unusual. Many phase one and phase two clinical trials have holding rules. And if those holding rules are met, it requires a review by the data and safety monitoring committee to make a decision as to whether the risk benefit profile is in favour of ongoing evaluation.
A balancing act between scientific data and health and broader socioeconomic implications is needed when policymakers prioritise interventions and measures.
The Covid-19 pandemic is complex and trade-offs are inevitable. As policymakers navigate these difficult trade-offs within a context of resource scarcity and broader uncertainties, there is a need for priority-setting processes that are evidence-based, as well as ethical and inclusive, to better inform these decisions. In addition, the Covid-19 crisis requires unprecedented social buy-in for interventions and measures to be effective. Much of this relies on meaningful public engagement.
The expectation on policymakers is to consider imperfect and evolving scientific data, take into account health and broader socioeconomic implications, and make appropriate and urgent decisions that will serve the best interests of the country. Even if the initial response to the crisis required an urgency that could not have aligned practically with meaningful public engagement, there areongoing decisions that will prevail even likely into 2022. These decisions will be based on extremely difficult trade-offs between health needs (Covid-19 and non-Covid-related), financial impacts on individuals, national economic impacts, nutritional consequences and growing inequalities, among others, and public engagement will be key to the success of these decisions.
In South Africa, where participatory democratic principles prevail and are protected in the Constitution, there is commitment to the active engagement of the public in thedecision-making processes of government, but in reality, this is challenging. Decisions are usually made by a handful of experts with minimal meaningful dialogue with those who are affected by these decisions. This can lead to a disconnect between government decisions and what is most important to the public.
When the legitimacy of the decision-making process is questioned, it results in low levels of public trust and acceptance of most measures to address the pandemic and mitigate its impact, even if many of these measures are evidence-based.
Public engagement in decision-making is important for transparency, at least to generate trust and buy-in. This in turn would increase the success rate of Covid-19 interventions. It would also manage expectations and improve public understanding of the various issues.
Beyond this, participatory community engagement approaches can assist in gathering insights into how the pandemic and related measures are impacting communities and what the social barriers and facilitators are of interventions, as well as gather ideas and garner active support for such interventions. This can assist decision-makers in developing solutions that are context-specific and more appropriate.
Public engagement, however, should go even further than this. In order for public priorities to influence policy-making in a more meaningful way, these priorities need to be positioned as trade-offs within a constrained budget. Through the use of deliberative approaches the public can be engaged in balancing trade-offs, and the justification behind these trade-offs can be understood.
There are different methods of public deliberation, but key components include providing participants with factual information that generates a shared knowledge base, ensuring that individuals with diverse perspectives are represented, and creating a setting wherelocal knowledge, values and moral claims can be voiced and challenged.
CHAT is designed like a board game and allows people to make collective decisions about what interventions are most important to them as a group, within a limited budget. The justifications behind the trade-offs are made clear through the use of CHAT. Alongside the scientific evidence, the epidemiological data and cost-effectiveness analyses which continue to evolve in relation to Covid-19, deliberative engagement tools like CHAT could be useful in considering social values in the decision-making process, leading to more active buy-in of interventions at community level. Other deliberative methods likecitizens’ juriesandmini-publicscould also play a role. The challenge of meaningful public deliberation in the context of physical distancing and soaring inequalities, where many do not have access to virtual platforms, would need to be addressed through innovative approaches that allow communities to congregate in meaningful ways so that health risks are mitigated.
By bringing the voices of decision-makers and the public together through deliberative engagement tools like CHAT, the priority-setting agenda can be determined not just by experts but also by the public. This could ultimately ensure priority-setting approaches for both routine health coverage decisions and pandemic responses that are not only evidence-based but also ethical, legitimate, sustainable and inclusive.
Aviva Tugendhaft and Karen Hofman are at the SAMRC/Wits Centre for Health Economics and Decision Science (PRICELESS SA), at the School of Public Health at the University of Witwatersrand. Rhian Twine is at the MRC/Wits Rural Public Health and Health Transitions Research Unit (Agincourt) at the School of Public Health at the University of the Witwatersrand. This article was first pubished in the Daily Maverick/Maverick Citizen.
Wits University resumes vaccinating in the Oxford Covid-19 vaccine trial
- Wits University
Wits University has resumed vaccinating in the Oxford Covid-19 vaccine trial currently also underway in the UK, Brazil and the U.S.
The South African Health Products Regulatory Authority and various South African universities’ ethics committees approved resuming vaccination in South Africa this week.
Vaccination in the Ox1nCov19 vaccine trial in the UK paused last week following a medical event in one trial participant in the UK.
A spokesperson for the University of Oxford said on Saturday, 12 September that the UK’s independent review process had then concluded and following the recommendations of both the independent safety review committee and the UK’s Medicines and Healthcare products Regulatory Agency, the trials will recommence in the UK.
Professor Shabir Madhi, Executive Director of the Vaccines and Infectious Diseases Analytics Research Unit (VIDA) who leads the Ox1nCov19 trial in South Africa confirmed today that vaccination resumed in South Africa on Tuesday 15 September, once local regulatory and ethics committees gave the go-ahead.
“The South African study is overseen by the same independent Data and Safety Monitoring Committee [DSMC] as in the UK so all sites in South Africa paused vaccination. The South African Health Products Regulatory Authority [SAHPRA] and local ethics committees have now approved resuming vaccination, and we have done so,” says Madhi.
Globally some 18 000 individuals have received study vaccines as part of this trial. In large trials such as this it is expected that some participants will become unwell and every case has to be carefully evaluated to ensure careful assessment of safety.
The University of Oxford spokesperson said, “We cannot disclose medical information about the illness for reasons of participant confidentiality.”
However, the DSMC review concluded that the event in the UK was unlikely to be related to the vaccination process.
“Pausing vaccination to review safety is evidence of the application of sound clinical practice and demonstrates the rigour of the independent oversight process under which this trial is being conducted,” says Madhi. “Assessing the safety of the vaccine is the reason why studies such as these are essential in South Africa, before there is widespread use of the vaccine.
Work from home reserved for the privileged few in SA
- Ruth Castel-Branco, Sandiswa Mapukata and Edward Webster
Digital divides ensure that only 11% of households have access to the internet.
Working from home is not new. Until the industrial revolution, most economic activities took place within the household. With industrialisation, the household remained a site of production, and employers outsourced tasks to homeworkers under the putting-out system.
The problem for the employer was the lack of control over the pace of work. The factory emerged as the solution; workers now had to travel to the factory and clock in. Though production became spatially separated from reproduction, they were tightly interlinked. As time became a commodity, the early struggles of factory workers were over the length of the working day.
Of course, in Africa, where 90% of workersare in the informal economy, factory work was always the exception. Though SA is comparatively more industrialised, home-based work remained widespread. Today, home-based workers are spaza shop owners, hair salon operators and outsourced textile workers. They are also crowd workers who use online platforms to connect with customers. And they are teleworkers in clerical, professional and managerial positions.
With the Covid-19 pandemic, home-based work has become pervasive. The shift enabled companies to continue to operate and workers to be paid. It also allowed for greater flexibility and more time with family. But working from home also poses risks including a return to task-based work, characterised by low and irregular income and benefits; an increased burden of paid and unpaid care work, particularly for women; and the risk of gender-based violence.
Ultimately, the ability to work from home is mediated by underlying structural conditions, including the nature of the labour market, the availability of affordable housing, and the accessibility of digital technologies. Across Africa, access to mobile phones, financial services and the internet reflect broader patterns of socioeconomic inequality between and within countries.
For instance, in SA more than80% of the populationhas access to a mobile phone. In Mozambique this figure is just more than a third. Access to cellphones is highest among men in urban centres and lowest among women in rural areas, though the degree of inequality varies. In SA, for example, men are 4% more likely to have cellphones than women, whereas in Mozambique the gender gap is as high as 14%.
When it comes to access to mobile banking and financial services, more SA women have access (70%) than SA men (68%). This runs counter to trends across Africa and may be due to the expansive nature of social grants, weighted towards women, which highlights the importance of government policy in bridging the digital divide.
Disparities are even larger when one looks at internet usage. In SA, 56% of the population has access to the internet. Men are 7% more likely than women to have access to the internet. However, if one looks at coverage at the household level, 11% of households have access. Though SA has higher levels of internet coverage than most countries on the continent, access to the internet is concentrated in a minority of households.
Unequal access to mobile phone and internet services prevents workers from meaningfully participating in online-based remote work. According to a survey conducted by Research ICT Africa,reasons for the digital divide include the exorbitant cost of mobile phones and data, inadequate network coverage and access to electricity, users’ limited literacy, and gender norms that discourage women from using cellphones.
The International Labour Organisation (ILO) estimatesthat less than 10% of SA can telework from home. It is still unclear how long the Covid-19 crisis will last. If working from home is to become a “new normal” states will have to invest resources in inclusive digital infrastructures. It will also be essential to ensure that home-based workers’ labour and social rights are protected. Theseinclude the application of the prevailing minimum wage, the correct employment classification and opportunities for career progression, freedom of association and collective bargaining rights, and the provision of social security benefits and maternity protection.
Of course, the nature of home-based work varies. Some workers are self-employed, others self-employed but dependent on intermediaries, and yet others effectively employed, even if the employment relationship is disguised as a commercial one. Concerned with the lack of regulation of home-based work the ILO extended worker rights to all home workers in 1996 (Convention 177).
Data on the scope, size and conditions of home-based work in SA is still minimal. However, if the Covid-19 crisis continues, home-based work may well become the next terrain of worker struggle.
The authors are researchers on the Future of Work(ers) project at Wits University's Southern Centre for Inequality Studies. This article first appeared in Business Day.
Covid-19 Update 46 - Level 1 is here
- Wits University
We welcome the news that South Africa will move to national lockdown level 1 from Monday, 21 September 2020.
However, given that we are still in the midst of a pandemic, let us continue to remain vigilant, and to follow all regulations and protocols in order to stave off a second wave of the coronavirus.
Implications for staff and students
We have received many queries pertaining to the return to our campuses and residences (including emails from international students), the continuation of the emergency remote academic programme (contact and/or online teaching and learning), and the mode of the upcoming examinations.
We are waiting for the Minister of Higher Education and Training to announce level 1 regulations for the sector. In the interim, please note the following:
The academic programme will continue as is, unless you are notified otherwise by your faculty,
Your school/faculty will advise you directly about the mode of your examinations,
You should only return to campus if you receive an invitation (and permit) from your faculty,
International students should not return until we have clarity on the regulations from the Ministry,
Students who are invited to return to residences will be issued with permits, and
Staff members should return if requested to do so by their line managers.
Please note that staff and students who are at risk due to co-morbidities should not return to campus, and should follow the University’s policies and protocols in this regard.
A further announcement will follow next week, once the Ministerial regulations are announced.
Update on student and staff infections
One staff member and three students reported testing positive for COVID-19 during the past week. These include staff members who are working from home. This is out of a population comprising of approximately 5 500 permanent staff and 37 500 students. Affected staff members and students are self-isolating in line with governmental directives and University protocols.
of infections
10 Sept – 17 Sep
22 June – 17 Sep
Staff
1
104
Students
3
187
News and Analysis
For the latest COVID-19 news, opinion, analysis and updates from Wits, please visit www.wits.ac.za/covid19.
COVID Alert SA App
President Cyril Ramaphosa has encouraged all people living in South Africa to download the free exposure notification COVID Alert SA app. It lets you know when you have been in close contact with someone who has tested positive for COVID-19 in the last 14 days.
#JerusalemaChallenge
The President also encouraged people to participate in the Heritage Day #JerusalemaChallenge. No need to rush to the Library Lawns – simply tag #WitsJerusalemaChallenge on Twitter, YouTube, Facebook or Instagram once you have mastered your moves.
You will receive a further update next week, once the new regulations are announced.
Take care
SENIOR EXECUTIVE TEAM
18 SEPTEMBER 2020
Covid 19 Update 47 - Preparing to return to campus under Lockdown Level 1
- Wits University
The Senior Executive Team (SET) met this week and agreed in principle to the coordinated return of more students and staff to our campuses from 5 October 2020.
In order to protect staff and students, this will happen in a controlled manner, under strict conditions, in line with level 1 lockdown regulations and the University’s COVID-19 policies and protocols.
Consultation with the relevant internal stakeholders is underway, in order to ensure that all health and safety protocols are in place, and to determine which cohorts of students and staff should return to our campuses and residences. A further communique will be sent out next week, detailing these decisions (including specific plans for international students). In the interim, the academic programme continues online. For now, students should only return if invited to do so by their respective faculties or the Dean of Student Affairs. Staff members must return if requested to do so by their line managers.
Update on student and staff infections
Three students reported testing positive for COVID-19 during the past week. This is out of a population comprising of approximately 37 500 students. Affected students are self-isolating in line with governmental directives and University protocols.
Thank you to all the students and staff who participated in the #ShowYourRoots Campaign. Check out the fabulous images and videos on the Wits Facebook and Instagram pages.
Look out for emails detailing the level 1 return to campus plan.
SENIOR EXECUTIVE TEAM
25 SEPTEMBER 2020
How social security could make life better in SA after COVID-19
- Stephen Devereux and Alex van den Heever
Emergency relief measures were operational for six months and are due to end soon. But the impacts of COVID-19 will be felt long after.
The national state of disaster declared by the South African government on 15 March 2020 was a direct response to COVID-19. But that response inadvertently intensified three other existing disasters: poverty, unemployment and inequality. More South Africans are poor and unemployed now than before the lockdown was imposed. But some people in government and the private sector are richer than before, thanks to tender corruption and price gouging.
Six months later, South Africa is at a low lockdown level. This is the “new normal”. But the hardship and vulnerabilities that COVID-19 created or exacerbated are not normal, and people still need government support. It’s needed on at least three levels: humanitarian response, structural poverty reduction policies and economic recovery stimuli. At a recent webinar hosted by the DSI-NRF Centre of Excellence in Food Security, we agreed broadly on four priorities for social security in South Africa, to “build back better” after COVID-19.
1. Make COVID-19 emergency relief measures permanent
Recognising the social and human costs of the pandemic and the lockdown, the government announced interventions to provide protection. These included top-ups to existing social grants (R250 a month), a caregiver grant (R500 a month), a COVID-19 Social Relief of Distress grant (R350 a month), a Temporary Employee Relief Scheme, and food parcels.
These emergency relief measures were operational for six months and are due to end in October 2020, but the impacts of COVID-19 will be felt long after. The lockdown shut down both the supply- and the demand-side of the economy simultaneously. At least three million people lost their jobs or livelihoods in the first month of lockdown, and with the negative economic consequences predicted to last for at least the next three years, that number is more likely to rise than fall.
There is no case for withdrawing the special relief programmes at this time. Social grants should continue to be paid at their higher levels, and the caregiver and Social Relief of Distress grants should be made permanent. Working age South Africans also need and have a constitutional right to social assistance.
2. Introduce basic income support
COVID-19 exposed a huge gap at the heart of South Africa’s social security system: the lack of any form of income support for low-income or unemployed people aged 18-59.
The lockdown forced economically active adults to sit at home for months. The less fortunate (usually poorer) had no income and, especially in the case of informal workers, no access to unemployment benefits or temporary employee relief. Millions applied for the special Social Relief of Distress grant, but R350 a month is not enough to live on.
Unemployment protection needs to expand to cover all workers, regardless of their prior employment status.
Income support should also be connected to labour activation strategies. Until this happens, in the absence of social insurance for workers in the informal sector, we support the campaign led by a coalition of civil society organisations for basic income support. This should be paid at the upper-bound poverty line of R1,227 and linked to a system of labour activation.
3. Overhaul the social security system
One lesson from the COVID-19 response – not only in South Africa – is that it is simpler and more efficient to build on existing systems than to set up new programmes in the middle of a crisis. Topping up the social grants was straightforward and worked best of the emergency relief measures.
The process of verifying applications for the COVID-19 special grants was slow, error-prone and, according to the Auditor-General, susceptible to the abuse and mismanagement of funds. In September the Temporary Employer-Employee Relief Scheme and several senior managers of the Unemployment Insurance Fund were suspended. Many COVID-19 food parcels were also stolen or diverted by local government officials.
This has generated another important lesson from COVID-19. All these schemes have been found wanting in terms of their delivery capability. The entire social security system needs to be reviewed: its criteria, online registration, payment methods and monitoring. It needs linked registries of beneficiaries, entitlements and contributions. Officials must be held accountable. All social security agencies must be supervised independently of political office-bearers.
4. Launch a national conversation about social security
What social security are poor and vulnerable South Africans entitled to? The constitution provides for access to all to adequate food and water, healthcare, housing and social security. But the right to social security, while referred to in the Bill of Rights, is not formally defined in any law. Conceptual and legal clarity is needed about what is meant by social security in South Africa. It is broader than just the right to grants.
South Africa does not have a social security policy or strategy. The White Paper for Social Welfare dates from 1997. The National Development Plan of 2011 notes the gap in protection. Only about 7% of unemployed people are covered by unemployment insurance.
The constitutional right to social security or social protection has two components: coverage and adequacy. Coverage must be universal, but the support provided must be enough to ensure that people can survive with dignity. Benefits must relate to the cost of a decent standard of living.
There is a deep conservatism among policymakers about giving income to working-age people. But COVID-19 has changed this. Recognising that unemployment in South Africa is structural makes giving income support to the working-age unemployed unavoidable, not only during the COVID-19 lockdown but in the long term. This opportunity to reconfigure the social contract around social security must be embraced.
Conclusion
The Treasury and the Minister of Finance will complain that extending the emergency relief measures and introducing new grants is unaffordable. South Africa was already facing a fiscal crisis before COVID-19, with low growth, rising government debt and falling tax revenues. Increasing social spending would increase the deficit.
On the other hand, there is an economic argument, supported by international evidence, in favour of positive growth effects of social grants. Injecting purchasing power into poor households will stimulate demand and assist economic recovery. Reimagining social security in South Africa is not only a humanitarian imperative and a means of achieving social justice, it makes economic sense. It is something that the country cannot afford not to do.
Wave 2 of the Nids-Cram survey shows how women have fared with the gradual reopening of SA’s economy as the lockdown levels are eased.
In the 2008 recession men were disproportionately affected by job losses, but the Covid-19 pandemic has hit women more severely, with the crisis now frequently referred to as a "she-cession".
One of the main reasons for this is that women and men continue to be concentrated in different parts of the economy, and many of the hardest-hit sectors have been those that typically employ large numbers of women (tourism and hospitality, retail trade, personal care, domestic and child-care services).
Another reason for the disproportionate effect on women has been the concurrent crisis in child care as a result of school closures. Given that women were more likely to care for children pre-Covid, it is not surprising that they have borne the brunt of additional (unpaid) care work at home.
Data from the first wave of the Nids-Cram survey showed women in SA were especially hard-hit by the crisis during the first month of the lockdown. Though women accounted for less than half (47%) of employment in February, they accounted for 2-million, or two-thirds (67%), of the 3-million net job losses that were recorded between February and April.
In addition, women were found to have taken on more of the extra child-care work in April. This was because women in SA are much more likely than men to be living with children. But even among male and female respondents living with children, women reported spending more hours on extra child care than men.
The release of Nids-Cram wave 2 provides the opportunity to track how women have fared as the economy started to reopen.
The "good" news is that, in the labour market at least, their situation relative to men didn’t deteriorate with the move from level 5 to level 3 of lockdown. There was hardly any difference in the net jobs recorded between April and June, and if anything, women may have gained a bit relative to men.
Nonetheless, women remain well behind men in reaching their pre-Covid employment levels. Women’s employment was still down 20% in June against February, while men’s was down 13% (see graph).
In total, women accounted for 58% of the net job losses that occurred between February and June.
A worrying finding is that even though women were overrepresented among the job losses, they were underrepresented in the income support received in June. Only 41% of the beneficiaries of the Unemployment Insurance Fund (UIF) or the UIF temporary employer/employee relief scheme, and 34% of those who had been paid the new Covid-19 social relief of distress grant (SRDG), were women.
It is likely that fewer women received the SRDG because it can’t be held concurrently with another social grant, such as the child support grant.
It means unemployed women are effectively being penalised if they are also the main caregivers to children, raising questions about the fairness of SA’s social protection system.
The time-use data collected in wave 2 suggests men benefited more from the return of some school grades and child-care services in June.
That many men were also spending more time on child care during the first phase of the lockdown has led a number of people to ask if this might be a transformative moment for society. This unprecedented "social experiment" within households might lead to a longer-term redistribution of care work if men form new attachments with their children or become more accustomed to child care.
The study’s results cast doubt on this idea: men seem to be reverting to pre-Covid child-care levels faster than women as the economy reopens.
This reflects in the responses individuals gave when asked how child care during the lockdown had affected them. Twice as many women as men (about 3.4-million vs 1.7-million) said child care negatively affected their ability to work, to work the same hours as before lockdown, or to search for work.
From the evidence we have so far, the pandemic and ongoing lockdown are having a much more severe effect on women and their prospects in the labour market. This threatens to reverse some of the (slow) gains towards gender equality over the past 25 years in SA.
As we regrow our economy, there needs to be a focus on helping women regain their jobs. Until then, women need to be provided with income support to help compensate for the haemorrhaging in the labour market.
Daniela Casale is an Associate Professor in the School of Economics & Finance at Wits University; Debra Shepherd is a Senior Lecturer in the Economics Department at Stellenbosch University.
Our results show that the prevalence of depressive symptoms seems to have doubled between 2017 and June 2020 (Covid-19 era).
Specifically, while 12% of South Africans screened positive for possible depressive symptoms in 2017, when those same individuals were resurveyed in 2020 (June/July 2020), this had increased to 24%.
The negative impact of the Covid-19 pandemic suggests that it disproportionately affects vulnerable groups in terms of income and health. Studies have shown that the impact of the pandemic in terms of job and income loss vary by factors like gender, race, and type of employment (Spaull & the NIDS-CRAM team, 2020). Furthermore, it has been argued that poor health is more concentrated among the poor relative to the pre-Covid period with hunger, income inequality and employment status explaining the inequality (Nwosu and Oyenubi, 2020).
One aspect of health that is often less researched but is particularly important in the context of the pandemic is mental health. Prior to the pandemic, problems related to mental health generally received little attention. This has to do with resource constraint, cultural barrier and cost of training clinicians (Kagee,et al, 2013). However, given the expectation that the pandemic and associated lockdown imposes additional mental health burdens (see Galeaet al,2020; Vindegaard & Benros, 2020), policy makers need to pay attention to the short and long-term effects of the pandemic on mental health.
We explore how the distribution of depressive symptoms in 2020 (Covid-19 era) has changed relative to the pre-Covid-19 period (2017), and how variables known to be correlated with depressive symptoms (eg gender and employment status etc) explain these changes. It is important to note that in our data, depressive symptoms are measured with screening instruments. While these instruments provide a way to measure likelihood of being depressed, they are not to be confused with clinical diagnosis of depression. Broadly, the pandemic precipitated (i) health and (ii) financial concerns which may have an adverse effect on mental health. This is because the pandemic and the associated lockdown introduces new stressors. For example, preventative measures like social distancing and frequent hand washing may be harder to observe in poor communities because of overcrowded spaces and poor service delivery.
Our results show that the prevalence of depressive symptoms seems to have doubled between 2017 and June 2020 (Covid-19 era). Specifically, while 12% of South Africans screened positive for possible depressive symptoms in 2017, when those same individuals were resurveyed in 2020 (June/July 2020), this had increased to 24%. Contrary to what one might expect, the largest increases in reported depressive symptoms are found among historicallyadvantagedgroups with many of the pre-existing gaps in reported depressive symptoms (between men and women and between rich and poor) seem to have disappeared. However, we note that the narrowing of the gap occurs at a higher level relative to 2017. For example, it is not that the poor show less depressive symptoms relative to 2017, rather depressive symptoms have increased even more among the rich to narrow the gap.
We identified subjective risk perception, social grants, household structure and Covid-19-related employment transition as some of the factors that are correlated with depressive symptoms in 2020. Specifically, while subjective risk perception is positively correlated with depressive symptoms for affluent individuals, number of grants receipts and household size is negatively correlated with depressive symptoms for the less affluent (we think the former has to do with the increase in grant payments). Even after controlling for all the above-mentioned factors, hunger and hunger severity remains an important factor. Those who reported that someone in their household went hungry in the last seven days are more likely to screen positive for depressive symptoms. In addition to experiencing any hunger, respondents that reported perpetual hunger (“Every day” or “Almost every day”) had twice the prevalence of depressive symptoms (42%) compared to those who experienced hunger one to two days a week or not at all (about 23%).
Source: Oyenubi and Kollamparabil, 2020
Policymakers need to pay attention to the impact of the pandemic on emotional wellbeing and mental health and make adequate provision for what may be an upsurge in acute mental health issues that could, if not addressed, become chronic and prolonged.
Emerging patterns from economies that opened up earlier than SA (European countries) are anything to go by, one cannot rule out the possibility of lockdown in future. Policies that address hunger like the food feeding programme should be operational even in the event of another lockdown. The enhanced social grants and the Special Covid-19 Social Relief of Distress grant have played a major role in mitigating the devastating effect of the lockdown on the economically vulnerable. The government needs to seriously consider extending these interventions beyond the intended period.DM/MC
Adeola Oyenubi (PhD) is a Senior Lecturer at the School of Economics and Finance, University of the Witwatersrand. His research interest includes Development and Mathematical Economics. Uma Kollamparambil is the Head of School of the School of Economics & Finance at the University of the Witwatersrand. This article was first published in Daily Maverick.
Covid-19 Update 48 - Return to campus under lockdown level 1
- Wits University
Covid-19 policies and protocols pertaining to lockdown level 1.
Following the publication of lockdown level 1 regulations, in line with the University’s COVID-19 policies and protocols, and after consultation with internal stakeholders, the Senior Executive Team (SET) agreed to the following as from Monday, 5 October 2020:
Academic Programme
The teaching and learning programme will continue online as far as possible.
Selected cohorts of students who are required to participate in contact teaching, laboratory/studio work, additional classes, and/or field trips, may return as determined by academics and faculties. All academic activities for these specific groups of students must be conducted with the requisite COVID-19 health and safety protocols in place.
Students will participate in online assessments and/or sit-down examinations, which will be stipulated in the schedules due to be published on the Examinations and Graduation Office website on the 16th of October 2020.
Return of day students
Students are encouraged to continue studying online and from home as far as possible.
However, following requests from some day students to return to campus (some of whom find it difficult to study at home), all libraries (except the Education Library, due to construction), selected large venues and selected computer laboratories will be made available for study purposes from Monday, 5 October 2020 until the end of the examination period. Venues not cleared for day student occupancy may not be utilised under any circumstances.
Permits will not be required but access to all facilities will be limited to ensure physical distancing and the adherence to health and safety protocols. Security officers will manage traffic, disband congregations and gatherings, and/or deactivate access cards if required.
Return of residence students
The return to residences is by invitation only. In order to reduce the risk of infection in residences, it has been agreed that a total of 5 000 students will be accommodated. Preference will be given to returning international students and students who find it difficult to study from home. Insofar as possible, students will be placed in single occupancy rooms. No visitors will be allowed entry into residence rooms.
All shared facilities will be cleaned and managed in accordance with COVID-19 health and safety protocols. Take-away meals will continue to be provided, whilst the possibility of opening dining halls and staggering meal times is explored.
Buses are only allowed to be filled to 50% capacity and students must adhere to this rule. Intercampus buses will be scheduled to run more frequently.
Return of international students
International students who are permitted to enter the country under lockdown level 1 regulations, are permitted to return to campus and residences. A separate letter will be sent to international students.
Return of staff
University services will resume from 5 October 2020 and all professional and administrative staff will be required to return to work as directed by their line managers. Professional and administrative staff who can work productively from home may do so, with the express permission of their line manager. Managers are required to submit revised risk assessment and mitigation plans, which must be approved by the assigned Occupational Health and Safety Officer BEFORE staff return to the workplace. In open plan areas and congested spaces, staff may be required to return on a rotational basis, as determined by senior managers and Occupational Health and Safety Officers.
Academics will continue with the academic programme online insofar as possible, or via contact teaching, as agreed with their respective Head of School. Academic staff may return to work in their offices/laboratories with the permission of their respective Head of School.
No permits will be required for staff members to access campuses.
Staff with co-morbidities (as determined by a medical practitioner or the Wits-appointed healthcare practitioner based at the WDGMC) and as described in the HR Practice Note on this matter, should for the time being, with the approval of their line manager, work productively from home and undertake work that is assigned to them.
Meetings will continue to be conducted online where possible, and face to face meetings will be limited. No congregations in bathrooms, kitchens, tearooms and other spaces is allowed.
COVID-19 health and safety protocols
Any person who enters Wits’ campuses must do the following:
Complete the screening form on the Wits Logbox App every day before entering campus,
Enter using a staff or student card, which will serve as a permit,
Wear a face mask that covers the mouth and nose at all times,
Practise good hand hygiene, and
Maintain a physical distance of at least 1.5m to 2m from any other person.
Anyone who does not comply with these regulations will be asked to leave the campus immediately.Please report any violations to your nearest Campus Protection Services Office or call (011) 717-4444 or (011) 717-6666.
Retailers, contractors, visitors and suppliers
All retailers will resume trading with the necessary health and safety protocols in place. Inspections will be undertaken by OHS&E and Services Staff to ensure that all regulations are being followed. All contractors, suppliers and visitors will require permits that can be issued by the relevant senior managers for whom they are working or visiting.
Our collective responsibility
The lockdown restrictions may have eased but the coronavirus is still in our midst and it is up to us to prevent a resurgence of the pandemic. The return to campus plan described above can only work if we all observe health and safety protocols. We will carefully monitor the situation in the coming weeks, and will intervene or amend these plans if the risk of infection increases. We appeal to all staff and students, out of mutual respect for one another, and the collective health and safety of our community, to follow the rules above (and to encourage others to do the same). Now more than ever, it is up to us to care for one another and to act responsibly, in order to protect ourselves and those in our community who may be more vulnerable.
Access the latest Wits COVID-19 news, research and resources via www.wits.ac.za/covid19.
Trial to test if measles, mumps, rubella vaccine protects healthcare workers against Covid-19
- Wits University
The measles, mumps, rubella (MMR) vaccine may strengthen immune response to viral infections, including SARS-CoV-2, which causes Covid-19.
South African scientists from the University of the Witwatersrand and the University of Cape Town are launching a clinical trial to test whether the childhood vaccine for measles, mumps and rubella (MMR) can protect frontline healthcare workers from Covid-19 or reduce the severity of illness for those who do become infected.
The MMR vaccine has been given safely to hundreds of millions of people around the world since it was approved nearly 50 years ago and successfully reduced the incidence of measles, mumps and rubella worldwide. Typically, the vaccine is given to children, with most getting two doses before age 6.
The research team leading the trial points to growing evidence that suggests that the MMR vaccine may have benefits beyond protecting against measles, mumps and rubella. It could broadly boost an individual’s immunity and may prevent infection from SARS-CoV-2 for a limited period. This is because the vaccine carries small amounts of live, weakened viruses that could train the body’s immune system to fight multiple pathogens.
“We know that the MMR vaccine is safe and we think there are two main reasons that it could prevent Covid-19,” says one of the trial’s national principal investigators, Sinead Delany-Moretlwe, a Research Professor at the Wits Reproductive Health and HIV Institute (Wits RHI).
“Firstly, this type of vaccine, which contains small amounts of very weakened measles, mumps and rubella viruses, appears to strengthen the body’s immune response to infections in general, not just to the viruses in that particular vaccine.”
A second reason the MMR vaccine may be effective is that there are similarities between the weakened viruses in the vaccine and the SARS-CoV-2 virus that causes Covid-19. All of these viruses have similar proteins on their surfaces that are involved in infecting cells in the body, so the researchers think that antibodies made in response to the MMR vaccine also may recognise and fight the SARS-CoV-2 virus.
Unlike the drugs remdesivir and dexamethasone, the only medications so far identified as being helpful in treating Covid-19, the MMR vaccine would not be used to aid recovery from illness. Instead, the researchers want to learn whether the vaccine can elicit an immune response that slows the spread of the virus and protects frontline healthcare workers who work in high-risk settings from developing Covid-19.
Professor Bruce Biccard, national co-principal investigator and second chair in the Department of Anaesthetics at UCT believes that this approach is complementary to the search for specific SARS-CoV-2 vaccines. “If we discover that the MMR vaccine can help train the body’s immune response to SARS-CoV-2 infection, then we will have something to administer very quickly, while waiting for more specific vaccines and preventive therapies to be developed,” says Biccard. “If the trial shows that the MMR vaccine can boost the body’s immune response, we believe it also may enhance the effectiveness of vaccines currently in development to prevent SARS-CoV-2 infection.”
The CROWN Coronavirus Prevention (CORONATION) adaptive trial platform launched as the global pandemic was beginning and is co-led by Washington University, USA, University College London, UK, and the University of the Witwatersrand in Johannesburg via the CROWN (Covid-19 Research Outcomes Worldwide Network) Collaborative, an international research network of physicians and scientists from institutions in Africa, Europe and North America.
The trial itself is funded by a $9 million grant from the COVID-19 Therapeutics Accelerator — an initiative launched by the Bill & Melinda Gates Foundation, Wellcome, and Mastercard with support from an array of public and philanthropic donors including the South African Medical Research Council. The Therapeutics Accelerator works to speed up the response to the Covid-19 pandemic by identifying, assessing, developing and scaling-up treatments. Its partners are committed to equitable access, including making products available and affordable in low-resource settings. The COVID-19 Therapeutics Accelerator will play a catalytic role by accelerating and evaluating new and repurposed drugs and biologics to treat patients with COVID-19 in the immediate term, and other viral pathogens in the longer term.
Recruitment of frontline healthcare workers
The study will recruit frontline healthcare workers from low- and middle-income countries like South Africa, Zambia, Zimbabwe, Ghana, and Uganda, as well as high-income countries like the USA, U.K, and Ireland.
Protecting the healthcare work force is critical in many of these countries where the health system is already constrained and could provide a substantial public health benefit both in sustaining the COVID19 pandemic response, as well as preserving other important health care programmes.
Professor Linda-Gail Becker, a professor of infectious diseases at UCT and an investigator on the trial believes that focusing on health care workers is essential: “We need to focus on frontline healthcare workers and their safety as the cornerstone to an effective pandemic response. South Africa also provides an opportunity for us to show whether this vaccine can protect healthcare workers living with HIV against Covid-19”.
Healthcare workers in the trial will be divided randomly into two groups. One will receive the MMR vaccine, while the other group will receive an inactive placebo. Healthcare workers can join the trial even if they received the vaccine as children. Each participant will be followed for five months, and the entire trial is expected to last about a year. Those previously sick with Covid-19, those who are pregnant and those who are taking drugs that suppress their immune systems or are seriously ill will not be eligible to participate. The South African team hope to enroll up to 5,000 health care workers in several sites in Gauteng, the Western Cape, Free State and Kwazulu-Natal.
Professor Helen Rees, executive director of Wits RHI in Johannesburg, responsible for international governance and coordination on the trial, believes that the trial will have important results for the region. “Many millions of people in the world received the MMR vaccine during childhood, and it is known to be extremely safe,” Rees says. “If this widely available vaccine turns out to be helpful, it could be a very important tool for protecting healthcare workers, and we need additional tools beyond personal protective equipment and good hand hygiene, which remain vital in fighting the pandemic.”
Chinese businesses donate personal protective equipment to Wits students
- Wits University
Members of the Chinese community in South Africa open their hearts to Wits students to protect them from Covid-19.
On 13 October 2020, the Wits Students’ Representative Council (SRC) accepted a donation of over 200 000 items of personal protective equipment (PPE) on behalf of Wits students from Chinese business associations in South Africa.
The donated items included six barrels of 25l sanitizers, four medical thermometers, and 200 000 face masks.
With the move to lockdown level 1 in September, Wits has permitted more students on its campuses as national lockdown regulations eased. The PPE will aid in protecting students from Covid-19 and curbing the spread of it on campus.
The handover ceremony was attended by members of the SRC, representatives from the Student Affairs Division, and donors including Ausma Electronics; Cheetahway Express Pty Ltd; Cindystar Group; Newedge Group; the South African Chinese Public Security Forum; the South African Minnan Chamber of Commerce (SAMNCCOM) as well as the Southern Africa Canton Hongkong and Macau Commercial Liaison Association. These businesses are part of the Southern Africa Chinese Public Security Forum that donated 10 000 disposable medical masks to medical students in May. The forum is led by NG Siu Hong, whose organisation was one of the biggests donors.
Humanity and care towards students
Jerome September, Dean of Student Affairs at Wits, expressed his gratitude to the Chinese community for displaying humanity towards Wits students during the Covid-19 pandemic.
September said that the pandemic has brought people and communities together in a quest to tackle Covid-19 collectively.
“What this pandemic has taught us is that, as a world, we cannot each one sit in our corners. We cannot be divided, we cannot live separated as if we are not one human species. What this pandemic has taught us is that we are interconnected in ways that we have never imagined before. It is in that interconnectedness that our full humanity sits. It is when you say you see a need, and you want to work with us. It is in that moment that the very best of humanity thrives, that the very best of humanity comes out of us.”
“We want to thank you for putting the needs of the students and the less fortunate at the forefront and for coming here today in solidarity and in friendship,” he added.
Hong, Chairperson of Southern Africa Chinese Public Security Forum that donated 100 000 face masks, said they felt compelled to protect students and they believe it is their mission "motivate them to pursue higher education." After receiving the request to donate PPEs for students from Dr Lizhi Huang, chairperson of the Wits Chinese Students and Scholars Society (WCSSS), Hong spurred the Chinese community in South Africa to also contribute.
"We are here to deliver our promises for building a better community and protect our students. Students can study with a peaceful mind, together with the continuation of the academic work, the future of South Africa is within the reaching distance," he said.
Meishuang Wang, Senior Vice-Chairman of SAMNCCOM, said such acts of solidarity and kindness would help in the fight against the pandemic.
“We as the South African Minnan Chamber of Commerce believe that, together as communities helping each other, we can get through these trying times. Our organisation will try to do all we can do to help ensure the safety of the staff and students who are returning to the University,” she said.
James Feng, CEO of Ausma Electronics, which donated 20 000 masks, said the PPE will aid in the successful completion of the academic year.
“Knowing that the students of Wits University are about to return to campus to complete this academic year, protective equipment is needed. The management of our company made a decision to respond to this need by making donations. Education is the foundation of this country and protecting students is to protect the future,” he said.
“We see the great value of education in other business development schemes. In the near future, Ausma is willing to offer assistance to Wits students for future career developments.”
Lai Lai Ng, CEO of Newedge Group and a philanthropist who has devoted part of her life to charity work, said the group’s donation is a reflection of its dedication to the advancement of society.
“As a mother of two children, my particular attention and care goes to the education of students. The health and happiness of a child is the source of happiness for a family. I hope that our donation could help a little bit in restoring the hopes of the families and restoring the smiling faces of all the hardworking students,” said Ng.
Fresh Yang Yu, CEO of Cheetahway Express, said that through their donation, the company strives to make a positive impact in communities.
“A good organisation must have a strong sense of social responsibility and a good spirit of making contributions to all other societies. We hope this donation is just the beginning for us to contribute to the values serving and repaying to the society,” said Yu.
Cheetahway donated 5000 facemasks and two medical thermometers.
Sophia Zhao, from the WCSSS, established in 2020, also expressed her gratitude.
“We will continue to work hard for the exchange between the youth of China and South Africa. I would like to express my sincere gratitude to the various institutions that donated supplies to Wits University.”
Zhao, together with Huang, chairperson of the Wits CSSS, Xiang Fan and Dr Hairong Wanga also from the society initiated and organised the event.
Looking to the future: From donations to development
The donation marked the beginning of a potentially long-lasting relationship between Wits and individuals and organisations who contributed.
In their speeches, donors expressed their keen interest in cultivating a strong relationship with the University that will contribute to their career development through their companies and other initiatives.
Cindy Xin An, CEO of Cindystar Group, who took English language courses at the Wits Language School after relocating to South Africa in 2008, said she has a great affinity with Wits and a personal appreciation of its high standards and quality.
“In the near future I am willing to help Wits students who are interested in building their education networks and help students find a suitable platform for career development.”
Similarly, Yu said that Cheetahway Express, as one of the leading brands for logistics in South Africa, would be interested in recruiting distinctive Wits graduates to help develop the South African E-commerce logistics industry.
Ng was looking forward to contributing to women development initiatives at Wits.
“In the near future, I hope to pay more attention to the development of women and the growth of girls at Wits. I am also willing to communicate more with the students of Wits. We could encourage each other, and make the world and campus a better place to live and study.”
New global health research to reduce the impacts of Covid-19 across low- and middle-income countries
- Wits University
Wits Health Consortium divisions - PRICELESS-SA, Agincourt and Ezintsha - secure grant in association with Harvard T.H. Chan School of Public Health.
The global health research grant will be used to measure unanticipated opportunity costs of South Africa’s Covid-19 response for children, mothers, and people living with non-communicable diseases (NCDs).
The grant is awarded to three collaborative Wits entities within Wits Health Consortium (WHC) in association with the Department of Global Health and Population Harvard T.H. Chan School of Public Health.
The Wits grant beneficiaries include PRICELESS SA (officially the South African Medical Research Council Centre for Health Economics and Decision Science-PRICELESS SA); Agincourt (the South African Medical Research Council/Wits Rural Public Health and Health Transitions Research Unit - Agincourt); and Ezintsha (a sub-division of Wits Reproductive Health and HIV Institute – Wits RHI).
Dr Atiya Mosam, Public Health Medicine Specialist, Senior Researcher at PRICELESS-SA and project lead on the National Institute for Health Research (NIHR)/UK Research and Innovation (UKRI) Global Effort on Covid-19 (GECO) grant project awarded to the Wits Health Consortium divisions, said: “Health systems across the world have had to pivot suddenly and with great speed in order to address Covid-19. Although this may have been effective in containing the pandemic, it has not been without consequence to the burden of disease and the health services that existed pre-pandemic. In South Africa, service delivery and access to care are constrained, even under non-pandemic conditions, and it therefore vital that the impact of Covid-19 on healthcare and the burden of disease is measured, so we can work toward a more effective and resilient health system under all circumstances."
Through a mixed-method, multidisciplinary study, these Wits Health Consortium researchers will investigate how Covid-19 has impacted the supply and demand of routine health services, specifically those related to non-communicable diseases, as well as maternal and child health, in both urban and rural settings.”
The project will quantitatively measure the impact of Covid-19 on routine preventive and curative health services, from supply and demand side perspectives, through a time series analysis of health service data.
The researchers will also qualitatively evaluate the views of the community and healthcare workers on health service access and delivery. These results will enable policymakers to make evidence-based decisions regarding resource allocation that are also responsive to community needs and priorities.
About the National Institute for Health Research/UK Research and Innovation Global Effort on Covid-19 (GECO) grant
The grant awarded to Wits is one of 12 made by the NIHR in partnership with UKRI for new research projects specifically aimed at tackling the multiple health consequences of the pandemic in low- and middle-income countries (LMICs).
The new research spans more than 18 countries across Africa, South America and South East Asia and covers topics such as transmission and infection control, and how people are affected by the disease in different settings and their long-term outcomes, including the risk of neurological problems. Other projects focus on the indirect consequences of the pandemic, for example on mental health, tuberculosis, and provision of HIV care and other health services.
In addition to its national role, the NIHR supports applied health research for the direct and primary benefit of people in low- and middle-income countries, using UK aid from the UK government.
Dr Lesong Conteh, chair of the funding committee GECO Health Research funding call and deputy chair of the Independent Scientific Advisory Group for NIHR's Global Health Research Portfolio, said: “Coronavirus does not respect borders, and the impact of the pandemic is being felt across the globe. These varied multidisciplinary new research projects will directly benefit people in low- and middle-income countries, provide learning opportunities globally, and complement NIHR and UKRI’s cross government approach to funding Covid-19 research in the UK.”
UK Research and Innovation (UKRI) works in partnership with universities, research organisations, businesses, charities, and government to create the best possible environment for research and innovation to flourish.
What South Africans must do to avoid a resurgence of COVID-19 infections
- Laura Rossouw and Carmen S. Christian (PhD)
It is key to continue high-impact non-pharmaceutical interventions that will not impede economic activity, but limit the spread of COVID-19.
South Africa’s stringent lockdown earlier this year may have saved lives by containing the spread of COVID-19. New COVID-19 infections have been declining and lockdown restrictions relaxed. But this has triggered fears of a new wave of infections.
Several countries have experienced a spike in infections following the easing of harsh lockdown measures. These include South Korea, Canada, Spain and the UK. Health systems are once again becoming overwhelmed, and countries have resorted to stringent lockdown measures once again.
The new round has been characterised by increases in cases – mostly driven by infections among younger groups – but not necessarily increased deaths.
To understand how the country might avoid this it’s useful to look at patterns of behaviour among South Africans after the initial easing of lockdown restrictions from level 4 to level 3 on the 1st of June. A further easing was introduced on the 17th of August, moving people from level 3 to level 2. This left only a few restrictions in place, such as mandatory mask-wearing, no international travel and a six-hour curfew at night.
In a survey done during July and August we found that more people were wearing masks than was the case when we conducted the survey in May and June. But this was coupled with a significant decrease in staying at home.
The survey findings signal trade-off in behaviours. This doesn’t bode well for the country as people adjust to life with virtually no restrictions. It is key to continue high-impact non-pharmaceutical interventions that will not impede economic activity, but limit spread. These measures include wearing masks, handwashing and physical distancing.
More must be done to re-inforce these preventative behaviours to avoid a surge in infections. This is particularly urgent given that South Africa’s early strict lockdown resulted in tremendous social and economic costs to the country.
But for these to be effective, high levels of public adherence are required. For instance, research has shown that to flatten the infection curve, 80% of the population must wear masks.
Why human behaviour matters
Human behaviour has been shown to play a significant role in the spike of infections, commonly referred to as the second wave. As restrictions on movement have been relaxed, social activities have increased. In South Korea, nightclubs have been identified as one of the biggest COVID-19 clusters in Seoul. There have also been outbreaks at several churches.
An increase in social night life has also been identified as a significant contributor in Spain. A recent cluster outbreak at a nightclub in Cape Town may signal the start of similar events in South Africa.
The findings of the survey we conducted don’t bode well.
The broadly nationally representative panel survey collected information on 7,073 South Africans in May and June. Follow-up surveys were conducted with 5,676 individuals in July and August. The two surveys coincided with the relaxation of lockdown regulations from alert level 4 to alert level 3. This included a return to economic activity for more jobs, outdoor exercise, reopening of restaurants and the gradual return to schools.
Our study found that between May/June and July/August this year, self-reported mask-wearing increased from 49% to 74%. The use of hand sanitisers increased from 10% to 35%.
But over the same period there was a drop in physical distancing (23% to 19%), avoiding large groups (16% to 7%) and staying at home (44% to 36%).
Author supplied
The one silver lining was that there was little evidence of respondents placing their trust in poor science. In the July/August survey less than 2% of respondents reported protecting themselves against COVID-19 by drinking hot lemon water and eating garlic. The number was only 1% in the earlier survey.
Going forward
The concern is that non-pharmaeucital interventions adherence among South Africans may decrease over time. Mask-wearing and physical distancing are among the more cost-effective and least disruptive measures of mitigating the risk of infection. As South African policy makers err on the side of caution and take steps to prepare for another wave of infections, non-pharmaceutical intervention adherence should remain top of mind.
COVID-19 messaging must continue to highlight the importance of adherence to these interventions. Wearing masks and avoiding large gatherings should be considered the social norm. The South African government’s mandatory mask-wearing policy, published in July this year, should therefore remain in place until a vaccine is accessible to all.
Messaging should target young people, warning them about the danger of transmitting the disease to vulnerable groups, including populations older than 60 and those with comorbidities.
Non-pharmaceutical intervention messaging should also contain specific and actionable recommendations, as these have been found to be more effective than generalist recommendations. For instance, messaging that reads “wear a mask when you go shopping” may be more effective than just “wear a mask”.
South Africa is a long way off from being able to rely on immunity from infection. In any event, the evidence on whether people can contract COVID-19 twice is still mixed, and accurately measuring immunity to the virus is difficult.
This underscores the need to take the precautions that have been shown to slow the spread of infection. This will not only reduce the number of people dying from the disease. It will also mitigate against the need to impose tough new restrictions on economic activity.
Covid-19 Update 49: Clarity on return to campus plans
- VCO
Answers to queries raised by organised labour and staff members.
Following the return to campus communique distributed yesterday, some staff members and representatives from organised labour raised specific queries, which are clarified below.
Staff over the age of 60 years
In line with national regulations and the University’s practice note around this matter, all staff over the age of 60 years should be enabled to work from home. Employees over the age of 60 who are not at high risk of infection, who do not have co-morbidities, and who are healthy, are allowed to return to the workplace at their own risk.
Risk assessment and mitigation plans
All managers are required to complete and submit risk assessment and mitigations plans to the occupational health and safety officer assigned to the entity BEFORE staff members return to the workplace. These documents (OHSE officers can provide the templates) must include plans to ensure that workplaces, including shared facilities like open plan offices and laboratories, change rooms, tearooms, kitchens and bathrooms are not congested. Line managers should use both the lockdown level 1 regulations and their discretion to ensure that staff are not put at risk. For example, staff working in open plan offices could be rotated to ease congestion in order to ensure that only half of the office space is occupied at any given time.
All risk assessment and mitigation plans must be approved by the assigned health and safety officer who will also conduct spot inspections to ensure that all health and safety protocols are in place. Should departments or managers not comply with these directives, they will be held to account, in line with the University’s rules, policies and procedures.
Discretion of line managers
Executives, school leadership, managers and supervisors are requested to exercise their discretion during this period and to be flexible around the starting and finishing times of staff members, particularly those who depend on public transport. For example, it may be useful to stagger the starting times of employees where possible, so that staff members avoid having to travel in congested buses, taxis and trains.
ACCESS TO CAMPUSES
Staff and students will no longer require permits to access campuses. However, all contractors, visitors and suppliers will require permits, which can be issued by the senior manager of the department or school that they are visiting or rendering services. The University’s gates will be operational as follows:
Braamfontein
- Yale North (Gate 7) will operate 24 hours
- Yale South (Gate 10) will operate 24 hours
- Sturrock Park (Gate 8) will operate 24 hours
- Enoch Sontonga (Gate 9) will operate from 07:00 until 19:00
- Station Street (Gate 2) will remain closed due to construction
Parktown Education Campus
The Victoria Road Gate will operate from 07:00 until 00:00.
Parktown and Health Sciences Campuses
These gates will remain operational as per the current status.
Drop Off Zones
All drop offs (including ride hailing services) will take place at identified drop off points outside the precinct.
STAFF AND STUDENT COVID-19 INFECTION SUMMARY
Three students reported testing positive for COVID-19 during the past week out of a population comprising of approximately 37 500 students. The affected students are self-isolating in line with governmental directives and University protocols.
Number of infections
25 Sept – 1 Oct 2020
22 June – 1 Oct 2020
Staff
0
104
Students
3
193
For the latest Wits CCOVID-19 news, research and resources, visit www.wits.ac.za/covid19
Covid-19 Update 50: Keep safe
- VCO
Appeal to adhere to safety regulations and preventative protocols.
We are appealing to staff and students to strictly adhere to the University’s COVID-19 preventative protocols. The coronavirus remains a threat and staff and students are required to:
- Fill out the screening form on the Wits Logbox App before entering campus,
- Wear a mask at all times, and
- Maintain a physical distance of 1.5m to 2m from anyone else.
Three staff members and six students reported testing positive for COVID-19 during the past week. This is out of a population comprising of approximately 5 500 permanent staff and 37 500 students. Affected staff members and students are self-isolating in line with governmental directives and University protocols.
Number of infections
2 - 8 Oct 2020
Total Infections 22 June – 8 Oct
Staff
2
106
Students
6
199
We appeal to all staff and students to act responsibly and in the best interests of the entire University community. Please abide by all the University’s COVID-19 rules, policies and protocols.
Update 51: Infection summary
- VCO
Latest update on infections and university protocols.
Two staff members and five students reported testing positive for COVID-19 during the past week. This is out of a population comprising of approximately 5 500 permanent staff and 37 500 students. Affected staff members and students are self-isolating in line with governmental directives and University protocols.
Number of infections
9 - 15 Oct 2020
Total Infections 22 June – 15 Oct
Staff
2
108
Students
5
204
We appeal to all staff and students to act responsibly and to abide by all the University’s rules, policies and protocols.
Anticipating a 'second wave'
- The Scientists Collective
Covid-19: When and how South Africa should try to prevent or mitigate it.
In recent days, health minister Zweli Mkhize has warned about a marked increase in new Covid-19 infections as a result of declining adherence to measures such as mask-wearing, physical distancing and hand washing. The United States and many western European countries are experiencing a dramatic resurgence, often called a ‘second wave’, of the coronavirus.
Does this mean a second wave is inevitable in South Africa?
In South Africa, the possibility of such a resurgence has seemingly justified the extension of the powers of the National Covid-19 Command Council (NCCC), under the legal framework of the National Disaster Management Act.
While this appears consistent with the country’s strategy, it is unwise to simply extrapolate outcomes from the current resurgences in Europe and apply them to South Africa, more so given the extra-parliamentary posture of the NCCC and concern over the lack of transparency in its decision-making process.
This abundance of caution is critical to avoid reflexive interventions for the ongoing management of the pandemic, especially in anticipation of a resurgence (or “second wave”) such as that being experienced in Europe and elsewhere.
It is imperative that knowledge of transmission and exposure patterns relating to SARS-CoV-2 in SA’s own setting must inform a calibrated and transparent response, not least because the most important component of the response is willing and voluntary compliance with mitigation measures by the public.
What is the rationale for European countries to impose lockdown strategies to manage the resurgence?
The United Kingdom, France, Netherlands and Spain have introduced a new round of curfews and are considering lockdowns as a means to contain transmission. Such interventions might well be effective in these and other countries, especially if they are able to support a lockdown from a societal and economic perspective.
These measures are also underpinned by the low levels of immunity in the general population in the affected regions. The majority of EU member states still have low levels of seropositivity (see Germanyhereand Spainhere) to antibodies directed to SARS-CoV2, ranging between 0.9%- 8.5%. Regions in some countries are outliers such as Austria, with more than40% seroprevalenceof Covid-19 antibodies detected in its populace due to heavy infection in the first wave.
These data suggest that in certain European countries, such stringent measures may retard transmission and therefore the overall number of cases and deaths.
Should the same rationale apply in South Africa?
We believe the context is different in South Africa.
Countries implement public health measures to get transmission under control. To get transmission under control, countries have two choices.
First, they can try to reduce transmission in order to reduce a peak health demand. This is calledmitigation. Mitigation can be achieved by isolating cases and quarantining close contacts (requiring a robust test and trace capability), adherence to social or physical distancing, wearing masks, hand hygiene and protecting that part of the population with the highest risk of serious illness if they are infected. Collectively, these measures are termed non-pharmaceutical interventions, or NPIs.
Second, a country might attempt to suppress the epidemic and attempt to stop transmission. This is calledsuppressionorlockdownand aims to reverse epidemic growth, reducing case numbers to low levels by physically distancing the entire population indefinitely.
Seven months into the pandemic, it is evident that while SA’s hard lockdown at an early stage of the epidemic initially slowed transmission, and that some healthcare facilities in certain areas of the country were able to prepare for the expected increase in admissions, this was uneven and did not manage to stop transmission. There is even less chance now of being able achieve sustained suppression of virus circulation in South Africa through a lockdown, than was the case when circulation initially started.
South Africa, despite having one of the earliest and harshest lockdowns for a protracted period of time did not achieve suppression, nor was it likely to.
The reasons for this are self-evident:
The lack of an integrated approach to the SARS-CoV-2 outbreak, from initiating community screening and tracking Covid-19 disease outcomes;
The inability to scale-up community testing in time, with concomitant long turnaround times and inadequate contact tracing that would enable the timely isolation of cases and close contacts. Contact tracing was not achieved at the scale required to suppress the epidemic, despite SA having one of the largest testing programmes in Africa.
Compliance with lockdown rules and NPIs suffered a trust deficit arising mainly from poor communication, heavy-handed enforcement and random bouts of misinformation from dubiously qualified private lobbies.
The international experience is illuminating.
Except for a few island nations, most countries failed to achieve sufficient viral control, whatever mitigation or suppression measures were applied. The World Health Organisation (WHO) actually concurred with the view of some local scientists who had cautioned against a hard lockdown as a primary strategy prior to its imposition.
It was clear that a lockdown alone will not eliminate or permanently control the spread of the virus unless it was coupled with an efficient system of testing suspected cases of Covid-19 and ensuring their isolation, as well as exercising a high level of contact tracing and their proper quarantine.
The reality is that the massive societal, economic and health resources needed to emulate countries like South Korea and China, which were initially able to achieve impressive levels of suppression, were not available to countries like SA. Moreover, while the rate of virus infection can be controlled through measures such as NPIs, adherence to even these measures are challenging in most low income settings where overcrowding is a grim reality, and even access to water is compromised.
Consequently, the highly restrictive and even coercive lockdown measures deepened social discontent the longer the measures were in place; the enforcement of which deepened mistrust of the authorities and may have contributed to poor compliance with mitigation measures in all groups and classes of society.
Alongside an inadequate testing and tracking infrastructure, this resulted in only a temporary reduction in community transmission of the virus over the first three to four weeks of the lockdown.
However, failure of being able to test for Covid-19 at scale in the public and private sectors, plus the incoherent prioritisation in the testing regime and the delay in turnaround times of tests, as well as the incapacity related to the tracing of contacts and their quarantine, have led to the predictable consequence that community transmission persists and may yet seed another increase in cases.
Reproductive Rate of the South African epidemic under various stages of lockdown
Source: National Institute of Communicable Diseases.
This persistence of transmission is evident through an analysis of the effective reproduction rate (Re) of SARS-CoV-2 as modelled by the National Institute for Communicable Diseases (NICD). The effective reproductive rate determines whether the number of cases of Covid-19 in the population will go up (when Re>1) or down (Re<1).
In South Africa, during the Level 5 lockdown, the Reranged from around 1.5 to 2, indicating ongoing community transmission even during the lockdown.
The Reonly declined substantially after the surge in July, following large scale exposure to the coronavirus in various communities in the Western Cape and Gauteng, thereby reducing the number of people susceptible to infection.
At the time of lockdown Level 3, up to 40% of the population in the Western Cape (and empirically a similar percentage in major urban metro areas in Gauteng) demonstrated evidence of SARS-CoV-2 infection, including presence of antibodies to Covid-19.
Seroprevalence surveys in Western Cape
Source: National Institute of Communicable Diseases.
Did lockdown or mass exposure to SARS-CoV-2 lead to subsidence of the first wave?
Data suggest any claim that the highly restrictive lockdown was successful in preventing community transmission of the virus, and contributed to the first wave waning, is inaccurate. Paradoxically, infection rates only started declining and the Retrended downward to approximately 1 from July onwards, as restrictions were being eased and social and economic activity increased commensurately.
The proposition that the interruption in the chain of transmission of the virus – due to an increasing proportion of the population being gradually infected over time and developing at least partial immunity – is supported by surveys undertaken across different districts in the Western Cape, where 40% of women attending antenatal clinics, and people living with HIV, had evidence of infection in different sub-districts, suggesting that a massive “covert” wave of infection, far greater than in Europe, North America or Asia (excluding South Asia), occurred.
Certain practices such as maximum taxi occupancy and resumption of attendance at places of worship, which were incrementally allowed during relaxation of the lockdown, undoubtedly increased the risk of virus transmission to people still susceptible to infection.
Despite some reluctance to comply due to inadequate communication coupled with harsh enforcement, the partial adherence to NPIs may have somewhat mitigated the potential consequences of these actions and was the most effective aspect of our public health interventions.
Notably, the recommendation by the previous ministerial advisory committee for the use of non-surgical face masks – and emphasising the potential airborne transmission of SARS-CoV-2 in South Africa – preceded WHO recommendations and advisories on these measures.
Paradoxically, the approach to lessening lockdown restrictions as the epidemic gained momentum in South Africa, likely led to a massive surge in coronavirus infections during our winter months, inducing at least some immunity in a high percentage of the population, particularly in densely populated areas.
This most likely led to an interruption in the chain of transmission of the virus in South Africa, which, together with at least partial adherence to NPIs, resulted in the first wave of the epidemic waning.
However, the proportion of the population that has been infected is likely far less than what is estimated (60-70%) to enable sustainability of low rates of infection (Rt<1.) – so called “herd immunity”.
There is also evidence of increasing complacency around the adoption of NPIs.
Therefore a resurgence of Covid-19, consequent to declining adherence, is likely to be experienced in the short term.Furthermore, uncertainty regarding the longevity of immunity following infection makes projections difficult on the future course of the pandemic.
What can we learn from other countries and does it predict what will happen in South Africa?
One observable similarity between South Africa’s and Europe’s epidemics has been a reduction in cases correlated with a change to warmer seasons. Although climatic factors may play some role in the transmission of SARS-CoV-2, the role of changing human behaviour in reaction to the weather is probably the deciding factor.
Spending more time outdoors and the ability to ventilate closed (taxis, trains etc) and indoor spaces is a critical factor.
One lesson, however, is important: the opening up of European societies during the summer months was likely coupled with less adherence to NPIs, which allowed for a resurgence of infections and Covid-19 hospitalisations.
In South Africa, our adherence to these tried and tested public health interventions to control Covid-19 must continue unabated. This is absolutely critical if we are to be spared the worst ravages of the kind of resurgence being witnessed in the northern hemisphere.
Different testing rates and testing strategies in many of the European countries (including Spain and UK), make it impossible for head-to-head comparison of the scale of the resurgence, relative to what was experienced in their first waves. Similarly, we cannot make meaningful head-to-head comparisons between (and even within) countries in respect of the number of infections or death rates that may result here.
This makes the task of gaining any insights into what could happen in South Africa inordinately difficult. After all, the hard lockdown initiated in SA followed the examples of China, South Korea, Iran and Italy, all of which experienced high-surge phenomena, even before the virus took hold in the South.
As we have noted above, this was perhaps not the optimal response, given what we already knew about local epidemiological trends and the extreme unlikelihood of countries in Africa being successful when aspiring for containment of a respiratory virus.
Resurgence is likely but our response should be different
A resurgence of Covid-19 is certain to occur in South Africa, although indications are that a second wave is likely to be different to the wave currently sweeping over Europe.
It is possible that, because a large percentage of people who live in major urban metros with a high population density have already been infected, this will assist in limiting the rate of transmission in such settings.
Put another way, a resurgence in settings where there was a high force of infection during the first wave, is likely to be of a lower magnitude than experienced with the first wave. Conversely, communities with low rates of infection in the first wave, may be disproportionately affected during a resurgence of Covid-19.
Seroprevalence surveys designed to characterise the proportion of communities that have been infected during the first wave in all sub-districts of South Africa will be a vital indicator of where a resurgence of infection might be concentrated.
Provinces and communities which experienced a lower rate of infection in the first wave may be settings for higher rates of infection and mortality in a second wave if mitigation measures are not implemented.
Strategies to meet this expectation, including smart, targeted and strictly limited restrictions, must be urgently devised and based on credible and swift seroprevalence surveys and a rational and outcome-driven testing programme.
Active adherence to public health measures and building robust test and trace infrastructure, as well as strengthening healthcare infrastructure in anticipation of an increase in cases, are likely to be the deciding factors in how well the country navigates resurgence of Covid-19.
What we can be certain of is that the type of hard lockdown imposed in March will only inflict further, perhaps fatal, damage to an economy which was on the ropes before the pandemic – and which the hard lockdown rendered moribund.
It will also significantly undermine any chance of an economic recovery, without achieving any meaningful net health impact.
It is, moreover, unlikely that a Covid-19 vaccine will be available to South Africa before the end of the next winter. Consequently, the only instruments in our current toolkit to blunt and minimise the consequences of a resurgence is to actively motivate society to continue adhering to NPIs.
Even if NPIs are not always implementable at scale in our own context, they nevertheless contribute massively to the control of the rate of transmission of the coronavirus and would assist in avoiding overwhelming the beleaguered healthcare delivery system.
It is axiomatic that only the people can overcome a pandemic, as observed throughout history.
It is, therefore, the work of governments to act in support of – and not second guess – the scientific and health system imperatives.
To single-mindedly focus on providing the people with all the necessary information and support, and to eschew self-serving political considerations in this effort, represents the most important contribution of South Africa’s political leadership in this time of crisis.
Professor Shabir Madhi, Respiratory and Meningeal Pathogens Research Unit, University of the Witwatersrand; Professor Glenda Gray, South African Medical Research Council; Professor Francois Venter, Ezintsha, University of the Witwatersrand; Professor Marc Mendelson, University of Cape Town; Dr Lucille Blumberg, National Institutes of Communicable Diseases; Dr Aslam Dasoo,Convener of Progressive Health Forum.
Update on the latest Covid-19 testing and infection of staff and students.
One staff member and three students reported testing positive for COVID-19 during the past week. These include staff members who are working from home. This is out of a population comprising of approximately 5 500 permanent staff and 37 500 students. Affected staff members and students are self-isolating in line with governmental directives and University protocols.
Number of infections
16 - 22 Oct 2020
22 Jun – 22 Oct 2020
Staff
1
109
Students
3
207
The data provided in the table above is based on the number of infections reported to the Occupational Health and Safety Office and the Campus Health and Wellness Centre as at 22 October 2020. Read about Wits’ COVID-19 reporting procedures, policies, rules, protocols, resources and updates at www.wits.ac.za/covid19.
Biomimicry control for Covid diagnostics
- Wits Enterprise
Wits researchers develop solution to improve accuracy and safety of Covid-19 testing.
Containing the scourge of Covid-19 requires testing of individuals, and isolating those who test positive, together with recent contacts, so as to prevent further spread. It is therefore critical to ensure that testing is independently verified so as to assure its accuracy.
Given the urgent need to ramp up testing, a team from Wits University’s Centre for Biomedical Tuberculosis Research (CBTBR) has developed a unique “control standard”, which does exactly this for certain diagnostic testing platforms. What makes it unique is that it uses biomimicry, a safer alternative to incorporating the actual SARS-COV-2 virus.
The Wits team, headed up by Professor Bavesh Kana, used this biomimicry technique to engineer a control organism that mimics the genetic material of the virus, when used in diagnostic tests kits. If the tests work correctly, the genetically modified organism is identified as being SARS-CoV-2. This control is a safe, non-pathogenic (non-disease causing), and stable. It can be rapidly deployed in a range of settings – from central laboratories to clinics across the country. In contrast, viral based controls require specialist shipping and handling procedures, and the need for highly skilled staff and infrastructure.
Kana says that accuracy testing controls are central to the deployment of any successful diagnostic test. “The virus continues to spread viciously across countries, with infections again rising rapidly across Europe and North America. In order for governments to halt its spread, reliable tools with verifiable results are of utmost importance. Without appropriate controls to report whether tests are delivering the correct result, diagnosing and effectively managing Covid-19 will be very difficult, if not impossible,” says Kana.
The pandemic has put healthcare systems across the globe under immense pressure, particularly on the issue of rapid diagnostic test development and implementation. Specific sections of the DNA is typically the targeted molecule for diagnosing bacteria and viruses. With certain viruses like HIV and SARS-CoV-2, the genetic material is contained in the RNA, and consequently diagnosis relies on the detection of the SARS-CoV-2 RNA.
Recognising the gap in the verification of Covid-19 tests obtained via molecular diagnosis tools, and understanding the risks and complications of using the live virus, Kana and his team: Dr Edith Machowski, Dr Bhavna Gordhan and Dr Christopher Ealand, heeded the call to support the fight against the pandemic, by developing control standards for diagnostics tools used in the testing of the Covid-19 virus.
Having previously contributed to the development of biomimicry based control standards for diagnostics for drug resistant tuberculosis (TB), which are now deployed in more than 20 countries internationally, the team embarked on a fast tracked research programme to develop the SARS-CoV-2 diagnostic control as early as February 2020.
“As SARS-CoV-2 is an RNA virus, the biomimicry process was not straight forward as compared to TB. This is due to the inherent instability of RNA. However, we have been able to include elements to produce a control that mimics the diagnostic profile of SARS-CoV-2, which is stable, effective and a safer alternative to using the live virus,” says Machowski.
Previous controls developed by Wits have been commercialised through a Wits spin-out company, SmartSpot Quality (Pty) Ltd. Dean Sher, Managing Director of SmartSpot, says that “Through our development and rollout of packaged controls for diagnostics for TB, SmartSpot is well geared to package the bulk stock of Covid-19 controls in its Wits developed control cards. Under licence to WITS, we will drive the roll out of the controls, and the ongoing external quality assessment programme.”
As result of the outstanding efforts of Kana and his team, as well as the long standing relationship between Wits and SmartSpot, the new controls are now deployed in the National Health Laboratories’ testing programme.
Kana says “We are grateful for the opportunity to contribute to the Covid-19 testing efforts within the country, and internationally, enabled by the support provided by Wits, funders including the National Research Foundation, Department of Science and Innovation, Technology Innovation Agency, South African Medical Research Council, and the Innovation Support Unit at Wits Enterprise."
Covid-19 pandemic drives need for policy brief on physical activity for health in Africa
- Wits University
More than ever, the Covid-19 pandemic has highlighted the need to prioritise physical activity as an imperative for public health in Africa.
Wits physical activity experts in the African Academic Consortium for Physical Activity for Health in Africa and the African Physical Activity Network (AFPAN) have contributed policy briefs to guide decision-making during the pandemic and beyond.
Government’s lockdown to restrict population mobility to minimise transmission of Covid-19 created a window of opportunity. Restrictions were met with resistance from civil society, fitness centres, gyms, and community organisations, clamoring to be allowed responsible access for physical activity and to create “activity-supportive” environments.
The need to message and provide guidance to governments and civil society, to implement national plans, policies and programmes to promote physical activity in the African region, both during Covid-19 and beyond, became critical.
The consortium, which comprises more than 40 academics, researchers and implementation partners from nine countries in Africa, prepared two policy briefs: one for the general public and one aimed at children in three environments – home, school, and in communities.
Exercise saves lives
Nearly 30% of the disease burden in sub-Saharan Africa is attributable to non-communicable diseases (NCDs). Some of the very diseases that place individuals with Covid-19 at much higher risk of being hospitalized or dying are the same lifestyle-related diseases that are associated with being physically inactive. In fact, the risk from dying from Covid-19 is 1.5 to 3.5 times higher for people with diseases such as Type 2 diabetes, high blood pressure or cancer - and approximately 18% of men and 25% of women in Africa are still insufficiently physically active to protect them from NCDs.
Research has shown that regular, moderate physical activity has been associated with reduced death from infectious diseases, a strengthened immune response, reduced inflammation and a lower incidence of viral respiratory infections. It also reduces depression and anxiety, both of which have escalated during the Covid-19 pandemic.
“The easing of lockdown measures and reintroduction of economic activity has helped to regain some sense of normality, despite the ongoing impact of the disease. The recent reopening of parks and recreation settings to the public has created obvious opportunities for leisure-time physical activity and exercise in a safe manner”, says Associate Professor Philippe Jean-Luc Gradidge in the Centre for Exercise Science and Sports Medicine (CESSM) in the School of Therapeutic Sciences at Wits and a member of the African Academic Consortium for Physical Activity for Health in Africa and AFPAN.
Gradidge, along with Wits scientists Dr Georgia Torres in the CESSM, Professor Lisa Micklesfield, Deputy Director of the South African Medical Research Council- Developmental Pathways for Health Research Unit (DPHRU), and postdoctoral researcher in the DPHRU, Dr Caylee Cook were part of the consortium’s policy core writing group.
Get M.O.V.I.N.G after lockdown lethargy
The policy briefs firstly address five major challenges that need to be tackled to minimise the risk of community transmission while exercising during the pandemic:
Ensuring social distancing (2m)
Wearing masks (non-medical, cloth masks)
Exercising in small groups (outdoors, with social distancing)
Exercising indoors (only with proper ventilation)
Avoiding the use of shared equipment or sanitising in between users.
These apply to children as well, and to children in school settings in particular.
Secondly, the briefs adopt a policy framework created by the World Cancer Research Fund, known as M.O.V.I.N.G, which recognises that these policy actions can take place within three different domains: Active societies, active environments, and active people.
M.O.V.I.N.G is:
making physical activity programmes a priority in communities and schools
offering training to promote physical activity for health champions in community-based programmes, health-care providers in primary health care settings and educators in schools
visualising and enacting “active design” principles for structures and surroundings
implementing urban and rural transport plans that support active societies
normalizing and increasing physical activity through mass public communication
give physical activity education, assessment & counselling
M.O.V.I.N.G is aligned with the WHO’S Global Action Plan for Physical Activity (GAPPA).
Thirdly, the policy briefs introduce a four-step policy recommendation for physical activity for the general public in the African region:
The development of a National Plan for physical activity for health and development, which would allow for input from multiple sectors and stakeholders resulting in co-benefits and shared responsibility.
Training a cadre of health professionals, educators, sports coaches and community members to promote physical activity for health, such as the Western Cape on Wellness (WoW!) lifestyle programme, which has trained more than 600 community health champions in under-served areas.
Ensuring safe and enjoyable opportunities for physical activity through urban planning, provision of parks or public spaces and low-cost programmes close to where people live. This is particularly critical in communities that lack safe and accessible facilities where they can be physically active.
Adopting a “whole of government” systems approach towards physical activity embedded in multiple sectors, devising flexible, agile and cost-effective solutions. Critical to this is recognising physical activity as a vital component both in preventive health care and a means to build social cohesion in communities.
“We are witnessing an exciting era where for the first time, healthcare providers and policy- makers are acknowledging the importance of physical activity for health and development in the African region. Regular physical activity saves lives, improves quality of life, physical and mental well-being, and boosts the immune system,” says Catherine Draper, Associate Professor in the DPHRU at Wits and a member of the consortium's expert advisory panel.
Professor Vicki Lambert from the University of Cape Town Research Centre for Health through Physical Activity, Lifestyle and Sport, and Associate Professor Rowena Naidoo, from the College of Health Sciences at the University of KwaZulu-Natal spearheaded the policy briefs, which are endorsed by the African Physical Activity Network (AFPAN) and supported by the Western Cape Government Department of Health, which hosted a Physical Activity for Health in Africa public webinar on 22 September.
Moribund Council on Higher Education is immobilising academic agility
- Adam Habib and Shirona Patel
Quality assurance entities are immobilising the system and hindering the ability of more students to access online education.
The coronavirus pandemic has forced universities to respond with agility in a complex environment; to develop academic content, courses and programmes that can be delivered online; to adapt pedagogies for remote and emergency teaching and learning; to upskill and retool academics and students so that they are empowered to participate in learning and teaching in an online mode; to adopt new technologies and learning management systems; to distribute devices nationally and provide access to data; and to explore multimodal educational approaches across various platforms.
In effect, the global emergency has condensed the long-term blended learning plans of many universities from years to months. Take Wits, for example – it took all of three weeks for the institution to pivot from being a contact university to taking the majority of academic programmes online.
However, while universities are responding nimbly, quality assurance entities like the Council on Higher Education cannot keep up, thus immobilising the system, and hindering the ability of more students to access online education.
These systemic challenges existed well before the arrival of Covid-19, though they have been compounded by the contagion. The Council on Higher Education has always had a long backlog due to its cumbersome administrative procedures and budgetary and staffing constraints.
About 18 months ago, at a national conference hosted by Universities South Africa, given the incapacity and incapability of the Council on Higher Education to timeously review, approve and accredit educational programmes, Wits proposed an alternative for the way in which academic programmes are accredited. Wits put forward that reputable universities that had the requisite skills, talent, qualifications, infrastructure, governance systems, resources and other necessary requirements be accredited at the institutional level with representatives from peer universities playing an oversight role.
For example, Wits has a rigorous internal system for the approval of a course or programme which starts at the level of the academic who develops the content. This proposal for the new academic offering is vetted by the school or department before being elevated to the faculty level, where it is again scrutinised. If it passes, it must be approved by the Academic Planning and Quality Office before serving at a subcommittee of Senate, being approved at Senate, and noted at Council.
We cannot limit access to higher education because of moribund regulatory agencies.
Don’t get us wrong – quality assurance is essential in order to ensure that we offer students the best education of a high global standard, and that is locally relevant. We cannot compromise on excellence and standards if we are to participate in the global knowledge economy, if we are to resolve local challenges, and if we are to move South Africa forward. But just how this accreditation and quality assurance takes place should be up for debate. We can no longer be held to ransom by a failing regulatory system that is effectively depriving students of higher education.
Universities are mandated to generate new knowledge, to develop high-level and professional skills for the workplace and society and to advance the public good. It is also our duty to provide access to quality higher education that has the power to transform the lives of students and their families. Now, more than ever, we have the ability to combine our academic expertise with the relevant learning management systems and new technologies to offer pedagogically sound online courses and programmes and, in so doing, create access to education for more people – a social justice imperative for the nation.
We have multiple opportunities to collaborate with local and international partners in the academic, public and private sectors on shifting to digital platforms to offer online courses and programmes, but these are being stymied by the Council on Higher Education, and its laborious and ineffective processes.
In its founding document in 2000, the Council on Higher Education stated its intention to move from accrediting every programme of every institution to accrediting institutions – this is standard practice in many countries. Centralised programme accreditation was seen as necessary at the turn of the century while the higher education system was largely being reshaped. In 2020, it is no longer necessary.
In 2017 the Council on Higher Education held public consultations about its intended plan to accredit institutions. Earlier this year, it sent out a draft of its Integrated Quality Assurance Framework (which includes institutional accreditation) for comment. But the Council on Higher Education indicated that the timescale for implementation of this plan is three years. This means that our institutions of higher learning are bound in red tape and that the state is paralysing our ability to be responsive and innovative for at least the next three years.
We cannot limit access to higher education because of moribund regulatory agencies.
We cannot allow universities to be held to ransom because the Council on Higher Education stymies the system.
We cannot remain silent and allow this malaise to continue at the expense of depriving students from accessing education.
It is imperative for the government to urgently release universities with strong internal quality assurance systems from the injunction to have every online programme accredited by the Council on Higher Education. The Council is unable to respond in real time to the needs of universities, especially under emergency conditions. Universities are ready to respond to the historical challenges of the moment but need to be freed to deliver to the nation.
We have been patient for too long and we are confident that many higher education leaders will join in the call for these bureaucratic processes to be amended and for universities to be empowered to do what they do best.
Professor Adam Habib is vice-chancellor and principal of Wits University and Shirona Patel is coordinator of the Wits Advancement Division. This article first appeared in Daily Maverick.
Covid-19 Update 53: Infection summary
- Wits University
Update on the latest Covid-19 testing and infection of staff and students.
Two staff members and four students reported testing positive for COVID-19 during the past week. These include staff members who are working from home. This is out of a population comprising of approximately 5 500 permanent staff and 37 500 students. Affected staff members and students are self-isolating in line with governmental directives and University protocols.
Numbewr of infections
23 Oct - 29 Oct 2020
22 Jun – 29 Oct 2020
Staff
2
111
Students
4
211
The data provided in the table above is based on the number of infections reported to the Occupational Health and Safety Office and the Campus Health and Wellness Centre. Read more about Wits’ COVID-19 policies, rules, protocols, resources and updates at www.wits.ac.za/covid19.
Real-time data is critical for detecting outbreaks
- Cheryl Cohen, Sibongile Walaza and Mvuyo Makhasi
South Africa is testing digital technology to detect outbreaks of respiratory diseases.
Global mobility has increased and the world has become more connected. But this comes with a greater risk of the spread of respiratory diseases, particularly pneumonia, which is a leading cause of death in children under the age of five and the elderly. Real-time and more accurate data about respiratory diseases are critical for public health response – especially during an outbreak.
Pneumonia is a lower respiratory tract infection. It’s caused by very small organisms that cause the air sacs in the lungs to fill up with fluid. This makes breathing difficult and may lead to death. Data from respiratory disease surveillance programmes help public health officials to detect potential clusters that may lead to widespread outbreaks and implement strategies to minimise the impact.
Information collected in clinics and hospitals doesn’t provide the full picture of an illness. This information depends on people actually going to health facilities, which doesn’t always happen. Some people may not be severely ill, or may not be able to get to the health facility. And there may not be adequate laboratory capacity to run tests.
Relying on facilities for information about illnesses makes it difficult to detect an outbreak or seasonal increase as it happens – and hard to estimate the total case numbers. There can be a delay and under-reporting, which makes the public health response less effective. The sooner a cluster of cases is detected, the better it can be managed.
These days there are other ways to collect information about illnesses, using technology. They fall under the description of digital participatory surveillance. These are platforms that allow people to routinely report their own symptoms via the internet, on a mobile application or through social media surveys. They can also record questions about health-seeking behaviour. Health authorities can then analyse the digitally collected data, obtain a bigger picture of how prevalent a disease is in a population, and see trends that allow the health system to prepare and manage better.
The National Institute for Communicable Diseases in South Africa is planning a pilot phase of a digital participatory surveillance platform. The aim is to assess the feasibility and inform its structure, before incorporating it into the existing facility-based surveillance programmes. In particular, this pilot phase will be used to survey respiratory diseases such as influenza and potentially COVID-19.
Influenza is a vaccine preventable disease and one of the causes of pneumonia. It causes an estimated 11,000 deaths every year in South Africa. With regard to COVID-19, which can also cause pneumonia, the pilot phase may potentially assist in detecting a big increase in cases at an early stage.
The success of a digital participatory surveillance programme depends on the consistent participation of the population.
South Africa already has another technological tool designed to combat the pandemic: the COVID-19 Alert app. But that is intended for contact tracing, by helping the user ascertain whether they have been in close proximity to a confirmed COVID-19 case. It’s different from digital participatory surveillance apps that are intended for long-term surveillance of respiratory diseases beyond COVID-19, and do not serve contact tracing purposes.
Digital surveillance
Digital participatory surveillance is relatively low-cost and easily scaleable to any disease of public health significance. Users report on a weekly basis whether they have experienced symptoms related to respiratory illness or not. This allows for real-time estimation of cases without relying on access to medical care or testing capacity. This data can also be used to forecast how outbreaks might spread in a community.
To date, digital participatory surveillance has not been widely used on the African continent, despite its potential value. But it’s been used in other parts of the world.
The first platform of this kind was launched in Europe in the 2003/2004 influenza season and they are now used in several countries, where they have been able to detect flu outbreaks earlier. The USA, Australia and Mexico have their own digital participatory surveillance programmes. Today, 11 European countries have established a continent-based digital participatory surveillance network called InfluenzaNet. This allows for a comparison of trends within and between countries in Europe.
Countries in Europe, and the US and Australia have increased and sustained participation on these platforms through media campaigns and public health messaging. The National Institute for Communicable Diseases is employing similar strategies through public relations and media in South Africa.
South Africa’s digital participatory surveillance will face some important challenges, though.
Firstly, information and communications technology is limited. Some parts of the country may not have internet connectivity.
Secondly, the digital divide within a population means segments of the demographic may not be fully represented, because not everyone has access to smartphones or internet connectivity.
There may be some concerns and scepticism around social media and mobile apps with regard to data confidentiality and privacy. These are longstanding challenges that both government and various industries need to address.
Moving forward
As the digital world evolves, there is an opportunity to use technology to solve critical problems in public health.
Digital participatory surveillance allows the community to share in the responsibility of disease surveillance and contribute to the control and prevention of respiratory disease outbreaks.
Update on the latest Covid-19 testing and infection of staff and students.
Three staff members and three students reported testing positive for COVID-19 during the past week. This is out of a population comprising of approximately 5 500 permanent staff and 37 500 students. Affected staff members and students are self-isolating in line with governmental directives and University protocols.
Number of infections
30 Oct – 5 Nov 2020
22 Jun – 5 Nov 2020
Staff
3
114
Students
3
214
The data provided in the table above is based on the number of infections reported to the Occupational Health and Safety Office and the Campus Health and Wellness Centre. Read more about Wits’ COVID-19 policies, rules, protocols, resources and updates at www.wits.ac.za/covid19.
Covid-19 Update 55: All services must be operational
- VCO
Following President Cyril Ramaphosa's address.
Following the announcement of lockdown level 1 regulations, it was agreed that all University services would be operational from 5 October 2020. We would like to express our appreciation to all staff members who have continued to serve the University during this difficult time and who have reported for duty when requested to do so. Thank you.
It has, however, been brought to our attention that there have been service lapses in some areas, and that some staff members have not been reporting for duty or fulfilling their duties.
We would therefore like to reiterate the following:
Managers of all service units must ensure that their units function effectively, which means that professional and administrative staff from every unit are expected to report to work at all times, either simultaneously or on a rotational basis. Line managers must take overall responsibility for this decision. Staff members must report to work when requested to do so by their line managers. There should be no reduction in the quality, scope or volume of work at any time.
The only exceptions are as follows:
Staff members who have co-morbidities (as determined by a medical practitioner or the Wits-appointed healthcare practitioner based at the WDGMC) and as described in the HR Practice Note on this matter, should for the time being, with the approval of their line manager, work productively from home and undertake work that is assigned to them.
Staff members over the age of 60, who may be at risk, should be enabled to work from home as per national regulations and the University’s practice note around this matter. Employees over the age of 60 who do not have co-morbidities, and who are healthy, may return to the workplace at their own risk.
In cases where the environment does not enable social distancing and the observance of all occupational health and safety protocols, executives and line managers must put in place working arrangements that comply with these protocols, as recommended by the assigned occupational health and safety officer.
All managers must submit revised risk assessment and mitigation plans, which must be agreed upon with the assigned Occupational Health and Safety Officer before staff return to the workplace. In open plan areas and congested spaces, staff may be required to return on a rotational basis, as determined by line managers, and with the approval of Occupational Health and Safety Officers.
Should you have any further queries, please direct these to your respective line manager and if required, escalate issues to your respective Head of School, Divisional Head, or SET member.
Wits University statement on Oxford Covid-19 vaccine results in UK and Brazil populations
- Wits University
Scientists at Wits University are encouraged by results announced today by colleagues at the University of Oxford in collaboration with AstraZeneca.
Scientists at Wits University, which leads the South African trial of the ChAdOx1 Covid-19 vaccine developed by the University of Oxford, commented on the findings announced by Oxford/AstraZeneca following a pooled interim analysis of the Phase 3 arms of the UK and Brazil studies of this vaccine.
The findings indicate that the vaccine is 70.4% effective in protecting against Covid-19 in UK and Brazil when combining data from two dosing regimens.
In the two different dose regimens, vaccine efficacy was 90% in one and 62% in the other. The higher efficacy regime used a halved first dose and standard second dose.
Early indications are that the vaccine could reduce virus transmission from an observed reduction in asymptomatic infections.
Crucially, the vaccine can be easily administered in existing healthcare systems, stored at ‘fridge temperature’ (2-8 degrees Celcius), and distributed using existing logistics.
Large scale manufacturing is ongoing in over 10 countries to support equitable global access.
Although these interim results do not include analysis of South African participants in the global trial, they suggest similarly encouraging results can be expected here.
Professor Shabir Madhi, Executive Director of the Vaccines and Infectious Diseases Analytics (VIDA) Research Unit at Wits, which leads the trials in SA, said: “The results from this study add further hope that accessing vaccines to fight the Covid-19 pandemic are fast becoming a reality.The results from this study are intriguing, in that a dose-sparing regimen may inadvertently end up being more protective. This has implications not only for the cost of the vaccine, but also how many more people could possibly be vaccinated in the near future when vaccine supply is likely to be constrained.
Also, the ability to scale up production of this vaccine, and it only needing to be stored at 2-8oC, would greatly assist in the deployment of the vaccine in low and middle income countries. The cost of this vaccine is also anticipated to be much cheaper than other Covid-19 vaccines that have recently been shown to be efficacious.”
The trial in South Africa has enrolled 2,100 participants and analysis of the trial in South Africa is expected after an adequate number of Covid-19 cases have been identified.
Madhi emphasised the importance of testing the vaccine in diverse populations, such as South Africa: “The results of the study from South Africa remain of global interest, and to inform recommendations on Covid-19 vaccine in Africa, as the Covid-19 experience in South Africa has been very different to the UK. As for many other vaccines, genetic factors and local conditions could also affect the performance of the vaccine in different populations.”
The results of the pooled analysis from UK and Brazil creates optimism that we will also show protection against COVID-19 in the South African study, where participants are still being followed-up.
Professor Andrew Pollard, Director of the Oxford Vaccine Group and Chief Investigator of the Oxford Vaccine Trial, said: “These findings show that we have an effective vaccine that will save many lives. Excitingly, we’ve found that one of our dosing regimens may be around 90% effective and if this dosing regime is used, more people could be vaccinated with planned vaccine supply. Today’s announcement is only possible thanks to the many volunteers in our trial, and the hard working and talented team of researchers based around the world.”
Update on the latest Covid-19 testing and infection of staff and students.
No students or staff members reported testing positive for COVID-19 during the past week. But we should not be complacent. Watch and share this animationon the precautions that must be taken in order to keep safe.
Staff and Student COVID-19 Infection Summary
Number of infections
6 – 12 Nov 2020
22 Jun – 12 Nov 2020
Staff
0
114
Students
0
214
The data provided in the table above is based on the number of infections reported to the Occupational Health and Safety Office and the Campus Health and Wellness Centre. Read more about Wits’ COVID-19 policies, rules, protocols, resources and updates at www.wits.ac.za/covid19.
Covid-19 Update 57: Infection summary
- VCO
Update on the latest Covid-19 testing and infection of staff and students.
We appeal to all members of the University community to please maintain social distancing, wear masks, sanitise regularly, and obey all Wits’ COVID-19 policies and protocols.
Staff and Student COVID-19 Infection Summary
Five students reported testing positive for COVID-19 during the past week and are self-isolating in line with governmental directives and University protocols.
Number of infections
19 – 26 Nov 2020
22 Jun – 26 Nov 2020
Staff
0
114
Students
5
219
The data provided in the table above is based on the number of infections reported to the Occupational Health and Safety Office and the Campus Health and Wellness Centre. Read more about Wits’ COVID-19 policies, rules, protocols, resources and updates at www.wits.ac.za/covid19.
Fake news and misinformation kill
- Scientists Collective
How can you trust what you are told about Covid-19?
In the past 10 months, as Covid-19 has swept the globe, the internet and media have also been ablaze with stories, reports and ever-changing guidelines on how to stay safe in a world that appears to be out of control. But what should we believe and what can we trust? As importantly, how do we spot ‘fake news’ and misinformation? In this special advisory, a collective of over 20 of SA’s leading doctors and scientists offer their advice.
Living in a digital world means that we have access to the latest information on just about any subject. While this can be powerful and empowering, it can also be harmful. Access to information online is empowering because we can stay abreast of the latest knowledge about Covid-19 and can share useful data that, in the interests of public health, can help people change their behaviour and stay safe.
However, it’s increasingly difficult to know how to sift out the truth from the masses of lies, misinformation and myths that are also all over the internet and social media, in an environment where the phrase “fake news” is applied to anything someone does not agree with, and truth is a political and ideological tool.
As scientists and clinicians, we are in a challenging position with Covid-19. We are discovering how to approach this novel virus in real time, just as it creates chaos and devastates communities all over the world. We still don’t know enough about why the virus manifests so severely in some people and not others; whether some people can be infected more than once, and what the lasting impacts of Covid-19 are on the body.
Scientific and medical advice around Covid-19 has changed since we first began our steep learning curve in early 2020. To begin with, public health advice focused on physical distancing and hand hygiene. As the peer-reviewed, evidence-based, scientifically sound research emerged, we also began recommending that people wear masks, with South Africa one of the first countries to recommend universal mask-wearing outside of Asia.
The practice was already common in many east Asian countries, so was more easily adopted there.
Evidence is clear that the Covid bundle works
This bundle is a collection of practices such as increasing ventilation by opening windows, physical distancing, wearing a mask in crowded spaces and sanitising your hands, which reduces the number of viral particles you might inhale.
Debates and disagreements are usual in the world of scientific and medical research. We welcome debate among colleagues, and we have rigorous processes like peer review, ethics committees, regulatory oversight, safety boards and double-blind research methods that help to inform our discoveries and ensure that any biases are brought to light.
These processes are not always perfect – the sciences are not immune to fraudsters, media-hungry charlatans, and reckless outsized egos – but agreement on what we know tends to be a self-correcting, iterative process. And, in general, debate and dissent are not suppressed or controlled.
Over the last few months however, while frontline health workers have been risking their lives (and many healthcare workers have died in South Africa, as have some of their family members) to treat people ill with Covid-19, we have been dismayed at the spread of accusations that we “know nothing about this virus”.
This is simply untrue; a huge amount of new knowledge has emerged since January 2020, and this has built on substantial prior knowledge about this class of virus, as well as the novel coronaviruses responsible forSevere Acute Respiratory Syndrome(SARS) andMiddle East Respiratory Syndrome(MERS). This improved knowledge has had positive effects: For example, the survival rate of people with Covid-19 has improved.
We are even more dismayed at the extraordinary claims that some researchers have falsified evidence or misled public health officials around the best ways to handle this pandemic.The scientists and clinicians in this advisory group live in a world where we exchange data, new research, hypotheses, disagreement, controversy and wild ideas every day.
In fact, research thrives on these debates and disagreements. We have active discussion groups on WhatsApp, where we discuss and critique everything from the government’s approach to lockdown to new understandings of immunology. We represent a wide array of disciplines, which stimulates interesting and challenging discussions, and our research and other collaborations means we are wired into scientific debates from every corner of the globe.
We do not suppress evidence-based dissent. We have seen this during the Covid-19 pandemic already – some substandard or even fraudulent “research results” were published but soon called out and corrected or withdrawn.
There is a strong incentive for scientists to not remain quiet when they encounter poor research. Apart from scientific ethics, one can gain a lot (recognition, research grants, promotion) from publishing valid evidence to the contrary.
When scientific consensus supports a measure such as mask wearing, this is not based on suppressing dissent, but simply expresses the fact that the best available scientific data indicates that wearing masks in public spaces, especially when indoors and when gathering in groups, helps to slow transmission of Covid-19 and protects people who may be particularly vulnerable to infection.
This is not controversial; it is established science and it is best practice.
It is not up for debate.
It is not only pointless to set up debates about this, but it is also an actively harmful fake controversy. We advocate wearing masks, not because we want to make life difficult for the public, but because we are doing our best to save lives and ensure that the virus is contained in the absence of biomedical preventive measures, including prophylaxis and vaccines.
Truth and fiction
There is a famous adage that journalism students are taught: if you have one person telling you it’s raining and one person telling you it’s sunny, you do not just quote them both. Instead, you look out the window and find out for yourself which person is telling the truth.
In this digital age, there are many people claiming it is raining outside when all the scientific and medical evidence tells us it’s sunny. Ordinary people don’t know who to believe, especially when some of those promoting the lies are people with resources and power and hidden agendas. Rumours and misinformation spread quickly on platforms like Facebook or in WhatsApp message groups.
We, as scientific and medical professionals, have a duty to ensure that we communicate scientific fact properly and make this information as widely accessible as possible for all to see. We are bound by professional ethics to make sure that anything we communicate can be defended by evidence, and we try to be transparent about this.
When we don’t know something, we are honour-bound to admit it. And when we do know, we have a responsibility to ensure that we disseminate these findings far and wide in a way that is easily digestible to a wide array of audiences.
This is the essence of public health; to use our knowledge to communicate to the populace and to develop strategies and behaviours to keep people safe and well.
We also have a duty to speak truth to power
Where a government makes poor choices or lapses into secrecy and does not communicate the reasons behind decisions, professionals must call these behaviours out. Where senior media personalities or advocacy groups put us all in danger with misinformation, they must be held to account.
Control of this virus, in some ways more than ever before, demands a collective sense of responsible community – this means we must be critical of those hiding behind cries of “groupthink”, conspiracy theories, or reckless and inexpert interpretation of data.
Scientists who collude with governments to legitimise unscientific approaches have been a feature of many country responses across the globe and need to be challenged.
Tips on how to counter misinformation
We urge the South African public to take this mandate to end “fake news” as seriously as we do. To this end, we encourage every single person to become critically aware of misinformation and fake news, and we recommend the following tips to help:
Check the source.Be sceptical of any information that does not come from a credible scientific source. Any scientific research worth its salt will contain references to research conducted by universities and reputable research bodies. If you aren’t sure, check if the source is listed in one of these databaseshereorhere.
Ask yourself who is publishing this information and what their agenda might be.Be very cautious of anything that promises “ground-breaking” new developments unless it is being widely shared by well-established and reputable channels. By this, we mean journalists working for established media organisations where they will do fact-checking and have good editors in place. Or journals that have been in publication for a long time, and that provide peer-reviewed scientific articles. There are many websites out there that look credible and have lots of information on them, and that even promise this information is evidence-based, but it only takes a little investigation to show that these are not legitimate and not backed up by honest scientific endeavour.
Search engines are your friend.If you have any doubts, enter the name of the person you’re seeing spreading this information or look up the article online. See what comes up, follow the links to the names of those involved and test their veracity. Real medical experts are easy to find online because they participate in publicly available research; they attend conferences with their peers, and they work for credible scientific organisations like universities or public hospitals. Try googling the names of the people who wrote this article.
Use the services of established fact-checkers.In South Africa, we have an excellent organisation called Africa Check – their only purpose is to very carefully and thoroughly investigate information in the media and in the public domain to assess whether or not it’s true. They’re doing a great job on Covid-19 too. Find themhere. TheWorld Health Organisationoffers a WhatsApp service (+41798931892) for updates on fake news.
Be alert to emotion.If you receive a video that makes you feel angry, scared or anxious, be very cautious. Evidence-based science might have significant implications but, in most instances, it won’t seek to make you fearful. Be careful to avoid those pundits who whip up emotion in order to make people afraid to follow their doctor’s advice.
Just because they wear a white coat, have certificates on a wall or have graphs or statistics doesn’t mean they are a doctor or a scientist. Just because they speak with calm authority, have lots of papers on their desk and books on shelves behind them, does not mean they are an expert. There are too many people out there claiming to be scientists and some of them are very sophisticated in using props to create an image of scientific integrity.
Use your critical mind to ask yourself the following questions: who is this person? Are they properly trained and accredited? Are they trying to sell a “quack” remedy that makes them a lot of money? Is their message supported by other scientists or professionals that are trustworthy?
A single person spouting a lot of information about Covid-19 that’s not backed up by lots of other credible sources should make your fake news antennae quiver.
If a friend or relative, co-worker or community group sends you something about Covid-19 (or any other health condition), ask them where they got it.If they can’t or won’t give you a recognisable source, then it might be fake news. And “my brother’s friend’s cousin” is not a reputable source.
Similarly, if you’ve found something interesting online, consider checking its validity before sharing it uncritically with others in your circle.Don’t become an unwitting accomplice to the distribution of unreliable and unhelpful fake news, but rather take a conscious stand in support of evidence-based, reliable public health information. Each of us has a responsibility to take Covid-19 seriously, and it’s only through every citizen actively playing his or her part that we will overcome this pandemic.
When considering whether you might be supporting a conspiracy theory, ask yourself how many people would have to be lying or covering up for this claim to be true, and how plausible it really is that this is happening.Even if you think it is plausible thatonegovernment could create a fake pandemic for political purposes, is it really plausible that governmentsall round the world, including democratic and not democratic, libertarian capitalist oriented and social welfare oriented, Western and non-Western, high and low income, could all be promoting a hoax pandemic? Is it really plausible thatmostscientists in Europe, Asia, Africa and elsewhere are sheeple, subject to group-think, while one person or a small number of people have seen the truth?
Some of the more common myths about Covid-19
“Covid-19 is a scam and there is no virus.”
There is no evidence to support this claim.
The information communicated by the World Health Organisation, National Institute for Communicable Diseases, and the national department of health, as well as from other stakeholders, is reliable and credible.
The new coronavirus (SARS-CoV-2) is totally real.
At the time of writing, there are just under 50 million people globally who have been confirmed to have been infected with SARS-CoV-2. More than 1.2 million people have died of Covid-19.
While comorbidities may present an additional risk to some affected persons, this does not negate the existence or direct impact that Covid-19 has had on the health and lifespan of millions around the world. Some of us are clinicians who have first-hand experience of this virus in the last few months.
We promise it’s real and can be severe and scary – not because we saw it on YouTube, but because we have seen it in our hospitals and clinics, among our colleagues, friends and families.
“Doctors write Covid as cause of death if someone has tested positive, no matter what they die of, whether it is cancer or a car accident, with Covid massively over-reported.”
Absolutely not.
South Africa has one of the world’s best mechanisms for reporting deaths.
There are currently delays (related to lockdown’s impact on paperwork), and cause of death without an autopsy is dependent on the judgement of the health worker filling in the form.
However, in our experience, the cause of death is usually reported with the most obvious cause. In fact, if someone dies due to cancer or in a car accident, where Covid precipitated that death, it is likely Covid is not reported unless very clearly diagnosed, and hence is likely to be under-reported.
Therefore, looking at the numbers of “excess mortality’’ is really important to get a sense of this under-reporting. Check out the MRC’s weekly reportshere.
“The World Health Organisation was created by people like the Rockefeller or Gates families to control global health policy.”
The funding of the WHO is completely transparent, although it is under-resourced for its vital public health mandate. Member states contribute to the funding of the WHO. Private charities, such as Rotary International and the Bill and Melinda Gates Foundation, are also major donors.
Some countries – like the United States – have refused to pay their UN dues, which undermines the work of the WHO.
The WHO employs thousands of well-trained, experienced staff from all over the world. Many of the people on this advisory are part of WHO processes, as volunteers. It makes recommendations based on scientific evidence and has been known to revise its recommendations when new evidence comes to light. There is absolutely no evidence we have seen of any conspiracy in the way the WHO operates.
“The virus (SARS-CoV-2) which causes Covid-19 hasn’t actually been isolated in South Africa.”
Not true. A collaborative effort between the University of the Western Cape and Stellenbosch University obtained the first-known laboratory isolate of SARS-CoV-2 in South Africa on 1 April 2020 (see reportshereandhere).
“The SARS-CoV-2 virus was created in a Chinese laboratory (or by the CIA or the Russians).”
No. We have no evidence of this. We do, however, have evidence that this virus came through infection in animals, a process we have seen before with coronaviruses and others. The facts show us that the virus “jumped” from an animal species into the human population. This virus was not deliberately created in any laboratory. See explanationshereandhere.
“Covid is no more dangerous than the flu and it is crazy to worry about a disease that is more than 99% survivable.”
How likely you are to die from it is evolving, with a complex interaction of factors including your own health, the health care you have access to and possibly how high the infectious dose was. Some people claim Covid is less dangerous than the common flu and claims of a 99.9 percent survivability rate are promoted by those who think it is grossly exaggerated.
TheCDC currently estimatesthat Covid in the US has a 0.65% infection fatality rate (deaths per person infected); that is six times the flu infection fatality rate of 0.1%. And 0.65% of the South African population is 390,000 people, nearly eight times ourcurrent excess deathsin the past months and nearly 20 times our official Covid deaths.
If we took the worst case scenario and assumed everyone in South Africa had COVID, 0.65% IFR would translate into 390 000peopledeaths, nearly 8 times our current excess deaths in the past months and nearly 20 times our official covid deaths . But we know not our whole population is infected and if we take our current cases, using the CDC IFR this would amount to 50 630 deaths. This is a lot more deaths than we would expect from flu.
Also, comparing your frail granny to a healthy 14-year-old is silly. Your granny’s chance of getting severely ill and dying is far, far higher. If a 14-year-old falls down the stairs, she is likely to be okay, bar a few bruises. Granny is way more likely to get hurt or die. Aggregating their risk does not help anyone.
And this is only considering deaths; we are learning more every day about long-term effects of Covid (explained in our Advisory here) which can be very serious and debilitating, so of course the fatality rate is not the only concern.
“Mask-wearing is controversial.”
Aspects of mask-wearing (for example, the precise degree of protection they provide from getting the virus or stopping transmission) may be a debate, or which kind of mask is the best, but no one reputable now debates whether masks should be a major part of our response (for more advice and science on masks, seehere,here,here).
“The vaccines are just a money-making scheme, and are a way to track you/collude with 5G networks.”
This is one of the most pernicious and dangerous falsehoods.
You can trust (seehere,hereandhere) that there are huge checks and balances in place before a vaccine gets on to the market, including from sceptical regulators and scientists reviewing the data on both efficacy and safety. If a vaccine gets offered to you, it means it has been subjected to meticulous scrutiny, and if you read the package insert, you should get a good sense of how effective and safe it is.
Fears that it is linked to tracking mechanisms and weird associations with 5G are false. Worry about your cellphone, your search history, your bank password, and your FaceBook public profile – not about a Gates Foundation-linked microchip in a vaccine.
“Fogging/deep-cleansing/mouthwash (insert your favourite intervention here) will save you.”
These myths crop up everywhere, often promoted by commercial interests trying to make quick money from your fear, or by those who inexplicably enjoy drumming up controversy. The Scientists Collective offers practical guidancehere.
We applaud when governments, news outlets and social media fact-check and at times penalise people who spread misinformation, or at least flag that the media being posted is dodgy and that their fact-checking suggests it should be viewed with scepticism.
This is not “gagging’’ or groupthink or censorship – they can tell their stories on endless blogs and social platforms – it is responsible information sharing.
When you have an uncle who thinks UFOs are controlling the world, you may roll your eyes at his Facebook posts but you don’t help him to share his weird theories.
In this time of coronavirus uncertainty, myths and misinformation can be especially disempowering. You can beat that by playing detective – follow the tips we have suggested if you see something that makes you feel uneasy; if it sounds too good to be true, or if it seems to be whipping up emotions in a destructive manner.
Then, if you want to do something about it, report it toReal411.org, an excellent local online resource that can sift truth from fiction. That way, not only will you be helping to combat disinformation, but you will also be helping ensure others are less likely to fall for it. Every little bit helps.
And, in the meantime, please do wear your mask, keep a physical distance and practise regular hand hygiene.
There are, of course, a range of useful sites that we can recommend people visit to check on myths, including:
This article first appeared in Daily Maverick/Maverick Citizen.
We thank William Bird of the Media Monitoring Project and editor Nicola Spurr for their guidance with the writing of this advisory. The Scientists Collective who collaborated on this piece are:
Dr Nomathemba Chandiwana, Dr Simiso Sokhela, Dr Samanta Lalla-Edwards, Dr Bronwyn Bosch, Nkuli Mashabane, Dr Roxanne Govender, Celicia Serenata, Professor Francois Venter, all at Ezintsha, University of the Witwatersrand.
Andy Gray, Division of Pharmacology, Discipline of Pharmaceutical Sciences, University of KwaZulu-Natal.
Dr Ndiviwe Mphothulo, primary care specialist
Professor Shabir Madhi, Respiratory and Meningeal Pathogens Research Unit, University of the Witwatersrand.
Professor Lucy Allais, University of the Witwatersrand.
Professor Wolfgang Preiser, University of Stellenbosch.
Dr Elijah Nkosi, private practice.
Professor Shaheen Mehtar, University of Stellenbosch.
Dr Jeremy Nel, University of the Witwatersrand.
Professor Yunus Moosa, University of KwaZulu-Natal.
Professor Wendy Stevens, University of the Witwatersrand.
Professor Lucille Blumberg, University of Stellenbosch.
Professor Glenda Gray, University of the Witwatersrand and Medical Research Council.
Dr Jantjie Taljaard, Tygerberg Hospital and Stellenbosch University.
Dr Francesca Conradie, University of the Witwatersrand.
Professor Marc Mendelson, University of Cape Town.
Professor Morgan Chetty, Visiting Prof Health Sciences, Durban University of Technology.
Dr Aslam Dasoo, Progressive Health Forum.
Professor Eric Decloedt, Stellenbosch University.
Professor Alex Van Den Heever, University of the Witwatersrand
Professor James McIntyre, Anova.
Adrienne Wulfsohn, Emergency Medicine Physician, UKZN
Dr Regina Osih, infectious disease specialist.
Dr Angelique Coetzee, South African Medical Association
Covid-19 Update 58: Advice from Scientists Collective
- VCO
Update on the latest Covid-19 testing and infection of staff and students.
Two staff members and five students reported testing positive for COVID-19 during the past week out of a population of approximately 37 500 students and 5 500 staff members. They are self-isolating in line with national directives and are observing all University protocols.
Number of infections
27 Nov – 03 Dec 2020
22 Jun – 03 Dec
Staff
2
116
Students
5
224
The data provided in the table above is based on the number of infections reported to the Occupational Health and Safety Office and the Campus Health and Wellness Centre. Read more about Wits’ COVID-19 policies, rules, protocols, resources and updates at www.wits.ac.za/covid19.
We appeal to all members of the University community to please maintain social distancing, wear masks, sanitise regularly, and obey all Wits’ COVID-19 policies and protocols. [WATCH] this video on how you can prevent the spread of COVID-19 and take heed of the advice offered by The Scientists Collective (many of whom are Witsies).
Covid-19 Update 59: Infection Summary
- VCO
Update on the latest Covid-19 testing and infection of staff and students.
Two staff members and seven students reported testing positive for COVID-19 during the past week. They are self-isolating in line with directives from government and University protocols.
Number of infections
4 – 10 Dec 2020
22 Jun – 10 Dec
Staff
2
118
Students
7
231
The data provided in the table above is based on the number of infections reported to the Occupational Health and Safety Office and the Campus Health and Wellness Centre. Read more about Wits’ COVID-19 policies, rules, protocols, resources and updates at www.wits.ac.za/covid19.
Covid-19 Update 60: Infection Summary
- VCO
Update on the latest Covid-19 testing and infection of staff and students.
Staff and Student COVID-19 Infection Summary
One staff member and four students reported testing positive for COVID-19 during the past week. The affected staff member and students are self-isolating in line with governmental directives and University protocols.
Number of infections
11 Dec – 17 Dec 2020
22 Jun – 17 Dec
Staff
1
119
Students
4
235
The data provided in the table above is based on the number of infections reported to the Occupational Health and Safety Office and the Campus Health and Wellness Centre. Read more about Wits’ COVID-19 policies, rules, protocols, resources and updates at www.wits.ac.za/covid19
This is the last COVID-19 update for this year. We wish you and your loved ones well over the holiday season. Remember to sanitise, wear your masks, and maintain a safe physical distance of at least 1.5 metres from others.
Keep safe.
AI helps to identify new Covid-19 hotspots in Gauteng
- Wits University
Gauteng Government, IBM Research and Wits University are fighting the pandemic with artificial intelligence.
Accurate modelling is one of the tools being used to fight the Covid-19 pandemic globally. It is essential for policy makers, experts and the population to get access to reliable information on the evolution and severity of the pandemic based on relevant and robust advanced analytics and modelling.
In the last two weeks there has been a large increase in the daily number of cases throughout South Africa. These increases show clear signs of being the beginning of the second surge experienced in many countries around the world. In order to manage the rapidly growing numbers in Gauteng, it is vital to be able to target areas where the spread of the virus is growing fast and can be categorised as a hotspot. The determination and modelling of hotspots are complex tasks that require the use of techniques derived from artificial intelligence (AI).
In order to make this exercise possible, back in August the Gauteng Government launched a dashboard with IBM Research, Wits University and other stakeholders to visualise the data and modelling for the province. The partners have now updated the dashboard to visualise hotspots in the Gauteng Province. The tool provides information about the location, the number of cases, the area, affected administrative regions and the level of severity for each hotspot.
In order to fully characterise the danger that may be associated with a hotspot it is essential to assign to it an index in addition to its location and other characteristics. This index is referred to as the index of severity. This index is intended to enable policy makers and authorities on the ground to determine the best course of action to most efficiently curb the hotspots.
The Wits Institute for Collider Particle Physics (ICPP) applies analytical methods and tools used at the CERN (European Organization for Nuclear Research), to develop indexes that help policy makers and other stakeholders track the evolution of the pandemic. These indexes are developed on the basis of extensive research and observations of how the pandemic is evolving in South Africa and internationally.
“One of the indexes that our team developed is the risk index for the second wave. This index is a tool for the early detection of the second wave and it can be visualised and tracked for the different administrative regions of South Africa. The development of the severity index for hotspots is a continuation of earlier studies,” says Thuso Mathaha and Kgomotso Monnakgotla, researchers at the ICPP.
“We are observing a sharp increase in the number of infections across the province. We identified hotspots and the active ones are mapped in our dashboard that is available for free to the public, researchers and policy makers. We encourage public use of this information as it is relevant for following the movement of the pandemic and to be alerted to emerging hotspots. We urge the public to continue to adhere to the regulations so that we can reduce infections and save lives,” says Mduduzi Mbada, Head of Policy at the Gauteng Office of the Premier.
“This dashboard contributes to the Covid-19 pandemic response by making data on the spatial location of active hotspots in Gauteng readily available to the public, researchers and policy makers. It is anticipated being able to visualize the specific locations of hotspots will influence people's perceptions of Covid-19 risk and potentially shape personal protective behaviour. The dashboard also provides data useful for the Advisory Committee to guide policy makers on where to target interventions for mitigating the pandemic. Further, the dashboard provides policy makers granular data useful for planning and monitoring the pandemic response at ward level,” says Dr Mary Kawonga, Public health Medicine Consultant at Wits University and Chair of the Gauteng Premier Covid-19 Advisory Committee.
“The problem is how to identify areas of high activity of coronavirus. Given the locations of Covid-19 patients provided by the Health Department, we must group the cases into severely infectious zones, or clusters. We are able to find these clusters optimally within the Gauteng region, by using technologies in artificial intelligence. With this information, we can compare the growth of a cluster to epidemiological models derived for infectious disease spread, thereby giving accurate predictions for the evolution of any cluster. This means we can now describe the severity of coronavirus cases for various locations within the province. The success of this integration of AI algorithms with standard epidemiological models is a powerful example of how 4IR research can be used to aid South Africa,” says Roy Gusinow, a researcher at the ICPP.
“Hotspots areas are defined thorough a thorough analysis of the first wave using AI together with advanced analytics we are able to examine each cluster of cases geographically and through epidemiological modelling. Once the dynamics of normal clusters and hot-spot clusters is clearly understood we are able to extract potentially vulnerable and volatile clusters as hot-spots and/or developing hot-spots and visualise them through IBM’s specially developed platform. Through the gpcoronavirus platform, stakeholders in all industries are able to identify hot-spots and enforce appropriate measures, distribute necessary resources and/or provide guidance to the area’s population to control the spread of Covid-19,” says Benjamin Lieberman, a researcher at the ICPP.
This fruitful collaboration between the Gauteng Department of Health, and other stakeholders in Gauteng, IBM and Wits University involves many individuals from diverse backgrounds. This includes policy makers, practitioners and researchers from a wide range of disciplines.
“The new hotspot visualization in the dashboard includes the severity of infectiousness in an area and is grounded on epidemiological models that capture the dynamics of the spread of the disease,” says Dr Sibusisiwe Makhanya, a research scientist at IBM Research – Africa.
“Artificial intelligence is a versatile set of tools in modern analytics that allows us to tackle modelling of complex system through learning from experience. AI has proven to be very effective in the inter-disciplinary ecosystem established to tackle a this major crisis,” says Professor Bruce Mellado, Director of the Wits ICPP, who is also a senior scientist at iThemba LABS and a member of the Gauteng Premier Covid-19 Advisory Committee.
The dashboard is available via the IBM Cloud using the latest Chrome or Firefox web-browsers at https://gpcoronavirus.co.za.
Map of the active Hot Spots in the Gauteng Province
The Wits ICPP is grateful for the continued support by the Department of Science and Innovation and the National Research Foundation. The ICPP is also grateful for grant awards from the IEEE, the International Development Research Centre (IDRC) and the Swedish International Development Cooperation Agency (SIDA).
All you should know about where we are with Covid-19 vaccines
- Scientists Collective
What are the urgent steps that South Africans need to take to prepare for a timeous life-saving roll out of vaccines?
Some of the members of the Scientists Collective are acknowledged as world leaders in the vaccine field, and are in a position to consider and provide answers to the difficult questions about meeting one of the greatest challenges South Africa has ever faced,the mass vaccination of the population.
We can’t do full justice to all the intricacies of vaccines and how they work, but in this Advisory we will link you to trustworthy and relevant information (see our article on misinformationhere), together with safe links to trusted sites.
In the meantime, here is the headline news on the new Covid-19 vaccines.
Millions of South Africans are alive and healthy today thanks to modern vaccines. Vaccines are right up there with clean water and sanitation, safe food, antibiotics and effective anaesthesia in saving lives.
Over the last 100 years, vaccines have had a huge impact on human and animal health, resulting in the greatest effect on health and longevity than almost any other intervention throughout recorded history. Vaccines have changed the trajectory of generations, improved the prospects for all classes of society, generated prosperity through freedom from many debilitating diseases and allowed more people than ever before to have the opportunity to live full and healthy lives. They have brought diseases, such as smallpox, polio, measles and diphtheria, which had our great-grandparents living in justifiable fear, under almost complete control.
For an entertaining history podcast about one of the founders of many modern vaccines and the huge efforts vaccines take, seehere.
To achieve control of Covid-19, a safe and effective vaccine would be enormously helpful in getting us beyond the pandemic – ‘natural’ infection, even in the worst affected areas, has not reached levels where population-wide immunity is reached – which is why one should ignore arguments for letting the virus simply spread naturally.
In addition, ‘natural’ infection carries substantial health risks that do not apply to vaccines.
Do the Covid-19 vaccines work?
They seem to work very well, at least for the early candidates, results for which seem very promising: these vaccines have stopped people getting sick, and reduced the severity of the disease in those with “breakthrough” infections.
Initially, results were released through press statements, which is not the same as independent or “peer” review, the scientific standard that applies. The data on two of the vaccine trials have now been published in highly regarded scientific journals, and the results look very promising.
At the time of writing, three countries, the USA, Britain and Canada, issued Emergency Use Authorisation (EUA); the US and UK have already started vaccinating high-risk people. Germany will follow suit. China and Russia have similarly started vaccination programmes for certain designated groups with their candidate vaccines, although the full trial data on these have not yet been internationally reviewed.
There are lots of questions about these vaccines, mainly about how long the immunity will last.
Some vaccines last for a lifetime, some have a steadily waning (decreasing) immunity that needs a “top-up” or booster shot, or possibly even a new one every so often. It is unclear at this time in which category the Covid-19 vaccines will fall, in how long the immunity will last (they have only been trialled for a few months!).
Over time we will understand more about these vaccines: how protective they are, how long immunity lasts for, what impact they have on disease progression and death; the level of protection in the older as compared to younger populations, and safety in use in pregnant women, and children. Each successful vaccine will need to be carefully evaluated on an ongoing basis by theSouth African Health Products Regulatory Authority(SAHPRA), and plans will need to be made for their proper and effective distribution.
But are they safe?
The data thus far show that they all seem to be very safe.
Theside effectswe have seen have generally been what anyone who has had any vaccine will relate to – some pain at the injection site, and occasionally some chills, which disappear after a few days. These can scare people if they are not prepared, like any side effects, so counselling recipients will be important. Even in sicker people – frail or people with other illnesses, the vaccines seem safe for now. One vaccine has been associated with some allergic symptoms, some serious, in a very small number of those vaccinated who had previous allergies.
We always weigh safety against benefit with any medical intervention, including vaccines, and the safety bar for any vaccine is set very high, far higher than for tablets or other injections. Ideally, more safety data is required – and this will come – but this pandemic is serious enough to push forward with getting them into people, while keeping a very close eye on all safety data, something every regulator and hordes of researchers are doing.
SARS-CoV-2, the virus that causes Covid-19, provides much cause for concern – highly infectious with a high death rate among older people and people with serious illnesses like diabetes. In addition, we are concerned about the condition referred to as “long Covid” – a constellation of symptoms possibly related to the acute illness, which persist after the acute illness subsides. (see ouradvisoryproviding information about Long Covid).
The safety of vaccines is highly regulated by therelevant authorities, in our case SAHPRA. Before a vaccine can be licensed or registered in a country, the regulators examine all the data from all the studies. Long-term evaluation forsafetyandefficacyis important and is monitored by the regulators in tandem with the manufacturers.
As scientists and health practitioners, we are reassured that these vaccines have been tested in tens of thousands of people, some in relatively diverse populations (including in people with HIV), and some in South Africa. This gives us confidence that they will be effective in our setting and for all our people.
That sounds all very reassuring. So, we will be able to control the virus and get back to normal?
Regrettably, the answer, for now, is no.
At this time, there is a lack of information from the government on detailed plans to procure and distribute Covid-19 vaccines. The development of a safe and effective vaccine is only the first step. The trial results are better than we dared hope for (so far), but that is only the first step in what is a massive project, possibly greater than anything the country has attempted before. The scale rivals that of the preparations for the FIFA World Cup of 2010 and the roll-out of ARVs for HIV-positive people. But our experience and the know-how we developed there should stand us in good stead.
Preparations for vaccine distribution and access in South Africa
We are concerned that there is insufficient planning by the government thus far considering the magnitude of the project ahead and an inadequate sense of urgency regarding the vaccination project. It is possible, of course, that the government may well be far down the road, but the lack of communication and information on these possible developments equally create unease.
At the time of writing, the vaccination has begun in the US and UK, with other countries in Europe and Asia expected to follow soon. We have been assured that at this time, there is sufficient money available to vaccinate about 10% of the population. We are concerned that despite world-class vaccinology talent, substantial financial commitment in the Department of Health budget to other vaccines, a history of successful vaccination for children and aMinisterial Advisory Committeesolely focused on Covid-19 vaccines, the lack of information detailing a comprehensive vaccination programme is not yet on the table.
At the time of writing, not a single advisory of the Vaccine MAC has been published.
We are all heavily invested as scientists, health workers, and the population of SA that we are beholden to, to ensure our best efforts to control this pandemic. We are pleased to offer some practical suggestions, based on our experience from other pandemics, vaccines and health systems interventions. (If you are interested, read thefull published article in the SA Medical Journal, on which this advisory is based, for all the detail, including probable costs, some of the assumptions, possiblescenariosand some excellent articles, including a scaryeditorial).
In order to get the ball rolling, two urgent decisions have to be made.
First, South Africa has to swiftly identify a candidate or a portfolio of candidate vaccines and ensure they are speedily registered for use locally. We must pro-actively engage directly with manufacturers and work with other countries to ensure we are not left behind in the queue to get vaccines.
Second, there should be an engagement with big business, local philanthropic foundations, high net worth individuals, banks and medical schemes, with the express aim of developing public-private partnerships that will negotiate, finance, procure and deploy vaccines in our country.
Initially we will have to buy the vaccines from international manufacturers and possibly acquire some vaccine doses through theWHO’s Covax scheme. We must be aware that we are competing with the whole world for these vaccines and against far richer governments who have already bought up massive amounts of stock. (Canada, for example, has bought up to 10 times the amount of doses needed for its population, although they have announced that a significant amount of excess doses will be given to poorer countries in need).
South Africa dismantled its robust capacity to make vaccines for some reason in the early 1990s relying instead on importing vaccines from overseas manufacturers. We have some capability to be part of a tech-transfer agreement to locally scale up vaccine availability, and this should be part of our long-term plan. But it is unlikely to result in any local manufacture of vaccines during the course of 2021.
It is also vitally important that the government decisively secures the finances for vaccine access.
We can acquire the vaccine via three mechanisms:
Through the Covax facility;
bilateral agreements with manufacturers and
via bilateral agreements with other countries e.g. those with excess vaccine stock.
The Solidarity Fundis providing the initial deposit for the government’s procurement through the Covax scheme, in which it will be allocated vaccines according to various criteria at prices set by Covax. But the government must also simultaneously negotiate directly with vaccine manufacturers, in order to remain in control of direct procurement outside of Covax.
Who should be vaccinated first?
While we are waiting for the vaccine, there needs to be discussion about how we prioritise vaccine allocation.
Health care workers, the elderly, other front-line essential workers and those with comorbidities should be the first recipients of the vaccine. We can’t afford to have our health care workers and front-line workers ill if we are going to face recurrent surges. Ideally, we would then steadily vaccinate from the most vulnerable to the least in a systematic roll-out over the months following the receipt of vaccine stock.
We also need a public debate as to who else is regarded as front line – taxi drivers, waiters, food-till operators?
Health care workers and other essential workers should get their vaccine through work-places. For the elderly, strategies to vaccinate them will include deploying nurses and other qualified medical staff to offer vaccination at pension points, in communities and primary health care centres where people with chronic illnesses like diabetes and hypertension get their medication. Mass immunisation strategies in rural areas would have to be developed at district level in recurrent roll-out programmes. Using existing networks, such as private pharmacies, makes sense for broader distribution.
We will have to distribute the vaccine throughout the country.
This will require massive logistical coordination – one vaccine has extremely stringent refrigeration requirements, generally only found in research laboratories. Many of the other candidates require less onerous refrigeration, but still a cold chain – in a country where reliable electricity is a challenge. For a fascinating and sobering podcast on these logistics (which involve jet airliners, glass, dry ice and trucks, listenhere). Getting this right will require skilled planning.
Finally, the benefits of being vaccinated must be visible and noticeable to encourage people to get vaccinated – some vaccine candidates need to be given twice, a few weeks apart.
To get to the levels of immunity we need to breathe freely again, known as population immunity, where there is sufficient suppression of the virus to allow near-normal activity to resume, we probably require 60-70% of the population to develop immunity. For young children, it is fairly easy to offer Covid vaccination through the South African vaccination programme. However, no country in the world has successfully vaccinated adults at this scale – even for adult vaccines such as influenza, numbers are small in even the most highly vaccine accepting societies. We will need to learn from other countries and innovate locally to reach scale.
Collaboration and coordination on a grand scale
To be able to vaccinate 60-70% of the population will require deep collaboration among social partners and expert co-ordination. Vaccines will need to be delivered to and properly stored at clinics, pharmacies and all health facilities, public and private, that render care in the normal course. South Africa is blessed with thousands of such facilities, widely distributed throughout the land. They will all have to be made available and logistical coordination and support from all sectors of society will have to be mobilised. Organisations like the Red Cross, Gift of the Givers, MSF and others with technical skill and capability must be enlisted in this effort, as well.
Ethical obligations
As scientists and clinicians we are obliged to invest the programme with ethical obligations that must be diligently applied.
Vaccine access must be equitable and fair.There should not be an opportunity for exclusive access by the privileged and those with means only, as was the case in the early phase of the Aids pandemic. This underscores the need for the deep collaboration between, in particular, the private and the public health sectors.
There must be full inclusion into the vaccination programme of all those within our borders, including documented and undocumented foreign nationals, asylum seekers and refugees. It will be intolerable from an ethical point of view to subject foreign nationals to the exclusion that currently bedevils their access to public health. Such xenophobia would defeat the public health goal of controlling infection.
Vaccine prices must be transparent, fair and equitable.
The secrecy and lack of transparency that governments and manufactures employ must not be a feature of this vaccine procurement, or it will not only jeopardise access but will be the subject of rightful anger. The government and manufacturers must think long and hard before going with business as usual in a pandemic, as this lack of transparency will undermine trust, and reinforce the hands of anti-vaxxers.
Pharmaceutical companies should share technology, policymakers need to tackle patents that are barriers to access, and profits assessed against substantial public investment that has gone into many vaccines.
We need an urgent communication strategy that deals with vaccine hesitancy, that builds public trust and participation.
Are vaccines all we have available to us?
There are drugs and other interventions being evaluated that may provide both protection and treatment (as we have for malaria, flu, hepatitis B and HIV). None have proved successful yet for mild or asymptomatic Covid-19 although we have some interventions that work for severe disease. But keep an eye on theNICD,WHOand other trustworthy websites – and the press is likely to be flooded with reports if one comes through. We’re all holding thumbs and many of us are busy with this research.
In the meantime – physical distance, try your best to move social events and gatherings outdoors, avoid crowds both indoors and outdoors where physical distancing is not possible, wear a mask around others, and wash your hands regularly.
These methods really do prevent new infections.
If the vaccine works, can we go back to 2019?
We would so like to say yes, but that is unlikely, at least for the foreseeable future.
As we are likely to have more waves and hotspots in the future, the physical distancing and masks are likely to be with us until at least two-thirds of the population develop immunity against Covid-19. It will take months to years to vaccinate even two-thirds of South Africans (‘normal’ infection rates as we indicate above, are not nearly high enough to give population immunity),and then there is the issue of being able to access sufficient quantities of vaccines in the foreseeable future.
Some commentators have asked “well, if we can’t get rid of the masks, what is the point?’’ The point is to ensure older and more vulnerable people do not die of a scary virus, and the rest of us not be nervous of long-Covid symptoms. Vaccines won’t take away the nuisance of masks and physical distancing perhaps for most of 2021. With HIV, condoms played and continue to play a major role in stopping transmission, even when drugs are so effective they behave as a vaccine. Consider masks as the “condoms” of Covid.
Unfortunately, unlike SARS and MERS, it is highly unlikely that the virus which causes Covid-19 is going to disappear anytime soon, if ever. There may also be a future where the vaccines and natural infections eventually provide enough community protection for us to return to approximate normalcy. But it is fair to say that this pandemic, like all the other pandemics throughout history, will leave society on a different footing, with new ways of living to be adopted and new opportunities for re-making society on offer.
For additional trusted resources (and some fascinating history on the development of vaccines), see here:
The following people contributed to this advisory:
Professor Glenda Gray, University of the Witwatersrand and Medical Research Council.
Professor Shabir Madhi, Respiratory and Meningeal Pathogens Research Unit, University of the Witwatersrand.
Professor Marc Mendelson, University of Cape Town.
Dr Jeremy Nel, University of the Witwatersrand.
Professor Wolfgang Preiser, University of Stellenbosch.
Dr Aslam Dasoo, Progressive Health Forum.
Nkuli Mashabane, Dr Esther Bhaskar, Dr Karlien Moller, Dr Bronwyn Bosch, Dr Jo Woods, Celicia Serenata, Professor Francois Venter, all at Ezintsha, University of the Witwatersrand.
Fatima Hassan, Health Justice Initiative
Dr Dulcy Rakumakoe, private practice
Professor Wendy Stephens, Head, Department of Molecular Medicine and Haematology, University of the Witwatersrand
Professor Eric Decloedt, Stellenbosch University.
Dr Francesca Conradie, University of the Witwatersrand.
Professor Alex Van Den Heever, University of the Witwatersrand
Dr Regina Osih, infectious disease specialist.
Professor James McIntyre, Anova.
Professor Morgan Chetty, Visiting Prof Health Sciences, Durban University of Technology.
Dr Elijah Nkosi, private practice.
Professor Lucille Blumberg, University of Stellenbosch.
Adrienne Wulfsohn, Emergency Medicine Physician, UKZN
Dr Jantjie Taljaard, Tygerberg Hospital and Stellenbosch University.
Beyond the pandemic and possibilities for new knowledge architectures.
The Covid-19 pandemic is reshaping all dimensions of life as we know it, including higher education. Its impact is dictating how we interact with others, transforming how we socialise and care about one another, restructuring business and the economy, and altering how we think about sustaining our world. The pandemic has forced the global academy to question what it means to be a university, to reconsider its role in society and its relationship with other social actors.
Concomitantly, it has provided the academy with a moment to pause, to reflect and to propose new knowledge architectures that enable its reconfiguration in ways that advance flexible futures for all. The traditional role of higher education institutions centres on the creation of new knowledge, the development of high level and scarce skills, and the advancement of the public good.
This is against a rapidly changing technological landscape, in a world where new challenges emerge daily, and which, like the coronavirus, force change into unchartered waters. How, then, can universities be reconsidered to create social impact and to remain resilient amidst uncertainty?
This article proposes shifts in six areas – research and innovation, learning and teaching, people, transformation, partnerships and sustainability – which, coupled with strong, empathetic, visionary leadership, has the potential to develop revitalised knowledge architectures that enable the knowledge project of the academy to prosper.
The coronavirus pandemic and the subsequent national lockdowns exacerbated Africa’s already dire socio-economic challenges, including unemployment, poverty, inequality, the digital divide, corruption and the disproportionate share of diseases, amongst others. It brought to the fore the opportunities that exist on the continent, including Africa’s demographic advantage, its youth bulge and its ability to manage diseases.
The pandemic also underscored the important role of universities in conducting research, developing vaccines and potential treatments, influencing policy decisions, documenting the disease, adapting pedagogies for remote teaching and learning, and producing personal protective equipment for those serving on the frontline. It brought to light the capabilities of the academy to create quality knowledge whilst saving lives.
Covid-19 has paved the way for African universities to lead from the front on local issues whilst tackling global challenges head-on; ensured that the knowledge project supports a multiplicity of voices, methods and framings; and forged inclusive communities of scholars across the world.
Going forward, universities will also have to adopt an ecological ethos which values the interconnections between knowledge forms; draws strength from diverse ways to produce and disseminate knowledge; takes environmental and financial sustainability seriously and values people. Strategic and agile leadership, coupled with demonstrable shifts in the areas mapped later, may be the coordinates for reconsidering higher education.
Research and innovation
The response of universities to the coronavirus pandemic has repositioned higher education institutions as valuable knowledge generators. It has provided an opportunity to stimulate discovery research, including new clinical studies; to apply research in the domains of education through remote emergency teaching and online learning; to develop new scientific models in big data, development economics, bioinformatics and health economics; and to study the impact of the coronavirus through the humanities and social sciences, amongst others. It has entrenched the importance of evidence-based research, even though there has been a tendency to default to a health sciences approach based on mathematical modelling.
Universities may have missed a chance for transdisciplinary explorations that embody a multiplicity of perspectives, which are readily available in their midst. Universities should question if they have harnessed the opportunities to conduct more inter-, trans- and multidisciplinary research that demonstrate social solidarity in action.
The time is ripe for universities to reconsider their research horizons and to reflect on whether they are producing enough research with impact. In an environment where health inequality is growing, where there is greater social fragmentation, and gender-based harm and systemic racism is on the rise, a new research framework which balances large quantities of high-quality scholarship with impact is essential as is moving beyond measuring the impact of research by citation numbers and global ranking.
The new framework should include the rapid dissemination of knowledge, including publishing in quality open access journals and knowledge generation that encompasses training for innovation and entrepreneurship. It should nurture the next generation of scholars, entrench integrity and ethics, and be responsive to environmental changes.
Beyond the knowledge pipeline, this will require formally integrating the intellectual work of postdoctoral fellows and postgraduate students as knowledge producers in their own right. It is also important to map the research–policy– practice nexus and to ensure that intellectual labour is maximally translated into benefits for Africa and the world.
Global research alliances will have to work in concert towards deliberative, integrated goals rather than in ad hoc, often competitive and reactive ways, as is often the case.
The project of learning and teaching
As a response to the pandemic, universities globally have implemented emergency remote learning and teaching to rescue the academic year. Contact universities have had to repackage content, resolve issues related to data and devices, and digitise quality education.
The pandemic may have disrupted and displaced current orthodoxies around teaching and learning, which provides an opportunity to develop a new educative focus to fundamentally reshape the relationship between teacher, student and content, and the academy and society more broadly.
The emergency response to the pandemic has highlighted technology and digital inequality but has also presented opportunities to explore penetrable boundaries between contact, online and distance teaching and learning and the possibilities that this permeability allows.
Universities will need more time to explore the implications of online as a mode for engagement, while being aware of the limits and potentials for screen-based reasoning and thoughtfulness. When confronting new situations, good teaching enables peer engagement in class or remotely, so students gain different perspectives on issues in order to find solutions. Pedagogy that brings a diverse set of learning approaches to bear on transdisciplinary issues or ideas under discussion or study is experienced as the norm. Groups of students exchanging their views, integrating their experiences, and imagining different and flexible futures could be the basis for truly innovative thinking that is sparked by creative experimentation.
People
The pandemic and its disruptive nature should provoke focussed engagements on the possibilities of new knowledge architectures where students are integral producers of knowledge. Universities would need to explore thinking in communal and experiential ways and shift knowledge so that it can occupy multiple spaces at the same time.
Scholars should be able to evaluate and distill information and knowledge from multiple sources, have the capacity to think critically and be empowered to live ethical and socially responsible lives. They must share a multiplicity of voices with people across the world, enjoy access to new global publics and actively participate in the public sphere.
This happens when universities equip students at the undergraduate level with skills that will enable them to work at the cutting edge of disciplines and pursue a postgraduate trajectory that pushes the boundaries of their disciplines in ways that will deepen their academic and professional knowledge.
The pandemic has redistribute the knowledge economy in such a way that students can be sitting in a virtual class with students from other universities and academics from two universities can co-teach a course from completely different locations. The use of space and time has been reshaped fundamentally. Modern technology has also allowed us to extend our reach during this pandemic to reshape north–south knowledge relations in ways that were not previously possible, providing at once an opportunity for African universities to leverage their epistemic and physical location to advance and strengthen the knowledge project of the global academy.
For students, universities will need to be repaired so that they become aspirational sites that address their academic, health and wellness in a holistic way. Universities of the future will expand their engagement with students so as to inspire students to become active social citizens in their own spaces. It will provide an opportunity to rethink the concept of ‘graduateness’ – students who are able to think critically, who are problem-posers and problem-solvers, not only in relation to labour market priorities but also in relation to being human, vibrant, alert, caring and compassionate.
Universities will need to accelerate investments to meet the social, emotional and mental health needs of their staff members who are struggling with the stress and trauma of the pandemic and who have been isolated from colleagues and support systems for a prolonged period of time.
Working remotely has exposed that universities are high pressure environments for all.
Diversity and inclusion
Covid-19 should provoke dialogues on higher education and inclusivity. Universities will need to engage the intersectionality of discrimination and be alive to new forms of inequality and asymmetries. They must nurture well-rounded, active, resilient citizens who will contribute towards advancing society and transforming our world for the better. Universities will need to function as places of compassion, truth and, above all, reason. These values have largely been hidden from public view, resulting in a ‘narrowing’ of the ways in which higher education is understood.
An interdependent relationship exists between the diversity of people, knowledge, ideas and the curriculum, and future universities should be poised to drive social transformation both within and beyond the institution.
Transformation is critical because difference is central to the academic mission of any university, and diversity and inclusion are ambitions worth pursuing.
Building mutually beneficial and strategic partnerships
Future-facing universities will need to steward, maintain and cultivate strategic partnerships in an intentional way at the local, continental and global level. Continental networks and alliances need to be expanded based on common strengths, similar values and thematic areas.
The post-Covid-19 environment proffers opportunities for emerging alliances, strategic research partnerships, at all levels. It has levelled the playing field to a certain extent – universities across the globe face common challenges, some sharper in one place and less in another. African universities need to position themselves as generators of global knowledge and seize these opportunities as the world reframes itself.
Sustainability
This is a fundamental pillar on which all other areas are reliant. It means thinking beyond a post-Covid-19 future and includes optimising statutory income, activating new income through digitisation and innovation, securing third stream income and enhancing efficiencies and operations.
This includes cost replacement strategies, better and efficient use of resources, leveraging technology to innovate and reform administrative systems, and establishing cross-functional literacy and multidisciplinary teams in the administration of universities. More importantly, it means creating a culture of sustainability that pervades all aspects of work and treats sustainability as an intergenerational question, always knowing that how we act today, will impact those who come after us.
Leading African universities into the future
Amidst the global uncertainty inflicted by the coronavirus and the polarisation of the higher education terrain, societies are looking for alternatives to learning, educating and creating social impact. While universities have many moving parts, a shift in the six areas explored here may lay the basis for collegiality, cooperative governance and global solidarity.
These ambitions and values could be the compass as universities navigate a shared imagination of what it means to be a university in uncertain times.
Professor Ruksana Osman is the Deputy Vice-Chancellor: Academic at Wits University. This article was first published in the Issue 3 of the Wits Journal of Medicine, 2020.
Update 61: Adjusted level 3 implications
- VCO
Implications of adjusted Level 3 regulations for staff and students.
President Cyril Ramaphosa announced on 28 December 2020 that South Africa would move to adjusted COVID-19 level 3 restrictions from 29 December 2020 until 15 January 2021. The implications for staff members and students during this period are outlined below.
Supplementary and Deferred Assessments in January 2021
The majority of assessments including the supplementary and deferred assessments which are scheduled for January 2021 will be conducted remotely and online as far as possible. There are some exceptions where in-person assessments will continue with the appropriate COVID-19 protocols in place. Students should please check the examinations website and their student emails to determine if there are any changes to the format of their assessments. Readmission applications will be processed as they are submitted online.
Residences
Students who are completing the 2020 academic year or who are scheduled to write supplementary or deferred assessments may be allowed to stay in residences until their examinations are completed. Given that the majority of these examinations are online, a limited number of applications will be considered from those who may need to return to residences in January in order to complete the 2020 academic year, in line with the relevant ministerial directives and COVID-19 protocols.
Wits residence students who wish to return in January must apply for permission from their respective cluster managers and must provide proof of the examinations that need to be written in January 2021. Students in private, accredited off-campus accommodation are encouraged to make appropriate arrangements with these establishments.
Limited catering services (take-away meals) will be available in line with students’ meal plans. Students in need of food support are encouraged to make appropriate arrangements with the Wits Citizenship and Community Outreach unit.
The University reopens on 4 January 2021 and line managers (in consultation with relevant SET members) are requested to ensure that all offices are operational and adhere to Wits’ COVID-19 rules and protocols.
Employees are allowed to work from home if they are able to perform their duties remotely, with the permission of their line managers.
Those employees who are unable to work productively from home may be required to report to work if requested to do so by their line managers.
Workers whose services are required on campus for operational reasons are also required to report to work if requested to do so by their line managers. These employees may work on a rotational system as determined by their line managers, in line with national directives and University protocols.
Staff members who are over the age of 60 and who feel that they may be at risk, employees who may be living with co-morbidities, and expectant mothers who may be at risk should work productively from home during this time. Healthy employees over the age of 60 who do not have co-morbidities and who are not at high risk of infection are allowed to return to the workplace at their own risk.
Risk assessment and mitigation plans
All managers are required to update their risk assessment and mitigations plans and to ensure that the necessary measures are implemented timeously so as to minimise risk. A copy of the risk assessment must be forwarded to the entity’s assigned OHS&E Officer for reference and record purposes. The assigned OHS&E Officer will conduct ad-hoc inspections to check whether risk mitigation measures and health and safety protocols are in place, and will advise managers accordingly.
Permits
Permits will not be required but access to campuses and facilities will be limited. Security officers will manage pedestrian traffic, disband gatherings, and/or deactivate access cards if required.
Let’s keep safe
The best way to keep our community safe is to practice social distancing and good hand hygiene, and to avoid crowded, indoor spaces. It is compulsory for every person to wear a mask that covers the nose and mouth at all times, in line with the adjusted level 3 regulations.
It is distressing to hear senior officials increasingly talking down the prospects for the availability and usefulness of Covid-19 vaccines in South Africa.
The world is in the grip of a massive resurgence of the Covid-19 pandemic, in which SARSCoV-2, the coronavirus, appears to have produced a variant suspected of such great transmissibility that even the most stringent attempts at mitigation by non-pharmaceutical intervention is failing to contain the spread.
More chillingly, the increased spread of the virus is generating a corresponding acceleration in the numbers of people getting infected and, by extension, is exposing health systems in even the best resourced countries to an overwhelming burden with which they’re increasingly unable to cope.
Humanity is now facing the full force of the greatest public health emergency in modern history, with no sign that the force of the pandemic will abate anytime soon. The only instrument humanity now has to contain the pandemic, effective vaccines, are becoming available through an uneven and desperate race among nations. Even this hopeful intervention will not bring solace anytime soon.
It will take many months and huge resources to inoculate sufficient numbers of people for the pandemic to be suppressed. And that is the outlook if countries begin mass inoculation right now, as some 40 countries have embarked upon.
Many more are preparing to receive vaccine supply in the next several weeks to join the vaccination drive. For the rest, mainly the poorest nations on the planet, the global COVAX facility offers the only hope of receiving an adequate vaccine supply sometime in the next six to nine months, only after which can the months-long vaccination programmes begin.
It beggars belief that South Africa, against all reasonable expectations, finds itself in this group, since it is not a poor country, despite the best efforts of a corrupt political class to ensure that moniker. The stunning reality is that It has neither a secured vaccine supply nor a plan for mass inoculation in the foreseeable future that can withstand scrutiny. This portends for this country the worst ravages of Covid-19 in the year ahead.
This lack of foresight will visit on us the consequences of the greatest man-made failure to protect the population since the Aids pandemic, when we refused to provide life-saving medicines out of choice and against the desperate pleas of horrified medical and humanitarian agencies here and abroad and directly caused the deaths of hundreds of thousands of people. A high probability of a reprise of this is a monumental and unforgivable failing.
Developed and developing nations alike appear to have proceeded with early negotiations for future vaccine procurement several months ago without any qualms. South African officials appear to have eschewed such efforts, but what unique insights they may have in this regard is unknown. Assertions that SA knew better than many advanced and peer nations might have been dismissed as misplaced confidence, were the consequences not so deadly.
Astonishingly, even now, in the full knowledge of what we face and with dozens of countries worldwide, including African nations, embarking on mass vaccination programmes against Covid-19, it is distressing to hear senior officials increasingly talking down the prospects for the availability and usefulness of Covid-19 vaccines in South Africa.
This position is, at best, inexplicable, given the depth of available knowledge about efficacy and safety among several leading vaccine candidates being clinically trialled and evaluated right here in SA. That is why the recent commentary by senior officials regarding the government’s vaccine strategy in response to pointed enquiries from the press, health experts and labour and civil society formations, has sown great disquiet.
The unconvincing and defensive exposition of the department’s efforts, or to be precise, the lack thereof, deepens suspicions of and perhaps even confirms the absence of a coherent and composite vaccine acquisition strategy.
This communication strategy bears the hallmarks of a frantic cover-up and evasion of culpability. South African society has a fully justified expectation that, as a member of the G20 group of leading nations, most of whom are in the process of implementing vaccination, this country will also imminently embark on its own vaccination programme. There appears to be a public narrative to deliberately diminish these expectations.
Public acknowledgement by officials that they didn’t think it prudent to begin bilateral negotiations with vaccine suppliers, because they could not ‘take the risk’ of ordering vaccines in the event that they would not work, is shockingly disingenuous. An Advanced Market Commitment does not require upfront payment for the vaccine and commits the buyer to purchase vaccine only when it becomes available, at an agreed price and quantity.
It is a dangerous misconception, often exercised by arrogant local officialdom, to presuppose that a populace will willingly believe any deliberate fiction put to them. However, it will be even more worrying if these officials’ comments were made in ignorance of an elementary advance purchase mechanism and impels urgent enquiry into their fitness to manage such a critical portfolio.
The posture of the Ministerial Advisory Committee on Vaccines appointed last September, suggests that it has been dragooned into the specious approach of the department. The comments of the chairman of the vaccine committee align closely with the comments of the DDG and other officials of the department who are supposed to lead the vaccine acquisition programme of the government. Their admonishment that vaccines are not a silver bullet”, or that they “do not end epidemics” are frankly astounding.
Several advisories of the vaccine committee have been issued, but none have been published. The committee’s silence on the matter has been deafening. This suggests that the committee either concurs with this lack of transparency and condones a wholly inadequate vaccine acquisition policy, or it does not, but has been officially muzzled.
This can only mean that the responsible officials have indeed missed the vaccine boat and a huge damage limitation exercise is underway to escape scrutiny and likely censure for this unforgivable failure, which will be measured in lives lost in their thousands, sickness for tens of thousands, a broken healthcare system and profound and ongoing economic damage.
It is unconscionable that this has been allowed to occur and it is to the discredit of the advisory committee that it appears to have been enlisted in this exercise. Its members have the ability and expertise to produce a transparent and accelerated vaccine acquisition strategy, measured in weeks, not months. That such a strategy is lacking puts them in the invidious position of having to reaffirm their scholarly credibility and ethical composure. This dissonance deepens the suspicion that the committee is not free to do its work.
In a moment of existential threat, this incoherence in lead institutions is simply intolerable. The lack of any visible sense of urgency to inoculate healthcare personnel is particularly worrying because they are at the highest risk of contracting Covid-19 and are the people’s ultimate resort in the frightening eventuality of infection. If such a critical sector has been neglected, what chance then of the rest of the population being vaccinated in good time?
South Africans, pummelled mercilessly by the pandemic, have an untrammelled right to demand the immediate public disclosure of the advisories of the vaccine MAC and a full account of the disposal of any of its recommendations. There must be no further cover-up of the ongoing failure to secure vaccine supply sufficient for South Africa’s needs. Getting beyond the pandemic is far more urgent and infinitely more important than preserving political fortunes, bureaucratic careers or ministerial appointments. The well-being of the people must always come first.
The President of the Republic, through his constitutional authority, will have to dispense with his otherwise admirable political consensus management and wield the axe against the members and officials in his administration who are responsible for this perilous fiasco and immediately set about correcting the course we have been placed on. Covid-19 leaves him no other choice, because, as it has so viciously demonstrated, it has no respect for the banal affairs of state or government.
Dr Aslam Dasoo, Convenor, Progressive Health Forum; Prof Glenda Gray, President, SA Medical Research Council; Prof Guy Richards, Emeritus Professor in Critical Care, Wits University; Professir Marc Mendelson, Head of Infectious Diseases and HIV, University of Cape Town; Dr Fareed Abdullah, AIDS and TB Research, SA Medical Research Council; Professor Francois Venter, CEO, Ezintsha, Wits University; Professor James McIntyre, School of Public Health, University of Cape Town; Dr Adrienne Wulfsohn, Specialist in Emergency Medicine, Inkosi Albert Luthuli Hospital; Professor Alex van den Heever, School of Governance, Wits University(Writing in their personal capacities and with the support of colleagues here and abroad.)
Towards herd immunity from Covid-19: Costing a vaccine strategy for South Africa
- Alex van der Heever, Imraan Valodia, Lucy Allais, Martin Veller, Shabir Madhi, and Francois Venter
This article examines and estimates the financial implications of a vaccine strategy with a goal of achieving herd immunity.
It takes account of the roll-out phases identified by the Department of Health and vaccine prices available in the public domain. It finds that such a programme is affordable and implementable.
The overall cost of all three phases of a vaccine roll-out in South Africa, based on the AstraZeneca (AZ) vaccine andCovaxsupplies, would be R7.4-billion — with the need to consider an additional R1.2-billion for nursing costs. This makes a total outlay of R8.6-billion.
On the high side, the total cost of using the rival Pfizer vaccine would be R15.2-billion, with the extra R1.2-billion for nurses resulting in an outlay of R16.4-billion.
In evaluating the economic merits of this outlay, consideration has to be given to the approximate loss of R389-billion in economic output that occurred due to Covid-19 in 2020, together with the dramatic deterioration in the fiscal position of government. Even the highest cost is roughly half the value of tax revenue lost on tobacco and alcohol in 2020, estimated at R35-billion (which includes all tax revenue lost and not merely the excise taxes).
Based on this, it would be a false economy to delay the implementation of a full-scale vaccination programme on the basis of affordability. It is also highly probable that many sources of funding outside of government can be mobilised to expedite implementation.
It is therefore crucial that any further delays to the vaccine programme be removed and it be given the highest priority in government and the country.
Context
South Africa lost approximately 8.2% of GDP (or R389-billion) in 2020 due to the Covid-19 pandemic. In large part this was the result of the Level 5 and Level 4 lockdowns beginning in March. The remainder is due to reduced demand for certain services both before and after the heavy lockdowns ended. These include, inter alia, restaurants, hotels, gyms and medical practices.
However, many high-risk settings are vulnerable to behavioural lapses as life appears to return to normal. Viral transmission therefore increases as people return to work, certain behavioural adaptations lapse and society tries to find a “normal” that includes human contact. As the virus continues to circulate it also mutates, posing the risk of new variants that are more transmissible, involving more cases of severe illness and death.
In the absence of herd immunity (where the population levels protected from infection or less infectious are sufficient to bring about an interruption in the chain of transmission of the virus between people and within the population) all countries will experience years of periodic surges, resulting predominantly from the swings and roundabouts of human behaviour and government interventions of various forms.
Of all public health responses, vaccines are among the most effective and permanent. Asevidence of this, smallpox, poliomyelitis, hepatitis B, measles, tetanus, diphtheria (whooping cough) and pneumococcal conjugate vaccine have reduced the morbidity and mortality of infectious diseases worldwide.
Efficacious vaccinesaretherefore central to the management of many infectious and contagious diseases globally. Other infectious diseases, such as HIV and tuberculosis, are contained through early diagnosis and treatment, while cholera requires clean water.
In the case of Covid-19, vaccine development has taken on unprecedented proportions and has had unparalleled success in efficiency of development. Multiple vaccine candidates began development and trials on an expedited basis in the second quarter of 2020. To address the international crisis, many vaccines began production in anticipation of approval in late 2020 and early 2021.
For South Africa to derive advantage, however, it needs to implement a vaccination strategy at a population level. Without this there will be insufficient immunity to avoid any resurgence in the substantial residual susceptible population.
The achievement of herd immunity depends on approximately 70% of the population developing immunity against SARS-CoV-2 infection or reducing their infectiousness. However, the longer it takes to roll out a programme, the more times a country will face a significant resurgence with all the contingent economic and social harm.
The success of a vaccination programme for Covid-19 will therefore influence the time taken to achieve herd immunity. The longer it takes, the more damage to the economy and society.
Elements of a strategy
Vaccine procurement
Two approaches to accessing vaccines present themselves.
First, there is the Covax arrangement which seeks to pool funding for a number of countries and to guarantee that up to 20% of their populations are covered. An upfront deposit is paid into the pool equivalent to 15% of the value of the commitment a country makes to purchase.
As and when vaccines are approved as efficacious and safe, vaccine manufacturers are committed to making agreed doses available for distribution. This framework seeks to assist low-income countries to gain access to vaccines. Higher and middle-income countries such as South Africa have participated to cross-subsidise income-compromised countries that will have difficulties accessing vaccines through bilateral arrangements.
Second are bilateral arrangements which many countries have entered into to expedite vaccine availability throughadvance market commitments(AMCs). As vaccines were under development during 2020, to ensure availability in 2021, many countries paid deposits against the supply of designated doses for delivery once regulatory approval had been obtained.
The significant benefit for the purchaser is guaranteed access once the vaccine has been developed.
Once a vaccine has regulatory approval, however, it is relatively risk-free for a country to procure supplies based on vaccine availability. The AMCs may, however, indirectly serve to restrict supplies for countries seeking to obtain vaccines without such an arrangement – at least initially. Up to 8.6 billion doses had been committed by the end of 2020, the bulk of them to high-income countries. It is probable that most of these arrangements involved AMCs.
South Africa, which falls into the upper-middle-income country group, however, had no advance purchase commitments through bilateral agreement at the time of writing, other than the Covax facility (which is also a version of an AMC). Other upper-middle- and lower-middle-income countries have, nevertheless, made commitments to accessing 1.1-billion and 1.96-billion doses, respectively.
By the end of 2020 South Africa had only committed to being part of the Covax arrangement, with a commitment equivalent to 10% of the national population, at a cost of R2.2-billion.
Despite falling into the upper-middle-income category of countries, South Africa chose not to enter into any bilateral agreements using AMC arrangements. This creates some risk that South Africa may face constraints in accessing vaccines in the early part of 2021 and may not be able to achieve herd immunity targets by the end of the year.
Indications are that the Covax facility will only deliver some vaccines around April 2021, exposing South Africa to an expected winter resurgence without vaccines as a preventive measure.
As a strategic objective, therefore, South Africa needs to urgently focus on high-volume bilateral agreements to supplement the Covax arrangement prior to April 2021 (i.e. in preparation for the anticipated winter resurgence). This would make available vaccines that have proven to be efficacious, safe, affordable and with manageable cold chain implications. It would, however, be optimal to finalise such agreements before the end of January 2021. Selected manufacturers need to be expressly encouraged to seek domestic regulatory approval where they have not applied as yet.
While this is recognised as an aspirational goal, it reflects the best possible outcome for managing the local epidemic.
Prioritisation
Government has outlined in broad terms a prioritisation strategy for rolling out a Covid-19 vaccine programme for South Africa. This involves three broad phases.
Phase 1focuses on frontline health workers, including support staff and community health workers. The Department of Health (DOH) indicates this number at 1.25 million or 2.1% of the total population.At two doses for a complete regimen this would amount to 2.5 million doses.
Phase 2focuses on high risk groups, including the aged and people with comorbidities. Broadly speaking, this could amount to about five million people or 8.3% of the total population.At two doses for a complete regimen this would require 10 million doses.
Phase 3focuses on the rest of the adult population, excluding persons under the age of 16. The young are excluded as the vaccine trials did not cover them. Broadly speaking, this amounts to about 35.8 million people or 59.6% of the total population.At two doses for a complete regimen this would amount to 71.5 million doses.
Assuming vaccine availability, phases 1 and 2 should be completed prior to May 2021, to reduce the impact of any winter resurgence on healthcare workers and those more vulnerable to severe illness.
An important question arises concerning the feasibility of vaccinating the residual adult population during 2021. From a strategic perspective, South Africa should pursue this as a goal even if it proves logistically impossible to finalise during 2021. As vaccinating this part of the population is required to achieve herd immunity and (hopefully) slows the emergence of mutations, it is imperative that every attempt is made to begin phase 3 in April/May and complete it if possible in 2021.
Again, it is recognised that this is aspirational. But nevertheless it offers an indication of the approach which best addresses the contingencies facing South Africa in 2021.
Financial feasibility
South Africa has the benefit of two large health systems, one tax financed and one through prepayment (contributions) to medical schemes. Together these systems achieve universal coverage through some form of prepayment. It will be important to fully utilise the capabilities of both systems to expedite the rollout of vaccines.
Two features of both systems will determine the speed and efficiency of any rollout. The first is funding the vaccine procurement. The second is the administration of the vaccine to the entire adult population. The former is evaluated here, while the latter is only addressed from a costing perspective.
To assess the financial implications of the proposed phased strategy of government, a range of vaccine candidates are analysed based on their pricing to date and the evidence of efficaciousness and safety. Their main characteristics are summarised inTable 2.
The three vaccines are: Pfizer, which requires two doses per regimen (this vaccine has been found to be efficacious and safe); Johnson & Johnson (J&J), which requires a single dose per regimen (this vaccine has not as yet been approved by a regulator and data for the single dose regimen is not yet available but is assumed to be sufficiently efficacious and safe for the purposes of this costing); and AstraZeneca (AZ), which requires two doses per regimen (which has been found to be efficacious and safe).
Of the three, both J&J and AZ have manageable cold chain implications as both can be refrigerated with a normal household fridge. The Pfizer vaccine, however, requires storage at -70oCelsius, which could prove problematic in South Africa as the required fridges tend to be available only in research facilities and to procure them at scale would probably prove difficult.
Including supply chain costs, assumed to be 25%, the cost per regimen (accounting for the number of doses) works out the lowest for AZ at R145 with J&J a close second at R181. The Pfizer vaccine is higher than both at R362.50.
When all the characteristics are taken into account, the AZ vaccine is a good candidate for wider rollout given its cost. Its only disadvantage relative to J&J is the need for two doses rather than one. However, it is not as yet known whether the single dose works or, if it does, what the relative durability will be to two doses of AZ.
If South Africa adopts the DOH rollout and excludes the Covax arrangement, the following costing implications are implied (excluding supply chain costs): (Table 3):
For phase 1 the total cost ranges from R0.2 to R0.5 billion.
For phase 2 the total cost ranges from R0.7 to R1.8 billion.
For phase 3 the total cost ranges from R4.3 to R10.8 billion.
For herd immunity, the total cost ranges from R6.1 to R15.2 billion
Based on the DOH budget agreed with Covax, a higher cost per regimen (R366.70) is implied than with either AZ or J&J. The agreement actually comes in closer to Pfizer’s R362.50.
Based on this, if supply can be guaranteed through bilateral agreements it would make sense to limit exposure to the Covax arrangement.
If the Covax agreement is included in the mix, the total cost for herd immunity, based on the AZ vaccine, becomes R7.4-billion, i.e. a difference of R1.5-billion without Covax.
A further consideration is the implication of supply chain costs, which often include significant questionable mark-ups. It is not always easy to estimate these. For the sake of simplicity, a simple 25% mark-up has been assumed to provide a rough indication of the full cost of a programme to achieve herd immunity. For illustrative purposes, this adds R1.5-billion to the AZ-based programme with Covax in the mix, and R1.2 billion without Covax. It should be noted that these markups are included in the total costs discussed above and outlined inTable 3.
For completeness, it may be necessary to employ an additional nursing staff complement to avoid any diversion of the workforce away from frontline services. A rough indication of the nursing requirement assumes that one nurse can vaccinate roughly 26 people in a day. To vaccinate 40 million people over a 12-month period, assuming weekends and public holidays are used, will therefore require 8,851 staff nurses. Based on present salaries, this would translate into an annual cost of R1.227 billion.
While the cost of a vaccination programme appears relatively affordable for South Africa, the pandemic has severely affected government’s finances. Consideration therefore must be given to diversifying the revenue sources to remove or at least mitigate fiscal considerations as an obstacle to affordability.
A number of options are therefore raised here, together with an indication of possible prerequisites for their consideration.
First, South Africa’s medical schemes are in a position to finance all the vaccination costs for their members.
To ensure this happens, the Minister of Health has added the Covid-19 vaccine and all associated costs to the list of mandatory medical scheme benefits (referred to more commonly as prescribed minimum benefits or PMBs) that must be covered at full cost.
In vaccinating 40 million people, medical schemes will carry between R0.9-billion and R2.3-billion of the total cost through PMBs.
Medical schemes could make an advance payment into a facility/fund which would then facilitate access to vaccines without complications.
Second, as medical schemes achieved underwriting surpluses in 2020 due to the significant net drop-off in demand for healthcare services due to Covid-19, consideration can be given to a request that medical schemes donate a portion of their funds toward the purchase of vaccines for non-medical scheme members.
This arrangement would have to be on a voluntary basis as not all schemes may be in the same financial position. However, as medical schemes cannot by law pay for services for non-members, the Council for Medical Schemes would need to provide individual exemptions in terms of section 8h of the Medical Schemes Act.
The council has broad powers to exempt any person from any provision of the Act. An exemption should be granted where it conforms to the objects of the Act, which would be the case in this instance as the ending of an epidemic has implications for medical scheme members and non-members alike.
Third, large private corporations could agree on a voluntary basis to make donations toward the vaccination of non-members of medical schemes.
A single facility could be created into which the finances from the above three sources are paid. This could be the Solidarity Fund, or any other vehicle able to serve a similar purpose.
Putting it all together
Based on this analysis, the cost of a Covid-19 programme is far from prohibitive and could easily be financed by government on its own, private actors on their own or a partnership between government and private actors.
It is clear that the Covax facility cannot address South Africa’s goal of achieving herd immunity timeously. Bilateral approaches are therefore urgently required to expedite a national rollout programme to begin as early as possible. The three phases as proposed by the DOH appear reasonable.
The total cost of the first two phases of the rollout are negligible, irrespective of the vaccine chosen. Phase 1 would cost between R0.2-billion and R0.5-billion with a requirement for 2.5 million doses assuming two doses per regimen. Phase 2 ranges from R0.7-billion to R1.8-billion with a requirement for 10 million doses assuming two doses per regimen. In total, phases 1 and 2 require 12.5 million doses.
It should be noted that virtually all frontline healthcare workers are on medical schemes and the government need not fund their vaccines. (Note thatTable 2doesn’t reflect this as the split between the public sector budget and medical schemes is just a straight ratio of medical scheme members to the population dependent on the public sector.) The entire phase 1 is therefore an expense for private funds without any change to any law or public service configuration.
Phase 3, which takes South Africa to herd immunity, is also affordable, ranging from R4.3-billion to R10.8-billion. On the two-dose regime, 59.5 million doses would be required.
The overall cost of all three phases, based on the AZ vaccine together with Covax in the mix, would be R7.4-billion, with the need to consider an additional R1.2-billion for nursing costs, i.e. a total outlay of R8.6-billion.
On the high side, the total cost based on the Pfizer vaccine would be R15.2-billion, with an extra R1.2-billion for nursing, i.e. a total outlay of R16.4-billion.
The nurse contingency would depend on the operational approach adopted as some of the costs can be carried through the diversion of staff from current activities. However, overtime and additional nurses will carry a net cost implication.
It is worth noting that Level 5 lockdown cost South Africa in the region of R13-billion a day and has resulted in an estimated 8%-9% decline in gross domestic product for 2020. The accumulated debt of government is moving rapidly towards 100% of GDP and key industries are suffering harm from which they will take years to recover.
Furthermore, government is not in a position to provide social relief to people harmed by the pandemic due to its stretched resources.
Importantly, even the high estimate of the vaccine programme is roughly half the cost of the tax revenue foregone by government due to the alcohol and tobacco bans, which amounted to roughly R35-billion (taking account of all tax revenue sources and not just the excise taxes).
While the delay in expediting bilateral arrangements may work against South Africa, initiating negotiations are the test of what is feasible. As bilateral arrangements are plainly in the national interest, these should be expedited.
The need for an expedited programme also requires that trade-offs may need to be made between prices and speed of implementation. The costs of being slow potentially far outweigh the costs of a failure to reach herd immunity expeditiously.
It is worth noting at least two uncertainties that need to be accounted for in any strategy.
First, it may not be necessary to vaccinate 70% of the population to achieve herd immunity if natural infections induce durable immunity. The reported infection levels potentially undercount by several million people, a number that may increase significantly by the end of the current (second) surge. This could work in favour of an expedited strategy to achieve herd immunity.
Second, vaccine trials have mainly evaluated efficacy against Covid-19 illness, which is difficult to determine if the vaccine protects against asymptomatic infection. The high efficacy against mild Covid-19 illness, however, suggests that vaccines may have an impact on infection as well. Also, a vaccine may reduce infectiousness even if not preventing infection, which would contribute to inducing “herd immunity”.
These unknowns need to be taken into account as any vaccination programme is rolled out.
Alex van den Heever isAdjunct Professor at the Wits School of Governance
Shabir Madhi is Professor of Vaccinology: University of Witwatersrand and director: MRC Vaccines and Infectious Diseases Analytics Research Unit (VIDA)
Francois Venter is Deputy Executive Director of the Wits Reproductive Health and HIV Institute at the University of the Witwatersrand
Imraan Valodia is Professor of Development Economics at the University of the Witwatersrand
Martin Velleris Dean of the Faculty of Health Sciences at the University of the Witwatersrand and a Professor in the University’s Department of Surgery
Lucy Allais is Professor of Philosophy at the University of the Witwatersrand and director of the Wits Centre for Ethics
Why the state’s new toys won’t help South Africa’s response to Covid-19
- Jo Vearey, Sally Gandar, Rebecca Walker and Francois Venter
Drones, dinghies and an army helicopter - the new toys are diverting resources, and diverting attention.
The government’s decision to focus on tracking, detaining and deporting migrants as they cross into South Africa ensures that their ‘illegal’ status and/or failure to secure the bona fide negative Covid-19 test certificates, currently required to enter into South Africa, is focused on at the expense of the many systemic challenges faced in accessing documentation – including Covid certificates.
Whilst it was colonial cartographers who initially penned the painful lines that broke up communities across the region, it is the South African state that is now thickening them.
Long associated with anti-foreigner, xenophobic and nationalistic sentiments, South Africa’s politics have – prior to and during the Covid-19 pandemic – driven uninformed, non-evidence-based and potentially dangerous international immigration/migration policy discussions and processes.
As a medical doctor by training, the Minister of Home Affairs – Dr Aaron Motsoaledi – should know better. Whilst he haspreviously failed to ensure the safetyof South African citizens who work in or access services at Department of Home Affairs (DHA) offices, throughinadequate provision of PPE, Motsoaledi has invested in increasingly restrictive measures at our borders, including an array of new security toys:drones, dinghies and an army helicopter.
This is in spite ofprevious studiesthat have clearly demonstrated the wasted expenditure of state funds in its failed attempts to restrict movement across South Africa’s borders.As predicted, the 40km fence erected along South Africa’s border with Zimbabwe in March 2020 did nothing more than waste money, which could have been put towards South Africa’s dismal vaccine procurement approach.At the discounted rate of $20 — approximately R200 for two doses ofPfizer-BioNTech Covid-19vaccine(that South Africa says is still too expensive), 200,000 healthcare workers could be vaccinated. The minister’s new toys are diverting resources, and diverting attention.
For an infectious disease containment strategy to succeed, everyone must be included. This applies to diseases such as HIV and tuberculosis, for which South Africa has some of the highest rates in the world, and now, most urgently, to Covid-19. Despite the fact that non-discriminatory inclusion is a basic public health and disease control principle, hard battles have had to be fought over many years to ensure thataccess to HIV and tuberculosis services is available to all in South Africa– including both citizens and non-citizens alike – and it looks like this is going to be the case once again in 2021 with Covid-19 testing, treatment and, ultimately, vaccination.
Non-citizens have predominantly beenside-linedin South Africa’s Covid-19 interventions while the government falls back on those familiar (and unsubstantiated) claims that foreigners are to blame for state failures with its Covid-19 response and forward-planning. The spectacle of heightened security at the borders combined with dramatisation of the numbers returning to South Africa is a politically convenient distraction from the real challenges experienced by non-citizens – which are often the result of South Africa’s political and administrative processes.
Annually, migrants travel home to visit family and friends and return to South Africa for the start of the New Year. Yet this year, with a full lockdown imposed by the Zimbabwean state and the “amended” Level 3 lockdown in South Africa, it is unsurprising that many are desperate to return, fearful of being unable to resume work and education, and to get back to their lives, families and communities here. But the government’s decision to focus on tracking, detaining and deporting migrants as they cross into South Africa ensures that their “illegal” status and/or failure to secure the bona fide negative Covid-19 test certificates, currently required to enter into South Africa, is focused on at the expense of the many systemic challenges faced in accessing documentation – including Covid certificates.
This focus also diverts attention from thecatastrophic (and for some, fatal) situation witnessed in Musina in December, and from the need for appropriate border management of Covid-19 we require at all our ports of entry and exit. Collectively, these processes risk producing challenges that will further stall progress towards effective management of the Covid-19 pandemic by undermining attempts to develop coordinated, cross-border, migration-aware and mobility-competent health programmes. They risk pushing migrants into irregular routes and/or deterring both regular and irregular cross-border migrants from accessing Covid-19 interventions once in South Africa. And, yet again, political opportunism is able toignore the realitieson the ground and instead continue to claim that being undocumented is a chosen act of criminality rather than the result of political and systemic failures which plague the immigration processes.
This chimes well withthe latest false claimsand hate speech of the#PutSouthAfricansFirstmovement on social media,which drivexenophobia and the incitement of violenceand indicate anincredibly dangerous and often life-threatening symptom of South Africa’s unhealthy social and political environment. Whilst by no means unique to South Africa, it is this increasingly nationalistic context that the necessarily inclusive programming needed to control the Covid-19 pandemic must contend with. A consequence of South Africa’s growing nationalism is its “investment” in an increasingly restrictive and security-focused approach to the management of international migration (whilst simultaneously claiming it cannot afford the necessary vaccination plan urgently required to control Covid-19).
The metaphor of a border – of keeping “them” away from “us” – often creeps into popular thinking about infectious disease control. Whilst there is some truth in this, it is not as straightforward as many would like. These borderlines, however thickly drawn and secured, don’t prevent the spread of communicable diseases, including diseases endemic to the highly mobile southern African region – HIV, tuberculosis and malaria – and, as of 2020, Covid-19. As political tools, they do not reflect the realities of an economy built on migrant labour and a region shaped by the movement of people.
Damaging government processes include the development of theWhite Paper on International Migration(July 2017),amendments to the Refugee Act and Regulations(effected in January 2020) and worrying clauses in theNational Health Insurance White Paper; collectively, the rights of non-citizens to preventative and curative healthcare have been increasingly eroded. This does not make public health sense.It seems that theCovid-19 pandemic is being used by the DHA and others to justify the implementation of increased security measures along borders, with a focus on the Beitbridge/Musina land crossing.
The latest DHA policy documents were published for public consultation on 31 December 2020. TheDraft One-Stop Border Post Policy, and theDraft Official Identity Management Policy, both illustrate significant focus on national security and the protection of South Africa’s sovereignty. Such issues and functions are not usually associated with a government department tasked with governance and administration roles in terms of the civic registration of citizens, and the management of international migration.
Increased security measures at borders, as well as the intensified focus on national security by the DHA and the current Covid-19 context, open up opportunities for health status (or perceived health risk) to be applied as an additional securitisation measure through which to further restrict movement across national borders and to justify the arrest, detention and deportation of non-nationals. At present, this takes the form of the requirement for a negative (costly) Covid-19 PCR test and compulsory health screening at borders.
For those without a valid Covid-19 negative test certificate,rapid antigen testing (at a cost of R170, to be borne by the traveller)is now offered. Whilst the management of any pandemic requires appropriate disease management strategies – including in relation to the movement of people – they can all too easily become counterproductive. Given that South Africans moving extensively across the country aren’t required to provide proof of a negative Covid-19 status, why should we be demanding this from those crossing land borders?
Current work in South Africa, including efforts led by theHealth Justice Initiative, to overcomevaccine nationalismand hold the state to account presents a critical moment for ensuring that all in South Africa are included in the vaccination plan and that strategies for a regional approach to vaccination are actively considered. Whilst questions around the adequacy of Covax are being asked, and realisation of the limited action taken by the state to date, there is a need to consider collective, multicountry negotiations with pharmaceutical companies.
Services at points of entry, and mobile healthcare services in border areas, involve well-trained, immigration-sensitive and capable healthcare workers/community-based workers who should be involved in all mobilisation campaigns and in the roll-out of the vaccination programme. Civil society networks that involve migrant populations – such asMigrant Health Forums, including those that function across borders – need to engage with work surrounding the vaccination plan.
Whilst theCovid-19 vaccine fiascoplays out in South Africa, we highlight three key considerations related to migration. Firstly, the movement of people within the country – how will planning and roll-out approaches engage with the high levels of mobility nationally? Will people have to attend the initial facility for their second dose? What if someone has since crossed a border into or out of South Africa? Secondly, how will inclusive access for all in South Africa be assured (via a “one country one plan” approach)? And finally, given our position within a region of high population mobility, how will we support regional vaccination planning and programming? TheInternational Health Regulations(IHR) recommends that states sharing borders enter bilateral/multilateral agreements for the development of a common response to a health crisis. Not only should this mean that more appropriate interventions are in place in border areas, but a regional strategy for vaccination must be considered.
A key question that must be engaged with relates to vaccine passports; will these be required for Southern African Development Community (SADC) nationals and what will this mean in both the short and longer term? Concerns have already been raised about the potential for a black market in vaccinations (in addition to the black market developing in the provision of negative Covid-19 PCR test certificates), including the need to ramp up security when transporting the vaccine.
Without a transparent roll-out plan that appears reasonable, rational and accessible to all, then there may well be a security risk for the vaccine doses themselves (including a potential black market in vaccinations and threats to the transportation of the vaccine), but it’s unlikely to come from migrants or migration.
Basic public health sense states that everyone everywhere must be included in all responses to Covid-19. This is especially critical when thinking about vaccines, including rethinking the ways in which states finance health interventions and urgent action to address the ways in which non-citizens are treated by the state and all in South Africa.
Southern Africa is already behind in vaccination plans, and South Africa has the opportunity to lead the way for the region, ensuring all within the SADC are protected, not just those fortunate enough to be born south of the Limpopo River. We need all hands on deck and all inhabitants included in the solution. Only then will we stand a chance of gaining control of this pandemic.
Jo Vearey is with the African Centre for Migration and Society (ACMS), Wits University. Sally Ganda is with the Scalabrini Centre of Cape Town. Rebecca Walker is a post-doctoral research fellow at the African Centre for Migration & Society, University of the Witwatersrand. Francois Venteris the head of Ezintsha at the University of the Witwatersrand.
SA's vaccine strategy mistakes
- Ina Skosana, Ozayr Patel with Shabir A. Madhi
Pasha 91: Blunders that left South Africa trailing in the vaccine stakes
The South African government has announced plans to vaccinate about two-thirds of its population against COVID-19 by the end of the year. The aim is to do this in three phases, starting with healthcare workers in phase one, the elderly and those with co-morbidities in phase two and the rest of the population in phase three.
But the plan has been vehemently attacked as lacking in any detail. In addition, the government has been lambasted for failing to acquire vaccines.
Professor Shabir Madhi unpacks what’s gone wrong. The first major error was the South African government’s decision to put all its eggs in the COVAX facility basket. This was a bad decision because South Africa is viewed as a middle-income country, which meant that it would pay more for vaccine procurement through COVAX than if it had pursued bilateral agreements with the likes of pharmaceutical companies such as AstraZeneca.
Madhi, who is Professor of Vaccinology and Director of the SAMRC Vaccines and Infectious Diseases Analytical Research Unit, University of the Witwatersrand, explains that this is just one of a litany of mistakes.
South Africa failed to get its act together on vaccines
- Shabir A. Madhi
Critics of the South African government argue that it has done too little too late to secure vaccines, and that it doesn't have a proper roll-out plan in place.
South Africa has an estimated population approaching 60 million. To achieve herd immunity against COVID-19, the government recently set the ambitious goal of vaccinating 67% of the population - roughly 40 million people. According to the outline of this plan, this would be achieved within 2021.
But is this ambitious target even feasible?
In my view the proposed COVID-19 strategy is not a strategy, but rather an aspirational goal. And an unrealistic one at that.
The elephant in the room is that the government has set a target of immunising two thirds of the population but it hasn’t as yet secured the 80 million doses this would require.
This is what we know. South Africa had committed to purchasing enough vaccines for up to about 10% of the population through the COVAX facility – roughly 12 million doses. The facility is a global collaboration for speeding up the development, manufacture and “equitable” distribution of new vaccines. These vaccines are likely to become available from February onward and spread out over the course of the next few months.
The Department of Health has also indicated that 20 million doses of vaccine will likely be received by the end of June or July. As such, it appears that the government has been successful in procuring an additional 6.5 million over and above vaccines from the COVAX facility, and procured about 1.5 million doses from the Serum Institute of India (SII), which is producing the Astra Zeneca vaccine. The initial 1.5 million vaccines from SII have been earmarked for the immunisation of health care workers during the first phase of the COVID vaccine rollout.
But there’s a lot that remains unclear. For example how will the jabs for 1.2 million workers in health facilities be covered given that the 1.5 million doses assigned can only reach 750,000 of them. This means that there would need to be some prioritisation of which staff to vaccinate in health facilities.
So aside from the reality that the country doesn’t actually yet have the 80 million doses of vaccine required for 40 million people, there’s been very little planning that’s gone into how these vaccines are going to be deployed. This has become clear over the past four weeks as government has come under attack for not having a plan.
It appears that government put all its eggs in a single basket and decided to only focus on procuring vaccine through COVAX facility, and only started engaging in meaningful bilateral discussions with manufacturers over the past few weeks.
The Department of Health has now set up a task team to look at operational issues. A good place for this team to start would be to run a reality check in order to set more achievable targets and timelines. The team must also begin to broaden its approach to tap the potential of the private sector and civil society to deploy the vaccine.
Reality check
The government envisages three phases of immunisation. The first targets healthcare workers. The second would expand the rollout to essential workers – people involved in managing disasters such as fire fighters – individuals over 60 years and people with co-morbidities who are at particularly higher risk than most. In total 16.5 million people are targeted in this phase.
In the third phase, the general population older than 18 years would be the target – a total of 22.5 million people.
This is easier said than done. Health care workers are relatively easy to reach. But I’m not convinced that the logistics are in place to be able to reach out substantially – even just to individuals over the age of 65 and those with co-morbidities. Without proper planning, vaccines end up being stuck in depots simply because the logistics haven’t been dealt with in terms of how to deploy them.
Even assuming that government procures 80 million doses of vaccine for the 40 million targeted, these are unlikely to become available in substantial quantities until April. And assuming the government started vaccinating people from April 1, 150,000 people would have to get the jab each day, seven days a week, for the first month. And after that, that number would have to climb to 300,000 people each and every day right through to the end of 31st of December 2021 as most vaccines would require a two dose schedule.
No country other than Israel has come close to 150,000 jabs per day, let alone 300,000. Even countries such as the UK and the US have been struggling to vaccinate even up to 50,000 per day.
Furthermore, since none of the COVID-19 vaccines are authorised for use in children under 16 years of age, who make up about 30% of South African population, the target of vaccinating 40 million South Africans would require immunisation of close to 95% of all adults in South Africa. Considering that a recent Ipsos poll of South African adults indicated that only about 53% of adults would be willing to be vaccinated – and it’s unlikely COVID-19 vaccination would be made mandatory – the aspiration of immunising 40 million South Africans by the end of 2021 is unlikely to materialise.
A more realistic target is vaccinating about one third of the population. This is roughly two thirds of the adult population, but not two thirds of the South African population. But even for that to work, there would need to be decentralisation in terms of roles and responsibilities. If the country depends solely on public sector control in the distribution of COVID-19 vaccines, it will fail dismally.
For this reason, it’s critical that the private sector takes a leadership role at the point of delivery. When it comes to the deployment of vaccines, the private sector with general practitioners and numerous number of pharmacies have got much better outreach in terms of being accessible to South Africans, than public health clinics.
The private sector – be it large pharmacies or general practitioners – need to show social solidarity. They should, for example, guarantee that anyone can walk in and be immunised without having to pay. Without this there will be inequity.
What went wrong
The current muddle stems from two mistakes over the past year. The first was government’s decision to pursue – exclusively – vaccine access through the COVAX facility. COVAX was set up to ensure that countries can get enough vaccine for at least 20% of the population. The pricing mechanism built into the equitable access facility meant that bigger economies would pay a premium to subsidise poor economies.
South Africa found itself having to pay $12-$13 per dose as an upper middle income country to participate in the COVAX facility. That is more than three times the cost of procuring the vaccine directly from AstraZeneca (or Serum Institute of India) at the prevailing price of $3 per dose.
Participation in the COVAX facility expresses social solidarity with less resourced countries whose per unit cost is cross-subsidised by wealthier countries and philanthrophic organisations. But the initiative is largely agnostic to the realities of the dire straits of South Africa’s economy.
The second mistake is that government compounded the problem by not timeously engaging in bilateral agreements directly with manufacturers through an advanced market commitment mechanism. Many other countries, including middle income countries, did this as soon as vaccines went into phase two and three trials.
It’s only recently – after the public uproar – that government appears to have been activated to engage in substantive bilateral discussions. The problem is that it’s too little too late. Many of the vaccines, which have been authorised for use in North America and Europe, to be produced over the next 6 months are already earmarked to other countries that made prior commitments.
As a result, South Africa will probably experience another one to two resurgences of COVID-19, before a substantial proportion of the population will have been immunised.
Update on the latest Covid-19 testing and infection of staff and students.
South Africa is in the midst of a second wave of the coronavirus and this is impacting on our University community. We have noted a significant increase in the number of staff and students who have reported testing positive in the last ten days, as reflected in the table below.
Staff and Student COVID-19 Infection Summary
Twenty staff members (including those working from home) and 11 students reported testing positive for COVID-19. The affected staff members and students are self-isolating in line with national directives and University protocols.
Number of infections
8 Jan – 14 Jan 2021
Staff
20
Students
11
The data provided in the table is based on the number of infections reported to the Campus Health and Wellness Centre and the Occupational Health, Safety and Environmental Management Office.
We appeal to you to please do the following:
Complete the screening form on the Wits Logbox App every day. Show your clearance note to the security officers before entering campus.
Wear a face mask that covers your mouth and nose at all times.
Stay at least 1.5 metres from anyone else.
Wash your hands regularly (for at least 20 seconds with soap and water) and dry them properly OR sanitise your hands regularly.
Your overall personal wellness continues to be a priority. If you, or anyone you know is in need of counselling, please make use of the services offered by the University.
Students can reach out to CCDU via info.ccdu@wits.ac.za or call the Wits Student Crisis Line on 0800111331 (24/7 toll free).
Staff members can make use of Kaelo’s counselling services (at no cost to staff) by calling 0861635766, by dialling *134*928, by sending a ‘Please call me’ to 0726205699, or by emailing asknelson@kaelo.co.za.
Our Collective Responsibility
In order to protect our entire community, we appeal to all staff and students, out of mutual respect for one another, and the collective health and safety of our community, to abide by all COVID-19 protocols, rules and policies (and encourage others to do the same). It is up to us to care for one another and to act responsibly, in order to protect ourselves and those in our community who may be more vulnerable.
Covid-19 policy briefs must be realistic: a review by young southern African scientists
- Puleng Segalo, Adeyemi Oladapo Aremu and Pradeep Kumar
African leaders can make strategies to fight COVID-19 more accessible to the people.
Just over a year after the coronavirus was first reported in China countries are still reeling from its effects. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes COVID-19 disease, has infected over 90 million people globally and resulted in more than 1.9 million deaths. In January 2021, South Africa has the highest number of cases on the African continent and has seen a surge in daily infections since December.
The race to find and provide effective vaccines and therapeutics continues. Non-pharmaceutical interventions are still needed to limit the transmission of COVID-19. They include isolating cases, quarantining contacts as well as relevant, accurate and timely risk communication. Hand and respiratory hygiene, infection control and prevention are also vital.
Evidence-based research and interventions are important in the fight against COVID-19. But it is equally important to pay attention to social measures and people’s everyday experiences. These contribute to adherence to government regulations relating to COVID-19. Adherence isn’t always easy or possible in certain circumstances. For example, living conditions may make it difficult to keep a safe distance, and access to water may be limited.
In view of these potential difficulties, a group of young scientists who are part of the Young Academies of Sciences from southern Africa came together to discuss how policy briefs that focus on non-pharmaceutical interventions could be made more accessible for the general public and policy makers alike. The group comprised experts in the behavioural, social, natural, health and human sciences.
In particular, we drew from policy briefs compiled by a public health initiative called Resolve to Save Lives. This initiative puts together data on COVID-19 trends in Africa from multiple sources. These briefs target decision makers involved in the COVID-19 response in Africa, including national task forces and emergency operation centres.
Issues and possible solutions
The briefs are intended to inform public health and social measures in Africa. They are based on social, economic, epidemiological, population movement, and security data from 20 African Union member states. The briefs highlight the various strategies African governments have taken in responding to COVID-19 and whether these are effective or not.
We discussed the briefs in a closed webinar. It aimed to assess whether the briefs take into account the real experiences of people in our communities. The people invited to the webinar included academics, students and representatives of non-governmental organisations.
The webinar highlighted some big issues. These are listed below.
Environmental factors are important in the southern African region’s responses to COVID-19. Most countries in the region did not have a disaster management plan in place, and this contributed to environmental challenges. An example is the disposal of used masks in the streets, with many ending up in rivers and other water bodies. There is, therefore, a need for a disaster management plan which would guide the safe disposal of these waste materials.
There is an overuse of hand sanitisers (for example in shopping malls when people move from one store to the next), which may lead to antimicrobial resistance. Some ways to limit the negative impact of overuse of hand sanitisers on the skin should entail thorough washing of hands with water and soap when available. There should also be extreme caution and avoidance of diluting and combining different sanitisers. A point also highlighted by Winston Morgan, a reader in toxicology and clinical biochemistry at the University of East London, in his assertion that we should “avoid combining pre-prepared products with other ones”.
While government task teams have some diversity and interdisciplinary experts, there is a bias towards the health and “core science” professionals. Psycho-social and political sciences should also be represented in policy decision making processes. The role of traditional leaders, faith groups and businesses must also be taken into consideration. It is important to have this multi-sectoral response as COVID-19 is more than just a health problem.
Governments should strengthen evidence-based risk communication and engage community leaders and trusted people to encourage adherence to public health measures and dispel misinformation. In addition, there needs to be an open and honest conversation between traditional leaders and governments on cultural practices and people’s need to perform rituals.
For example, in many communities, initiation schools are an integral part of community life. Such rituals are an integral part of many communities and people want to practise and observe traditional rites. But these events may be high risk as the initiates might find it difficult to observe COVID-19 safety protocols. Working closely with traditional leaders who have in-depth understanding of such rituals can assist in ensuring adherence.
Looking ahead
It is important to acknowledge that COVID-19 has affected all aspects of people’s lives. The young scientists’ webinar was an opportunity to understand the similarities and differences in challenges associated with COVID-19 in communities across southern Africa.
It highlighted the need for policies that are appropriate for people’s real lives. These need to be “living documents”. This can only happen if communities are consulted in making decisions affecting their lives. Pharmaceutical and non-pharmaceutical interventions have to be adopted alongside one another.
Implications for the (mis)management of Covid-19 in South Africa.
As countries begin to roll out Covid-19 vaccination programmes, principles of global health must be at the fore: equity in access will lead to equity in health for all. There is no place for ‘vaccine nationalism’ – already we have seen that Covid-19 has amplified existing and ever-increasing separatist, nationalistic and xenophobic politics globally.
Emerging from the racist and separationisthistoriesof colonial, tropical and missionary medicine, and in response to the limitations of international health — which focuses on the (poor) health of people and places “elsewhere” — the field of global health aims to achieve “equity in health for all people worldwide”.
While defining global health remainsmessy, we must act upon the central ambition of a collective, global response that focuses on attaining equity in health for all. This is about more than the right to health (which is of course key); it is about recognising basic population health principles whereby promoting and ensuring the good health of every individual benefits us all (conversely, leaving anyone or any population group behind is detrimental to the health of us all).
A true global health response requires the ever-elusive political will needed to address the multiple structural determinants of poor health, including promoting the health and wellbeing of people over profit.
While the aspirations of many of us for a fairer, healthier and more just world feel increasingly out of reach, the Covid-19 pandemic threw down a gauntlet. A global health approach is, by definition, necessary to successfully manage a global health crisis. But, as we have seen time and time again with various public health emergencies (Ebola, Zika, H1N1), necessity is not enough. And it is no different in this context. Rather, Covid-19 has amplified existing and ever-increasingly separatist, nationalistic and xenophobic politics globally.
Fears of the “contagious” migrant body overshadow sensible approaches to the management of Covid-19 in the context of a globalised and mobile world. Not only has vaccine nationalism brought the inequities inherent in global biopolitics — and the power of big pharma — to the fore, it has the potential to be translated at the microlevel, with nation-states holding the power to exclude the “undeserving”, “burdensome” migrant from their vaccination programmes. Vaccine nationalism will not only have results on individual and public health, but it will also amplify other forms of discrimination, including in access to vaccination certificates that will likely become a condition for movement across international borders.
Public health has, historically, involved the management of disease outbreaks, and many public health interventions were designed to prevent and/or restrict the movement of people to stop the spread of disease. While such practices are necessary in various forms and different times for communicable disease control, current moral panics circulating globally — and within South Africa — relating to population movements are increasingly used to support and reinforce global health security agendas, resulting in the use of health as an additional mode for securing national borders.
The prevailing fear and threat of the diseased, foreign body as an unknown outsider whose movements should be restricted in order to exercise sovereignty and “protect” a native population is not new. But these public anxieties about “the contamination of space itself by mobile bodies” have, over time, led to multiple actions to prevent or restrict population movements, with international security and sovereignty debates being inappropriately influenced.
Such approaches echo the ambitions of colonial and tropical medicine which worked to protect the (healthy) coloniser from the (unhealthy) colonised, and falling back on the reductive notion of “international health” which pits the health of “others, elsewhere” against “ours, here”. Such thinking has influenced the restrictions placed by states on people attempting to move from (other, unhealthy) lower-income contexts to (our, healthy) higher-income contexts.
Restricting movement into South Africa from neighbouring countries under the guise of Covid-19 disease control measures risks health for all, fuels xenophobic and anti-foreigner attitudes and fulfils the (unfounded) idea of a dangerous “other” travelling in order to contaminate an innocent “citizen”.
AsFelicia Chang et al write, “Just as open borders are not synonymous with disorderly migration, securitised borders are not synonymous with orderly migration. Walls and hard border controls on movement of people lead to friction between neighbouring states. The harder the borders for the movement of persons, moreover, the greater the risk of injury and death at those places where people may try to pass notwithstanding the heavy controls.”
But there is no question: an effective response to Covid-19 is an equitable one. This isn’t (only) about the right to good health for all; it’s basic public health programming. Failure to ensure access to preventative and treatment interventions — including vaccines — for all, everywhere, undermines any single nation’s sovereign response to Covid-19.
This co-opting of health concerns to justify the securitisation of borders and sovereignty began to emerge at the end of the Cold War, when a renewed approach to what is now framed asGlobal Health Security(GHS) was initiated.Sara Davies and colleaguesdescribe GHS as a framework for “identifying the threat posed by pathogens in a globalised world… as a way of promoting the need for a collective global response”.
Premised, once again, on the recognition that infectious diseases — such as Covid-19 — know no international border, GHS offers an approach for moving beyond nationalism, sovereignty and the reductive notion of “international health” to take necessary, coordinated action to control an unanticipated pandemic. But in an increasingly nationalistic world, GHS can be co-opted to support ever-more restrictive approaches to the management of movement across a nation’s borders.
TheWorld Health Organisation (WHO) cautions against this: “While some countries may still opt for extreme protectionism, importation of diseases is always difficult to prevent. The cross-border impact of infectious diseases is better addressed through multilateral efforts”; a collective, global health response is essential.
In an attempt to guide global health security actions, the WHO developed theInternational Health Regulations, which aim “to prevent, protect against, control and provide a public health response to the international spread of disease in ways that are commensurate with and restricted to public health risks, and which avoid unnecessary interference with international traffic and trade”.
This global health security agenda has, at times, been co-opted by nation-states to strengthen/justify national securitisation agendas, raising concerns about how Covid-19 could provide (further) opportunities for the (mis)application of the important global health security agenda to support and justify an increasingly securitised world. How to respond to this is of concern, particularly in the SADC region, where population mobility and communicable diseases are prevalent, the non-communicable disease burden is increasing and maternal health indicators are poor.
But there is no question: an effective response to Covid-19 is an equitable one. This isn’t (only) about the right to good health for all; it’s basic public health programming. Failure to ensure access to preventative and treatment interventions — including vaccines — for all, everywhere, undermines any single nation’s sovereign response to Covid-19.
As countries begin to roll out Covid-19 vaccination programmes, principles of global health must be at the fore: equity in access will lead to equity in health for all. But how this plays out in a globalised world remains to be seen. Vaccine nationalism is not only about addressing inequities in access to the vaccine globally, it is also about the ways that nation states roll out their Covid-19 vaccination plans. While common public health sense – the central tenet of any successful vaccination strategy – is clear that everyone must be included, will this be the case?
Beyond impacts on individual health and undermining the success of a national vaccination programme, excluding non-citizens promotes the global endeavour to further securitise borders. Given that vaccination certificates are likely to become a requirement for safe and regular international travel, vaccine nationalism may further harm non-citizens by pushing them into unsafe and irregular border crossings.
Ultimately, vaccine nationalism is more than “just” about inequity in health; it offers opportunities for states to further restrict and manage movement across borders.
How vaccine nationalism will finally play out in South Africa remains to be seen. Beyond the immediate concerns associated with vaccine nationalism — accessing vaccinations in the first place — we must caution againstlanguage referring to “citizens” and “South Africans”when developing vaccination strategies.
We must ensure that we refer to all in South Africa when advocating, developing and implementing our vaccine roll-out strategy. Ultimately, there is no place for hypocrisy. We cannot call out the international community on issues of Covid-19 vaccine nationalism if South Africa does not plan for an inclusive national response.
Jo Vearey is director and associate professor at the African Centre for Migration & Society, University of the Witwatersrand. This article was first published in Daily Maverick/Maverick Citizen.
Calling the (behavioural) shots over vaccines
- Leigh Crymble
It will take 67% of the population to be vaccinated to reach herd immunity; here is how those still reluctant can be persuaded to join in.
And so it will soon begin: mass vaccination. Let us fast-forward a few months and assume tens of millions of Covid-19 vaccines have arrived in SA. By this stage, too, we’ve all been allocated our rollout phase based on age, occupation and health status.
The big tasks of adequate supply, appropriate storage and streamlined distribution aside, there is still one piece of the vaccination puzzle that needs to be solved — and quickly. We need to convince the majority of the SA population, about 40-million people, to get it.
Medical experts agree that when about 67% of our population have been vaccinated (most likely through the double-dose option), we will reach herd or population immunity and the virus will be brought under control. While many of us are ready to line up for our shot of freedom, others will take a little more convincing before they roll up their sleeves.
The art of persuasion is something behavioural scientists are very familiar with. A central tenet to behavioural theory is libertarian paternalism; that it is both possible and ethical to guide someone’s behaviour while still respecting their freedom of choice. This is a critical component to our national vaccination rollout strategy. Health minister Zweli Mkhize has stated publicly that no-one will be forced by the government to get the vaccine.
Moving away from mandatory and giving people the freedom to choose is necessary for constitutional rights, but if too many South Africans choose not to have the vaccine, it could end up crippling us.
While figures vary, roughly 40% of South Africans are either undecided or against Covid-19 vaccination. Some have been misled by 5G conspiracy theories and cultural taboos, while others are nervous about the vaccine’s safety due to its record-breaking timeline. While its rapid development was certainly an accomplishment to be celebrated, fake news about vaccines not having gone through the proper testing process has led to widespread concern — not least helped by the semantic choice of the US vaccine development programme, Operation Warp Speed.
Having studied past vaccination efforts (smallpox, polio, influenza, HPV), behavioural experts offer proven insights to nudge people towards more positive vaccine mindsets.
Their first tip? Forget the extreme anti-vaxxers: they’re too far gone to convince otherwise.
Luckily for us, this group makes up a very small population, both in SA and around the world, so their non-compliance, while not ideal, is a negligible factor. Instead, we need to focus our attention on “the movable middle”, the unsure folks split between science and scepticism.
Here are some suggestions to help with this:
Forget just facts, tell stories.Message framing is one of the most important considerations to nudge vaccine adoption, as through storytelling we make experiences more personal and relatable. We now have a unique opportunity to merge that year-old “lives vs livelihoods” debate with the solution to saving both. We must reframe vaccinations as the powerful tool to help us achieve this: an indispensable tool to protect our health at the same time as support the recovery of our economy. Here, the golden thread of community,ubuntu,solidarity and patriotism must be highlighted with tangible reference to people’s lived experiences rather than data-heavy pharmaceutical facts. “Let me tell you why I am getting vaccinated” is a powerful statement to drive uptake.
The Elvis effect.An effective behavioural change campaign relies on three factors: social influence, social norms and vivid examples. As far back as 1956 the world was facing the threat of polio and had the similar challenge we have now of vaccine hesitancy. It was thanks to social-proofing that vaccination uptake increased, with celebrities such as Elvis Presley having his vaccine live on TV. This inspired reluctant American teens to get inoculated, which resulted in the upward trend of vaccination numbers.
Influential endorsements of the Covid-19 vaccine have already begun, with key public figures in the UK and US showing their support. Once rollout begins, social media posts from our front-line health-care workers getting vaccinated will help increase buy-in and build public confidence. This messenger effect is a core component to encouraging vaccine adoption. We are heavily influenced by who communicates to us, so a range of messengers — doctors, government officials, family, friends, influencers, business leaders — across a range of communication channels is important.
The “limited edition” of health-care.Without question we want enough vaccines, and we want them as soon as possible. But we can use the interim shortage to our behavioural benefit. People place more value on what’s in demand and there is huge power in scarcity. Positioning the vaccine as a scarce resource is one way to motivate people to get vaccinated. Once we know more about the rollout plans we can create some sort of waiting list. This becomes a way to get people invested in getting vaccinated and serves as a pre-commitment mechanism whereby people won’t want to lose their place in line — driving more urgency.
Always add fun.Gamification helps make tasks more fun, which drives uptake. Game-based features through digital apps, WhatsApp channels or USSD platforms can serve as both a source of awareness to educate, as well as encourage engagement through built-in quizzes or media. We should develop dynamic, digital vaccine counters that can be displayed across TV, websites and digital billboards. The effect of a count up to reach a target — or even a count down showing how many people are still needed to reach the 40-million mark — will help encourage people to participate. Inter-provincial challenges or company competitions with leader boards are other interactive approaches to both normalise and promote mass vaccination.
Everyone loves an incentive.Linked to the previous point on fun, incentives and memorabilia have their own part to play in vaccine persuasion — but adding incentives needs to be done cautiously. Research has shown that offering financial rewards to vaccine fence-sitters can have an adverse effect: people trust them less. Incentives can be intrinsic (making it easy for people to share online that they got the vaccine for social kudos); or extrinsic (such as automatic Discovery Vitality points for getting the vaccine).
Another idea gaining traction internationally is to gift those who get the vaccine with a branded memento as a piece of Covid-19 history. As an example, a UK-based brewery called BrewDog is offering a special commemorative beer with quirky labels to make them a desired collectable.
Getting the vaccine to SA is just half the battle — we now have to gently push people to take it. In addition to actively fighting vaccine myths, fake news and misinformation, it’s time to work towards changing our national vaccine narrative to encourage mass uptake. Using insights and nudges from the behavioural science toolkit is an effective way to achieve this.
Leigh Crymble is a doctoral student at the University of Witwatersrand specialising in behavioural linguistics. This article was first published in Business Day.
Covid-19 Update 63: Infection summary
- VCO
Update on the latest Covid-19 testing and infection of staff and students.
Fourteen staff members (including those working from home) and six students reported testing positive for COVID-19 during the period 15 to 21 Jan 2021. The affected staff members and students are self-isolating in line with national directives and University protocols.
Number of infections
15 Jan – 21 Jan 2021
Staff
14
Students
6
The data provided in the table is based on the number of infections reported to the Campus Health and Wellness Centre and the Occupational Health, Safety and Environmental Management Office.
SA can take on vaccine nationalism of rich countries
- Wits University
South Africa has the legal tools to challenge the vaccine nationalism of rich countries.
International and national legal frameworks could enable the government to ensure generic Covid-19 vaccines are manufactured locally and in other developing countries, particularly in Africa.
The latter point is important as South Africa, through its chairing of the African Union (AU) and its interventions at the United Nations, has emphasised a solidarity-based approach to the use of vaccines to combat Covid-19. This approach has been sought by UN Secretary-GeneralAntónio GuterresandDr Tedros Adhanom Ghebreyesus, the director-general of the World Health Organisation (WHO).
Vaccine nationalism as a barrier to defeating Covid-19, and non-solidarity
At the outset of the pandemic, the WHO, the UN and leaders of countries across the world called for solidarity and cooperation on measures to stem the spread of the virus. Yet, while committing to work with UN-led initiatives such as the Covid-19 Vaccine Global Access Facility (Covax), ostensibly aimed at equitable and science-led global vaccine distribution, the richer countries undermined such collective processes by practising vaccine nationalism – signing agreements with pharmaceutical companies to supply their own populations in a manner that reduces equitable access for others, often leading to forms of vaccine apartheid between countries. As scientists started work on vaccines these countries bought up vast quantities. Hedging their bets as there was not yet enough evidence for which vaccines would be effective, they ordered most of the stocks of all the leading candidate vaccines, enough to vaccinate all their people a number of times. The result is that 14% of the world’s population bought out 53% of the available vaccines, excluding those produced by Russia and China – while, as indicated byGuterres, nine out of 10 people in poor countries are set to miss out on Covid-19 vaccines in 2021.
This situation has alarmed the UN secretary-general, who said recently vaccine nationalism is a barrier to defeating Covid-19, which can only be done through international cooperation. The WHO has also said that inoculating all the people in some countries while leaving the vast majority of the world’s population without access to the vaccines is not only morally reprehensible, but would do very little to stem the tide of the pandemic.
The health, social and economic challenges of the pandemic will continue unabated. Moreover, the differential pace at which the vaccine is rolled out may create conditions for increased political turmoil between regions and potentially inflame global tensions and instability.
The continued disruption of global supply chains means national economies would continue to suffer and the global economy would continue to stagnate. This would deepen inequalities within and between countries; the latter because some countries are able to access vaccines and treatments and so recover more rapidly than others; the former is due to the fact that the hardest-hit sectors have low wages and the most vulnerable of society have little or no resources to compensate for the cut in income.
The key to ending a pandemic is to inoculate a critical mass of people around the globe, more or less simultaneously in a manner that will effectively break the virus transmission chain. That is, unless the unstated impulse by the rich countries is to block out the rest of the globe’s population from their countries based on their lack of immunity.
Given the history of colonialism, slavery and genocides associated with the richer countries, such Darwinist instincts can, unfortunately, not be discounted. That the rich countries, which purport to champion global governance, acted contrary to and in a manner that undermined UN-led initiatives to create global governance bodies to allocate and distribute the vaccines based on science and ethics, underscores the sentiment in much of the global south that rich countries of the north instrumentalise the institutions of global governance in ways that are only beneficial to them.
The apparent ease with which vaccine nationalism was embraced by the rich countries has perhaps irrevocably damaged initiatives and institutions of global governance that foreground solidarity and global well-being.
Covax
The UN secretary-general and the director-general of the WHO have reiterated calls for more money to be made available for Covax, which sought to break the chain of viral transmissions by pool-buying viable vaccines as they became available and distribute them ethically. There would have been elements of redress with pooled funds from self-financing countries such as South Africa cross-subsidising countries that lack the resources.
The problem is that Covax has supply, governance, transparency and classification limitations. This might have contributed to rich countries not being committed to such an arrangement and instead concluding bilateral deals for most of the vaccine supplies to the extent that only about 20% (maximum) would be available to poorer countries through Covax. This translates to only about 3% of the population benefiting from the facility.
Thus, while South Africa should get what it can from Covax in its current form, it cannot depend on it to meet its vaccination targets for breaking the transmission chain. Rather than allowing big pharmaceutical companies to maximise profits and pressure the government to let go of its “one country, one plan approach” (which seeks to reduce skewed access to vaccines), the government should consider a strategy that puts maximum pressure on those companies using the multilateral system, in conjunction with international and domestic legal measures.
Decisive action towards an equitable vaccine strategy
An equitable vaccine strategy requires monitoring by states, because this pandemic is existential in nature for people and economies and cannot be left, primarily, to the private sector and especially pharmaceutical companies. Wresting control of vaccines from the private sector, particularly the intellectual property regimes of these companies, is critical to meeting global vaccination targets.
International level:
At international level, South Africa should continue, in partnership with India, to push and lobby for a general waiverto the WHO’s Trade-Related Aspects of Intellectual Property Rights (TRIPS) Agreement in relation to Covid-19 drugs, vaccines, diagnostics and other technologies.
South Africa and India seek to suspend rights related to copyrights, industrial designs, patents and undisclosed information (trade secrets) for the duration of the pandemic, “until the majority of the world’s population has developed immunity”, to enable World Trade Organisation (WTO) members to produce and export generics of the vaccines in a way that might meet national and global demand.
This request is being blocked by WTO members that have already ordered the vaccines (such as the US, the EU, the UK, Norway and Canada). They argue that the TRIPS flexibilitiesprovide sufficient access to future vaccines for all people everywhere. In brief, the TRIPS provisions, as amended through the provisions of the Doha Declaration on the TRIPS Agreement and Public Health (Articles 31, 31bisand Annex 1), allow WTO members that cannot afford the original medicine but have the capacity to produce generics for its domestic market through the issuing of compulsory licensing. They also allow members that lack the manufacturing capacity to import medicines from those that produce them cheaply.
Why then a waiver? While these measures can and should be exploited, without a general waiver countries would need to initiate individual action to obtain compulsory licences. These processes are cumbersome and time consuming – which the people and economies of these countries can ill afford (particularly given the slow rollout of vaccines to developing countries).
Some licences require negotiations with right holders, and uncertainties exist around who determines what an adequate remuneration is (required according to Article 31(h) of the TRIPS Agreement).Despite South Africa having provisions for compulsory licensing, in more than a century of patent legislation no compulsory licence has been granted for pharmaceutical-related products.Moreover, some compulsory licences are only for public, non-commercial use, while the process does notapply to trade secret know-how and cell lines needed to copy vaccines and biologic medicines.
Importantly,some members, such as the US and the UK, where companies are working on the development of a vaccine, have not ratified the TRIPS amendment that allowsimports from countries that produce under a compulsory licence. Attempts to bypass patent rules on several Covid-19 related medical technologies have already faced implementation barriers.
Hence the importance of the South African and Indian initiative around a general waiver for the duration of the pandemic. Notably, the waiver would not, as regularly argued, prevent innovation considering that there are210 vaccines in the (pre-)clinical phase, nor would it prevent pharmaceutical companies from recouping research and development costs.
According to Labonte and Baker, governments have entered into $24-billion worth of advance-purchase agreements, which are expected to generate a 60% to 80% profit margin, not to speak of the $2-billion in public funding.A waiver would not change the fact that developing countries’ health-system capacities are underfunded or limited, but would create an environment for a more rapid solution to sharing manufacturing capacities and technical production knowledge that newer health technologies require, and allow export to countries in need, irrespective of the origin of the vaccine.
In the absence of consensus, which the WHO prefers, the adoption of the waiver requires a three-quarter majority – the support of 123 members. More than 100 developing countries, numerous NGOs, several UN agencies, the WHO and broader civil society support the waiver already. Thus, South Africa should continue to lobby and set a deadline for the General Council to decide on the issue.
Failure by the TRIPS Council to adopt the waiver could trigger action by the South African government to produce and import the vaccines, using compulsory licences enabled by domestic legislation; potentially even invoking article 73 of the TRIPS Agreement (security exceptions). In contrast, a waiver could stipulate specific conditions that make allowance for some of the pharmaceutical companies’ interests.
National level:
South African patent lawdoes provide for compulsory licensing and “state use” in an emergency. Section 4 of the Patents Act allows for “government use” of patents in cases of national emergency, subject to negotiations with patent owners, irrespective of the scale of the emergency.
Sections 55 and 56 provide for compulsory licences and, similarly, require a judicial process before the Commissioner of Patents. This involves time and costs associated with litigation.
Further, the Medicines and Related Substances Control Amendment Act and Section 57 of the Patents Act allow for parallel importation in general and would thus permit the import of generics produced under a compulsory licence in other countries, irrespective of South Africa’s manufacturing capabilities. This is inconsistent with the TRIPS provisions which only permit such export to least-developed countries and those without manufacturing capacity.
The Patents Amendment Bill, guided by the provisions of the government’s Intellectual Property Rights Policy, would allow for compulsory licensing without judicial processes, invoking “state use” and negotiations with patent holders. These amendments would accelerate the process of issuing a compulsory licence and should be tabled in Parliament as soon as possible. The passing of these amendments would also signal to the pharmaceutical companies and the WTO negotiators that all South African stakeholders, including all political parties and not only the government, are serious about ensuring equitable access to life-saving medication to all its people and people in the region.
Other than the patents legislation that may allow the government to immediately implement measures to produce and import generics, arguably, sections 7, 11 and 27 of the Constitution contain a positive obligation to fulfil the right to life and the right to access healthcare. In relation to Covid-19, and considering vaccine nationalism, the most obvious “necessary” measure to fulfil this obligation is for the government to issue a compulsory licence or import vaccines, enabled by the patent laws.
Big pharmaceutical companies that may pressure the government to let go of its “one country, one plan” approach can be referred to the government’s duty to consider international options when fulfilling its peoples’ rights (section 39(1)(b)).
The International Covenant on Economic Social and Cultural Rights (ratified by South Africa) provides that access to the right to health and therefore, medicine, should be realised without distinction on the grounds of race, colour, sex language, religion, political or other opinion, national or social origin, property, disability or other status; and the International Convention on the Elimination of all Forms of Racial Discrimination (ICERD) (ratified by South Africa) provides for states to prohibit and eliminate racial discrimination in the enjoyment of public health and medical care.
The manner in which vaccine nationalism is shaping the rollout of vaccines arguably contravenes these international law provisions. Given the transboundary nature of the pandemic, it would not be far-fetched to argue for an extraterritorial state obligation to effect measures to remedy this.
Using existing legal tools to access vaccines
Experience in the global HIV/Aids struggle for affordable antiretrovirals suggests that when drug companies are threatened with state-use licensing or compulsory licences, they will consider voluntary licensing to avoid compulsory licences. The Netherlands recently threatened Roche over its technology in a testing kit. The drug company complied and shared the technology. To advance solidarity on the continent, these licences should rely on African and Global South manufacturers, where possible.
South Africa has the legal tools to challenge the exclusionary vaccine strategy of rich countries and pharmaceutical companies. It should use these measures nationally and mobilise bias around them in the international arena, to urgently get the rich countries and the pharmaceutical companies around the table to agree on a UN/WHO-led global Covid-19 vaccine strategy that is controlled by members.
The impact of this pandemic is the premier global emergency and has peace and security implications given its potential to degrade economies and undermine stability within states. The situation is too urgent and precarious to be left to the dictates of pharmaceutical companies and their drive for profits, and the narrow nationalist impulses of a few rich countries.
The national and global situation is such that patent rights should be secondary to patient rights. In this pandemic, all people in all parts of the world are patients, through the impact the pandemic has on health, lives and livelihoods. The vaccines should be first considered public health goods and then private goods, and their manufacture and distribution should be managed within that context.DM
Zane Dangor is Special Adviser to the Minister of International Relations and Cooperation and chairs the Institute for Economic Justice on a voluntary basis. He holds an LLM in International Law.
Franziska Sucker is Associate Professor, School of Law, University of the Witwatersrand.First State Exam in Law, Second State Exam in Law, LLM, PhD.
Novavax Covid-19 vaccine the first to demonstrate clinical efficacy against South African variant
- Wits University
Clinical efficacy demonstrated in Phase 2b South Africa trial.
Wits-VIDA is the lead institution in the Novavax Covid-19 vaccine trial in South Africa, which today announced results of the SA phase 2b and the UK phase 3 trials.
Clinical efficacy demonstrated in Phase 2b South Africa trial with over 90% of sequenced cases attributable to prevalent South Africa escape variant
Strong efficacy in Phase 3 UK trial with over 50% of cases attributable to the now-predominant UK variant and the remainder attributable to Covid-19 virus
The Novavax vaccine, known as NVX-CoV2373, is the first vaccine to demonstrate not only high clinical efficacy against the prototype SARS-CoV-2, but also significant clinical efficacy against both the rapidly emerging South African (501Y.V2 variant) and UK mutant (N501Y) variants.
In the South Africa Phase 2b clinical trial, 60% efficacy for the prevention of mild, moderate and severe Covid-19 disease was observed in the 94% of the study population that was HIV negative. The trial also achieved its primary efficacy endpoint in the overall trial population, including HIV positive and HIV negative subjects, showing efficacy of 49.4%.
“The higher efficacy of the vaccine in the UK than in South Africa is because the variants circulating in SA are less sensitive to vaccine induced immune responses. Nevertheless, the 60% reduced risk against Covid-19 illness in vaccinated individuals in South Africans underscores the value of this vaccine to prevent illness from the highly worrisome variant currently circulating in South Africa, and which is spreading globally. This is the only COVID-19 vaccine for which we now have objective evidence that it protects against the variant dominating in South Africa,” says Professor Shabir Madhi, Executive Director of the Vaccines and Infectious Diseases Analytics Research Unit (VIDA) at Wits, and principal investigator in the Novavax Covid-19 vaccine trial in South Africa.“The public health value of vaccines extends beyond a simple point estimate. The ability of Covid-19 vaccines to impact the pandemic will depend on the product, its efficacy, and how quickly we can scale up coverage of the vaccine eventually.”
About the South African Novavax Covid-19 vaccine phase 2b trial results
In the South Africa Phase 2b clinical trial, 60% efficacy (95% CI: 19.9 – 80.1) for the prevention of mild, moderate and severe Covid-19 disease was observed in the 94% of the study population that was HIV-negative. Twenty-nine cases were observed in the placebo group and 15 in the vaccine group. One severe case occurred in the placebo group and all other cases were mild or moderate. The clinical trial also achieved its primary efficacy endpoint in the overall trial population, including HIV-positive and HIV-negative subjects (efficacy of 49.4%; 95% CI: 6.1 – 72.8).
This study enrolled over 4,400 patients beginning in August 2020, with Covid-19 cases counted from September through mid-January. During this time, the triple mutant variant, which contains three critical mutations in the receptor binding domain (RBD) and multiple mutations outside the RBD, was widely circulating in South Africa. Preliminary sequencing data is available for 27 of 44 Covid-19 events; of these, 92.6% (25 out of 27 cases) were the South Africa escape variant.
Importantly in this trial, approximately 1/3 of the patients enrolled (but not included in the primary analyses described above) were seropositive, demonstrating prior COVID-19 infection at baseline. Based on temporal epidemiology data in the region, the pre-trial infections are thought to have been caused by the original COVID-19 strain (i.e., non-variant), while the subsequent infections during the study were largely variant virus. These data suggest that prior infection with COVID-19 may not completely protect against subsequent infection by the South Africa escape variant, however, vaccination with NVX-CoV2373 provided significant protection.
“The 60% reduced risk against Covid-19 illness in vaccinated individuals in South Africans underscores the value of this vaccine to prevent illness from the highly worrisome variant currently circulating in South Africa, and which is spreading globally. This is the first Covid-19 vaccine for which we now have objective evidence that it protects against the variant dominating in South Africa,” says Professor Shabir Maddi, Executive Director of the Vaccines and Infectious Diseases Analytics Research Unit (VIDA) at Wits, and principal investigator in the Novavax Covid-19 vaccine trial in South Africa. “I am encouraged to see that Novavax plans to immediately begin clinical development on a vaccine specifically targeted to the variant, which together with the current vaccine is likely to form the cornerstone of the fight against Covid-19.”
Novavax initiated development of new constructs against the emerging strains in early January and expects to select ideal candidates for a booster and/or combination bivalent vaccine for the new strains in the coming days. The company plans to initiate clinical testing of these new vaccines in the second quarter of this year.
“A primary benefit of our adjuvanted platform is that it uses a very small amount of antigen, enabling the rapid creation and large-scale production of combination vaccine candidates that could potentially address multiple circulating strains of COVID-19,” said Gregory M. Glenn, M.D., President of Research and Development, Novavax. “Combined with the safety profile that has been observed in our studies to-date with our COVID-19 vaccine, as well as prior studies in influenza, we are optimistic about our ability to rapidly adapt to evolving conditions.”
The Coalition for Epidemic Preparedness Innovations (CEPI) funded the manufacturing of doses of NVX-CoV2373 for this Phase 2b clinical trial, which was supported in part by a $15 million grant from the Bill & Melinda Gates Foundation.
About the UK Novavax Covid-19 vaccine phase 3 trial results
The study enrolled more than 15,000 participants between 18-84 years of age, including 27% over the age of 65. The primary endpoint of the UK Phase 3 clinical trial is based on the first occurrence of PCR-confirmed symptomatic (mild, moderate or severe) Covid-19 with onset at least 7 days after the second study vaccination in serologically negative (to SARS-CoV-2) adult participants at baseline.
The first interim analysis is based on 62 cases, of which 56 cases of Covid-19 were observed in the placebo group versus 6 cases observed in the NVX-CoV2373 group, resulting in a point estimate of vaccine efficacy of 89.3% (95% CI: 75.2 – 95.4). Of the 62 cases, 61 were mild or moderate, and 1 was severe (in placebo group).
Preliminary analysis indicates that the UK variant strain that was increasingly prevalent was detected in over 50% of the PCR-confirmed symptomatic cases (32 UK variant, 24 non-variant, 6 unknown). Based on PCR performed on strains from 56 of the 62 cases, efficacy by strain was calculated to be 95.6% against the original Covid-19 strain and 85.6% against the UK variant strain [post hoc].
The interim analysis included a preliminary review of the safety database, which showed that severe, serious, and medically attended adverse events occurred at low levels and were balanced between vaccine and placebo groups.
About the Novavax vaccine known as NVX-CoV2373
NVX-CoV2373 is a protein-based vaccine candidate engineered from the genetic sequence of SARS-CoV-2, the virus that causes COVID-19 disease. NVX-CoV2373 was created using Novavax’ recombinant nanoparticle technology to generate antigen derived from the coronavirus spike (S) protein and is adjuvanted with Novavax’ patented saponin-based Matrix-M™ to enhance the immune response and stimulate high levels of neutralizing antibodies. NVX-CoV2373 contains purified protein antigen and can neither replicate, nor can it cause COVID-19. Over 37,000 participants have participated to date across four different clinical studies in five countries. NVX-CoV2373 is currently being evaluated in two pivotal Phase 3 trials: a trial in the U.K that completed enrollment in November and the PREVENT-19 trial in the U.S. and Mexico that began in December.
Covid 19 Update 64 - Return to campus
- VCO
Update on the return to campus of staff members.
Thank you to all those staff members who made it possible for Wits to complete the 2020 academic year and who ensured that the University remained operational. Your contribution and commitment is recognised and appreciated.
It will now require our collective effort to prepare for the 2021 academic year and to fulfil our mandate to deliver academic, research and service excellence.
To this end, all University entities are required to be fully operational as from 1 February 2021.
Professional and administrative staff are required to return to campus as from Monday, 1 February 2021. Members of the Senior Executive members (SET) have been authorised to determine and approve the level of staff required in their respective faculties and divisions, in order to ensure that offices and services are fully operational. Line managers are required to act in accordance with the SET’s directives in this regard.
Academics are required to be accessible for academic and research purposes.
The following exceptions apply:
Employees with co-morbidities (such as active or on treatment for cancer, diabetes, asthma or other respiratory illnesses) should voluntarily declare these ailments to their line manager or provide a valid doctor’s letter that indicates specifically why they cannot report for work. Where line managers believe that it is necessary, a second opinion may be obtained from selected healthcare practitioners based at the Wits Donald Gordon Medical Centre, as described in the HR Practice Note on this matter (available on the HR page on the Intranet). These staff members should work productively from home.
Staff members over the age of 60 who may be at risk should be enabled to work from home as per the University’s HR Practice Note on this matter. Employees over the age of 60 who do not have co-morbidities, and who are healthy, may of their own volition return to the workplace at their own risk.
Staff members who work in open plan offices or under other conditions which may be high-risk, may work on a rotational basis as determined by their line managers, with the approval of their SET member. Work in open plan spaces becomes a risk for Covid-19 infection when the relevant protocols aimed at the prevention of infection are not adequately adhered to by employees.
Workplace Safety
The health and safety of every member of the Wits community is paramount, and again, it will require our collective effort to keep everyone safe.
Staff members are required to:
Complete the self-screening form via the Wits LogBox Screening App every day before entering campus;
Wear a mask over your mouth and nose at all times;
Practise physical distancing (stay a minimum of 1.5 meters from anyone else);
Refrain from gathering in closed spaces that are not adequately ventilated (no gatherings should be allowed in tearooms and canteens);
Sanitise regularly, or wash your hands with soap and water for 20 seconds and dry them properly; and
Abide by all Wits’ COVID-19 policies and protocols.
Responsibilities for Line Managers
Line managers must complete or update a risk assessment for their respective entity and must implement the risk mitigation measures before staff members return to the workplace.
Line managers must work with their assigned Human Resources and Health and Safety Officers, the Services Department, and any other University entity to ensure that the following measures are in place:
the physical distancing of staff members in the workplace;
the adequate provision of sanitisers and/or soap and water;
the regular cleaning of venues and work spaces;
the provision of personal protective equipment for specialised areas (and ensuring that it is correctly worn);
the completion of the daily symptom screening form on the Wits LogBox Screening App; and
the adherence to Wits’ protocols to prevent the spread of infection.
Reporting infections
Managers are requested to report all Covid-19 infections immediately. Staff infections should be reported to the Occupational Health, Safety and Environmental Management Directorate via Dept-OHS-Admin@wits.ac.za and student infections should be reported to Anna.Moloi@wits.ac.za.
Conclusion
Let us take the necessary precautions to ensure our own personal safety and that of our colleagues, students and friends, as we return to campus. Please chat to your line manager or relevant executive should you have any further queries about the return to campus plans.
Results from Novavax vaccine trials in the UK and South Africa differ: why, and does it matter?
- Shabir A. Madhi
The Novavax vaccine is the first that provides objective scientific evidence that it can protect people against the variant virus circulating in South Africa.
To fast track the response to the COVID-19 pandemic, a broad range of candidate COVID-19 vaccines are being investigated. The results of clinical trials being run on some of them have started to be released. The Novavax vaccine trial is one of them. Phase 3 trial results from the UK and phase 2b results from South Africa were recently announced. Shabir Madhi was the lead researcher in the South African leg of the trial. The Conversation Africa’s Ina Skosana asked him to provide context.
Novavax vaccine trials run in South Africa and the UK indicate that its efficacy in the UK was 89% at least seven days after individuals had received two doses of vaccine.
In South Africa, the vaccine efficacy was 60% in people living without HIV. A small group of individuals living with HIV – about 150 – was included in the efficacy analysis. However, the study didn’t have the statistical power to evaluate for vaccine efficacy specifically in this population.
Why the major difference in risk between the UK’s 89% and South Africa’s 60%?
We’ve got two different studies that have evaluated the same vaccine. But they’ve evaluated them under very different conditions.
Firstly, conditions in South Africa and the UK are different in terms of the socio-economic environment, which could influence the force of infection by SARS-CoV-2.
Over and above that, the trials evaluated vaccine efficacy against two very different variants, which would differ in their susceptibility to antibodies induced by vaccination (as well as by natural infection from past infection by prototype SARS-CoV-2).
The South African efficacy readout is against the B.1.351 variant – 92% of all of the cases in the main analysis developed COVID-19 following infection by this variant.
The UK trial involved people infected with the B.1.1.7 and other variants.
The variants originating in the UK and the one in South Africa share a common mutation (N501Y) that has been associated with increased transmissibility of the virus. However, the variant found in South Africa has an additional three or four mutations involving immunodominant components of the spike protein that could interfere with the vaccine induced neutralising activity of the virus.
How is the Novavax vaccine different from others that have reported data on their efficacy?
Firstly, it’s a different vaccine based on a more novel technology. It’s a protein based vaccine. It involves the spike protein of the virus itself, which is produced and formulated as a nanoparticle type structure. Once injected, it stimulates the immune system to start producing antibody and also induces T-cell immune responses.
This is different to messenger RNA based vaccines. These aren’t delivering the actual protein, but delivering the blueprint coding for the spike protein.
It’s important to understand that it wouldn’t be scientifically robust to do any head-to-head comparisons between the study that was done in South Africa and studies for the messenger RNA vaccines, as well as the AstraZeneca vaccine, where there was a pooled analysis of data from the UK as well as in Brazil. The same thing goes for the Sputnik V vaccine.
Efficacy of 95% was reported for the two messenger RNA based vaccines from Moderna and Pfizer. For the AstraZeneca vaccine, an average of about 70% efficacy in the pooled analysis from the UK and Brazil was reported. For the Sputnik V vaccine, it was around 85%.
Notably, however, none of these studies were done in settings similar to South Africa. And most importantly, the vaccine efficacy in those studies was evaluated against the prototype virus, which did not have the mutations evident in the B.1.351 variant against which the vaccine efficacy of the Novavax study was evaluated in South Africa.
What makes the Novavax vaccine stand out?
It’s the first vaccine that provides objective scientific evidence that it can protect people against the B.1.351 variant circulating in South Africa. This is true even though the vaccine efficacy is only 60% against all severe COVID-19 illness, with the majority of cases being mild to moderate.
The 60% efficacy reported for the Novavax vaccine needs to be benchmarked against the World Health Organisation and other regulatory authorities criteria, that any COVID-19 vaccine with at least 50% efficacy and which protects for at least six months would be considered to be useful from a public health perspective.
Unfortunately, the vaccine is only likely to become available in April or May. The government needs to engage with the relevant stakeholders to secure supplies earlier given the threat of the new variant.
Why was it important for South Africa to participate in this trial?
I believe the data we’ve released speaks to why it was important to be active in getting vaccine studies done in South Africa. Without them we would simply be clueless whether vaccines work in South Africa.
The first reason is that we’ve got different populations as well as different social and economic conditions. It was important to be able to evaluate vaccines within a context of high density of population and overcrowding. The types of infections that take place under those scenarios are very different from those taking place in high-income countries.
And then there are the health factors and differences in terms of prevalence of comorbidities. These include HIV, obesity and hypertension.
All these types of factors could influence the efficacy readout of the vaccines.
It took a lot of convincing both for Novavax as well as for AstraZeneca vaccine for their sponsors to eventually agree to bring studies to South Africa. And the studies were largely led directly by us in South Africa. We also had to convince funders to support the studies in South Africa. The Novavax study, for example, is co-funded by the Bill and Melinda Gates Foundation and Novavax. The AstraZeneca vaccine study is sponsored by the University of Oxford, but funded by the South African Medical Research Council and the Bill & Melinda Gates Foundation.
This is just to emphasise that companies were not rushing to Africa to get their COVID-19 vaccines evaluated on the continent. On the contrary, there seems to be little incentive for them to do their studies here, as it’s not seen as a market that will provide a return on their investments. Unless we are proactive in ensuring that studies are done in Africa, we will continue lagging behind in knowledge on how vaccines work in our own context. We are being compromised by not having more clinical trials done in Africa, especially for diseases which disproportionately affect Africans.
Has South Africa secured access to the vaccine because of its involvement in a trial?
The involvement in a clinical trial and the ability of a country to procure vaccines are completely different processes. The role players involved in these processes differ within a company as well as within a country.
As an investigator, my responsibility is to provide the scientific evidence as to whether the vaccine works or not. It would be a conflict of interest if, as an investigator, I started engaging with companies, even before the vaccine trials are done, to make a case, or at least to negotiate on behalf of the country, that South Africa should get vaccine if the vaccine studies are shown to be working.
This would be construed as an undue incentive on my part, and could lend itself to the potential for manipulating study results to come up with a favourable answer.
The data that’s been forthcoming from South Africa certainly should put it in a favourable position to engage with Novavax. But that type of engagement should have started when the vaccine trial started, rather than after the results were released.
I’m uncertain whether the South African government has as yet engaged with Novavax, which is a small biotech company in the US. However, Novavax has partnered with the Serum Institute of India to produce the Novavax vaccine. It would be important for the government to engage with the Serum Institute of India on accessing this effective vaccine.
The Wits Vaccines and Infectious Diseases Analytics (VIDA) Research Unit, which runs the Oxford Covid-19 vaccine trial in South Africa, has announced results.
In an analysis, submitted as a pre-print prior to peer-review publication, a two-dose regimen of the ChAdOx1 nCoV-19 vaccine provides minimal protection against mild-moderate COVID-19 infection from the B.1.351 coronavirus variant first identified in South Africa in mid-November 2020.
Efficacy against severe COVID-19 infection from this variant was not assessed. The analyses being submitted in the pre-print show the vaccine had high efficacy against the original coronavirus non-B.1.351 variants in South Africa.
Researchers from South Africa and the UK found that viral neutralisation by sera induced by the ChAdOx1 nCoV-19 coronavirus vaccine against the B.1.351 coronavirus variant were substantially reduced when compared with the ‘original’ strain of the coronavirus.
These early data, which will be submitted for scientific peer-review, appear to confirm the theoretical observation that mutations in the virus seen in South Africa will allow ongoing transmission of the virus in vaccinated populations, as has been recently reported in those with prior infection.
In this study of approximately 2,000 volunteers where the median age was 31 years old, mild disease was defined as at least one symptom of COVID-19. Protection against moderate-severe disease, hospitalisation or death could not be assessed in this study as the target population were at low risk.
Work is already underway at the University of Oxford and in conjunction with partners to produce a 2nd generation of the vaccine which has been adapted to target variants of the coronavirus with mutations similar to B.1.351, if it should prove necessary to do so.
Shabir Madhi, Professor of Vaccinology and Director of the Vaccines & Infectious Diseases Analytics (VIDA) Research Unit at University of the Witwatersrand, and Chief Investigator on the trial in South Africa, said:
'Recent data from a study in South Africa sponsored by Janssen which assessed moderate to severe disease, rather than mild disease, using a similar viral vector, indicated that protection against these important disease endpoints was preserved. This could be relevant to the ChAdOx1 nCoV-19 vaccine, which has been developed using similar technology as the Janssen vaccine, and for which vaccine induced immune responses are also similar.
‘These findings also force us to recalibrate thinking about how to approach the pandemic virus and shift the focus from the aspirational goal of herd immunity against transmission to the protection of all at risk individuals in population against severe disease.’
Andrew Pollard, Professor of Paediatric Infection and Immunity, and Chief Investigator on the Oxford vaccine trial, said:
‘This study confirms that the pandemic coronavirus will find ways to continue to spread in vaccinated populations, as expected, but, taken with the promising results from other studies in South Africa, such as those using a similar viral vector, vaccines may continue to ease the toll on health care systems by preventing severe disease.’
Sarah Gilbert, Professor of Vaccinology at the University of Oxford said:
‘Efforts are underway to develop a new generation of vaccines that will allow protection to be redirected to emerging variants as booster jabs, if it turns out that it is necessary to do so.’
‘We are working with AstraZeneca to optimise the pipeline required for a strain change should one become necessary. This is the same issue that is faced by all of the vaccine developers, and we will continue to monitor the emergence of new variants that arise in readiness for a future strain change.’
Note: these findings are early preliminary data, which have been submitted for peer review and will appear as a pre-print in the days ahead.
About the Wits Vaccines & Infectious Diseases Analytics (VIDA) Research Unit
Formerly known as the Respiratory and Meningeal Pathogens Research Unit (RMPRU) and founded in 1995, the Vaccines and Infectious Diseases Analytics (VIDA) Research Unit of the University of the Witwatersrand (Wits) is an internationally recognised, African-led research unit in the field of epidemiology of vaccine preventable diseases, and clinical development of life-saving vaccines.
Under the guidance of Professor Shabir Madhi, a global leader in the field of paediatric infectious diseases and the Dean of the Faculty of Health Sciences at Wits University, Wits VIDA is conducting translational research on vaccine preventable diseases and training the next generation of clinician scientists. Combining clinical, microbiological and epidemiological expertise in an African setting, Wits VIDA’s cutting-edge scientific research informs local and global policy recommendations on the use of next-generation and novel vaccines today. In addition to various other studies on COVID-19, Wits VIDA championed and led the first two COVID-19 vaccine trials in Africa in 2020, for the Oxford and Novavax vaccine candidates.
Oxford Covid-19 vaccine shows sustained protection of 76% during 3-month interval until second dose
- Wits University
Researchers at the University of Oxford have today published in Preprints with The Lancet an analysis of further data from the ongoing trials of the vaccine.
The Vaccines and Infectious Diseases Analytics Research Unit (VIDA) at Wits University runs the South African Oxford Covid-19 vaccine trial. Professor Shabir Madhi, Executive Director of Wits VIDA and Dean of the Faculty of Health Sciences at the University, leads these trials and he is a co-author in the Preprints.
In releasing the data regarding sustained protection of 76% during the 3-month interval until the second dose, scientists at Oxford reveal that the vaccine efficacy is higher at longer prime-boost intervals, and that a single dose of the vaccine is 76% effective from 22- to up to 90-days post vaccination. The analyses reveal:
Single standard dose efficacy from day 22 to day 90 post vaccination of 76% with protection not falling in this three-month period
After the second dose vaccine efficacy from two standard doses is 82.4% with the 3-month interval being used in the UK. (82.4% effective, with a 95% confidence interval of 62.7% - 91.7% at 12+ weeks)
Data supports the 4-12 week prime-boost dosing interval recommended by many global regulators
Analyses of PCR positive swabs in UK population suggests vaccine may have substantial effect on transmission of the virus with 67% reduction in positive swabs among those vaccinated
In this preprint, which is currently under review at The Lancet, they report on an analysis of additional data to include information from the trial up to the 7th December 2020, which includes a further 201 cases of primary symptomatic COVID-19 (332 cases from 131 reported in previously), they report that the effect of dosing interval on efficacy is pronounced, with vaccine efficacy rising from 54.9% with an interval of less than six weeks to 82.4% when spaced 12 or more weeks apart.
They also detail that a single standard dose of the vaccine is 76% effective at protecting from primary symptomatic COVID-19 for the first 90 days post vaccination, once the immune system has built this protection 22 days after the vaccination, with the protection showing little evidence of waning in this period.
Professor Andrew Pollard, Chief Investigator of the Oxford Vaccine Trial, and co-author of the paper, says, "These new data provide an important verification of the interim data that was used by more than 25 regulators including the MHRA and EMA to grant the vaccine emergency use authorisation. It also supports the policy recommendation made by the Joint Committee on Vaccination and Immunisation (JCVI) for a 12-week prime-boost interval, as they look for the optimal approach to roll out, and reassures us that people are protected from 22 days after a single dose of the vaccine."
The exploratory analyses presented in this preprint paper suggest that it is the dosing interval and not the dosing level which has a great impact on the efficacy of the vaccine. This is in line with previous research supporting greater efficacy with longer prime-boost intervals done with other vaccines such as influenza, Ebola and malaria.
The authors also report further on the potential for the vaccine to reduce transmission of the virus, based on swabs obtained from volunteers in the UK arms of the trial with a 67% reduction after the first dose of the vaccine.
They also hope to report data regarding the new variants in the coming days, and expect the findings to be broadly similar to those already reported by fellow vaccine developers.
About the Oxford COVID-19 vaccine
ChAdOx1 nCoV-19, now known as AZD1222 co-invented by the University of Oxford and its spin-out company, Vaccitech, is being trialled by the University’s Jenner Institute and Oxford Vaccine Group. The team started working to develop a vaccine against coronavirus in January 2020.
Developed at the Jenner Institute, the recombinant adenovirus vector ChAdOx1 nCoV-19 uses a viral vector based on a weakened version of the common cold virus (adenovirus) containing the genetic material of SARS-CoV-2 spike protein. After vaccination, the surface spike protein is produced, which primes the immune system to attack COVID-19 if it later infects the body.
Over 50,000 people to date have taken part in clinical trials of The ChAdOx1 nCoV-19 vaccine sponsored by the University of Oxford and AstraZeneca, and many more have received the vaccine through public vaccination programmes following emergency use licensure. It has been shown to be safe and well tolerated, although it can cause temporary side effects, such as a temperature, flu-like symptoms, headache or sore arm.
The potential vaccine entered Phase III clinical trials in May to study safety and efficacy in healthy volunteers. In total, nearly 24,000 volunteers have joined the University of Oxford sponsored trial, in sites around the UK (approximately 12,000 volunteers), Brazil (approximately 10,000 volunteers) and South Africa (approximately 2,000 volunteers). Interim efficacy and safety data were published in The Lancet in December, including an extensive safety database of over 74,000 ‘person months’ of safety data follow-up.
Our partners, AstraZeneca, have committed to delivering billions of doses of its COVID-19 vaccine across the globe in a broad, equitable, and timely way at no profit during the pandemic. This includes an agreement with the European Commission to supply up to 400 million doses, starting in early 2021 following the regulatory approval from the European Medicines Agency, with tens of millions of doses due to be supplied in February and March.
Not for profit information
As part of the agreement between University of Oxford and AstraZeneca, the vaccine will be supplied on a not-for-profit basis for the duration of the pandemic and in perpetuity for low- and middle-income countries, with any future royalties received by the University of Oxford being re-invested in the medical sciences.
Funding
This trial is funded by the National Institute for Health Research, UK Research and Innovation, the Bill & Melinda Gates Foundation, the Lemann Foundation, and the South African Medical Research Council. We are grateful to the NIHR infrastructure provided through the NIHR Biomedical Research Centres and the NIHR Clinical Research Network at the UK study sites.
Reasons to be optimistic about sub-Saharan higher education after Covid-19
- Himdat Bayusuf, Imed Hammouda, Zeblon Z Vilakazi, Chelsey R Canavan and Wafaie W Fawzi
Tertiary education often carries societal benefits that far outweigh the initial investments necessary to establish a strong and productive system.
Highly skilled workers are needed to address complex challenges in public health, agriculture, climate, technology and engineering, among other fields.
Higher education in sub-Saharan African countries has expanded greatly over the past several decades, but the majority of the population remains unable to access the limited number of higher institutions of learning, with large inequities in access between and within countries.
Between 1970 and 2013, enrolment in tertiary education in sub-Saharan Africa increasedat a rapid annual rate of 4.3%, compared to the global average of 2.8%. The number of students in these institutionsincreased from5.9 million in 2010 to 8.3 million in 2019.
Despite such growth, the gross tertiary enrolment ratio in sub-Saharan Africa wasstill the lowest in the world in 2018, at 9.4% compared to 38% globally.
The primary challenge to expanding access relates to a lack of opportunity: supply of tertiary education has failed to keep pace with demand. Vast improvements in primary and secondary educational attainment have led to greater numbers of students seeking further educational opportunities.
According to theUnited Nations Population Division, the number of youth in Africa aged 10-24 years is projected to reach 700 million by 2050, while estimates from theWorld Banknote that the proportion of youth who have completed at least one cycle of secondary education is projected to increase from 42% in 2012 to 59% in 2030.
Virtual learning opportunities and challenges
The pandemic has only exacerbated poor and inequitable access to higher education. Virtual education was necessary as part of lockdown measures in various countries to curb the spread of the virus.
Yet, a survey among students and researchers conducted by theMawazo Institutein May 2020 found that only 38.5% of respondents were based at institutions offering e-learning opportunities, with higher rates in East and Southern Africa compared to the West. The same survey found that 72.5% of respondents reported interruptions in research activities.
Universities in Africa have been working on virtual learning prior to COVID-19 in an effort to bring down costs and expand access to education. COVID-19 accelerated that need as institutions were forced to go digital, raising major concerns around equitable access to electricity and technology.
Routine disruptions in power supply, evident even prior to the pandemic, create a multitude of challenges for promoting virtual education. Outages mean that online courses cannot be offered consistently at set times. Furthermore, internet connectivity in most sub-Saharan African settings is slow and unreliable.
UNESCOreports that 89% of students in sub-Saharan Africa do not have access to household computers and 82% lack access to the internet.
To grapple with these challenges during COVID-19, schools have broadcast lessons on radio and television and in some cases instructors have tried to connect with students via text messaging platforms such as WhatsApp. In South Africa, several universities partnered with the telecommunication and logistics sectors to distribute free computers and ensure network access for students at home.
In addition to issues of connectivity, universities were forced to figure out in short order how to create engaging digital content, project- and team-based activities and learning assessments in a virtual environment. Creating effective digital content typically takes several weeks to several months, yet in 2020, some universities were forced to transition to virtual learning in a matter of days.
The transition to digital online education has been a regulatory challenge for many universities. For instance, current regulations in Tunisia forbid online assessment and place limitations on online course delivery.
Inequitable access to higher education and virtual learning for certain students, such as those from low-income and-or rural households and women, is a major challenge in many countries in Africa. Presently, those from wealthier households and those in urban areas have greater access to higher education and earn proportionally higher wages throughout their careers.
And while women make up approximately43% of sub-Saharan Africa’s tertiary students, the Mawazo Institute’s May 2020 report showed greater disruptions in coursework and research among women due to COVID-19.
Universities with greater resources and with experience in online learning were better equipped when the pandemic hit. At the privateSouth Mediterranean Universityin Tunisia, the pandemic accelerated processes that were already underway to transition more content to virtual learning platforms.
Moving forward, ACE Impact, through the Association of African Universities, will facilitate further learning on the establishment of digital education in African universities.
To ensure virtual learning is effective, greater support is needed for investments in online platforms, faculty training and development of digital content. Strengthening of existing platforms that span countries is also imperative, for example, the African Union’sPan African Virtual and E-University, which was established in 2019 as the online arm of the Pan African University.
Higher education’s role in the COVID-19 response
Higher education institutions in Africa have played a triple role in the COVID-19 response.
First, they have been actively working to ensure the safety and well-being of school communities. While much emphasis has been placed on virtual learning, the reality for most students in sub-Saharan Africa is that in-person studies remain the only real option for continued learning.
Frequent on-campus COVID-19 testing has been a key strategy enabling colleges and universities across the globe, particularly in the United States and other high-income settings, to remain safely open.
Laboratory capacity is a key barrier to greater testing capacity at many institutions in Africa. Some institutions in the African region have significantly reduced the number of students allowed on campus at one time while also instituting health guidelines such as social distancing, handwashing and quarantine practices. Given their standing in communities, universities have an opportunity to set strong examples for others with their own response strategies.
Second, institutions of higher learning often have large medical centres, with the ability to provide care for severely ill patients. Medical and public health students have also been called upon to assist campuses with mass testing and support communities with contact tracing.
Some engineering colleges have provided important contributions, such as production of personal protective equipment, 3D-printed face shields, hand sanitisers and solar-powered handwashing stations.
Finally, universities have ramped up research, education and advocacy efforts to assist governments in controlling the virus. For example, theCentre of Excellence in Mathematics and Informaticsat Gaston Berger University in Senegal built mathematical models to track the spread of the pandemic.
TheUniversity of the Witwatersrandin Johannesburg, South Africa, re-purposed its labs to help develop personal protective equipment for health workers, developed statistical modelling programmes to inform decision-making, contributed to vaccine trials and developed a digital app for COVID-19 symptom and exposure screening that was made available to other universities.
Of notable mention is theAfrican Center of Excellence for Genomics of Infectious Diseasesat Redeemer’s University in Nigeria, which, in addition to being the first to sequence the COVID-19 virus in Africa, has also developed a new vaccine candidate that has gone through a successful preclinical trial and is now at the human trial stage.
The University of Ghana Health Services and Noguchi Memorial Institute for Medical Research formed aJoint Emergency Response Teamto provide education and awareness on preventive measures and diagnosis of COVID-19.
And Makerere University in Uganda developed adedicated websiteto provide a trusted source for accurate and timely information about the disease.
The way forward
Greater investments are needed for a higher education sector that can respond to workforce demands, including the type of trained professionals who can respond to outbreaks and prevent future pandemics.
A positive externality of COVID-19 is the potential increased interest among future tertiary students in the sciences. Education reform to expand access should include investments in blended online learning, tuition assistance programmes for in-person and virtual education and programmes to increase gender and ethnic diversity among students, faculty and staff.
Importantly, investments in tertiary education are needed to produce highly skilled graduates today who will be tomorrow’s leaders. Researchers and scientists are in high demand to address Africa’s development challenges, including diseases like tuberculosis, malaria and respiratory infections. The higher education sector in sub-Saharan Africa has demonstrated that it is capable of making large-scale changes in a short period of time with laudable results.
The current transition to virtual learning presents a prime opportunity to intentionally design systems to reduce social inequalities. It is a social justice imperative that higher education systems serve to reduce social inequities, including expanding opportunity to women, low-income and rural populations and minority groups.
As we continue to respond to the urgent needs posed by the pandemic and look toward a post COVID-19 world, there is reason to be optimistic about the future of higher education in sub-Saharan Africa.
Himdat Bayusuf is an education global practice specialist for the West and Central Africa Region at the World Bank; Imed Hammouda is from the Mediterranean Institute of Technology, Tunis, Tunisia; Zeblon Z Vilakazi is from the University of the Witwatersrand, Johannesburg, South Africa; Chelsey R Canavan is from the department of global health and population, Harvard TH Chan School of Public Health, USA; and Wafaie W Fawzi is based at the Harvard University Center for African Studies, USA.
Wits staff members share their Covid-19 experiences and quest to survive.
Disbelief, shock and agony were recurring emotions when some Wits staff members tested positive for the novel coronavirus.
A year ago, the first case of Covid-19 was reported in South Africa and weeks later, the President announced a national lockdown as the number of infections began to surge. For many, this was their interaction with the virus was limited to broadcast media and social media platforms. However, the virus started to infiltrate communities coming closer to home.
“I used to follow the daily statistics and at that time, it was distant from me. It was only when I contracted it in May last year that I felt its existence,” says Horatio Williams, a Covid-19 survivor from Wits ICT. “Before you contract the virus, you do not think much about it.”
Sifiso Vilakazi, from the same Department echoes the same sentiments, stating that before he contracted the virus, he ridiculed it and dismissed its existence.
Covid-19 scare and fears
Although Williams was asymptomatic and learnt of his Covid-19 status through a medical procedure he had to undergo, the virus affected him psychologically as he asked himself endless questions and was worried whether he had transmitted it to his colleagues and family.
“I kept asking myself where and how I got the virus. Did I infect anyone? Why did I get infected when I had been so careful?”
Another staff member, Faye Khan from Marketing baffled with the same questions. As a person with a comorbidity, she says she had been extra careful as she is considered high risk.
“None of my family members contracted the virus, I had not been in contact with anyone known to have tested positive and I was staying at home most of the time.” Not knowing where she may have contracted Covid-19 was distressing for Khan and fuelled fear in her life.
“I am diabetic. So when I got my results, I looked at the SMS and thought, ‘this is the end of me’,” she says. At the time she tested positive, Khan had just lost her twin sister and as such, her fear of death intensified. This worsened when she found herself hospitalised when her symptoms became severe.
Tackling symptoms: Road to recovery
Experts have described Covid-19 symptoms being similar to those of the normal flu and these can vary from mild to severe symptoms where hospitalisation is required as was the case with Khan when she experienced high fever and breathing difficulties.
Anna Veileroglou from the Function and Events team, tested positive in December. Her symptoms were mild, she says but she felt weak and her body was in pain. “At some point I said I am going to text my family and say goodbye.” The prescribed medication assisted with her symptoms and helped her regain strength. Taking time to rest also contributed to her recovery she says.
Tebogo Sibilinga, a paramedic from the Campus Health and Wellness Centre says he had a high fever and chills. During his recovery period, he took everything that could aid his health. This included eating immune boosting vegetables raw, to get the full benefits of their medicinal properties.
ICT’s Vilakazi who considers himself fit and healthy with no comorbidities says his initial symptoms were mild and resembled those of a normal flu. Consequently, he was not too worried and thought these would disappear with over the counter medications. However, they exacerbated instead. He shares how his symptoms went from mild to severe within a few days while on holiday with his family in KwaZulu-Natal in January.
“I started coughing but thought I was acclimatising to the new environment. On the third day of our holiday, I started losing my sense of smell and taste. I did not want to spoil the holiday and decided to ride it out,” he says.
Vilakazi was forced to cut the holiday short when his fever rocketed and began coughing blood. Upon his return, he headed to the doctor and was prescribed antibiotics while recovering from home but his health deteriorated rapidly. “Hardly two hours when we got home, everything turned haywire. Suddenly I could not breathe. I could not even call my wife to help me. I had to send her a WhatsApp to take me back to the doctor and I was immediately admitted into hospital,” he says.
“The scariest thing is not being able to breathe and gasping for air. When you try to breathe through your mouth or nose and nothing comes through it is scary and you literally feel like you are dying when that attack starts and you panic.” After spending more than a week in hospital, his condition improved and could now breathe on his own without a ventilator.
Positivity for a positive outcome
While in hospital, trying to recover and regain his strength, Vilakazi took a hard knock when he witnessed his wife, who had also tested positive being wheeled into hospital. This experience motivated him to recover and to remain optimistic.
“At that moment I realised I needed to fight more. I started thinking positively. I saw myself out in my garden playing with my kids,” he says.
Khan stresses the importance of a positive mind set while fighting Covid-19. “People must remain positive and have faith.
Sibilinga says contracting the virus comes with a lot of pressure and family support is crucial during recovery. He states that a healthy mind set is important because the virus can affect you psychologically. Sibilinga is currently taking care of his mother who is battling Covid-19 and seeing her sick has affected him. He says people need to heal mentally as well from their Covid-19 trauma.
“People must go for counselling if they can. It does not help to be recovered (physically),” says Sibilinga.
Living beyond Covid-19
While Covid-19 has had some negative implications and brought about unprecedented changes in society, it has inspired a changed in behaviour for many. For Williams, the pandemic enacted a sense of self-awareness.
“I pondered a lot when I tested positive, but I am glad that I had Covid-19 because some good came out of it. Covid-19 helped me to re-evaluate my life and to appreciate my family and friends more,” he says.
Although he has recovered, he says the storm is not yet over and he is extra cautious now. “I do not want to relax. I have told myself that I am not going to be the person who is going to test this thing,” he quips. He wants to continue complying to protect those around him. “Besides keeping our family safe, we have an obligation to keep each other safe.”
Post his recovery journey, Sibilinga has adopted a healthier diet as part of his lifestyle and in a quest to boost his immune system. His health has become his greatest asset, does not take it for granted. Having lost his uncle to Covid-19, he implores others to do the same.
“Covid-19 has showed me that life is short. If you have dreams, stop postponing them and pursue them. People need to comply with the regulations.” We need to protect ourselves because it does not mean that if you recovered you cannot be re-infected again.”
Veileroglou, who recently lost her father to Covid-19 says although she is still dealing with the pain of her loss, she feels motivated and is mentally ready to tackle the world.
Wits University through the independent services of Kaelo Lifestyle offers free counselling support for all staff members. The services are provided in all South African languages 24/7 days a week. Staff may call 0861 635 766 OR dial *134*928 OR Send a ‘Please call Me’ to 072 620 5699 OR emailasknelson@kaelo.co.za for assistance.
Not using AstraZeneca vaccine goes against the spirit of what the Health Department espoused
- Shabir A Madhi
Every additional day of procrastination lends itself to much of the R75m used to procure the vaccine going to waste.
The past month has been a roller-coaster ride when it comes to the rollout of Covid-19 vaccines in SA. The government has halted the distribution inside SA of one million doses of the AstraZeneca vaccine and is poised to make a potentially historic mistake.
After much criticism early in January 2021 of the virtual absence of any strategy beyond procuring a limited quantity of Covid-19 vaccines through the Covax facility, the government successfully negotiated procurement of 1.5-million doses of the AstraZeneca Covid-19 vaccine through a bilateral agreement with Serum Institute of India.
This was, however, at a price ($5.25) more than double what EU countries ($2.5) had negotiated to pay for the same vaccine (but from a European manufacturer). Within a week surrounding the fanfare of the arrival of one million doses of the AstraZeneca vaccine at a cost of R75m came the disappointing news from a study evaluating this vaccine in SA since June 2020 that the vaccine does not protect against mainly mild (usually limited to infection of the upper airways) Covid-19.
The telltale signs that the AstraZeneca (and probably all other) Covid-19 vaccines might be less efficacious in protecting against mild-moderate Covid-19 in SA was evident from reports that have emerged since mid-January 2021, from local scientists, which indicated that the ability of antibody induced by natural infection by the ancestry SARS-CoV-2 variant had greatly diminished activity against the B. 1.351 variant that emerged in SA late in October 2020.
This was a consequence of gene mutations that affected key epitopes of the spike-protein of the virus, which are the components of the protein that most of the current first generation Covid-19 vaccines induce functional antibody against. Consequently, it was expected that even antibody induced by the first-generation Covid-19 vaccines would have diminished activity against the B. 1.351 variant which had undergone substantive changes in key components of target of these vaccines.
Corroborating this were interim results from another study, also conducted in SA, on the Novavax Covid-19 vaccine which drew much less publicity than the results of the AstraZeneca vaccine study, despite it being the only vaccine then to show protection against the B. 1351 variant.
Notably in the Novavax study, the attack rate of mild-moderate Covid-19 (probably mainly due to the B. 1351) variant did not differ in the unvaccinated control group between those who had already been infected with the SARS-CoV-2 prototype virus compared to uninfected individuals at the time of study-enrolment.
This provided the first conclusive evidence that the mutations included in the B. 1.351 were clinically significant, and that despite 35-45% of South Africans (especially in densely populated urban areas) likely to have been infected during the course of the first wave by the prototype virus, such infection did not confer any protection against developing mild to moderate Covid-19 due to the B. 1351 variant.
The rude awakening of these results (for some) was that the notion of relying on “herd immunity” evolving by allowing people to be unabatedly naturally infected was doomed not to materialise. Instead, the high force of infection that occurred in SA (despite attempts at restrictive and economically devastating lockdowns) probably contributed to the problem of the evolution of a variant that was now resistant to antibody induced by past infection.
Furthermore, the Novavax vaccine results from the South African study showed lower efficacy (49%-60%) against mainly mild-moderate Covid-19 mainly due to the B. 1.351 variant compared with results of the same vaccine in the UK (89% efficacy), where the efficacy was not affected by another variant (B.1.1.7) circulating there.
In studies on other Covid-19 vaccines, including the mRNA vaccines of Biontech/Pfizer and Moderna, for which vaccine efficacy has been reported to be 95% against Covid-19 due to the ancestry virus, laboratory investigations have reported 6.5-8.5 fold reduction in the potency of the antibody induced by those vaccine against the B. 1351 variant relative to that observed for the prototype virus.
For the Johnson and Johnson (J&J) vaccine, which uses a similar technology for design of vaccine as the AstraZeneca vaccine and also induces almost identical functional antibody response after a single and two-dose schedule, the laboratory testing of the antibody activity against the B. 1351 variant have not yet been released. I expect they will be no different to that observed for the AstraZeneca vaccine.
In contrast to the lack of efficacy of the AstraZeneca vaccine againstmild-moderate Covid-19 in SA, the J&J Covid-19 vaccine results from the South African arm of the study reported a 89% reduced risk ofsevereCovid-19, also mainly due to the B. 1.351.
Unlike the AstraZeneca vaccine trial in SA, which targeted a younger age-group demographic with low prevalence of co-morbidities, a high proportion of participants in the J&J study were individuals at high risk of severe disease — that is, older than 60 and with high prevalence of co-morbidities such as diabetes and hypertension.
Hence, any direct comparison of the efficacy of these two vaccines is misguided and fundamentally flawed. Whether the J&J vaccine indeed protects against the same spectrum of mild illness that is caused by the B. 1.351 variant is yet to be reported or established for any such head-to-head comparison between these two vaccines (or other Covid-19 vaccines) to be meaningful.
So why might there be a difference in how well Covid-19 vaccines work against mild illness compared to severe disease. First, this would not be unique to Covid-19 vaccines. Vaccine against other respiratory pathogens, including seasonal influenza virus, respiratory syncytial virus in infants born to vaccinated women, and pneumococcus consistently report that protection against mild illness (usually of the upper airways) is more challenging to accomplish than prevention of severe disease (usually lower airway disease — pneumonia for example).
The reasons for this may differ between vaccines, including possibly requiring lower concentrations of antibody to protect against severe than mild illness. In addition for Covid-19, challenge studies in vaccinated non-human primates indicate that protection against lower airway infection can be conferred largely independent of vaccine induced antibody, through the stimulation of natural killer cells (also referred to as part of T-cell immunity).
Fortunately, there is a broader repertoire of spike-protein peptides that induce T-cell immunity, most of which are unaffected by even the B. 1.351 spike protein mutations. For the AstraZeneca vaccine, almost none of the B. 1351 mutations are likely to compromise the killer cell responses induced by the vaccine.
Consequently, there remains a strong biologically plausible reason to expect the AstraZeneca vaccine will protect against severe disease due to the B. 1351 variant, likely to a similar magnitude as the J&J vaccine.
It is largely premised on this, that the World Health Organization in mid-February 2021 recommended that the AstraZeneca vaccine still be rolled out even in countries where the B. 1.351 variant or other similar variants of concern are circulating.
The AstraZeneca vaccine, as well as many other first-generation Covid-19 vaccines, are unlikely to bring about interruption in transmission of SARS-CoV-2 or protect against mild infection where these variants of concern such as the B. 1351 variant are circulating.
This would be compounded if there is sluggish rollout of the vaccine which is drawn out over a year, rather than within a few months. Nevertheless, these first-generation Covid-19 vaccines even in settings such as SA still provide the only sustainable option of preventing flooding of our hospitals with severe Covid-19 cases and mitigate Covid-19 deaths once the next resurgence is upon us.
Hence, the decision by SA not to deploy the vaccine goes against the spirit of what was previously espoused by the department of health — that it would take its lead from WHO recommendations.
Furthermore, this decision inadvertently leads itself to choosing between leaving high-risk individuals largely unprotected against being hospitalised and dying of Covid-19, as opposed to rolling out the available AstraZeneca vaccine to those who choose to take the chance of deriving potential protection by being immunised with a safe vaccine that has been established to reduce the risk of severe Covid-19 by 80% even among people older than 80 years in the UK.
The decision by SA would have less repercussion if high-risk individuals were likely to be vaccinated with other Covid-19 vaccines for which clinical (and not only extrapolation of laboratory-based data) protection is established against the B. 1351 variant before the next resurgence.
Unfortunately, based on the latest sharing of information on the pipeline of Covid-19 vaccines likely to become available to SA, other Covid-19 vaccines, all besides the J&J vaccine which will not have been evaluated clinically against the B. 1351 variant, are only likely to become available from mid-April onward, without any clear indication on what quantities and how soon these may be deployed into the arms of people.
Consequently, the current strategy to try to offload the AstraZeneca vaccine to other African countries where the variant might not have been identified (mostly due to there being little sequencing to actually identify its presence rather than its actual absence) is problematic. This is compounded by the current expiry date of the vaccine being April 30 2021.
Even were there to be reversal of the decision by government to take its chances with the AstraZeneca vaccine and target it to high-risk individuals who choose to take their chances of being vaccinated rather than remaining unprotected when the resurgence is upon us, getting a million people vaccinated before the end of April would be a mission.
Every additional day of procrastination lends itself to much of the R75m used to procure the vaccine going to waste, while the elderly and other high-risk individuals would certainly remain unprotected as opposed to being offered a fighting chance of being protected against Covid-19 severe disease and death.
Professor Shabir Madhi is the Dean of the Faculty of Health Sciences at the University of the Witwatersrand and Director of the SA Medical Research Council Vaccines and Infectious Diseases Analytics Research Unit.
Declaration of interests: National principal investigator of the University of Oxford (AstraZeneca vaccine) and Novavax Covid-19 vaccine trials. The AstraZeneca vaccine study was funded by BMGF and SAMRC, and the Novavax vaccine trail; by BMGF and Novavax. All funding for these studies goes to the Wits Health Consortium of the University of the Witwatersrand.
Novavax Covid-19 vaccine trial results in SA and UK confirm high levels of efficacy
- Wits University
Results of the Novavax Covid-19 vaccine trial in SA and UK have confirmed high levels of efficacy against the original and variant Covid-19.
The results show 100% protection against severe disease in both the SA and the UK trials.
Results announced today also showed efficacy against variants circulating in SA and the UK.
An updated analysis of the Novavax vaccine trial in South Africa shows vaccine efficacy of 55.4% against mainly mild Covid-19 among HIV-negative trial participants, in a country where the vast majority of strains are B.1.351 escape variants.
In addition, protection against severe disease due to the B.1.351 variant dominating in South Africa was 100%, with all Covid-19 hospitalization and deaths having occurred in the placebo group.
Professor Shabir Madhi, Executive Director of the Wits Vaccines and Infectious Diseases Analytics (VIDA) Research Unit, leads the Novavax Covid-19 vaccine trial in South Africa.
“The results from the South African trial reinforce that, even with the evolution of the SARS-CoV-2 virus developing mutations in an attempt to evade immune responses induced following natural infection by ancestry virus, the first generation of Covid-19 vaccines still offer great potential especially in mitigating severe disease and death from Covid-19.
This was evident in South Africa where all the cases of Covid-19 hospitalization and death occurred in the unvaccinated control group. This despite the effectiveness of the first generation Covid-19 vaccines being variably affected in reducing the risk of mild Covid-19 caused by the B.1.351 variant, due to the variant being relatively resistant to the antibody induced by all Covid-19 vaccines.”
In a separate study of the Novavax Covid-19 vaccine in the UK, efficacy was 96.4% against the original virus strain and 86.3% against the B.1.1.7/501Y.V1 variant circulating in the U.K (post hoc).
These updated final analyses build on the successful interim results announced in January 2021, adding substantially more Covid-19 cases and statistical power in both studies.
In both the SA and UK trials, these analyses showed that the vaccine is well-tolerated, with low levels of severe, serious and medically attended adverse events at day 35, balanced between vaccine and placebo groups.
“We are very encouraged by the data showing that NVX-CoV2373 not only provided complete protection against the most severe forms of disease, but also dramatically reduced mild and moderate disease across both trials. Importantly, both studies confirmed efficacy against the variant strains,” said Stanley C. Erck, President and Chief Executive Officer, Novavax.
About the South African Novavax Covid-19 vaccine trial
The South Africa trial was a randomized, observer-blinded, placebo-controlled Phase 2b clinical trial.
One cohort evaluated efficacy, safety and immunogenicity in approximately 2 665 healthy adults.
The second cohort evaluated safety and immunogenicity in approximately 240 medically stable, HIV- positive adults.
A complete analysis of vaccine efficacy among 147 PCR-positive cases (51 cases in the vaccine group and 96 in the placebo group) demonstrated an overall efficacy of 48.6% with majority of illness being mild or moderate.
The vast majority of cases during the efficacy analysis were due to the B.1.351/501Y.V2 variant circulating in South Africa. All five cases of severe disease observed in the trial occurred in the placebo group. Among HIV-negative participants, 55.4% efficacy was observed.
The complete analysis shows that vaccine-induced protection began 14 days after dose 1, although increased efficacy was observed seven days after dose 2, the primary endpoint for the study.
A previously reported initial analysis from the study through 60 days indicated that prior infection with the original Covid-19 strain might not completely protect against subsequent infection by the variant predominantly circulating in South Africa.
However, the complete analysis of the South Africa trial indicates that there may be a late protective effect of prior exposure with the original Covid-19 strain. In placebo recipients, at 90 days the illness rate was 7.9% in baseline seronegative individuals, with a rate of 4.4% in baseline seropositive participants.
Madhi says: “As a benefit to the study volunteers, without whose selfless contribution this important study would not have been possible, we now plan to offer all of them the Novavax vaccine so they can be protected immediately against mild – and more importantly – severe Covid-19 being caused by the B.1.351 variant.”
South African Oxford AstraZeneca Covid-19 vaccine study a global game-changer
- Wits University
Findings of the SA study in the Oxford AstraZeneca Covid-19 vaccine trial have been published in the New England Journal of Medicine (NEJM).
The NEJM, which published the study on 16 March 2021 following peer review, is the leading medical journal globally.
This is a landmark study in so far as being the first to raise the alarm that, despite early successes with Covid-19 vaccines, further research is warranted on a next generation of Covid-19 vaccines.
The results from this study, however, only indicate that the AstraZeneca vaccine does not have at least 60% efficacy against mild-moderate Covid-19 due to the B.1.351 (N501Y.V2) variant.
Based on a broader body of evidence, the World Health Organization recommends that this vaccine still be deployed in countries where the B.1.351 variant circulates, as it likely still protects against severe infection, hospitalisation, and death caused by Covid-19.
Professor Shabir Madhi, Executive Director of the Vaccines and Infectious Diseases Analytics (VIDA) Research Unit at the University of the Witwatersrand, Johannesburg, led the trial in South Africa:
“Despite the disappointing finding that the AstraZeneca vaccine did not protect against mild Covid infection because of the B.1.351 variant first identified in South Africa, peer review and publication of our research validates the findings and makes a compelling case for the development of a second-generation vaccines worldwide,” says Madhi.
First-generation vaccines refer to those designed to respond to the original SARS-CoV-2 virus. Second-generation vaccines refer to technology and design innovations that can provide protections against the constantly evolving variants that cause Covid-19 disease.
A rapid response to variant reality
The findings of this study were previously publicised as a preprint on Sunday, 7 February 2021, and concluded that the ChAdOx1 nCoV-19 vaccine provided minimal protection against mild to moderate Covid-19 infection from the B.1.351 coronavirus variant first identified in South Africa in mid-November 2020.
Prior to the evolution of the B.1.351 and P.1 variants, the South African National Department of Health (NDOH) had ordered and taken delivery of approximately one million doses of the Oxford AstraZeneca vaccine on 1 February 2021, after a published pooled analysis of this vaccine in December 2020 showed an overall vaccine efficacy of 66.7% in the UK and Brazil.
“We were in a state of euphoria about the high efficacy of several Covid-19 vaccines against the original virus, but then the AstraZeneca study threw us a curve-ball,” says Madhi. “In this study now published in NEJM, we found that two doses of ChAdOx1 nCoV19 had no efficacy against non-hospitalized mild to moderate Covid-19, mainly due to the B.1.351 variant.”
What the SA study published in NEJM reveals
The randomised, multi-centre, double-blinded trial enrolled 2026 participants between 24 June and 9 November 2020.
The trial was a phase 1b/11 trial that aimed to evaluate the safety, immunogenicity, and efficacy of the AstraZeneca vaccine ChAdOx1 nCoV19 in preventing symptomatic Covid-19. Immunogenicity refers to the ability of a foreign substance, such as an antigen, to provoke an immune response. Vaccine efficacy refers to the percentage reduction of a disease in a clinical trial.
“A trial enrolling just 2026 participants is considered small, while phase 3 trials enroll tens of thousands of participants,” says Madhi. “Yet the startling data that our small trial generated was irrefutable, and the implications profound.”
Profile of a South African AstraZenca Covid-19 vaccine trial participant
The majority of participants enrolled were relatively young (under 65-years-old), generally healthy, and HIV-negative. The median [middle] age of participants was 30 years old. More than half (56.5%) of the trial participants identified as male, 70.5% were Black Africans, 12.8% were white, and 14.9% identified as ‘mixed’ race.
“These demographics are important because they reflect characteristics of the overall population in South Africa. Conducting clinical trials in diverse settings like these is critical to understanding how vaccines work in local contexts,” says Madhi.
Testing a hypothesis
The primary ojective of this trial was to establish this vaccine’s efficacy against all-severity Covid-19, irrespective of variants.
A secondary objective was to evaluate the vaccine’s efficacy against the B.1.351 variant specifically.
“When this trial began in June 2020, we were testing a vaccine against SARS-COV-2,” says Madhi. “By January 2021, SARS-CoV-2 had spawned variants, including the B.1.351 first discovered in South Africa. As a secondary objective, we tested a hypothesis: would this vaccine prove at least 60% efficacious in preventing mild to moderate Covid-19 disease? It did not.”
The results showed that a two-dose regimen of ChAdOx1-nCov19 did not show protection against mild to moderate Covid-19 due to the B.1.351 variant.
Crucially, Madhi notes that, “This vaccine may still help protect high-risk individuals with co-morbidities from contracting severe Covid-19 disease, having to be hospitalised, mechanically ventilated, or dying. The AstraZeneca vaccine remains essential in the arsenal against this virus, particularly in Africa, which has already received 14 million doses of this vaccine as the Covid-19 immunization programme starts in multiple countries.”
How the WHO took note
On 15 February 2021, the WHO recommended that the AstraZeneca vaccine still be rolled out, even in countries where the B.1.351 variant or other similar variants of concern are circulating.
A WHO news release says that the vaccine was reviewed on 8 February by the WHO Strategic Advisory Group of Experts on Immunization (SAGE), which makes recommendations for vaccines’ use in populations (i.e. recommended age groups, intervals between shots, advice for specific groups such as pregnant and lactating women). The SAGE recommended the vaccine for all age groups 18 years and above.
“While the AstraZeneca vaccine – like many other first-generation Covid-19 vaccines – is unlikely to interrupt transmission of SARS-CoV-2 or protect against mild infection from variants like B.1.351, these first-generation vaccines could still provide the only sustainable option to prevent flooding our hospitals with severe Covid-19 cases, and to mitigate Covid-19 deaths once the third wave hits,” says Madhi.
Second-generation vaccine innovation
The development of an Oxford AstraZeneca and other Covid-19 vaccines targeting the B.1351 variant is currently underway.
The South African study increased awareness worldwide of the necessity of developing vaccines that target variants specifically – and even reimagining vaccines entirely.
Innovations in vaccine technologies, platforms and designs suggest exciting advances in this field.
“The finding of our [Oxford AstraZeneca Covid-19 vaccine] study are truly a turning point in Covid vaccine development – and a rude awakening,” says Madhi. “This one small South African study has alerted the world to the fact that second generation Covid-19 vaccines will be required to provide protection against inevitable and persistent SARS-COV-2 variants. If we had not conducted this trial in South Africa, the world would be none the wiser.”
Novavax Covid-19 vaccine trial results show efficacy against the B.1.351 variant in SA study
- Wits University
Results from the initial primary analysis of the Novavax Covid-19 vaccine trial conducted by Wits VIDA in SA have been published.
The New England Journal of Medicine (NEJM) today published findings of the Phase 2b clinical trial conducted in South Africa.
NEJM is recognised as the world’s leading medical journal.
Shabir Madhi, Professor of Vaccinology, co-author of the study, and the Director of the Vaccines & Infectious Diseases Analytics Research Unit (Wits VIDA), led the Novavax Covid-19 vaccine trial in South Africa.
The published data provide additional detail of an initial analysis conducted in January, while more robust data from a complete analysis of the study was subsequently shared in March 2021.
Publication of initial primary analysis highlights cross-protection by the Novavax Covid-19 vaccine against the B.1.351 variant prevalent in South Africa during the study.
This is the first published study to show protection against mild Covid-19 caused by the B.1.351 variant circulating in South Africa.
An updated analysis of the study indicated 100% protection against severe Covid-19 due to the B.1.351 variant.
“An efficacy of 50% is sufficient to meet the World Health Organization criteria for regulatory approval of the vaccine,” says Madhi.
The Novavax Covid-19 vaccine, known as NVX-CoV2373, is made by Novavax, Inc., a US-based biotechnology company developing next-generation vaccines for serious infectious diseases.
Gregory M. Glenn, M.D., President of Research and Development, Novavax, says: “This data publication reinforces the encouraging safety profile and cross-protective effect across variants seen in studies of our vaccine to-date.”
About the study
The Phase 2b randomised, observer-blinded, placebo-controlled trial conducted in South Africa evaluated efficacy, safety and immunogenicity in healthy adults, and in a small cohort of medically stable adults living with human immunodeficiency virus (HIV).
The study met its primary endpoint – i.e., the Novavax vaccine demonstrated an overall efficacy of 49% in the initial analysis (published in NEJM), and 49% in the subsequent complete analysis (unpublished).
Among healthy adults without HIV, the Novavax vaccine demonstrated efficacy of 60% in the initial analysis, and 55% in the subsequent complete analysis.
In the initial analysis, cases were predominantly mild-to-moderate and due to the B.1.351 variant that dominates in South Africa, and increasingly in southern Africa.
In the subsequent complete analysis, circulation of the B.1.351 variant continued to dominate, and all five cases of severe disease observed in the trial occurred in the placebo group.
The initial analysis, now being published in NEJM, suggested that prior infection with the original Covid-19 strain did not protect against subsequent infection by the variant predominantly circulating in South Africa through 60 days of follow-up.
However, with additional follow-up, the complete analysis of the South Africa trial indicates that there may be a modest protective effect of prior exposure with the original Covid-19 strain.
Among placebo recipients, at 90 days of follow-up, the illness rate was 8.0% in baseline seronegative participants and 5.9% in baseline seropositive participants.
“The data make a compelling case for use of the Novavax Covid-19 vaccine in settings where the B.1.351 variant dominates – which is most of southern Africa – to reduce the risk of mild disease and also to maximise the opportunity for protection against severe Covid,” says Madhi. “Further work is required for Novavax and all other Covid-19 vaccines, particularly in people living with HIV.”
In addition to directing Wits VIDA, Madhi is Dean of the Faculty of Health Sciences at the University of the Witwatersrand, Johannesburg (Wits), and co-Director of African Leadership in Vaccinology Expertise (ALIVE).
About the Wits Vaccines & Infectious Diseases Analytics (VIDA) Research Unit
Formerly known as the Respiratory and Meningeal Pathogens Research Unit (RMPRU) and founded in 1995, the Vaccines and Infectious Diseases Analytics (VIDA) Research Unit of the University of the Witwatersrand (Wits) is an internationally recognised, African-led research unit in the field of epidemiology of vaccine preventable diseases, and clinical development of life-saving vaccines.
Under the guidance of Professor Shabir Madhi, a global leader in the field of paediatric infectious diseases and the Dean of the Faculty of Health Sciences at Wits University, Wits VIDA is conducting translational research on vaccine preventable diseases and training the next generation of clinician scientists.
Combining clinical, microbiological and epidemiological expertise in an African setting, Wits VIDA’s cutting-edge scientific research informs local and global policy recommendations on the use of next-generation and novel vaccines today.
In addition to various other studies on Covid-19, Wits VIDA championed and led the first two Covid-19 vaccine trials in Africa in 2020, for the Oxford and Novavax vaccine candidates.
About the Novavax vaccine known as NVX-CoV2373
NVX-CoV2373 is a protein-based vaccine candidate engineered from the genetic sequence of the first strain of SARS-CoV-2, the virus that causes Covid-19 disease.
NVX-CoV2373 was created using Novavax' recombinant nanoparticle technology to generate antigen derived from the coronavirus spike (S) protein and is with Novavax' patented saponin-based Matrix-M™ adjuvant to enhance the immune response and stimulate high levels of neutralizing antibodies.
NVX-CoV2373 contains purified protein antigen and can neither replicate, nor can it cause Covid-19. In pre-clinical studies, NVX-CoV2373 induced antibodies that blocked the binding of spike protein to cellular receptors and provided protection from infection and disease.
It was generally well-tolerated and elicited robust antibody response in Phase 1/2 clinical testing.
NVX-CoV2373 is stored and stable at two degrees Celsius to eight degrees Celsius, allowing the use of existing vaccine supply chain channels for its distribution. It is packaged in a ready-to-use liquid formulation in 10-dose vials.
Five ways to measure the effects of COVID-19 on women
- Odile Mackett
Women have been affected by the pandemic more than men in many ways. Policies should reflect this.
The case has been made for the need to include gender in every analysis of social policy. But many of the toolkits which have been designed to do so have come up short. This is for a variety of reasons. Some of these shortcomings include a singular focus on women rather than relations between men and women; a focus on policy outcomes without a change in policy processes; and the inclusion of aspirational gender equality goals rather than goals for practical implementation.
But a framework developed by retired economics professor Marilyn Power offers a practical solution. Her framework can be used to evaluate the effects an event is likely to have on women. It can be applied to policies too. It draws together common aspects applied in gender studies and includes accounting for caring and domestic labour, considering human well-being, human agency, making ethical judgements, and undertaking an intersectional analysis.
I have used Power’s framework to examine the impact of COVID-19 on South African women. My research found that many of the challenges women experienced had been made worse by the pandemic. This was mainly as a result of the slowdown in economic activity and the restrictions on movement. These made women particularly vulnerable to physical abuse, a loss of income, and a decline in mental and emotional well-being, among others.
How women were affected
Household circumstances: The framework states that household circumstances should be considered in addition to individual circumstances. Household circumstances are vital when studying women because they tend to be the primary caregivers in the home, the number of female-headed households has grown, and they perform the bulk of domestic or household labour.
The importance of looking at both household and individual circumstances becomes clear when one looks at the impact of the COVID-19 pandemic. The closure of schools and early childhood development centres meant that women experienced an increase in their domestic responsibilities. Evidence shows that far more women than men reported increased time spent on childcare during the first few months of the hard lockdown.
Human well-being and agency: The pandemic affected both the well-being and agency of women.
Human well-being has been defined as “what people are able to be and do”. Amartya Sen, an award-winning economist, has recommended the use of five instrumental freedoms to measure well-being. These list aspects which define an individual’s relationship to their communities or the state. They include political freedoms, economic freedoms, social freedoms, transparency guarantees and protective security.
These freedoms include, for instance, having enough assets, the right to live a life of dignity, and the peace of mind which goes with feeling safe in one’s community.
Agency, on the other hand, has been defined by political analyst and feminist Lois McNay as “the capacity of a person (or other living and material entities) to intervene in the world in a manner that is deemed … to be independent or relatively autonomous”. Thus, the more freedoms individuals are guaranteed in society, the more their human agency will be enhanced.
During the pandemic women were more likely to lose their jobs than men. This loss had a major impact on women’s economic freedoms as well as their social freedoms.
Making ethical judgements: Ethical judgements in the framework relate to traditional economic assumptions which predicate that economic analyses or policies are value and judgement free. Others have argued, however, that policies and interventions which do not explicitly deal with value judgements only serve to mask “implicit assumptions about race, class and gender”, even if unintentionally.
It is thus important to engage with value judgements to make clear what implicit assumptions underlie public policy decision making.
One example of this was the South African government’s social security response to the pandemic, which included the Social Relief of Distress grant. This grant was only made available to unemployed individuals who didn’t get any other grant or qualify for Unemployment Insurance Fund benefits. The conditions under which the unemployed could apply for this grant were stringent – and still emphasised the need to work.
The stringent conditions meant that many vulnerable individuals were excluded. These included those who might already be receiving existing grants or received remittances from family members, but who might still be living in poverty. A large percentage of these would be women.
Intersectional analysis: This requires thinking about other social identities which define women beyond just their gender, such as race, sexual orientation and class, among others. These additional social identities privilege and disadvantage women in varying ways.
Black women, for instance, would be more severely affected by the social ills which have accompanied this pandemic than any other group of women in South Africa. Separating women by race in policy analysis would thus provide useful information which would not be otherwise observed had women been studied as a homogeneous group. Similar arguments could be made for further segmenting groups according to their social identities.
Next steps
Women make up half of the South African population. It’s therefore important to consider how decisions and policies affect them. Failing to undertake a gendered analysis doesn’t equate to men and women being treated equally. Rather that women are likely to be implicitly negatively biased.
How South Africa dropped the ball on health communication
- Sue Goldstein, Nancy Coulson and Nirvana Pillay
Community leaders and outreach community workers are calling on education to enhance their understanding of Covid-19.
Ongoing case study research conducted by the SA Medical Research Council (SAMRC), Human Sciences Research Council and thewww.sarraouniatrust.orgon the Covid response and likely vaccine hesitancy in four wards in South Africa has found that on the ground the Department of Health is absent as an authoritative voice about Covid-19 and vaccinations.
Instead, community leaders have relied on popular media and the “family meetings” hosted by President Cyril Ramaphosa for information. As a consequence, despite being more than one year into the Covid crisis, community leaders and outreach community workers are asking for education to enhance their understanding of Covid and to build their capacity to respond to questions and health emergencies in their areas.
How did it come to this?
Epidemics are not new in South Africa. The country has a long history of health communication work to respond to infectious disease. In the early 1990s as the HIV epidemic escalated in South Africa there was a thread of misinformation about HIV being brought into the country by ANC cadres who had been living in exile. HIV stigma and homophobia were commonplace.
Over time, the Department of Health positioned itself through effective partnerships with NPOs, media and communication consortiums to challenge this and boost prevention efforts (increasing consistent condom use from 11% in 1995 to 84% of young men in 2012) by launching successive well branded and researched campaigns that included media and social mobilisation.
The Department of Health’s Khomanani Campaign (in its early years), and the Department of Health-funded Love Life andSoul Citycampaigns were all found, in successive evaluations, to increase knowledge, challenge social norms and support behaviour change, including increasing knowledge about antiretroviral therapy (ART) and prevention of mother-to-child HIV transmission.
Importantly all these campaigns confirmed that where communities are met with education activities on the ground that reinforce mass media messaging this is an effective approach to behaviour change. Thedecision of the Department of Healthto include community health workers into ward-based outreach teams to work in specific neighbourhoods in 2012 was the opportunity to establish a sustainable mechanism in the Department of Health for on-the-ground health promotion activity that could complement national mass media messaging.
The last decade has witnesseda severe decline in health promotionand health communication capacity in the Department of Health. For example,research has foundthat community health workers are poorly prepared for their education role.
There are no publicly available evaluations of Department of Health campaigns. The impact of thePhila campaignwas not measured; however, an independent evaluation of all NPO campaigns in 2012 showed that the joint impact of these campaigns was good, but needed to be consistent and continue to support changes in behaviour.
Over the past 10 years, less funding has been made available by the government to NPOs working in health communication. Given the ongoing seriousness of HIV and TB in SA, this decline in resource allocation makes no sense. One argument put forward in explanation of this is that the option for treatment, such as ART, has outpaced disease prevention, making health communication, which is more often associated with disease prevention rather than treatment, redundant (treat to prevent).
However, the enormous cost to our health service of managing HIV as a chronic health condition for the estimated seven million affected people should challenge this orthodoxy, and in addition health communication is critical in maintaining adherence to long-term treatment. In fact, if anything, the introduction of HIV treatment made the health messaging around HIV more complex, not less.
In the last 10 years there has been no dramatic policy shift in the Department of Health away from prevention activities, yet with a burgeoning crisis of non-communicable diseases, communication around prevention of these, including decreasing alcohol, tobacco and highly processed food consumption, is absent from the department.
Thus, the demise in health communication capacity is more likely to be because of the absence of political will and/or its vulnerability to corruption.
In 2020, as South Africa was gripped by the early months of the Covid crisis, an offer to the Department of Health was made by a group of health communication researchers and practitioners from the School of Public Health at the University of the Witwatersrand, the SAMRC and the NPO sector to support Covid communication. This support was rebuffed. In addition, a carefully designed strategy by one of the NPOs and supported by the other players was examined and rejected.
The revelations about the siphoning of resources by Digital Vibes provide the first convincing explanation of why this happened, suggesting that the primary reason for the collapse of health communication capacity in SA has been the vulnerability of these resources to corruption. Current revelations beg questions about the past 10 years.
Covid communication has become an exercise in high-level public relations, with the president himself leading communication efforts. While the stance of the president is to be commended, it should not be confused with being an adequate substitution for an evidence-led national health campaign.
Although theSolidarity Fundhas a communication campaign, this is no substitute for a government-led campaign, (and support and oversight of this campaign was also rejected by Solidarity). In the absence of such communication, community leaders on the ground are left to try to make sense of news stories.
On the ground, the authoritative voice of the Department of Health is missing in action.
The world is in the throes of a climate crisis, and the possibility of future pandemics and disasters related to this crisis is ever-present. Preparing for these crises is critical, especially in an unequal world and country. One way to prepare for this is to ensure that all people are health literate,which is definedas:“The degree to which individuals have the capacity to obtain, process, and understand basic health information needed to make appropriate health decisions.”
It is incumbent on the Department of Health to take a leadership role in ensuring that the SA population is health literate, and not to use communication resources for public relations, or worse, for individual enrichment.
Sue Goldstein is deputy director at SAMRC Centre for Health Economics and Decision SciencePRICELESS SA. Nancy Coulson is director at the Sarraounia Public Health Trust and visiting senior lecturer at the University of the Witwatersrand. Nirvana Pillay is director at the Sarraounia Public Health Trust and visiting researcher at the School of Public Health at the University of the Witwatersrand.
All University entities are required to be fully operational as from 1 February 2021.
Thank you to all those staff members who made it possible for Wits to complete the 2020 academic year and who ensured that the University remained operational. Your contribution and commitment is recognised and appreciated.
It will now require our collective effort to prepare for the 2021 academic year and to fulfil our mandate to deliver academic, research and service excellence.
To this end, all University entities are required to be fully operational as from 1 February 2021.
Professional and administrative staff are required to return to campus as from Monday, 1 February 2021. Members of the Senior Executive members (SET) have been authorised to determine and approve the level of staff required in their respective faculties and divisions, in order to ensure that offices and services are fully operational. Line managers are required to act in accordance with the SET’s directives in this regard.
Academics are required to be accessible for academic and research purposes.
The following exceptions apply:
Employees with co-morbidities (such as active or on treatment for cancer, diabetes, asthma or other respiratory illnesses) should voluntarily declare these ailments to their line manager or provide a valid doctor’s letter that indicates specifically why they cannot report for work. Where line managers believe that it is necessary, a second opinion may be obtained from selected healthcare practitioners based at the Wits Donald Gordon Medical Centre, as described in the HR Practice Note on this matter (available on the HR page on the Intranet). These staff members should work productively from home.
Staff members over the age of 60 who may be at risk should be enabled to work from home as per the University’s HR Practice Note on this matter. Employees over the age of 60 who do not have co-morbidities, and who are healthy, may of their own volition return to the workplace at their own risk.
Staff members who work in open plan offices or under other conditions which may be high-risk, may work on a rotational basis as determined by their line managers, with the approval of their SET member. Work in open plan spaces becomes a risk for Covid-19 infection when the relevant protocols aimed at the prevention of infection are not adequately adhered to by employees.
Workplace Safety
The health and safety of every member of the Wits community is paramount, and again, it will require our collective effort to keep everyone safe.
Staff members are required to:
Complete the self-screening form via the Wits LogBox Screening App every day before entering campus;
Wear a mask over your mouth and nose at all times;
Practise physical distancing (stay a minimum of 1.5 meters from anyone else);
Refrain from gathering in closed spaces that are not adequately ventilated (no gatherings should be allowed in tearooms and canteens);
Sanitise regularly, or wash your hands with soap and water for 20 seconds and dry them properly; and
Abide by all Wits’ COVID-19 policies and protocols.
Responsibilities for Line Managers
Line managers must complete or update a risk assessment for their respective entity and must implement the risk mitigation measures before staff members return to the workplace.
Line managers must work with their assigned Human Resources and Health and Safety Officers, the Services Department, and any other University entity to ensure that the following measures are in place:
the physical distancing of staff members in the workplace;
the adequate provision of sanitisers and/or soap and water;
the regular cleaning of venues and work spaces;
the provision of personal protective equipment for specialised areas (and ensuring that it is correctly worn);
the completion of the daily symptom screening form on the Wits LogBox Screening App; and
the adherence to Wits’ protocols to prevent the spread of infection.
Reporting infections
Managers are requested to report all Covid-19 infections immediately. Staff infections should be reported to the Occupational Health, Safety and Environmental Management Directorate via Dept-OHS-Admin@wits.ac.za and student infections should be reported to Anna.Moloi@wits.ac.za.
Conclusion
Let us take the necessary precautions to ensure our own personal safety and that of our colleagues, students and friends, as we return to campus. Please chat to your line manager or relevant executive should you have any further queries about the return to campus plans.
The third wave of the coronavirus has started in Gauteng and is rapidly gaining momentum as we head into the winter season.
We are about two weeks to the start of the examination period, and whilst most students are learning remotely, there are still thousands of Witsies in residences, and many others accessing campuses and buildings every day. For the good of all members of the community, please abide by Wits’ COVID-19 policies and protocols at all times.
Infections are rising
We appeal to you to please:
Complete the updated screening form on the Wits Logbox App every day. The App is being simplified to make it easier to use.
Show your clearance note to the security officers before entering Wits’ campuses or buildings.
Wear a face mask that covers your mouth and nose, especially when indoors with other people.
Stay at least 1.5 metres from anyone else.
Stay away from gatherings (no social events are permitted) and crowded areas, especially when indoors.
Keep rooms well ventilated – leave windows and doors open even if it is cold.
The national vaccination programme has commenced but will take several months to roll-out. It is currently only targeted to individuals older than 60 years of age. If you are 60 years or older, register for the COVID-19 vaccination programme via the national Electronic Vaccination Data System or click here: https://www.gov.za/covid-19/vaccine/evds
Mental Health and Wellness
Your overall personal health and wellness is important. The pandemic is affecting our physical, emotional and mental health in different ways. Read more about the impact of the pandemic on students and women. If you, or anyone you know needs counselling, please make use of the following services offered by the University.
Students can reach out to CCDU via info.ccdu@wits.ac.za or call the Wits Student Crisis Line on 0800111331 (24/7/365 toll free).
Staff members can make use of Kaelo’s counselling services (at no cost) by calling 0861635766, by dialling *134*928, by sending a ‘Please call me’ to 0726205699, or by emailing asknelson@kaelo.co.za.
Our Collective Responsibility
We appeal to all staff and students, out of mutual respect and in the interests of the collective health and safety of our community, to abide by all COVID-19 protocols, rules, and policies (and encourage others to do the same). We must act responsibly for the greater good of our broader community and society.
One of the world’s coolest inventions
- Professor Barry Dwolatzky
South African-born engineer and entrepreneur is making a significant contribution in the fight against Covid-19.
Athens, Ohio, and Potchefstroom, South Africa, seem to be worlds apart, but they do have some surprising similarities and connections. Athens is a small city in America’s Midwest. It has a tiny “downtown” area with a few shop-lined streets, some churches and modest historical buildings. It has more than its fair share of trendy food places, bars with live music and coffee shops. These serve the needs of its nomadic population of university students. Dominating the city is the largest campus of the Ohio University with an enrolment – in Athens – of about 22,000 students. The non-student population of Athens is about 5,000.
Potchefstroom, usually called “Potch”, and now officially renamed Tlokwe, is also a university town. North-West University (NWU) dominates the town. It has roughly the same size student population as Athens. The non-student population is, however, more than 43,000 – making it far larger than Athens. The area around NWU also has a vast selection of bars and food places.
For me the link between Athens and Potch is the person responsible for one of the world’s coolest inventions. His name is Dr Dave Berchowitz, a South African innovator and fiercely persistent entrepreneur. Berchowitz was born and raised in Potch. After finishing school at Potch Boys High, Berchowitz went to Wits University to study aeronautical engineering in the 1970s. This is where I met him. I was studying electrical engineering at the same time. We became lifelong friends.
Berchowitz is a stereotypical nerd with a sharp intellect, broad-ranging interests, a quirky sense of humour and strong sense of social justice. He is also a fantastic engineer – one of the best I know - able to easily move from the highly theoretical to the deeply practical within the space of a single sentence.
As a master’s and later as a PhD student at Wits working under Professor Costa Rallis, Berchowitz became interested in Stirling Engines. I won’t at this point shoot off on a complicated technical tangent. Suffice it to say that these are “external combustion” engines developed in the early 1800s. They have many attractive properties, particularly their very high level of energy efficiency. The Stirling Engine lost out to “internal combustion”, the familiar petrol- or diesel-powered engines under the bonnets of our cars, in the 1920s. They soon dropped off the mainstream engineering radar screen.
In the late 1970s Berchowitz took his new-born passion for Stirling Engines to the USA where he joined a company called “Sunpower” in Athens, Ohio. Sunpower was established in the 1960s by William Beale, a passionate inventor and mechanical engineering lecturer at the Ohio University. It was one of very few companies in the world developing technology based on Stirling Engines. Beale recognised Berchowitz’s engineering genius and quickly promoted him to a senior technical position at Sunpower. One of Berchowitz’s projects was to develop a Stirling cooler. This is a refrigerator driven by a Stirling engine rather than a conventional compressor.
In the mid-1980s I visited Berchowitz at Sunpower in Athens. On his desk was a steel cylinder the size of a 1 litre cold drink bottle lying on its side. Berchowitz lit a small blowtorch and focused the naked blue flame on one end of the cylinder. As it heated up icicles started to form on the other end. The more the flame heated its end of the cylinder, the colder the other end became. In my fascination I stretched out a hand to touch the cold end. “Careful!” Berchowitz shouted. “It’s so cold your finger might stick to it.”
The technology was world-leading then, and it’s still at the forefront of cooling technology today. One of Berchowitz’s coolers went into space as part of an experiment on one of the NASA Shuttle Missions. After a few years Berchowitz set up his own company, called Global Cooling, to take this amazing technology to market. Over the next 30 years Berchowitz lived the very unexotic life of a tech entrepreneur. There were a few highs when it looked like Global Cooling would achieve it’s “big breakthrough”. Partnerships and joint ventures with some of the biggest technology companies in the world were explored, but … as any entrepreneur will tell you … unsuccessful deals are far more common than successful ones.
In 2009 another Wits alumnus (BSc (Eng), Mechanical, 1982), Neill Lane, joined Global Cooling as CEO. Berchowitz’s small factory in Athens grew a bit and shrank a bit as the years went by and the engineer from Potch struggled to find his niche. He was driven by the unwavering conviction that his Stirling coolers were unique and far better than any of its competitors. His belief and passion for what he had built never faltered even when money ran low and yet another deal ended in disappointment.
And then … in March 2020 … the Covid-19 pandemic reached the USA. The race for a vaccine became the overriding priority for scientists and engineers in every corner of the world. The most promising vaccines, using mRNA-based medical formulations, have one major downside. They need to be stored at an extremely low temperature: minus 70 degrees Celsius! Where will we get coolers that can work efficiently at such a low temperature? A small company, Global Cooling, now called Stirling UltraCold, in Athens, Ohio, had the answer, and knew that its time had come!
In the wake of the global pandemic, so many terrible and negative outcomes have resulted. There have, fortunately, been a few bright lights. One of these is that our own determined inventor from Potchefstroom and Wits University has at last achieved his long awaited and well deserved “big breakthrough”. Berchowitz, South African-born engineer and entrepreneur, is making a significant contribution in the fight against Covid-19, and prospective investors are beating a path to this small university town. I recently heard that Stirling UltraCold has been acquired and merged with the listed company BioLife Solutions, opening up many exciting new opportunities for Berchowitz, Lane, who is now Chief Strategy Officer, and their team.
Book calls for a rethink of capitalism amid the ravages of Covid-19
- Edward Webster
Rethinking capitalism requires that the primary focus should be on the distribution of economic power as the potential leading causal factor driving inequality.
Instead of being the great leveller, as pandemics have been throughout history, the coronavirus pandemic has revealed and compounded pre-existing inequalities in wealth, race, gender, age, education and geographical location.
This is the paradox with which Ian Goldin – the former CEO of the Development Bank of Southern Africa and now a professor at the University of Oxford – begins his recently published book, “Rescue: from global crisis to a better world”.
Past studies of the forces driving the reduction of inequality have foregrounded ‘malign forces’ – such as wars, natural catastrophes and epidemics – and ‘benign forces’ – more widely accessible education, increased social transfers and progressive taxation.
Social scientist Goran Therborn, in his classic 2013 study of inequality, brings these two forces together. He acknowledged the significance of the ‘malign’ forces of violent revolution and war. But he also emphasises the ‘benign’ forces of peaceful reform that led to the ‘egalitarian moment’ after World War Two. This is when welfare states were built around the notion of full employment, universal health care, education and social security.
Under certain circumstances, far-reaching peaceful reform has been possible.
Why then has the coronavirus pandemic deepened inequality rather than reduced it?
Goldin attributes this paradoxical outcome to four decades of neoliberal thinking.
I agree with his critique of neoliberalism. But he doesn’t give sufficient attention to power, particularly the concentration of economic power. This book, nevertheless, offers important opportunities for the elites of the world and ordinary citizens to explore ways of reducing inequality.
The case for a rethink
Inequality, Goldin suggests had been rising in both Europe and the US since the 1980s. He argues that this is:
mainly due to the tide of liberalisation that was ushered in when Margaret Thatcher in Britain and Ronald Reagan in the US initiated a race to the bottom in taxation, attacks on trade unions, and a weakening of competition policy, which all allowed for the growing concentration and strength of employers.
What is needed, Goldin believes, is a fundamental rethinking of capitalism. Big government and the activist state is back, he says. The pandemic has led to a counter-revolution. Conservative governments now go beyond even arguments put forward by the economist Maynard Keynes in the 1930s that governments needed to spend their way out of the Great Depression.
Unless inequality is reduced, he warns, populism and protectionism will become dominant.
The tragedy is that the policies implemented by these populist leaders benefit the few not the many, thereby deepening and entrenching inequality.
For Goldin this global trajectory of populism is not inevitable. He believes that it is human actions and leaders that shape societies, not simply events.
The chapter Reducing inequality is full of sensible proposals designed to reduce inequality. Among these are:
the closure of tax havens and loopholes,
the introduction of wealth taxes on the assets of the top 1% earners,
higher inheritance taxes on the transfer of wealth of the top 1 per cent, and
progressive income taxes that exempt the lowest earners and then rise steeply for the highest earners.
Goldin discusses how five biggest American tech companies -– Facebook, Amazon, Apple, Netflix and Google –- dominate the stock markets. He cites the fact that the US$28 trillion attributed to these companies is five times greater than all the physical assets owned by all the other 500 companies in the Standard and Poor’s stock index.
Jeff Bezos, the founder of Amazon, saw his wealth almost double. This makes him the first person in history to be worth more than US$200 billion. Meanwhile, the wealth of Elon Musk, the founder of Tesla, increased by more than US$160 billion during the pandemic, to US$184 billion.
What needs to be done
Goldin draws on Nobel Prize Winner, Amartya Sen, who sees inequality as the function of the distribution of capabilities. From this perspective, inequality is above all about inequality of opportunities available to people to lead fulfilling lives. Central to this is education, gender and human rights.
Sen is far removed from orthodox neoliberalism. He adopts human well being, rather than mere growth, as the goal of development. But his approach to development is grounded in pragmatic neoliberalism. His message is clear: people in developing countries should adopt free markets, strictly delimit the role of the state, promote liberal democratic institutions , ensure the provision of basic education and health care and welcome open discussion of issues.
I disagree with Goldin when it comes to drawing on Sen. This is because I am sceptical of Sen’s faith in free markets, free speech and reasoned social progress. He abstracts freedom from power relations and focuses on individual actors.
But inequality is primarily a power relation. Sen gives a false promise to the poor and excluded. He does not challenge the concentration of economic power, centred on global and national markets. Instead he takes them for granted.
A ‘rethinking of capitalism" requires that our primary focus should be on the distribution of economic power (rather than the unequal distribution of capabilities) as the potential leading causal factor driving inequality.
This perspective requires that the distribution of economic power be addressed head-on and necessitates a bolder more integrated approach.
One of the strengths of this book is its historical perspective. At the height of World War Two, the deadliest conflict in human history with an estimated 70 to 80 million fatalities, civil servants in the UK, were told to collaborate with economists like John Maynard Keynes and British economist and liberal politician William Beveridge to plan for a better life for all.
The Beveridge Report, published in the UK in November 1942 at the height of the war, provided the foundations for the welfare state. It set out to overcome the ‘five giants’ of ‘want, disease, ignorance, squalor and idleness’.
Whether this optimistic and inspirational scenario of post-war Europe is feasible in many countries, including South Africa, is questionable.
But by identifying some of the ways in which we can precipitate change to reduce inequality, this book is a valuable contribution to the debate on any country’s future.
We must seize the moment for a global pandemic surveillance and response scheme
- Amandeep Gill with Bruce Mellado and members of the I-DAIR Pandemic Scientific Group
No more pandemics—this is the ambitious goal set by the Independent Panel for Pandemic Preparedness and Response
Its report reviews the international community’s response to covid-19 and identifies lessons learned.
Covid-19 has shown that our lack of globally accurate, real-time data on outbreaks is a matter of life and death. A leading group of scientists and experts, from every part of the world, must come together urgently to create a new, neutral, and trusted digital system that can revolutionize how data is gathered and used globally.
We have done this before with weather, and more recently with predicting tsunamis through a global system of sensors. The resulting information rich environment enables all of us to adapt to the forecast. To prevent the next disease outbreak becoming a global crisis, we need similarly routinised data flows to generate epidemic intelligence and alerts.
Digital technologies, particularly artificial intelligence (AI), are now mature enough to sift the signal from the noise in the mass of mobility data, social media posts, and clinical reports.AI can weigh data across human, animal, and plant health and spot patterns. It can help derive intelligence from unusual data sources such as sewage samples or empower citizen scientists to report unusual events using mobile phones.Democratization of molecular biology, such as serology or next-generation sequencing of the genomes of pathogens, has opened up new avenues for monitoring risks.
But bringing this together globally won’t be easy for three reasons.
First, our existing health data systems are fragmented and plagued with gaps. Their architectures are based on a narrow foundation of a few disciplines. You cannot simply wire them together.
Frameworks to pool information across international organizations dealing with One Health—animals, humans, plants, and their shared environment—have been created, but lie dormant without adequate workflows. Despite laudable initiatives such as the World Health Organization (WHO)’s Global Outbreak Alert and Response Network (GOARN), the Global Health Security Agenda, or the Coalition for Epidemic Preparedness Innovations (CEPI), a winning coalition has never come together to support a truly global and coordinated response.
Mistrust in global institutions is rife. Nations do not share information in a timely and complete manner despite legally binding obligations under WHO’s International Health Regulations.
Current reporting obligations require an outbreak to be reported through a labyrinthine bureaucratic chain before it reaches a global agency, days or even weeks after it was reported by a local clinician.
The second challenge is privacy and digital trust. Many countries lack data protection laws or fail to enforce them. Few people have basic data literacy and struggle with partial information or misinformation about what happens with their data. Technological solutions could help, including new techniques for protecting data and preserving privacy such as distributed learning, but it is equally important to engage the community in the development of these solutions in order to gain acceptance. The infrastructure for hosting outbreak data, should also be neutral and not beholden to any government or corporate interest. As far as possible, raw data should stay local and contribute to the global picture, without having to leave national jurisdictions. Winning the trust of the public will take time and concerted effort.
A third challenge is politics. An agenda set up by a narrow group of countries or disciplines will not result in a critical mass of international support or win the trust of the general public.A global, science-based, digitally enabled, and end-to-end pandemic surveillance and response scheme needs to be built out collaboratively. Its data architecture and information sources need to be examined from a multi-disciplinary perspective across epidemiology and public health, molecular biology, social and behavioural sciences, complex systems, networks and computer sciences, environmental sciences, gender, ethics and governance as well as health economics and policy. The new generation of researchers from the Global South now emerging should play a role in their design so that its deployment is feasible in all income settings.
Mutual suspicions and reluctance to collaborate, need to be overcome among government, academia, the private sector and civil society.An innovative governance structure tiered to accommodate contextual specificity for data access and data use in different countries would be essential. It should rest on principles such as trustworthiness, transparency, fairness, equity, independence, and neutrality. Investments in data infrastructure, and capacity development of the health workforce,will be needed.
We should begin by convening a globally representative group of scientists to examine how this could work in practice and to suggest a research and development agenda, ensuring that, as the Independent Panel warned, their report does not gather dust on a shelf, but sparks immediate and transformative global action. We have the tools to prevent the next pandemic before it starts, and cannot afford delay in putting them to work.
Amandeep Gill,project director & CEO, International Digital Health and Artificial Intelligence Research Collaborative (I-DAIR), GenevaSwitzerland.
Acknowledgements: The author acknowledges the contribution of the following members of the I-DAIR Pandemic Scientific GroupAnurag Agrawal (Council of Scientific and Industrial Research, India); Gershim Asiki (African Population and HealthResearch Center (APHRC), Kenya); Hala Audi (Trinity Challenge, UK); Marc Choisy (University of Oxford, UK, and Oxford University Clinical Research Unit (OUCRU), Vietnam); Sara (Meg) Davis(Graduate Institute of International and Development Studies, Switzerland); Ayman El-Mohandes(City University of New York (CUNY), United States of America); Antoine Flahault(University of Geneva, Switzerland); Emma B Hodcroft(NextStrain, United States of America, and University of Bern, Switzerland);Ashish Joshi(CUNY, United States of America);Olivia Keiser(University of Geneva, Switzerland);Sylvia Kiwuwa-Muyingo(APHRC, Kenya), Jeffrey V Lazarus(University of Barcelona, Spain);Sam Makau(WACI Health, Kenya);Malebona Precious Matsoso(University of the Witwatersrand, South Africa);Rosemary Mburu(WACI Health, Kenya);Bruce Mellado(University of the Witwatersrand, South Africa); Vinh-Kim Nguyen(Graduate Institute of International and Development Studies, Switzerland) ;Patrick Okwen(eBASE Africa, Cameroon);James Orbinski(York University, Canada);Tavpritesh Sethi(Indraprastha Institute of Information Technology-Delhi, India);Serge Stinckwich(United Nations University, Macau SAR);Le Van Tan(OUCRU, Vietnam);Yik Ying Teo(National University of Singapore, Singapore);Guy Thwaites(University of Oxford, UK, and OUCRU, Vietnam); Andrea Sylvia Winkler(University of Oslo, Norway, and Technical University of Munich, Germany) and Peiling Yap(I-DAIR, Switzerland)
Children are easy targets for exploitation and traffickers during Covid-19
- Ajwang’ Warria, Margaret Roper, Marcel van der Watt, Susan Marx and Heather Dixon
The theme for this year’s Child Protection Week, which began on 31 May, is “Let us all protect children during Covid-19 and beyond”.
Child trafficking is the buying and selling of children for exploitative purposes such as sex, labour and domestic work. Globally, one in every three victims of trafficking is a child. However, characteristics linked to the age profile and risk factors of the victims vary from region to region and also differ according to social contexts.
According to a recent report released by the United Nations Office on Drugs and Crime (UNODC), children make up a third of trafficking victims who are identified and rescued – a figure that has tripled in the past 15 years, with girls mainly being trafficked and exploited for sex and boys for (forced) labour.
The profile of a child victim of trafficking is often characterised by many intersecting vulnerabilities. Age-related risks are compounded by socioeconomic dimensions and other factors such as the child’s behavioural and developmental needs, lack of parental care and/or dysfunctional families. In addition, domestic violence, migration and discrimination can increase a child’s risks to trafficking.
The vulnerabilities that are evident in child victims of trafficking are often connected to their family background. In poor communities, socioeconomic and social norms play a big role in trafficking, whereas in more affluent communities dysfunctional parenting or lack of parental care may make the child vulnerable. Generally, children with family problems are easy to recruit because traffickers create some attachment with or a sense of belonging in the victim. Traffickers use drugs or alcohol and isolation tactics to increase their control over the child.
Although children are not the face of Covid-19, they risk being among its biggest victims based on the pandemic’s broader economic and social disruptions. The pandemic and the lockdowns have exacerbated children’s vulnerability – especially with partial or full school closures, and the loss of school-based services and nutrition programmes. While online learning has benefited some children, those children who do not have access to devices and the internet have suffered greatly.
The lockdown, school closures, and increased poverty rates during the pandemic mean that some areas have experienced increases in child labour, girls entering child marriages or boys being recruited into armed groups or gangs. Other regions have seen increases in teen pregnancies and abused children.
The volume of exploitative material online has increased considerably as traffickers have integrated technology and use digital hunting grounds. With more unsupervised children online and younger children accessing the internet, it has become easy for traffickers to approach and “court” children and young people on social media. In the quest for friendship, acceptance, affection and attention, children become easy targets for traffickers and exploiters.
Traffickers are also adapting their strategies, taking advantage of publicly available personal information, easily blending into social activities online and being anonymous in online spaces. Live streaming, webcams and other digital platforms are creating new forms of exploitation – where there is no need for transportation and transfer of victims and which allow for simultaneous abuse by multiple perpetrators in multiple locations.
What can be done to protect children from trafficking during Covid-19 and beyond?
Addressing known risk and vulnerability factors from a systemic perspective – looking at individual and demographic perspectives, household and family factors, community-level factors, structural factors and situational factors that temporarily increase exposure to child rights violations, gender inequalities and violence.
Implementing prevention activities such as promoting community awareness through education, fostering coalitions and networks, educating service providers and changing organisational practices.
Expanding social assistance to families.
Encouraging child participation in decision-making processes and in the development of interventions to protect children from exploitation and trafficking.
Addressing the psychosocial impact of the crisis on children and young people and having specific interventions for vulnerable children.
Advocating for the development of a collective distance public education system and additional support for children with disabilities.
Providing practical support to parents and caregivers.
Strengthening the child protection systems before pandemics in order to prevent or mitigate the increased risks of abuse and exploitation during periods of crisis.
Prioritising the continuity of child-centred services and advocating for resources to ensure telehealth and telesocial service access and expansion of outreach strategies such as home visits, mobile clinics etc;
Collecting data and the development of rapid assessment and response tools to gauge the effect of the pandemic on children, families and essential child protection services.
Reporting suspicious cases of child exploitation and trafficking to a social worker, the police or to the nearest Department of Social Development office or child welfare organisation.
The Covid-19 pandemic is an unparalleled crisis that presents extraordinary risks and challenges to the rights, safety, protection, care, development, and survival of children globally and in South Africa. These risks and challenges can only be mitigated and addressed through unique, innovative, equitable, culturally relevant, and cohesive interventions for children. Without quick concerted action, Covid-19 will have devastating impacts on children and other vulnerable populations in our society. However, we have the opportunity to defeat this pandemic and through it, uphold children’s rights and transform the way we nurture, develop and invest in children and young people.
During Child Protection Week, take the time to acknowledge the children around you and in your community and commit yourself to become part of the process of striving for and working towards the safety, care and protection of all children during Covid-19 and beyond.
This work is made possible through support from USAID and the South African Department of Science and Innovation (DSI), as a supplement to a USAID Cooperative Agreement #7200AA18CA00009 (LASER-PULSE) to Purdue University. Contents reflect the views of the authors and do not necessarily reflect those of USAID or DSI.
Ajwang’ Warria is a Lecturer in the Social Work Department at Wits University. Together with Margaret Roper, Marcel van der Watt, Susan Marx and Heather Dixon, he is a researcher on a National Counter-Trafficking study in South Africa. This article was first published in Daily Maverick/Maverick Citizen.
Survey to unearth health info practices around Covid-19 in SA
- Wits University
Various studies have been conducted to understand the issues surrounding the Corona virus, and its impact on different population groups.
However, these surveys have mostly been conducted in the Global North in contexts that are socio-economically and spatially different from South Africa. Knowledge of the trends and behaviours in the South African context is limited.
To fill this gap and to provide insight into how South Africans access and share information about Covid-19, the Human Sciences Research Council (HSRC) and Wits Health Communication Research Unit (HCRU) have launched the INSIGHTS study to understand the health information practices in South Africa during Covid-19.
The multidisciplinary collaborative online survey is aimed at exploring the dynamics of access to information and information-seeking behaviours of South Africans
“Since no treatment is guaranteed to fully prevent infection or severe disease, an important part of the Covid-19 response involves targeting behavioural change. An in-depth understanding of trends in how the public seek and share COVID-19 information in the South African context, will help us to develop contextualised and effective communication strategies with bigger potential for uptake and averting public resistance,” says Dr Konosoang Sobane from the HSRC.
The Covid-19 pandemic has created an ‘infodemic’ where false information and misinformation has increased amongst communities, says Jennifer Watermeyer, Wits Professor and Director of the HCRU.
“There’s so much information out there about COVID-19 and it can be difficult for people to know where to access information and what information to trust. People are accessing information about COVID-19 from all kinds of platforms – news media, social media, WhatsApp, friends, healthcare workers.”
“Successful public health responses hinge on simple, time-sensitive, proactive communication that engenders trust.”
The public is invited to complete the online anonymous survey which is available in various languages.
Covid-19 has worsened SA's system of developing the skills of young people
- Stephanie Allais
The pandemic has heightened existing weaknesses in South Africa's skills training regime.
The COVID-19 pandemic has affected not only how we live, think and work but also how we acquire skills. This is particularly crucial for young people, large numbers of whom are excluded from labour market. South Africa’s latest Quarterly Labour Force Survey showed joblessness for those aged between 15 and 34 at 46,3%.
To address the challenges of skills provision and acquisition, policy makers and researchers have set their sights on the vocational education and training system. But the view that this alone is the answer to solve existing labour market crises is flawed for three reasons.
First, it ignores the main problem – the lack of demand for labour. Second, it highlights a lack of understanding of how skills are developed, and that the nature of the economy shapes the nature of skills produced. And third, it disregards the fact that the existing weaknesses of the vocational and education training system are caused by lack of labour demand and insufficient analysis of the role of the economy in shaping skill formation.
The relationships between education, poverty and inequality in South Africa are complex. Labour markets are a key determinant of inequality. But lack of demand for skilled labour outweighs lack of skilled workers. Nonetheless, building the skills of the workforce remains a crucial part of economic development and reconstruction.
In terms of skills development, a complex array of institutions and policies have been established since 1994 in an attempt to improve relationships between labour markets and education providers. Incentives have been created to encourage employers to provide training to their workers and pre-employed people.
However, these policies and institutions have met with many challenges. One is that the institutional environment is now complex and expensive, without much visible improvement in the system. There’s little to show for years of reform, as well as an extensive range of donor initiatives to support projects, policy reforms, and institutional reform.
One example is the Technical and Vocational Education and Training system. This has been the subject of many reforms. But policy makers and industry continue to argue that the system remains weak and that the colleges don’t meet their needs.
On top of this the qualifications system is enormously complex. Layers of new qualifications and ways of designing qualifications have been added, without removing the previous ones.
Against this backdrop, our research set out to understand the impact of COVID-19 on skills formation in South Africa.
Weaknesses
The pandemic has heightened existing weaknesses in the system. Few vocational colleges have the necessary facilities for online learning. Also, few students have the prior educational background that makes online learning workable.
Only 10 out of 50 colleges had learner management systems enabling online teaching and learning. Some sought to make tutorials available on social media. However, often lecturers didn’t have their own data or even a quiet place to teach from. Learners faced the same problems.
The second area affected by the pandemic is workplace placements. As a result of the pandemic, companies have been unable to accommodate learners. This has similarly been a long standing challenge.
A third affected area is funding: the skills system has lost about R6.1 billion as a result of suspension of the skills levy during the lockdown and other factors. The levy was suspended as part of tax relief to companies during the pandemic.
A further issue affecting the skills development system is the qualification system. What’s lacking is a balance between shorter training programmes and long-term formal qualifications. The advocates of micro-credentials – these are industry aligned short courses which have a narrow focus on preparation for work – are suggesting them as the solution to this lack of balance.
Changes
The Quality Council on Trades and Occupations – established in 2010 to set standards for and quality assure qualifications linked to a trade or occupation – has recently reconfigured occupational qualifications. These include revisiting the formal requirement for workplace experience, which learners now simply cannot get (and most could not get before COVID-19).
It has also introduced new regulations to address the need for short programmes which can only be accredited as a “part qualification”, which is constituted by credits within a full qualification. Full qualifications are now defined in terms of number of credits.
This step sought to address the proliferation of part qualifications that didn’t lead to a full qualification, as well as qualifications of varied sizes. But it created the unintended consequence of negating the possibility that industry associations could determine the need for a short programme that is accredited and that enables the graduate to access a specific opportunity in the workplace.
Thus, the organising logic is based on where qualifications exist rather than on where demand is.
Flawed logic
The lack of success is partly due to the flawed idea that market mechanisms will ensure more responsive, agile, demand-led Technical and Vocational Education and Training, using qualifications, including “micro-credentials”, as a policy lever.
The focus is on the need for agility and short-term relevance. Reforms have emphasised employers specifying the skills or competences they require, and education and training institutions being given funding for courses that attempt to lead to these specific competences.
This should, according to advocates, enable educational institutions to provide only the required competences and thereby enable “consumers” – employers or individuals trying to equip themselves in labour markets – to purchase only the “bits” that they want without having to sit through long educational programmes.
In this magical world vocation and education training will ensure that:
curricula are decentralised and therefore responsive,
employers can specify their needs, and
both public and private providers can be held accountable as their programmes can be measured against the competences delivered.
But this is a simplistic supply and demand notion. Policy reforms based on it take no account of how skills are actually developed for work in the real economy.
The approach also works against building strong, robust, healthy institutions.
Alternatives
South Africa needs to focus on supporting institutions, building partnerships with employers, and ensuring that thinking about skills is incorporated into industrial policy processes.
Our research highlights the need to think about the quality of work and organisation of workplaces as well as skills development inside industrial policy and inside different economic sector strategies. This also requires having formal providers of vocational education and training to be embedded inside the industries.
One implication of this is the need for industry- or sector-specific and not general strategies for skills development.
In addition, education institutions should offer broad vocational and education training qualifications that include components of general education and components of locally needed skills.
At the same time, we need better funding mechanisms for shorter accredited programmes that are recognised by employers and professional associations, and less formal, responsive short courses.
This requires deeper relationships between colleges and employers. It also requires more support for institutions providing the training and a set of qualifications that focus on occupational streams and clusters.
Finally and most importantly, skills policy needs to be in line with an economic recovery focused on jobs. Skills planning needs to be incorporated inside the industrial policy process instead of an add-on.
Covid-19 resurgence in Gauteng: A crisis that is likely to worsen rapidly
- Shabir A Madhi and Jonny Myers
Despite the predictability of the resurgence, unfortunately, Gauteng health facilities are seemingly underprepared to deal with the spike of Covid-19 cases.
Gauteng, the province with the smallest landmass in South Africa, is home to 15.6 million (25%) of South Africa’s estimated 59.6 million population. Consequently, the trajectory of Covid-19 resurgences in Gauteng has a major influence on the national picture. Scientists (including one of the authors of this article) warned already in February 2021 as the second wave was receding, that South Africa was likely to experience another resurgence by late May to June 2021 — as has transpired. This educated prediction was premised on three major factors.
First, despite bold announcements by the government in early January 2021 that South Africa would rapidly vaccinate 40 million individuals by the end of 2021 (the goal post having since repeatedly shifted), this aspiration was doomed to fail in the absence of having actually tied down a supply of the much sought after Covid-19 vaccines.
Second, despite the high force of SARS-CoV-2 infection that likely transpired in South Africa during the course of the first two waves, the Beta variant that evolved in the country is relatively resistant to antibodies induced by infection due to the original virus. Coupled with this is likely waning of antibody (probably required to protect against infection and mild Covid-19), even following natural infection by the Beta variant.
This waning of antibody contributes to diminishing levels of community immunity to protect against SARS-CoV-2 infection where there is a high intensity of ongoing circulation of the virus (more likely when only a small percentage of the population is vaccinated even with highly efficacious vaccines), leading to further resurgences of Covid-19.
Third, considering 80% of SARS-CoV-2 infections are directly or indirectly related to super-spreader events resulting from gatherings, particularly in poorly ventilated indoor spaces, a resurgence was likely to transpire as people were more inclined to gather indoors as we headed into the winter months of the year. The risk of such super-spreader events occurring was probably exacerbated by a largely Covid-19 unvaccinated population (not due to any choice of its own) becoming more complacent about the use of face masks and other measures that could assist in dampening the rate of spread of the virus.
Despite the predictability of the resurgence, unfortunately, Gauteng health facilities are seemingly underprepared to deal with the spike of Covid-19 cases requiring hospitalisation. Across the private and public sector, daily reports indicated that severe Covid-19 cases are being “nursed” in emergency departments at some hospitals until such time as bed space may be freed up in the wards.
This includes receiving supplemental oxygen for up to three days while sitting on a chair in a cubicle shared with three other Covid-19 patients. This is already the case in at least one of the largest hospitals caring for Covid-19 patients during the past three weeks. Furthermore, the surge in severe Covid-19 cases is placing additional pressure on care and the availability of bed space for non-Covid-19 illnesses requiring hospitalisation.
The situation in Johannesburg is compounded by the closure of the 1,000-bed Charlotte Maxeke Johannesburg Academic Hospital (CMJAH), due to a fire that occurred on 17 April 2021. Seemingly, there remains an impasse between departments in the City of Johannesburg and the Gauteng Department of Health (GDoH) on how to expedite the phased re-opening of the facility, while patient care remains interrupted. Unfortunately, as severe disease and death rates due to Covid-19 lag behind those of generally reported cases, the forecast for Gauteng is one of a worsening situation — possibly for the next two to three weeks at least.
Nevertheless, the crisis being experienced in Gauteng regarding a shortage of “beds” to care for Covid-19 cases, is unnecessary and an unfortunate manifestation of inadequate planning to mitigate the consequences of the resurgence. The decommissioning of the Nasrec Covid-19 field hospital facility (which was expensive to operate and seemingly under-utilised during the past two Covid-19 waves), was likely undertaken with the knowledge that the billions of rands spent on building state-of-art Covid-19 treatment facilities developed using alternate building technology (ABT) would be available should a resurgence be experienced.
Despite delays in the completion of these Covid-19 treatment facilities, the majority have now been handed over to GDoH. This includes a 500-bed facility next to Chris Hani Baragwanath Academic Hospital (CHBAH). Other additional resources purposed by GDoH for Covid management include a 183-bed facility in Carletonville, 300 beds at George Mukhari hospital, 300 at Jubilee Mall (Hammanskraal) and 150 in Bronkhorstspruit.
Currently, the greatest pressure on available “beds” for Covid-19 cases is in the City of Johannesburg —largely driven by the closure of CMJAH. The pressure on the health system and healthcare workers in Gauteng can be addressed immediately by fully operationalising the CHBAH Covid-19 ABT facility.
Despite this particular facility being fully equipped with state-of-art equipment, only 100 of the 500 beds are commissioned for use. Furthermore, the facility is only being used to admit patients deemed to be clinically stable and recovering from Covid-19, despite being designed and equipped to provide high-level and intensive care. Unfortunately, it appears that the driver behind the overwhelming underutilisation of the facility is the lack of planning on how it (and probably others) would be staffed to ensure that available “beds” are more than just beds, but rather fit for purpose for which the facility had been designed.
Albeit late, this needs immediate remedial work. In addition to the redeployment of all staff that would otherwise have been working in Covid-19 wards at the now-closed CMJAH, there needs to be immediate mobilisation of provincial healthcare workers and those from further afield (including unemployed doctors and nurses) to ensure that quality care is provided at the Covid-19 treatment facilities built for that purpose.
The public demand to benefit from the investment that has gone into the building of Covid facilities and ensure they are immediately operationalised to maximum capacity should be non-negotiable. Also, opening and staffing of these Covid-19 facilities are the least that can be done to show gratitude and provide relief to the medical and healthcare professionals who have worked selflessly and tirelessly in adhering to their oaths to provide quality care to the ill over the past 15 months. The situation has come with immense stress, suffering and even loss of life among healthcare workers, which cannot be allowed to continue due to deficiencies in planning to provide better care to South Africans.
Note: Covid-19 deaths data usually lag the trends in numbers of Covid-19 cases by two weeks, and excess mortality data is currently only available for deaths until 11 June 2021.
The number of likely Covid-19 deaths in Gauteng based on South African Medical Research Council excess mortality estimates:
First wave: 12,474 deaths through to 12 June 2021;
Second wave: 10,971 deaths; and
Third wave: 2,565 as of 19 June 2021.
Covid-19 deaths based on reported Covid-19 deaths:
First wave: 3,811;
Second wave: 4,489 and
Third wave: 1,131 up to 19 June.
Declaration of interest: Funded for Covid-19 vaccine studies by BMGF, South African Medical Research Council and Novavax; and for epidemiology studies on Covid-19 vaccines by BMGF and South African Medical Research Council. All funding goes to Wits Health Consortium at the University of the Witwatersrand.
Shabir A Madhi is Professor of Vaccinology, University of the Witwatersrand and Jonny Myers is Emeritus Professor in Public Health Medicine, University of Cape Town. This article was first published in Daily Maverick.
Professor Zeblon Vilakazi on the impact of the third Covid-19 wave
- Professor Zeblon Vilakazi
Gauteng is currently the epicentre of the COVID-19 pandemic, with almost 11 000 new infections reported in the province on Wednesday.
Our healthcare systems are under pressure and our healthcare professionals, including our health sciences faculty, joint staff and senior students are working on the frontline trying to save lives. We recognise your efforts and thank you for your selfless service to humanity.
Similarly, I would like to extend my appreciation to all staff who are working tirelessly to ensure that university operations continue under lockdown level 3, especially as we are in the assessment period. I have advised all Senior Executive members to work with their managers to ensure that rotation systems are put in place as appropriate in their respective units, to ensure that the risk of infection in the workplace is minimised.
We all know someone who has been infected and I would like to extend my very best wishes to every person who is recuperating – may you recover completely, and soon.
Many of us have also lost friends, colleagues, family members and loved ones in recent months. I would like to extend my condolences to all those left behind during this difficult time.
We have all been affected by the pandemic in some way - physically mentally and emotionally. I urge you to seek help and to make use of the services offered through the University if required.
Confidential counselling services are available for students via the Wits Student Crisis Line on 0800111331 (24/7/365 toll free) or through arrangements made via info.ccdu@wits.ac.za.
Staff members can make use of Kaelo’s counselling services at no cost by calling 0861635766, by dialling *134*928, by sending a ‘Please call me’ to 0726205699, or by emailing asknelson@kaelo.co.za.
We can change our immediate future and the trajectory of the coronavirus if we behave responsibly. Please complete the screening app truthfully before entering campus. Wear your mask properly over your mouth and nose. Maintain a safe social distance of 1.5 metres from anyone else. Avoid gatherings, especially indoors – meet outside if you must with your masks on. Ensure that rooms are well ventilated and sanitise regularly.
Update 66: Reporting infections
- VCO
We are in the midst of the third wave, infection rates are rising steeply across the country and hospital beds are filling up quickly.
We are in the midst of the third wave, infection rates are rising steeply across the country and hospital beds are filling up quickly. We are reaching the end of this term and assessments will be starting soon. Whilst many of the University’s activities have moved online, we appreciate that it is necessary for some staff and students to be on campus.
For your own safety, and to protect your loved ones, colleagues, friends, and members of the Wits community, please adhere to the following:
Meet outdoors where possible,
Ensure that all rooms are well ventilated,
Stay at least 1.5 metres from anyone else,
Wear a face mask that covers your nose and mouth,
Do not congregate in social groups on or off campus, and
Sanitise and/or wash your hands regularly.
All persons over the age of 60 should also register to be vaccinated via the national Electronic Vaccination Data System – some vaccine sites are also accepting walk-ins for people over the age of 60.
Act responsibly
We have also been notified that some members of our community are not being honest when completing the LogBox screening app, and that they are reporting for duty or class, even when they suspect that they may be infected. Others are not wearing masks and are not abiding by the COVID-19 protocols. This endangers other members of the Wits community and puts everyone at risk.
High and low risk contact exposure
The Occupational Health and Safety Office has been inundated with queries from lecturers, managers and Heads of School seeking advice on how to deal with staff or students who may have been exposed to a person who has tested positive for the coronavirus.
The OHSE Office has provided the following instructions as outlined in the Wits COVID-19 Handbook, which must be followed:
If someone who tested positive for COVID-19 was at work 10 days prior to testing positive, then the person’s line manager, lecturer or supervisor must determine whether anyone was exposed or in contact with the infected person. If this is the case, then they must determine whether the contact or exposure was high-risk or low-risk.
Low-risk contact exposureare instances where there was no direct face to face contact with the infected person, where all persons were wearing masks properly, where there was a distance of at least 1.5 meters, and where the contact was for less than 15 minutes. For low-risk contact exposures, people can continue coming onto campus while following all the COVID-19 protocols.
High-risk contact exposure are instances where there was direct face to face contact with an infected person, where people were not wearing masks properly, where people may have been standing within a 1.5-meter radius for more than 15 minutes and the contact was indoors (for example, they were sharing an office). High risk contacts must self-quarantine for the prescribed period of 10 days (unless a PCR test after Day 5 is negative), even if not positively diagnosed. These contacts must carry out daily self-screening to check for symptoms and signs of illness. If these contacts develop COVID-19 symptoms, the protocols for managing COVID-19 cases applies.
Reporting employee COVID-19 infections
All COVID-19 infections must be reported, irrespective of whether the infection was contracted at Wits or at home. There are prompts in the reporting forms that advise managers, supervisors, and lecturers on steps to take and University entities that must be contacted. The necessary forms can be obtained from Ntabiseng.Nzimande@wits.ac.za or by calling 011 717 9064.
If an employee who tested positive for COVID-19 was on campus within a period of 10 days prior to testing positive, then the person’s line manager, lecturer or supervisor is legally obligated to investigate the matter and to determine:
whether any additional controls need to be implemented,
if the infection arose out of or in connection with the persons employment (i.e. is it a work-related infection which was contracted during his / her day to day activities at the University). The investigation must be completed on the prescribed COVID-19 investigation form and be sent to Ramakoae@wits.ac.za and Dept-OHS-Admin@wits.ac.za
If the infection arose out of or in connection with the employee’s employment, then the necessary IOD forms must also be completed and sent to Ramakoae@wits.ac.za and Dept-OHS-Admin@wits.ac.za. This is to ensure that a compensation claim is submitted to the Compensation Commissioner as prescribed by the COVID Act and other Government COVID-19 protocols.
Reporting student COVID-19 infections
For student infections, please send the completed prescribed student reporting form to Anna.Moloi@wits.ac.za.
Steps to follow if a student or employee tests positive for COVID-19
If a student or employee tests positive for COVID-19, the following actions should be followed:
Infected person: The employee or student must self-isolate and contact their manager, lecturer or supervisor. If symptoms get worse the infected employee or student must immediately contact a healthcare worker or medical practitioner for further advice. The infected person must not access campus for at least 10 days after being diagnosed. If no COVID-19 complications are experienced, then the employee or student must self-isolate for a minimum period of at least 10 days prior to returning to campus. The infected person’s supervisor, lecturer or manager must determine whether the infected person may potentially have exposed other persons in the workplace or class, and, if so, must contact them to let them know that they may have been potentially exposed to someone (do not share the person’s name) that has been positively diagnosed with COVID-19. High risk contacts must be informed that they should self-quarantine for 10 days.
Cleaning of spaces: As the risk of infection from contaminated surfaces is low, there is no reason for the closure of buildings or office spaces. The place where an infected case might have been present should be well ventilated and the usual cleaning processes should take place. There is no need for deep cleaning or fumigation (which could in fact be harmful).
Protection Services: The supervisor, manager or lecturer must provide Campus Protection Services (Gary Kruser / John Sibisi) with the employee or student number of the infected person and all those who are required to self-quarantine. The access cards of these persons will be temporarily blocked.
Campus Health and Wellness Centre: The supervisor, lecturer or manager must also provide Sister Maggie at the Campus Health and Wellness Centre with the names and contact numbers of the infected person and people who must self-quarantine.
Return to Campus: After completing the quarantine period, the person may return to campus and student or staff cards can then be reactivated.
A detailed step-by-step procedure is available in the Wits COVID-19 Handbook via the Wits Coronavirus Portal. Log in using your Wits username and password. You can also contact your respective Occupational Health and Safety Officer for more information.
Covid-19 Update 68: Implications of level 4 regulations on Witsies
- VCO
What the new regulations mean for Wits staff and students.
President Cyril Ramaphosa announced last night that South Africa has moved to Lockdown Level 4, due to the highly infectious Delta variant of the coronavirus spreading quickly across the country, particularly in Gauteng. In his speech, he indicated that new curfews are in place (9pm to 4am), that there are further restrictions on movement, both within and beyond the province, and that there are implications for students and employees, amongst other matters.
The regulations have been released and the implications for Wits students and employees are detailed below.
Teaching and learning (Undergraduates)
All faculties have completed teaching and learning for the second term, and the University is now in the assessment period until the 9th of July 2021.
The vacation period commences from the 10th of July until the 1st of August 2021 and the third term begins on the 2nd of August 2021.
The implications for the teaching and learning programme, and assessments in particular, at the undergraduate level are as follows:
All online assessments will continue as scheduled.
All in-person examinations will either transition to online or will be postponed to August 2021, as communicated by faculties.
Faculties may be allowed to adjust the teaching and learning timetable to ensure that the 2021 academic programme is optimised, that valuable learning time is not lost, and that we endeavour to complete the 2021 academic year timeously.
Students living in Wits residences
We are waiting for the announcement from the Minister of Higher Education and Training in respect of the impact of the amended lockdown status on university residences. In the meantime, the normal mid-year policies and processes for residences will apply. The rules for those living in residences are also being amended in line with the lockdown level 4 status of the country. Students who may have specific concerns are encouraged to contact their cluster managers or the Director of Campus Housing and Residence Life.
Students who require permits to travel home and to return before the third term commences, can request permits from their respective faculties.
Researchers, postdoctoral fellows, and postgraduate students
Postgraduate students, postdoctoral fellows and researchers can continue with research, if they adhere to all Wits’ COVID-19 protocols. Postgraduate students with 12-month residence agreements are allowed to remain in residences. The same applies to students serving on our various clinical training platforms. Libraries will closed as we have to abide by the regulations issued by government in this regard.
Employees
Senior Executives will work with their respective Heads of School and Department Managers to determine the level of staffing required on campus to ensure that the University remains operational while the risk of infection in the workplace is minimised. Managers need to ensure that all relevant COVID-19 health and safety protocols are implemented in the workplace.
Where feasible, staff members may work from home, with the permission of their line managers, and with the approval of the relevant Senior Executive.
All meetings will take place online, as far as possible.
Conclusion
We are doing our best to ensure that everyone remains safe, whilst the University remains operational. We thank you for your resilience during this difficult period and urge you to abide by all COVID-19 protocols.
Level 4 COVID-19 lockdown puts spotlight back on vaccination failures
- Shabir A. Madhi
South Africa didn't engage early enough with pharmaceutical companies in bilateral discussions to ensure it could get vaccines early.
South Africa is in the grip of another resurgence of COVID-19. Gauteng province, the country’s economic hub, where 25% of the population live, is the epicentre. But infection rates are expected to rise in other major provinces as well. To ease pressure on the health system and slow the rate of transmission, President Cyril Ramaphosa recently announced tighter lockdown restrictions. Shabir Madhi is the director of the South African Medical Research Council Vaccines and Infectious Diseases Analytics Research Unit and co-founder and co-director of the African Leadership Initiative for Vaccinology Expertise at the University of the Witwatersrand. He spoke to The Conversation Africa to shed some light on South Africa’s situation.
How bad is the situation?
Based on the limited sequencing that’s been done, it appears that the Delta variant has emerged as the dominant variant in the latest resurgence. According to the latest research, it is much more transmissible and possibly also more virulent compared to previous variants.
The previous COVID-19 resurgence, which peaked in January 2021, was dominated by the Beta variant.
The current resurgence in South Africa differs by province, and even within a particular province. Gauteng, the country’s economic hub and one of nine provinces, is probably two to three weeks ahead of what will likely be experienced particularly in the Western Cape, Eastern Cape and Kwazulu Natal provinces.
In Gauteng the data show that the daily rate of COVID-19 infections in the current wave is two and a half times higher than at the peak of the first or second wave. Unfortunately, President Cyril Ramaphosa’s announcement on Sunday of stricter lockdown measures is unlikely to stop the trend.
We are likely to see many more COVID-19 cases being hospitalised as well as people dying from COVID-19 in the next two to three weeks in Gauteng. This is because severe disease usually lags behind infections in the community by about two to three weeks.
But, looking at the trajectory of the outbreak in India, we can expect the number of cases to start gradually decreasing after that.
To a large extent it depends on whether people adhere to the regulations, particularly avoiding indoor gatherings in poorly ventilated spaces and ensuring they wear face masks when indoors or in crowded spaces.
What is your biggest concern?
We’ve simply failed the people of South Africa by not ensuring that they were timeously vaccinated. The vaccine programme that’s under way has struggled to meet even the revised targets set by the National Department of Health. To date, under 5% of South Africans have been vaccinated, including less than one-third of those older than 60 years who were targeted to be vaccinated by the end of June 2021.
Constraints in supply of vaccines have obviously been a challenge. Countries like South Africa have been unable to gain access to adequate numbers of COVID-19 vaccines. This has been due to the inequitable distribution of vaccines around the world.
These failures, however, also speak partly to lack of planning. South Africa didn’t engage early enough with pharmaceutical companies in bilateral discussions to ensure it could get vaccines early. It only started earnestly engaging with companies in January this year. This simply put it at the back of the queue.
But equally important have been the impediments in allowing easy access and inadequate community mobilisation, particularly of the targeted high-risk groups. This has held back the rapid scaling-up of vaccination.
Had we vaccinated high risk individuals above the age of 60, as well as others with other comorbidities before the onset of the current resurgence, the number of people being admitted to hospital, and the number of people dying, would have been reduced significantly.
That’s been the biggest disappointment.
There were a series of other miscalculations too.
One was around deployment of vaccines. People were asked to register on the electronic vaccination data system, an online portal to manage the COVID-19 vaccine rollout. All this did was exacerbate the inequity that exists in the country when it comes to healthcare. The demographics of those who have been vaccinated indicate that people on medical aid schemes (and likely from higher socio-economic groups) are more likely to have been vaccinated. This comes as little surprise considering their greater ability to register on the electronic data system, as well as more opportunities to be vaccinated in private and public facilities.
The system looked good on paper. But it is simply not doing what it was intended to do – to get as many people vaccinated as possible.
Furthermore, it appears that less than two thirds of the COVID-19 vaccines that had arrived in the country by mid-June have been used. Since then a few million more have reportedly landed.
This tells us that the country simply hasn’t sorted out the logistics to ensure that it can get vaccines into the arms of people as quickly as possible.
Another major setback was the debacle around the AstraZeneca vaccine. In January a South African study – which I led – showed that the vaccine didn’t protect against mild or moderate COVID-19 due to the Beta variant.
The World Health Organisation (WHO) looked at all the available data following the study, and recommended that even countries such as South Africa where the Beta variant was dominant should continue using the AstraZeneca vaccine because it was likely to protect against severe disease due to the Beta variant.
But a decision was taken by the government to ignore the WHO guidance.
The result was that South Africa chose to sell the 1.5 million doses it had secured from the Serum Institute of India to other countries through the African Union.
Six months later there’s even more evidence that the AstraZeneca vaccine would probably protect against severe COVID-19 due to the Beta variant and works extremely well against the Delta variant.
The study that showed that the vaccine didn’t protect against mild to moderate COVID-19 due to the Beta variant didn’t mean that the vaccine wouldn’t necessarily protect against severe COVID-19 due to the Beta variant. Which is why the WHO made its recommendation – a view I supported. The government’s decision dramatically set back the country’s vaccination programme.
As it happens, the effectiveness of the AstraZeneca vaccine against the Delta variant for hospitalisation is 75% after the first dose – and 92% after the second dose.
What should be done?
We need to ensure that we get as many people vaccinated as quickly as possible.
In my view we shouldn’t be trying to focus on getting a second dose of the Pfizer vaccine into people who have already received a single dose. We need to ensure that we get as many people as possible above the age of 60, and those above the age of 40 with underlying medical conditions, vaccinated.
A single dose of the Pfizer vaccine has been shown to have more than 90% protection against hospitalisation due to the Delta variant. With two doses of the Pfizer vaccine that goes up to 96%.
And we need to ensure that we use the 4 million doses of vaccine the country has in the space of the next two weeks, and not two months. That is what we need to focus on. Unfortunately, the rollout of COVID-19 vaccines is already too late to reduce hospitalisation and death due to the current resurgence in Gauteng, but could still be useful for those provinces that are at an earlier stage of the current resurgence.
Professor Audrey Msimanga, the Head of the Wits School of Education, has passed away.
We learnt today of the passing of Professor Audrey Msimanga, the Head of the Wits School of Education, who did not recover from her illness after contracting the coronavirus.
Our heartfelt condolences are extended to Professor Msimanga’s family, colleagues, and students during this very difficult time.
A leader in teacher education, Professor Msimanga was appointed as the Head of the School of Education in February this year. Prior to this she served as the Head of the School of Education at Sol Plaatje University for two years.
But Professor Msimanga was not new to Wits. She first joined Wits as a Lecturer in Science Education in 2007, progressing to Senior Lecturer in the Wits School of Education. Her PhD in science education followed, and her Postgraduate Certificate in Education. She also served as the Academic Head for Postgraduate Studies in the School from 2014 to 2019 while working as a Senior Lecturer.
Respected by her postgraduate students, Professor Msimanga taught courses to Master of Science and Master of Education students and supervised postgraduate student research at all levels. Her own research focused on the curriculum-pedagogy interface, with the goal of understanding how science can best be taught locally in contexts of teacher and learner diversity and multilingualism. She was widely published in local and international journals and well represented at local and international conferences.
A trained ornithologist, Professor Msimanga’s specialisation in science education stemmed from the grounding that she obtained through her Master’s degree in Zoology (University of KwaZulu-Natal), her BSc Honours in Biological Sciences (University of Zimbabwe) and her BSc in Botany and Zoology (University of Zimbabwe). She served as a Curator of Ornithology at the Natural History Museum in Zimbabwe for several years and taught for five and three years at the University of Botswana and Solusi University, respectively. She also spent six years as an educator in two high schools, which she thoroughly enjoyed.
The Chair of the Research Capacity Building Committee of the Southern African Association for Research in Mathematics, Science and Technology Education, Professor Msimanga served on several research and academic bodies, including as the Associate Editor of the Journal of Research in Science Teaching.
Professor Msimanga firmly believed that education is a great equaliser and that a good education can open doors and provide the skills and competencies for employment or entrepreneurship. She encouraged her students to never stop learning and to empower themselves to empower others.
We have lost a great leader in teacher and science education today.
Dear Audrey, you have done much to empower many generations of young people, who will walk in your footsteps and realise their potential because of your extraordinary efforts. May your soul rest in peace.
SENIOR EXECUTIVE TEAM
30 JUNE 2021
The Delta variant and South Africa’s vaccination problems
- Ozayr Patel with Shabir A. Madhi
Pasha 113: The Covid-19 resurgence in South Africa is likely to take a heavy toll. It is important for vaccination efforts to be ramped up.
The Delta variant of SARS-COV-2 – the virus that causes Covid-19 – is spreading across South Africa, sparking a strong resurgence of infections. The president has placed the country under stricter regulations in an attempt to curb the spread of the virus. Gauteng province, the country’s economic hub, where 25% of the population live, is the epicentre. It’s likely many more people will be hospitalised in the coming weeks and some will die. Severe disease usually lags behind infections in the community by about two to three weeks.
Based on what happened in India, the number of cases is expected to decrease gradually. That is dependent on people adhering to lockdown restrictions. And South Africa’s vaccination strategy needs to be reviewed. In today’s episode of Pasha, Shabir A. Madhi, a professor of vaccinology and director of the SAMRC Vaccines and Infectious Diseases Analytical Research Unit at the University of the Witwatersrand, discusses the flaws in South Africa’s vaccine rollout.
South Africa’s vaccine quagmire, and what needs to be done now
- Alex van den Heever, Imraan Valodia, Martin Veller, Shabir A. Madhi and Francois Venter
South Africa has clearly suffered the consequences of poor strategic decisions to this point. It doesn't need to continue along these lines.
South Africa’s approach to its COVID-19 vaccine programme has been characterised by a large number of missteps. In aggregate it has left the country behind many others on the continent, and essentially left millions unvaccinated as a savage third wave descends on the country.
This has happened despite an established vaccine procurement and distribution network, access to the first large batch of vaccines on the continent, and a large number of pandemic and vaccine experts.
As the country battles a severe third wave crisis, at great cost to health, economy and society, the rollout of a vaccine programme remains the only sustainable means to protect the population against COVID-19 severe disease and death and return to some level of acceptable economic activity.
Strategically, therefore, policy needs to be hyper-focused on the delivery of a responsive vaccine programme to protect especially high risk groups against severe disease and death.
In this article, we outline the history of the vaccine strategy and its pitfalls. We also suggest a way forward.
Some context
As the pandemic first unfolded South Africa had, from a vaccine perspective, a number of things going for it. It has a large childhood vaccine programme although with weaknesses in overall coverage. It also has a private sector able to distribute adult vaccines, and experience of rolling out large programmes, such as antiretrovirals.
While reeling from a devastating first wave and associated lockdown in this period, the country was well poised to rapidly implement a mass vaccine programme.
In September 2020, for instance, a vaccine subgroup (the MAC Vac) of the Ministerial Advisory Committee on COVID-19 (MAC) was set up. It was made up of a small group of virologists, regulators and other public entities. It recommended supporting COVAX, a pooled procurement and distribution initiative aimed at securing large volumes of vaccines for countries that might struggle with bilateral agreements.
But during early December 2020 it became worryingly clear that government had no vaccine strategy at any level of maturity apart from the fragile COVAX arrangement.
To quote the deputy director general of the Department of Health, Dr Anban Pillay:
We have not delayed the procurement at all. We took a decision at the time we will go to (sic) COVAX facility because COVAX was purchasing vaccine (sic) from multiple vaccine producers, rather than taking the risk and going with one vaccine supplier.
Despite also asserting that individual companies had in fact been approached, there was no evidence of this, including within the publicly released MAC Vac advisories.
In late June 2021 the first 1.4 million doses of Pfizer vaccine were finally delivered to South Africa through the COVAX facility. It still remains unclear what will be delivered of the roughly 10.6 million doses still owed to South Africa during 2021.
As no signs of a coherent strategy by the government were surfacing, a group of academics drafted a 10-point vaccine strategy in early December 2020 to prompt a strategic response from government.
But no strategy emerged during that month.
January – February 2021
In frustration a group of South Africa’s health academics and activists published an article in early January 2021 condemning the absence of a vaccine strategy. They raised the concern that South Africa would enter the winter wave of SARS-CoV-2 infections without a significant part of the population vaccinated against infection or severe illness.
The article provoked a response. The health minister called a news conference, announcing that a strategy would be forthcoming and that confidential bilateral negotiations were in fact under way.
He failed to disclose any details.
A day later, on 4 January 2021, the Department of Health for the first time began belated bilateral negotiations of any seriousness with the Serum Institute of India for whatever doses they could make available of the AstraZeneca vaccine.
Within a week a commitment of some 1.5 million doses was made for delivery during February and March, with the potential option to purchase another 1.5 million.
This revealed what was possible if government began to act with purpose.
Also, within a relatively short period, an application for registration was submitted to the South African Health Products Regulatory Authority and emergency approval provided.
However, there was no rollout strategy, with no vaccine sites or registration system to manage the process. The first AstraZeneca vaccine batch then arrived on 1 February 2021 with much fanfare and was immediately transferred to the Free State for quality assurance.
As there was no other commitment to purchase, until this period no other vaccines were being evaluated by the regulatory authority apart from a rolling application by Johnson & Johnson. And as government had indicated it would be the sole purchaser and distributor of COVID-19 vaccines, no other party had applied for registration.
Despite the rolling application, the Aspen facility in Gqeberha was set to fill and finish 300 million doses of Johnson & Johnson vaccine in 2021. But there were no plans to use these in South Africa as the government appeared to show little interest up to that point.
Aspen confirmed it had the capacity to make up to 300 million doses of the vaccine, in a Port Elizabeth plant, and that all those doses would be earmarked for export.
Confusion then ensued when the health minister announced that due to the AstraZeneca vaccine not demonstrating efficacy against mild to moderate COVID-19 against what is now referred to as the Beta variant in the small South African AstraZeneca trial, the rollout of the vaccine was put on ice. The decision was criticised by local scientists, and not supported by the World Health Organisation.
March 2021
Due to the intervention of researchers involved in the Johnson & Johnson vaccine trial in South Africa a workaround was quickly negotiated for 500,000 trial doses to be made available. These would be prioritised for health workers with implementation in March 2021.
However, this was an expanded observational trial (Sisonke trial), not a rollout. It could only rely on trial sites for expansion, severely restricting the scaling up of the programme.
Nevertheless, the Sisonke workaround was a local initiative that spared the lives of many frontline health workers.
April 2021
The minister of health then controversially chose to discard the initial one million AstraZeneca doses rather than use them. It is our understanding that this was based on the MAC VaC advice.
He also took a decision to forgo the additional doses that would have been made available from the Serum Institute of India in terms of both bilateral agreements and the first round of COVAX. This was despite the World Health Organisation position that while not effective against infection by the Beta variant, it would be effective against the original wild-type variant still prevalent in South Africa and would probably offer protection against severe illness due to the Beta variant, which was subsequently corroborated in animal model studies. The protection against Beta-variant severe COVID-19 in the animal model study was evident despite the low levels of neutralising antibody induced by the AstraZeneca vaccines against the Beta variant, indicating such protection is likely mediated by CD4+ and CD8+ cellular immune responses that are largely unaffected even due to mutations in the Beta variant.
A number of experts were critical of this decision. They argued that South Africa should urgently use all available vaccines.
The minister also indicated that South Africa would not make use of NOVAVAX either, despite it being the only vaccine shown to protect against mild to moderate COVID-19 from the Beta variant and considered in the same league as the mRNA vaccines for efficacy against severe COVID-19. No evidence was offered for the decision.
The AstraZeneca decision effectively knocked South Africa out of the running for the first round of COVAX doses, which were made up of AstraZeneca (237 million doses) and some Pfizer (1.2 million doses).
The decision not to pursue the NOVAVAX vaccine potentially explains why they did not seek authorisation through the South African Health Products Regulatory Authority.
While the South African government did begin to take bilateral contracts seriously, our understanding is that substantial negotiations with Johnson & Johnson and Pfizer only began from February 2021.
This guaranteed that South Africa would face a winter wave of the epidemic with most of the 17 million or so high risk population unvaccinated.
The bilateral negotiations bore fruit with both Johnson & Johnson and Pfizer making significant commitments. But delivery was to be spread out intermittently through the remainder of the year – largely missing the predicted winter wave.
May – July 2021
South Africa officially started its rollout in May 2021 with Pfizer. But it did so with limited sites.
Expansion to scale is now restricted by the availability of doses rather than the ability to expand the number of sites.
The achievement of scale during June was then scuppered by the Federal Drug Administration’s (FDA) determination that the very 2.2 million initial Johnson & Johnson doses earmarked for South Africa by Aspen were contaminated and needed to be destroyed.
Despite the very long lead time to this decision, no apparent contingency arrangements were negotiated in the meantime. This resulted in a scramble to compensate for the failure of Johnson & Johnson to deliver on time.
Although replacement doses were subsequently made available, South Africa’s already belated vaccination drive was substantially diminished.
By the end of June 2021 South Africa had administered only 3 million doses, 480,000 of which were from Johnson & Johnson through the Sisonke trial and the remaining 2.2 million from Pfizer.
The end of June target for vaccinations was however 5 million outside of the Sisonke trial. Going into July 2021 South Africa should therefore have stock of around 4.3 million doses available if the 6.5 million doses promised by the end of June have arrived.
However, this stock is largely due to the slow pace of vaccinations. We should have had only around 1.7 million doses available at the end of June if everything had gone according to plan.
The bungling continues. Vaccines have moved up to around 100,000 doses administered per day. But, inexplicably, virtually no vaccinations occur over weekends at the majority of sites. And government has not made arrangements for non medical scheme members to make use of private sector vaccination sites.
What has been learned?
Without a proactive strategy government will perpetually respond to events. Any reasonable strategy must account for contingencies.
What could go wrong? What is not yet known for certain but may be true?
This requires combining evidence with hedging decisions for unknowns where no evidence is yet available.
In this pandemic, as in many other aspects of government policy, decisions have to be made even when perfect information is unavailable.
With this in mind four strategic errors were made.
First, vaccine nationalism was plainly the greatest risk to securing doses in late 2020. Without timely and assertive bilateral contracting beyond COVAX it was guaranteed that South Africa would be at the back of the international queue when it began to realise its mistake.
Second, low vaccine efficacy, especially when confronted with variants, is a contingent risk you have to mitigate through careful vaccine candidate selection (for procurement) together with diversification – booking multiple candidates. This includes the advance contracting of booster doses updated for variants of concern.
Third, the ground-game – or rollout process – requires advance preparation to rapidly achieve scale. However, scaling up requires that you start early and learn from mistakes. South Africa has started. Finally. But it is nowhere near the levels required before the winter wave of infections.
Fourth, a substantial winter third wave was predictable and every effort was required to vaccinate the high risk population, particularly for those over the age of 60 and with co-morbidities, by May 2021 with at least one dose of a vaccine that could prevent severe illness. South Africa unfortunately gave this option away despite a contingent probability that AstraZeneca vaccinations would protect against severe COVID-19.
A look at the strategy for 2022?
South Africa has clearly suffered the consequences of poor strategic decisions to this point. It doesn’t need to continue along these lines.
But strategy going forward needs to account for three key factors.
First, from the end of July 2021 many of the advanced countries will have surplus doses and are likely to shift their focus to updated vaccines that address variants of concern. It is therefore probable that the COVID-19 vaccine world will be characterised by a simultaneous glut of original vaccines and constrained supplies of updated booster shots.
Second, global herd immunity, even though an aspirational goal, is unlikely to materialise with the current generation of COVID-19 vaccines and the ongoing evolution of the virus. Instead the objective should be centred on protecting against severe illness and death despite ongoing transmission. One possible contingency is that a single complete mass vaccination programme permanently reduces COVID-19 to a mild illness – with ongoing infections acting as a booster to immune responses. The alternative, less likely contingency is that new variants emerge that evade even natural infection and vaccine induced immunity against severe illness. Both contingencies need to be prepared for.
Third, the pace of vaccinations remains constrained by access to doses rather than the capability of the public and private health systems to administer vaccines. Addressing these supply constraints is therefore a priority.
Taking account of these factors, the following four considerations should form part of the strategy for 2021 and into 2022:
First, bilateral negotiations need to be assertively pursued despite the doses already booked. These should focus on the more effective vaccines that are likely to move into surplus during the latter part of 2021 and into 2022. Therefore negotiations need to be ongoing with proactive procurement for both 2021 and the whole of 2022.
Second, South Africa should be advance purchasing the updated vaccines which could have higher effectiveness against the variants of concern. These should include agreements well into 2022.
Third, rather than advance purchasing too few doses, or just enough, consideration should be given to purchasing more than is required. This would cater for the contingent risk of ongoing transmission resulting in severe illness in the vaccinated population.
It would be a mistake for South Africa to again take its foot off the pedal when the opportunities for bilateral contracting are increasing. But the window for astute early action is closing.
Fourth, and more generally, greater transparency in strategy, implementation, and the strategic rationale for decisions is required, given the importance these decisions hold for the well-being of the country.
Healthcare in South Africa: how inequity is contributing to inefficiency
- Russell Rensburg
Patients shouldn't be treated better simply because they can afford to pay more.
South Africa has a two-tiered, and highly unequal, healthcare system. The public sector is state-funded and caters to the majority – 71% – of the population. The private sector is largely funded through individual contributions to medical aid schemes or health insurance, and serves around 27% of the population. The public sector is underfunded while most South Africans can’t afford the exorbitant cost of private care. To balance the scales, the government tabled the National Health Insurance Scheme. The proposal was to provide universal healthcare by buying services from health professionals through a National Health Insurance Fund. These services would then be delivered at private and public facilities. But there are many unanswered questions about how exactly this scheme will work and many doubts about it. Russell Rensburg is the director of the Rural Health Advocacy Project, which champions equitable access to quality healthcare for the country’s rural communities. He shares with The Conversation Africa how the gaps may be plugged.
What has the pandemic exposed about South Africa’s healthcare system?
Firstly, South Africa’s biggest problem is that the health needs of its people exceeds capacity.
Secondly, the vast majority of people actually don’t know their health status which delays access to care.
Thirdly, the way the system is funded perpetuates inequality.
What are the solutions?
There’s a massive opportunity to reform the system. The biggest lesson that’s been learned from COVID-19 is that if there is poor health utilisation at the lower levels, people are at increased risk of severe illness and death due to COVID-19. Comorbidities are a risk factor for COVID-19. If the health sector did a better job of diagnosing and treating people living with diabetes at the community level, for example, the outcomes would be better.
If the country had a strong primary health care network with competent well trained community health workers, it would have had a better chance of containing the spread of COVID-19 as well as linking people to care sooner so that deaths could be reduced.
We also need to look at the efficiencies of hospitals. Some fundamental questions need to be asked, such as are we doing the work that should be done in a hospital? Yes, it’s hard to turn people away. But so much is being done poorly in public sector hospitals. Many are falling apart.
Another area that needs close attention is explicit prioritisation. Given the levels of poverty and inequality in the country, there should be explicit priority setting in determining who accesses key services such as surgery and when. Who benefits from that at the moment? Is access based on how close someone is to the system? For example, people who live in Cape Town or Johannesburg have a better chance of getting an elective surgery like a hernia repair.
The World Health Organisation says those people with the least coverage need to be prioritised before expanding access to others with more access to care. While everyone has the right to health, there is not equal enjoyment of that right. For example in the current response to COVID-19 how quickly people can access testing, care or even vaccination is determined by their ability to pay. This is neither just nor fair.
As the country considers the development of a comprehensive primary health care package, it should look at prioritising services where lower income groups enjoy the least access.
South Africa should also consider a universal pricing and admission criteria.
Access to medical schemes shouldn’t lead to over-enjoyment of capacity. The Competition Commission conducted a five-year investigation into the country’s private health sector. One of its findings was that South Africa admitted more people to ICU that other countries with comparable data.
Patients shouldn’t be treated better simply because they can afford to pay more. The high cost of private care has detrimental effects on public health care. If most doctors work in the private sector, there will be a limited number of doctors working in the public sector. These two markets affect each other. If the cost of private healthcare isn’t reduced, the costs will increase for everyone. Which means that the public health sector will suffer over the long term as it struggles to keep up with the cost of care.
How should South Africa manage the unequal nature of healthcare provision?
The country has to find a way to make sure the availability of care is spread more evenly throughout the system. We can’t look at the private and public sectors separately. One has an impact on the other.
South Africa’s healthcare system is inefficient – both public and private. The cost of healthcare is too high. In the long term, improving the quality of care in the public sector would balance out people’s need to have expensive medical insurance.
South Africa’s institutional frameworks perpetuate inequality, rather than address it. Publicly-funded healthcare is not allocated based on need, but determined by each province’s relative share of the population. In this scenario, funding for the Western Cape and Eastern Cape provinces would be roughly same – despite vastly different implementation context. When you consider the vast area covered by the Eastern Cape, it is clear the current arrangements do not address inequality of access.
When health services were officially desegregated in 1988, South Africa’s spending in the former mainly white provinces was R172 average per capita. Public sector healthcare expenditure was R55 in areas designated under apartheid for black people. Known as the “homelands”, it’s where most black South Africans were forced to live.
Many of these inequities have persisted with a disproportionate spend on health infrastucture in large metropolitan areas. This has lead to an under investment in primary health care where the 80% access services.
The system needs to be more responsive at the levels where the majority are likely to access it. This means moving services out of facilities and being proactive in engaging with people through lower level workers such as community health workers.
Doing this would easing the burden on facilities and health diagnose people at early stages of disease and infection – before they get sick.
South Africa has followed this approach with community testing of HIV. It saw also saw the effectiveness with the community screening and testing at the being of the COVID-19 pandemic in March 2020.
There are no simple solutions to South Africa’s health crisis but we have a once a generation opportunity to begin addressing the crisis . The improved electronic vaccine registration system can contribute to a better understanding of where people are, the investment in diagnostics can lay the platform for expanded screening and diagnostics and the introduction of reforms like the NHI can facilitate better cooperation between the public and private sector. Failure to act on these opportunities will show our disregard for the lives and living of the 80% of the population trapped in a poverty and under development.
Women suffered a large and disproportionate effect in the labour market as a result of the hard lockdown, but they’ve also been slower to recover.
With the release of the final wave of the Nids-Cram survey, we can take stock of how the Covid crisis has affected gender inequality one year on. The results are not encouraging.
Women suffered a large and disproportionate effect in the labour market as a result of the hard lockdown, but they’ve also been slower to recover. In March 2021, when the country was in its least restrictive lockdown, men’s employment and working hours were back to pre-Covid levels. Women’s employment was still down 8% against February 2020, and their working hours were down an average 6% (two hours a week).
So while there was a recovery in employment, it has been slower (and remains incomplete) for women. Covid has increased gender inequality in the labour market.
An important factor to consider is the gender split in job types. Women are more likely to be in the sectors hardest hit by the crisis. They are also in more precarious employment relationships, so it is easier for employers to reduce their employment or working hours when lockdown restrictions bite. This highlights the inequality that stems from job segregation and shows that policy to open opportunities for women in "male" sectors, and in more stable employment, needs to take centre stage.
Another likely reason for the uneven effect in the labour market is the uneven impact in the home. The Nids-Cram data shows that the burden of school closures has fallen disproportionately on women: twice as many women as men said child-care responsibilities during the lockdown affected their work prospects. Any serious attempts to close gender gaps in the labour market will need to address this inequality in the home.
An important finding is that even though women account for most of the unemployed and Covid-related job losses, they received the least state income support targeting unemployed and furloughed workers. Our data shows that only about a third of the recipients of the Unemployment Insurance Fund (UIF) temporary employer/employee relief scheme (Ters) and the special relief of distress (SRD) grant were women.
That fewer women received Ters benefits is because they are less likely to be (formally) employed and registered for UIF. However, fewer women received the SRD grant because it could not be paid concurrently with another grant, such as for child support. So unemployed women were penalised if they were also the main caregiver to a child.
If the SRD grant is reintroduced in future, this issue will need to be urgently revisited.
SA is well into its third, brutal wave of Covid, with tighter restrictions progressively reimposed since late May. But all state income support measures have been discontinued, with seemingly no intention to reintroduce them — despite the effect the new restrictions will undoubtedly have on employment. And, if past evidence is anything to go by, especially on the jobs of women.
The lack of additional income support when the pandemic is still raging is deeply worrying. Measures need to be reintroduced with urgency to help stave off the most devastating effects of this crisis.
Daniela Casale is with the Wits University School of Economics & Finance; Debra Shepherd is a member of Stellenbosch University’s Department of Economics. This article was first published in Financial Mail.
Spike in COVID-19 cases points to gaps in South Africa’s response
- Laetitia Rispel
Preventing new infections and containing the pandemic protects health systems from getting close to collapse.
The numbers of COVID-19 cases and deaths in South Africa have increased exponentially over the past 12 months. At the beginning of July 2020 the country had 168,000 cases of COVID-19 and 2,844 deaths. A year later, at the start of July 2021, there were over two million confirmed cases and more than 61,000 deaths. These numbers are only a snapshot of the kind of pressure South Africa’s healthcare system is under. On the one hand, the country needs to drastically increase the number of frontline health workers. And on the other hand, there’s not enough money, according to acting health minister Mmamoloko Kubayi, to employ medical interns, or even extra medical staff. Laetitia Rispel chaired the ministerial task team responsible for the development of the 2030 National Human Resources for Health Strategy. She spoke to The Conversation Africa’s Ina Skosana about the country’s COVID-19 response.
How is South Africa coping with the current wave?
The country is not coping. I think the third wave could have been avoided. There’s been a lot of focus on the vaccination programme. Although vaccination is important, you can’t look at the vaccination programme in isolation from the overall response to the pandemic.
Things could have been done differently.
First of all, the government declared COVID-19 a national disaster in March 2020. That was an opportunity for the National Department of Health to provide strong leadership for the entire health system. But the national department has either remained quiet, or played a supportive role to the pandemic response in the nine provinces. Consequently, the COVID-19 response has varied across the country. In a crisis like the pandemic, you need strong central leadership and management.
Second, there’s been a lot of attention on the ability of hospitals to cope. The first step of any public health response must be prevention. Preventing new infections and community transmission, and containing the pandemic protects health systems from being overwhelmed or getting close to collapse.
By the time hospitals are overwhelmed by people who need admission, it is almost too late. Gauteng is the epicentre of the current surge. The province’s early warning system showed increasing numbers weeks ahead of the surge. Yet very little was done to contain those infections, or prevent a rapid increase.
There has been insufficient involvement of civil society and ordinary community members.
There’s a certain degree of COVID-19 fatigue. But many people still don’t understand why non-pharmaceutical interventions – social distancing, hand washing, wearing masks – are important.
What are your biggest concerns?
There’s a chronic under-investment in the health workforce – the pandemic has exposed and amplified this. This is apparent in the reported shortages especially to deal with the people who are seriously ill and need to be admitted.
You can have as many hospital beds as you want. But if you don’t have the skilled staff to look after patients, then people won’t receive quality care or care at all.
There’s also been a failure to deal with the concerns and fears of frontline health workers. I don’t think there’s been sufficient attention to the psychosocial and emotional impact of the pandemic on these workers. The potential consequences are physical and mental exhaustion, stress, anxiety, and burnout. This could lead to medical errors, lower productivity, increased absenteeism and higher turnover, thus creating a vicious cycle.
What’s been working?
There are areas of innovation that we should recognise. For example government and South Africans were able to put together, at relatively short notice, significant financial resources. Digital innovation included the COVID-19 Alert App, the early warning system of hotspots or clusters of infections and the ability to get daily updates on COVID-19 infections and deaths.
One of the positive aspects was the “whole-of-government” approach and inter-governmental structures that were set up. These enabled different government departments and entities to work together, rather than in silos.
The other thing we have to acknowledge is the visible political leadership. There was very decisive leadership from the president at the early stages of the pandemic.
Hospital and district managers, as well as frontline staff, rescued the day. They went way beyond the call of duty. For instance, frontline nurses and doctors had creative ways of keeping communication going with family members who were not allowed to visit patients. There was a newfound public appreciation for frontline nurses and doctors.
I think the institutionalisation of public health measures is an amazing achievement. Wearing masks, handwashing and sanitising were adopted quite quickly. Compliance and enforcement, however, are still key issues.
What should be done?
The first thing is to strengthen and stabilise leadership and management. If people are in acting positions they are less likely to take risks and make tough decisions. Given the speed with which the pandemic is growing, it’s important to have rapid decision-making.
The second thing is to engage with and involve ordinary people. This can be done through existing community structures. South Africa can build on the experience of managing the HIV epidemic to get public buy-in. People must understand that it’s only through working together that we’ll be able to prevent new infections, contain the spread of infections, and save lives and protect our future.
The third point is the importance of investment in the health workforce. Without health workers it’s not possible to fight a pandemic, or have a functional health system.
Finally, it’s important to act on the data generated by information systems. What is the point of investing in health information systems when you don’t respond to the message? The government needs to take swift action at the first signs of hotspots and not wait for infections to spread.
Covid-19 vaccine research ALIVE and thriving at Wits
- Wits University
The Wits African Leadership in Vaccinology Expertise (ALIVE) has awarded research grants for cross-disciplinary Covid-19 vaccine-related projects.
ALIVE and the University Research Committee awarded funding to three Covid-19 vaccine-related projects during February and April 2021, in virology, human genetics, and public health respectively.
Investigating how the Covid-19 virus dodges human defences
As the Beta variant dominated Covid-19 infections in South Africa during the second wave and the Delta variant currently dominates the third wave, it is important to understand the impact of emerging variants on the current SARS-COV-2 vaccines available.
The SARS-CoV-2 spike protein is the main target of neutralizing antibodies. It’s this spike protein – the ‘corona’ crown of the virus – that facilitates entry into host cells and infection. This spike protein is also continually mutating and ‘escaping’ the antibody response that our bodies produce to fight off infection.
Understanding how this spike protein behaves as it mutates, and how this affects the antibodies we need, is important to vaccine design because these mutations may alter the effectiveness of vaccines and therapeutics currently in development.
Dr Thandeka Moyo-Gwete in Virology, School of Pathology at Wits and a Senior Medical Scientist in the Centre for HIV and STIs at the National Institute for Communicable Diseases leads a project on mapping SARS-CoV-2 spike determinants of escape from antibodies.
“This project harnesses our existing highly successful HIV-focused expertise and established methodologies in our lab to rapidly identify key viral mutations emerging in SARS-CoV-2 and to determine the neutralizing responses to these viral strains in the context of the Covid-19 epidemic in South Africa,” says Moyo-Gwete, whose research interests started in understanding the nature of broadly neutralizing antibodies that target HIV and HIV vaccine development.
The results from this study will provide insight into the effectiveness of SARS-CoV-2 vaccines in the presence of several viral variants circulating in South Africa.
This research grant facilitated the postgraduate work of Ms Bliss Musvosvi, an MSc (Med) Vaccinology candidate at Wits. “My goal is to serve and help achieve public health objectives through reduction in the mortality and morbidity of vaccine preventable diseases. Other areas of interest include vaccines for the prevention and control of emerging and re-emerging infectious diseases,” she says.
How does the genetic variation of South Africans influence Covid-19 infection and severity?
Michèle Ramsay, Director of the Sydney Brenner Institute for Molecular Bioscience (SBIMB) and Professor in the Division of Human Genetics at Wits, along with Dr June Fabian, nephrologist and Research Director at the Wits Donald Gordon Medical Centre (WDGMC) are co-Principal Investigators on the Host genomic susceptibility to COVID-19 in Black South Africans (COVIGen-SA) project.
The way an individual experiences and responds to Covid-19 differs from person to person; some people get severe disease, some die, and others present with very mild symptoms or are asymptomatic. These varying clinical outcomes are due partly to the genetic factors of the host (infected person).
Understanding how genetic variation affects the way people respond to Covid-19 could inform vaccine development, and improve disease management and therapeutics. Research studies in this area relate to the field of genomic medicine, where the approach to treatment is informed by the person’s genetic variation.
Globally, efforts are underway to describe the role that host genetic variation plays in infection by the novel coronavirus and progression to Covid-19. However, African populations are historically under-represented in global host genetic studies, and this threatens to worsen existing health inequalities.
The COVIGen-SA project is a unique and dedicated initiative to understand the role of host genetic factors in Black South Africans.
“Through collaborations, we aim to collect DNA samples from over 5000 Black South African participants, with varying Covid-19 disease severity. This will serve as a resource for current and future studies investigating the role of host genetics in Covid-19 and could inform more effective treatment and prevention strategies,” says Ramsay, who is a Research Chair on Genomics and Bioinformatics of African populations.
Dr Harriet Etheredge is a medical bioethicist and health communication specialist at the Wits Donald Gordon Medical Centre. She is responsible for implementing and overseeing a robust ethical and regulatory structure for COVIGen-SA.
Dr Andrew May, a postdoctoral fellow in the SBIMB will coordinate the COVIGen-SA project. May’s research interest is in how genetic variation impacts individual differences in health and behaviour.
Ms Heather Seymour will conduct doctoral research in the COVIGen-SA project. Her PhD in the SBIMB follows her MSc (Med) dissertation on Mutation profiling in South African patients with Cornelia De Lange syndrome phenotype using targeted next generation sequencing.
Covid-19 vaccine hesitancy among healthcare workers
Dr Janan Dietrich, Director of the Biobehavioural Research Centre in the Perinatal HIV Research Unit (PHRU), and Dr Fiona Scorgie, an anthropologist and Senior Researcher at the Wits Reproductive Health and HIV Institute (Wits RHI) are co-Principal Investigators on a study researching Covid-19 vaccine hesitancy amongst healthcare workers in South Africa.
In 2019, even before the Covid-19 pandemic, the World Health Organization identified vaccine hesitancy as one of the top 10 threats to global health. Now, evidence is emerging globally of vaccine hesitancy (delay or refusal of vaccination despite availability of vaccines) in relation to newly developed Covid-19 vaccines. Vaccine hesitancy has the potential to undermine vaccination efforts to bring the pandemic under control in South Africa.
Healthcare workers have been prioritized for vaccination in South Africa and are likely to be key in promoting vaccination amongst the public and countering misinformation about the vaccine. However, the attitudes of South African healthcare workers to Covid-19 vaccination have yet to be studied.
“We aim to explore knowledge and acceptability of Covid-19 vaccines among healthcare workers – both as recipients and providers of the vaccine – and to develop a novel method for addressing vaccine hesitancy in this population using AI [artificial intelligence] technology,” says Scorgie, a social anthropologist with expertise in vaccine acceptance and qualitative research.
The study combines multinational and complementary expertise across the social sciences, clinical trial expertise, digital health, AI, and biostatistics at Wits.
Data will be collected through a quantitative online survey, qualitative interviews, and a review of online vaccine sentiments. Categorised according to belief awareness; perceptions of vaccines; vaccine safety; and disease outbreaks, these data will inform the development of a targeted, vaccine-specific chat-bot to address vaccine hesitancy.
“Local online data will also be accessed with assistance from the Vaccine Confidence Project full-text media archive, and historical and real-time anonymized Google, Twitter and Facebook data via the Meltwater Social Media Monitoring platform,” says Dietrich, who is a research psychologist with experience in HIV vaccine research and digital health. “We envisage that the online chat-bot will address vaccine hesitancy by providing accurate, transparent information to healthcare workers and to members of the public.”
What last week’s vandalising of our research clinic in Kliptown, Soweto, means to science
Despite the critical role of the PHRU as part of the national and international Covid-19 response team, it was not spared during the recent unrest.
Loss of scientific equipment, research and infrastructure as well as threats to researchers’ safety compromises the ability to conduct the clinical research needed to address the pandemic and epidemics like HIV and TB.
More than 15 years ago, the Perinatal HIV Research Unit (PHRU) established its first adolescent and HIV research clinic in Kliptown, quite literally doing ground-breaking research on the ground. We chose Kliptown because of its historical significance as well as the desire to dignify this auspicious square with the clinical science that it deserved. Right across from our offices and clinic, 76 years ago, in this square now known as Walter Sisulu Square, the Freedom Charterwas signed, setting out the aspirations of the opponents of apartheid.
The Freedom Charter emphasised a non-racial society, liberty and individual rights. This Charter is seen by many as the foundation of South Africa’s 1996 constitution. In the spirit of this legacy, we established the Kliptown Research Clinic employing almost 50 people with more than 80% of employees living in the surrounding areas. We never lost sight of the significance of having our research site on the square.
Significant too, is the research we have done here, that has had a global impact. Established in 2008 as the Kganya Motsha (translated as “shine young one” in Sesotho) this site was the first in Soweto to provide youth-friendly HIV prevention, outreach, HIV testing services and psychosocial support to adolescents and young people. We extended this to doing medical research and exploring whether a gel containing an antiretroviral agent, tenofovir, could be used as a vaginal microbicide to avert HIV in young women.
We too have enrolled in pivotal HIV vaccine efficacy trials that contribute at a global level to the scientific assessment of what it will take to mount an immune response adequate enough to prevent HIV acquisition. Soweto is an HIV transmission hotspot and the most densely populated geographic location in South Africa. Given the high HIV prevalence and incidence, and lack of acceptable prevention modalities, a moderately efficacious preventative HIV vaccine or long-acting pre-exposure prophylaxis (PrEP) would be a critical contributor to ending the HIV pandemic. We are proudly trying to find the HIV holy grails, and our site is critical to this endeavour.
Although we have been part of the two most important and largest HIV vaccine trials in Africa, more recently and maybe more importantly, when Covid-19 struck our country, we rapidly availed ourselves to conduct the first-ever Covid-19 vaccine trials in South Africa. We were involved in the Chadox/Astra-Zeneca study that showed significantly reduced efficacy against the so-called South African or Beta variant.
We contributed to the selection of Covid-19 vaccine candidates for the South African national vaccine roll-out by implementing the Ensemble trial of J&J’s single-dose Ad26 vaccine. This trial was the precursor to Sisonke, the study which made 500,000 Ad26 vaccines available to healthcare workers as an implementation study when the government’s roll-out faltered. The Kliptown staff supported the vaccination drives at Chris Hani Baragwanath Academic Hospital and a private facility in Lenasia.
Our site, headed and run by a predominantly female team, has forged relationships with the tenants on the square and supported local entrepreneurs to ensure we can all co-exist and thrive together in the Kliptown community.
The Perinatal HIV Research Unit (PHRU) Centre entrance wall that was vandalised to gain entry to the clinic. (Photo: Anusha Nana)
Tragically, Walter Sisulu Square and the surrounding businesses were some of the worst-hit places in Gauteng during the recent violent and destructive riots. Shops and medical practices were looted, some burnt to the ground, and owners and tenants left destitute. Barely any of the tenants of the Square’s office building were left unscathed. Many of these businesses provided much-needed services to the community, including our clinic and neighbouring establishments such as New Heights which provide entrepreneurial and life skills courses witha special focus on women, youth and the unemployed.
Despite the critical role that we play as part of the local and international Covid-19 response team, our site was not spared during the riots. Opportunists broke into our main facility and stole all electronic equipment, including desktop computers, laptops, printers, mobile phones, televisions for participant education and a washing machine used to ensure sanitised staff scrubs.
They also took all our stethoscopes, blood pressure machines and space heaters. It will be difficult to restore the functioning of this once vibrant floor, as the taps stolen from the Square’s main restrooms and vandalised toilets have resulted in the water supply for the entire building having to be turned off.
With no water access and absolutely no ablution facilities in the entire building — a worrisome health hazard to the already traumatised tenants amid the third wave, this will impact on our ability to restore clinical research. Although we have suffered a chronic lack of access to adequate basic services to the building, we have always made a plan.
For example, the facility has been without electricity since 15 December 2020. We installed generators to run the research freezers and fridges in which the vaccines are stored but this came at an estimated cost of R4,000 a day in diesel. When nothing was done to rectify the situation, we were forced to hire private contractors to connect the site to the main power supply. However, we had to dip into the minimal resources that we had to do this and now do not have sufficient funds to extend this to the other tenants who remain without power.
Clinical science does not operate in a vacuum and is part of the ecosystem of communities. Loss of infrastructure and equipment, threats to researchers’ safety, and an inability to keep research clinics open in the field compromise our ability to do the clinical research needed to address this current pandemic and other pandemics or epidemics like HIV or TB. Loss of this ability makes us all the poorer.
So, despite all our challenges: looting, poor infrastructure support, security concerns, we are resilient and resourceful. We remain committed to Kliptown, because of our passion, a sense of community and love for the research we do. We will rebuild our site. Science can have setbacks, Kliptown can have setbacks, but our phoenix will rise again. Much like the phoenix — the long-lived bird that cyclically regenerates or is otherwise born again — we will obtain new life and will continue to make a global impact.
Anusha Nana, Erica Lazarus, Fatima Mayat and Ravindre Panchia are with the Perinatal HIV Research Unit, Faculty of Health Sciences, University of the Witwatersrand. Professor Glenda Gray is with the PHRU, the South African Medical Research Council and a Research Professor at Wits University. This article was first published in Daily Maverick/Maverick Citizen.
Covid-19 in children: the South African experience and way forward
- Tendesayi Kufa-Chakezha, Cheryl Cohen and Sibongile Walaza
Schools are not driving the COVID-19 pandemic and can safely remain open provided people stick to the non-pharmaceutical interventions for COVID-19 prevention.
Since its emergence in late 2019, SARS-CoV-2 has caused illness (COVID-19) and death in all countries in the world. The restrictions put in place to reduce the spread of this virus have devastated economies and livelihoods the world over. By the end of June 2021, the World Health Organisation estimated that there had been 180.4 million cases of COVID-19 and 3.9 million associated deaths globally.
From the outset, communities were concerned about the impact of SARS-CoV-2 on children. This was justifiable because many other respiratory viruses such as influenza and respiratory syncytial virus disproportionately affect children. With their immature and developing immune systems children have larger amounts of virus in their respiratory tract and release the virus from there for longer durations. This puts them at the centre of transmission of those viruses – to each other at schools and to adults and siblings at home. It was not surprising that early interventions to delay the spread of COVID-19 included shutting down schools.
But COVID-19 has bucked this trend of affecting children more than adults.
SARS-CoV-2 is known to infect children of all ages, from newborns to older adolescents and teens. But children have not been the drivers of the COVID-19 pandemic to date.
This is because children are less likely to:
be infected with the SARS-CoV-2 virus when exposed to it;
Our surveillance data in South Africa indicate that this lower risk of infection, disease, death or transmission experienced by children is age-dependent. Among children, the likelihood of infection, disease or death generally increases with age. Older teens and adolescents are acquiring COVID-19 at rates similar to adults in some instances. This routine surveillance has been in place since the beginning of the COVID-19 pandemic. The aim is to monitor disease trends in children and inform policy around prevention, care and treatment for children.
The South African experience
By mid-June 2021, South Africa had conducted 12.3 million tests and detected 1.8 million cases. Children 19 years or younger accounted for 13.4% of tests conducted, 10.2% of new cases reported, 4.2% of COVID-19 associated hospital admissions and 0.7% of COVID-19 associated deaths. This is despite children this age accounting for 36.6% of the South African population.
This age group was 3.7 times less likely to test for COVID-19, 5.7 times less likely to test positive for COVID-19, 13.3 times less likely to be admitted to hospital with COVID-19 and 6.7 times less likely to die in hospital once admitted compared to adults older than 19 years.
The data to date has not shown or suggested an association between case or admission rates with the opening and closing of schools in the country.
Given the adverse social and psychological impacts of closures on schools, it is encouraging to know that schools are not driving the COVID-19 pandemic. They can safely remain open provided there is implementation of and adherence to non-pharmaceutical interventions for COVID-19 prevention.
First, the increased case rates in older teens and adolescents, at rates similar to adults older than 19 years in the third wave, requires monitoring. Since the onset of the third wave to the peak, the fraction of all COVID-19 cases aged 19 years or younger was averaging 14.6% as opposed to around 9% in the first and second waves. Half of the cases were occurring in older teens and adolescents 15-19 years, bringing the case rate in this group on par with adults older than 19 years.
This could have been as a result of:
generally increased testing in children in the third wave. More testing would pick up more cases, including mild or asymptomatic ones.
increased testing in response to cluster outbreaks in schools, leading to more testing among symptomatic or mildly symptomatic children and adolescents
increasing vaccination rates among adults, leaving younger individuals contributing more cases; and
the Delta variant itself – which may have a greater predilection for children, although there is not yet any conclusive data to support this.
Second, infants under the age of one have experienced higher hospital admission rates compared to other children, especially after the second wave. In our most recent report, infants made up 2.2% of cases 19 years or younger but contributed 19.3% of the admissions and 31.8% of deaths in this group.
It is unclear why these infants are admitted to start with or what the causes of deaths are. Generally infants are much more likely to be admitted with non-COVID-19 conditions compared to older children. There is routine testing of all admissions at many hospitals, so it is possible that many of these admissions are for other reasons, with COVID-19 an incidental finding. More data are needed to investigate reasons for admission in this age group.
Lastly, children with underlying conditions made up 19.3% of children admitted with COVID-19 but 56% of those who died. The most commonly reported underlying conditions among those admitted were chronic respiratory diseases, diabetes, HIV and tuberculosis (active and previous). HIV, diabetes and tuberculosis were common among those who died.
What about vaccination?
South African children are not yet eligible for COVID-19 vaccination and may not be for a while. The reasons for this include the lower risk of disease and the need to prioritise the elderly; limited information on the efficacy and safety of the vaccines in children; and limited number of vaccines which are licensed for use in children.
Some countries in Europe and North America have opened up vaccination to children 12-16 years although coverage in this age group is still low. As more children are vaccinated in these countries, more data on side effects and effectiveness will be collected and many lessons to inform rollout in South Africa will be learnt.
In the South African setting, there is a case for the expedited vaccination of children with underlying conditions and older teens and adolescents based on burden of cases and hospitalisations in these two groups respectively.
Until then the onus is on everyone to ensure vaccination of adults around children to achieve herd immunity, and adherence to non-pharmaceutical intervention to reduce transmission in the community and spillover into schools.
Everything you need to know about vaccines — our only viable strategy for living with Covid-19
- Lucy Allais, Shabir Madhi, Imraan Valodia, Alex van den Heever, Martin Veller and Francois Venter
We are likely to keep being hit by further waves of this virus until at least all adults have immunity.
Our only hope for getting the pandemic under control is for as many people as possible to be vaccinated against it as quickly as possible.
Most importantly:
Vaccines will give you near-complete protection against severe illness and dying from Covid.
Vaccines are safe. All vaccines used in the vaccination programme in South Africa have undergone extensive trials and have been proven to be effective and safe.
The risk of serious side effects is similar to the chance of being struck by lightning, and side effects are treatable and generally go away on their own.
It takes time for vaccines to start working well — usually about two weeks, and their working steadily improves after this.
Vaccines differ in how well they protect against infection and mild Covid. Most vaccines will require at least two doses and provide good protection against severe illness from Covidtwo weeks after your first shot.Until you are fully vaccinated you should continue to take the same precautions as if you are unvaccinated.
Vaccines are our best hope in fighting Covid
Having caused at least four million recorded deaths worldwide, and probably almost200,000 excess deaths in South Africa(the official figure of 65,000 almost certainly understates the true picture, which is more accurately indicated by what is called “excess mortality’’), the Covid pandemic is one of the worst in history.
After 18 months of worldwide infection and deaths and with 10-15% of survivors experiencing the unpleasant “long Covid’’ symptoms, as well as severe social, economic, and educational disruption, it is clear that the novel coronavirus, SARS-CoV-2, which causes Covid-19, is not going to go away. But, as terrible as the pandemic has been, the good news is that a number of very effective vaccines have been developed.
As we can see from the devastating third wave South Africa has been reeling under, we are likely going to keep being hit by further waves of this virus that will cause further unnecessary suffering and death until at least all adults have immunity. Our only hope for getting the Covid pandemic and its severe health, social and economic consequences under control is for as many people as possible to be vaccinated against it as quickly as possible.
How do vaccines work?
Our bodies have many processes that detect and fight infection and disease: together these are called the immune system. When our bodies become infected, some cells figure out how to fight the infection, and if they are successful, and we survive, our bodies develop the memory of how to produce these cells that know how to fight this specific infection, usually far more efficiently and speedily the second and subsequent time round. This is called immunity.
Vaccinations are a way of triggering the body to develop an immune response to a particular disease without having to actually get the disease — a kind of fake first infection.
Traditionally, vaccines contain a component of the virus or other microorganism, or the organism in a weakened or killed state. The body then is able to recognise the virus when we are infected and respond to it, as if it was exposed the first time. The most recent mRNA technology, which is used in some of the latest vaccines, uses genetic material that tells our bodies to produce a protein of the virus which then stimulates the immune response.
Vaccines are one of the most successful, and safest, interventions medicine has ever come up with. They have eradicated dangerous infectious diseases such as smallpox, have controlled polio, and have saved billions of lives from measles, tetanus, pneumonia, hepatitis and diarrhoea. They have dramatically decreased viruses responsible for some cancers. They are also safe — bad side effects are very rare and the risk of developing severe illnesses is much smaller than the bad effects of the diseases the vaccines prevent.
Vaccines were not invented by Big Pharma and they are not unique to Western medicine — the first recorded use of something similar to vaccination was in China in the 16thcentury.
Will I immediately have protection?
No. Immunity takes time to build up in the body.
For most Covid vaccines it takes at least two weeks after the vaccine has been administered for you to start developing immunity. Most vaccines will start providing some protection against severe illness two weeks after the first dose. However, good protection generally requires at least two doses of the vaccine, and will start materialising 7-14 days after the second dose.
All vaccines work very well against severe Covid, irrespective of the variants (different versions of the virus) that are circulating. They differ in how well they protect against infection and mild Covid (usually sniffles, tiredness and other flu-like symptoms).
At the moment, two vaccines are being used in SA — both excellent choices.
The J&J is being used as a single shot; the Pfizer as a two-dose schedule, several weeks (minimum three weeks) apart. Other excellent options, mostly two-shot, are being evaluated. Don’t stress about which one is best — the best one is the first one you can get.
Even though you have had a vaccination, you should continue to act as if you do not have immunity until three weeks after your first (J&J) or second shot (Pfizer).
Do not assume you have enhanced immunity straight after getting your jab. Continue to take precautions. Mask when indoors with people and always open windows in rooms and vehicles.
We have seen many people get sick in those two weeks while waiting for their immunity to kick in, either infected just before or after their shot.
How safe are you once you are fully vaccinated?
All the vaccines currently in use give excellent protection against severe illness and death — they keep you out of hospital and off a ventilator.
We have less good information on how likely you might be to get a mild infection of Covid, and it is possible that you could get infected. We have seen many people get mild “breakthrough’’ infections even after the full two weeks after vaccination. Often this will be so mild that you don’t know you have it; some people get worse infections which can feel like a bad cold, but they usually recover after 2-3 days.
The possibility of being mildly infected means that when you are with people who are not fully vaccinated, you should continue to take precautions of masking, opening windows and avoiding being together indoors or in a vehicle, because you could infect those who are not protected. Even though it is possible to get Covid mildly once fully vaccinated,we now know that fully vaccinated people are less likely to spread the virus.Also, vaccines will differ in how well they protect against infection and mild Covid, which also depends on which variants are circulating.
We are still learning how best to deal with these mild infections, especially with the new, hyper-transmissible Delta variant. It is possible we may need additional shots for better protection, whether of the same vaccine or a different one. Stay posted.
Should I expect side effects?
You may feel no effects at all. But side effects can include having a sore arm where you were injected, getting a headache, or having a fever, for a day or two. The side effects experienced are much milder than getting severe Covid (some of the authors have had this experience). Also, these side effects generally indicate that the vaccines are inducing an immune response and doing what they are meant to do.
Severe allergic reactions are very rare, but can occur after any vaccination; if they occur, the healthcare provider who administered the vaccine can immediately and usually effectively treat the reaction.
The Pfizer vaccine can cause an allergic reaction which is easy to treat, and very rarely can cause inflammation of the heart, which normally goes away quickly.
The J&J vaccine has a very rare effect of blood clotting, and can be serious; Covid causes this effect far more often, though, so the benefits far outweigh the risks. Recently, the J&J vaccine has been associated with a very rare syndrome causing weakness, called the Guillain Barre Syndrome. This syndrome is also seen in patients who have had the flu and other viruses, and is treatable.
Are there any people who should not get vaccinated?
No. But some people may not respond — not everyone’s immune system learns equally well from vaccines.
People who have conditions involving immune suppression — for example, someone who has had an organ transplant and is taking immunosuppressant drugs to stop their body from rejecting the new organ, or people on chemotherapy or taking immunosuppressives for other condition like rheumatoid arthritis — may not develop as good immune responses from vaccines. We are learning, though, how to amend the doses so these people can get better protection — so watch this space.
In addition, people with severe allergies may want to avoid the Pfizer vaccine, or ensure that the person giving the vaccination is ready in case of a reaction.
What is the Delta variant? What is the story with these Covid variants?
Like all viruses, SARS-CoV-2, the virus which causes Covid, changes and develops. When a version develops that has important differences (for example, that increases its transmissibility, virulence or relative ability to evade immune responses), it is given a new label, such as the Delta version of Covid, which has been hitting South Africa hard.
TheDelta variantis two-fold more infectious than the original SARS-CoV-2 virus, which is why it has been spreading so quickly. So far the vaccines are still working well in protecting against severe Covid due to variants, but vary in how well they protect against infection and mild Covid from different variants.
Scientists are working on vaccines that might work better against infection and mild Covid irrespective of mutations of the virus. It may be that we need to get a booster vaccine every few years to deal with new variants, particularly if one is at high risk of getting severe Covid. But equally, it is possible that the current vaccines may be enough.
What is the difference between the different vaccines?
There are 19 different vaccines currently used around the world against Covid, and more are being tested.
The vaccines mostly being used in South Africa at the moment are made by Pfizer and Johnson & Johnson (J&J). These vaccines work in very different ways. While more traditional vaccines use a component of the virus or a weakened or killed version of the virus which stimulates your body to develop an immune response, the Pfizer vaccine uses a copy of a molecule in our bodies called RNA which causes cells in our bodies to produce the protein that our immune system responds to.
The RNA vaccines do not in any way affect or alter your genes or your DNA. All the vaccines eventually get your body to respond in a similar way to how it would if infected — to produce cells and antibodies that can fight Covid-19. The advantage of the RNA vaccines is that RNA is easier to design and can be produced very quickly. Also, since it does not require the production of any form of the potentially very dangerous virus, it is also safer to produce.
It is not very easy to compare how well the different vaccines work because the trials in which they were tested used different groups of people at different places, involved different variants of the virus and used different study methods. But both J&J and Pfizer are working very well and giving people good protection against severe Covid-19, including the variants of concern identified to date.
How were the vaccines developed so quickly and should this worry me about their safety?
Covid is a new kind of coronavirus, but coronaviruses are not new — the common cold we get every winter is often caused by one of the coronaviruses. This is part of what enabled vaccines to be developed so quickly. Also, huge amounts of funds and resources were mobilised very rapidly, which enabled swift development of the vaccines.
The vaccines have been thoroughly tested in multiple trials.
More than three billion doses of vaccine have been administered worldwide and in the US 150 million people are fully vaccinated. In the UK, about 55% of the population — about 36 million people — have been vaccinated. This is an extremely safe intervention.
How long will immunity last?
We do not yet know. It is possible that we will need to get a booster vaccine every year or two to keep up our immunity. Modelling studies suggest that people might require booster doses every 2-3 years to protect against severe Covid. To protect against infection and mild Covid might require annual boosting. We will find out over the next two to three years. The focus of vaccination is likely to be centred around protecting against severe Covid and death, rather than preventing infection and mild disease.
The myth of ‘herd immunity’
Some commentators still maintain the aim of vaccination is to develop population-wide immunity, or “herd immunity”. This is when enough people have immunity that the microorganism stops being able to circulate at all. Herd immunity was an aspirational goal until the virus started showing the ability of mutating, causing it to become more transmissible and relatively resistant to antibodies induced by past infection and by vaccines.
Consequently, it is unlikely that herd immunity will be achieved with this virus any time soon, and it will probably circulate, mutate, and recirculate throughout our lifetime, reinfecting us several times, like all the other coronaviruses. Luckily, individual protection against severe illness is still possible with the current vaccines even with the mutations that have occurred. Those who do not get vaccinated will face an increased probability of infection and potential severe illness as variants of the virus continue to circulate. This risk will increase as society returns to normal.
But it is likely that everyone, unless they hide behind a wall for the rest of their lives, will eventually get the virus. It’s all about how badly you get it — whether you get it vaccinated or unvaccinated.
Do I need the vaccine if I have already had Covid?
Having had Covid definitely does provide short-term protection from severe illness, as the vaccines do, but there is no evidence that it is better than the protection acquired from vaccines (and the consequences, as we have noted, are severe).
It is early days yet, and we will have more data to guide things, but we are aware of many cases, including among our colleagues, where people have had a second case of Covid, occasionally severe.
If you have had Covid, the good news is you have lots of protection from severe illness in the short term. However, adding a vaccine on top of this may well stimulate a slightly different response (and augment an already primed immune system), and mean you enjoy additional protection. As we point out, the vaccines are very safe, and Covid does dreadful things, occasionally even in people with prior infection, so it is worth getting the vaccine as an additional precaution. One should wait for 2-3 months after having Covid before getting a vaccine, and you probably only require a single shot.
How do I sign up and find a vaccine site?
TheElectronic Vaccination Data System (EVDS)offers online registration for vaccinations and identifies vaccination sites. Once registered on the system you will be allocated an appointment at a nearby vaccination site. You could also select which site you prefer. The registration system is becoming more flexible to enable more accessibility to getting vaccinated
Will I have to pay?
No. No one has to pay. If you do not have medical aid you will have free access to public sector vaccination sites. If you have medical aid it will cover the cost at the public sector or the private sites; you will not need to pay upfront. The government is in the process of setting up arrangements to ensure that all public and private sector sites can be accessed regardless of medical scheme membership.
Can I find a site vaccinating on weekends?
While many public sector sites are presently not working on weekends, many private sector sites are available. The government is working to achieve uniform coverage throughout the week. It is therefore important to get regular updates on weekend availability.
I’m waiting for my appointment but my friend just walked in and got a vaccine
Some vaccine sites have been allowing those who are registered in the system to come for a walk-in without an appointment. Which sites are doing this, and the extent to which the appointment system is being used, seems to be changing all the time. You might wait in a longer queue if you do a walk-in.
Finally, until you and the people you interact with are all fully vaccinated…
Continue to wear your mask when indoors and to keep windows open. Covid is an indoor respiratory virus: it is spread in the air, and it collects indoors where windows are closed. You are unlikely to get it outside, and opening windows in rooms, cars, taxis and buses makes everyone much safer. As you are fully immunised only two weeks after receiving your second vaccine dose, take this into account when making decisions about interacting with people.
Lucy Allaisis professor of philosophy jointly appointed at Wits and Johns Hopkins University;Shabir Madhiis dean and professor of vaccinology at the Faculty of Health Sciences at University of the Witwatersrand, and director of the SAMRC Vaccines and Infectious Diseases Analytics Research Unit;Imraan Valodiais dean of the Faculty of Commerce, Law and Management, and director of the Southern Centre for Inequality Studies, University of the Witwatersrand;Alex van den Heeveris an adjunct professor and holds the chair of Social Security Systems Administration and Management Studies at the Wits School of Governance;Martin Velleris the former dean of the Faculty of Health Sciences at the University of the Witwatersrand;Francois Venteris a professor of medicine at Ezintsha, Faculty of Health Sciences, University of the Witwatersrand.
Leave no one behind: We must urgently address vaccination of undocumented migrants and asylum seeker
- Jo Vearey, Sally Gandar, Rebecca Walker, Thea de Gruchy, Fatima Hassan, Tlaleng Mofokeng, Pinky Mahlangu, Nicholas Maple, Francois Venter and Sharon Ekambaram
We call on Acting Health Minister Mmamoloko Kubayi to do the right thing to ensure the Covid-19 vaccination programme is inclusive.
Without this we will fail to achieve population immunity, variants will continue to emerge and we will all suffer. Civil society and the research community are here to help, but we need a seat at the table.
Everyone, everywhere has the right to the highest attainable standard of health. But we don’t have to look too far to be reminded of how many people living in South Africa are left behind due to our failures to ensure not only timely and appropriate healthcare, but also the underlying determinants of health.
And the national response to Covid-19 — particularly ourvaccination strategy— is no different.
Amplification of inequalities
People living and working on the margins of society — physically and socially — remainthe most affectedby our public health failures, and — as the past 18 months have clearly shown us in the most painful ways — this is mirrored in thecontext of Covid-19. We know the pandemic has amplified the stark inequities that characterise South Africa and the world, most recently illustrated by vaccine inequity related to accessglobally,continentallyandnationally.
Of the 4,695,719 individuals who had received at least one vaccine dose in South Africa by21 July2021, 34% (1,599,581) have medical aid (representing a fifth of the population who have medical aid), while only 6.09% of the uninsured population — those reliant on the public health system — had been vaccinated. The total percentage of people in South Africa on medical aid is just16%. We believe this is because more supplies than needed have been sent to private sites, while the number of people without insurance are also being restricted from getting vaccinated at those sites, with priority given to members.
Details of this are only now emerging, hence the urgent need for the government to indicate the supply allocations of each and every vaccine site in the country. There is anationalroll-out — private vaccine sites should not be privileged in the programme.
Additionally, for all people living in South Africa, the Electronic Vaccination Data System (EVDS) for vaccine registration is in fact becoming a barrier to getting vaccinated, which explains why so many people over 60 have also not yet registered on the system and why some provinces are now taking “walk-ins”.
However, with no oversight mechanism, the effectiveness of the regulations islimited. Regardless, for any vaccination programme to be effective, we must vaccinate everyone if we are to reach the level ofpopulation immunityneeded to break the chain of transmission — and fast. The spread of the Delta variant makes this even more urgent.
The speed at which the third wave has swept across the country demonstrates, in real time, why we cannot wait to act. Where there’s a safe vaccine and where there are people at risk, we must vaccinate. This is Public Health 101:leaving anyone behind leaves us all behind.
And this includes upholding thepresident’s promise to“make the vaccine available to all adults living in South Africa, regardless of their citizenship or residence status. We will be putting in place measures to deal with the challenge of undocumented migrants so that, as with all other people, we can properly record and track their vaccination history. It is in the best interests of all that as many of us receive the vaccine as possible.”
An increasingly restrictive and dysfunctional immigration regime in South Africa that disproportionately affects black African non-citizens, as well as widespread incompetence andcorruptionwithin the Department of Home Affairs (which has on numerous occasions been found to be in contempt of the Constitution), means that many migrants and asylum seekers in South Africa struggle to access valid documentation.
These challenges have been compounded by theclosure— in some cases the illegal closure — of a number of refugee reception centres. Those that had remained open before the pandemic have been closed since March 2020. This has left those hoping to apply for or renew documents to deal with a poorly designed online application and renewal system instead. With the permit extensions granted during lockdown due to expire at the end of July, and no plan in place to prepare for this,further challengesare anticipated.
Home Affairs itselfadmitsthat it faces an insurmountable backlog of asylum claims and other applications. Due to its increasingly ineffective and dysfunctional systems, many non-citizens find themselves rendered undocumented by the very state system through which they seek to regularise their stay. This is unacceptable and the lack of political will by the state to fix the system is nothing short of xenophobic.
Languagelike “illegal” and “illegality”, and that used by government officials claiming that those without documents are undeserving of basic rights — including access to healthcare and the vaccine — highlights the cruelty of such a system.
Acting Minister Kubayi has not only perpetuated the short-sightedness, xenophobia and Afrophobia of health ministers who havepreceded herin terms of understanding movement and migration as a determinant of health, but, critically, seems to have missed a Public Health 101 briefing as part of her rapid induction into the world of pandemics. Whiletweeting about the “coffee generation”getting vaccinated, Kubayi — who is bound by the prescripts of the Constitution and the decisions of the National Coronavirus Command Council — appears to be out of her depth.
On 23 July 2021, the acting minister was asked by the media how people without state-issued documentation — including anestimated 12%of South Africans without identity documents — can register in the country’s vaccination programme which is only possible through theEVDS.
Shockingly,Kubayi responded that, contrary to thepresident’s promise made in February, she would “have to get guidance in terms of theunregisteredbecause we are dealing within the government systems and provision of services. We follow the laws of the country. So you have to be a documented person in the country. If you are undocumented it means you are illegal in the country. So it’s a different case. We have responsibility to those who are known to the state, by the state.”
In a situation where theforeign embassiesof wealthy nations are vaccinating their own citizens here in South Africa, we urgently need to vaccinate everyone at risk, as recommended by the World Health Organization and other expert bodies, to achieve global immunity. Fuelling anti-poor foreigner sentiments with public statements like this goes against all globally accepted principles of public health risk and need. It is also contrary to guidelines for an effective pandemic response in which clear statements outlining the importance of including everyone — including refugees, asylum seekers and migrants — have been made by theAfrican Commission, theInternational Organization for Migration, theUN Refugee Agencyand theInternational Labour Organization.
Urgent need for firewalls
We know our frontline healthcare staff are overstretched and the priority is processing as many adults as quickly as possible through vaccination sites, even walk-in sites.
The best way to ensure healthcare workers can meet their responsibilities to patients under the National Health Act, including in relation to the reporting and treatment ofNotifiable Medical Conditions(Covid-19 is a “category 1” Notable Medical Condition), is to ensure they arenot asked to act as immigration officials. Denying care, including life-saving vaccines, to people will only further burden the healthcare system and the responsibilities of healthcare workers down the line as Covid-19 outbreaks continue among communities who are unvaccinated by a state strategy of only vaccinating “its own” (and those with papers).
We need alegal, policy and humanitarian firewallthat will protect all people without documents. We need to ensure people are willing to access vaccination sites without fear of being arrested or harmed in any way. Given the violence of the past weeks, we do not need to unnecessarily add more health risk to the system by turning people away from vaccine sites.
Basic public health logic maintains that we need everyone in our country to be vaccinated so that we can mitigate this pandemic — and for this reason we also want to know what the public health and other experts on the Ministerial Advisory Committee have advised the government on this matter. Have our local and global experts stood up for the rights of all people living here, or only some? The public needs to see all the committee’s advisories now.
We must avoid making the mistakes of the past. The years of Aids denialism should remind us that we mustn’t forget how the impact of poor decisions is felt decades later; lives lost due to poor and ill-informed and xenophobic decisions, which go against all public health advice, cannot be recovered later. We mustdraw on the lessons learntfrom the global response to HIV.
For many years there have been calls to developmigration-aware health systems, in which population movement is central to the design of health interventions, policy and research.Researchclearly indicates this means establishing a national migration and Covid-19 task team and developing a basic “scorecard” to guide responses; this should include implementing systems to ensure that undocumented persons can access Covid-19 services, including vaccination programmes, and face no penalties when doing so.
We must ensure everyone has access to life-saving technologies, including vaccines: in a pandemic, effective health interventions belong to everyone. Denying access not only undermines the Constitution and international health law, it also means the national response to Covid-19 will fail.
As such, we echo thestatementby United Nations human rights experts on the universal access to vaccines, and we remind the state that it has “an obligation to ensure that any Covid-19 vaccines and treatments are safe, available, accessible and affordable to all who need them.
“This is particularly relevant to people in vulnerable situations who are often excluded from health services, goods and facilities, including those living in poverty, women, indigenous people, people with disabilities, older persons, minority communities, internally displaced people, persons in overcrowded settings and in residential institutions, people in detention, homeless persons, migrants and refugees, people who use drugs, LGBT and gender-diverse persons.
“Many of them may have lived experience of poverty and find themselves in situations where they are most likely to be exposed to the risk of contagion, yet the least likely to be protected from Covid-19 or supported by adequate and timely tests and health services.”
It is imperative that access to Covid-19 vaccines and treatment are provided to all without discrimination and prioritised for those who are most exposed and vulnerable to Covid-19.
We call on Kubayi to do the right thing and follow international guidelines to ensure the Covid-19 vaccination programme is inclusive. Without doing so, we will fail to achieve population immunity, variants will continue to emerge and we will all suffer. Civil society and the research community are here to help, but we need a seat at the table to do so.
Public Health 101: A cheat sheet for Acting Minister Kubayi
The immediate obligations of the state include the guarantees of non-discrimination and equal treatment, as well as the obligation to take deliberate, concrete and targeted steps towards the full realisation of theright to health;
Followexamplesfrom other countries and adapt administrative systems to allow everyone to register for vaccination regardless of the documentation system;
Urgently publish advisories of the Ministerial Advisory Committee to aid transparency; and
Establish a national migration and Covid-19 task team to support equitable action.
Jo Vearey, Director, African Centre for Migration & Society (ACMS), Wits University; Sally Gandar, Scalabrini Centre of Cape Town; Rebecca Walker, independent researcher and African Centre for Migration & Society (ACMS), Wits University; Thea de Gruchy, African Centre for Migration & Society (ACMS), Wits University; Fatima Hassan, Director, Health Justice Initiative; Dr Tlaleng Mofokeng, United Nations Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health (The views expressed herein are personal and do not necessarily reflect the views of the United Nations); Pinky Mahlangu, Medical Research Council; Nicholas Maple, African Centre for Migration and Society (ACMS), Wits University; Francois Venter, Director, Ezintsha; and Sharon Ekambaram, Lawyers for Human Rights.
Excluding migrants undermines the success of Covid-19 vaccine rollouts
- Rebecca Walker, Jo Vearey and Nicholas Maple
Failure to ensure access for all to prevention and treatment, including vaccines, undermines national responses to Covid-19.
Migration is increasingly recognised as a determinant of health. Research shows that, in many cases, cross-border migrants arriving in new countries are healthier than the host population. But the advantage often falls away as non-nationals encounter discrimination and challenges in accessing documentation, support services and employment.
The health and wellbeing of all individuals within a country’s borders must be addressed. But African states have failed to design and implement migration-aware health systems and responses. Many non-citizens, asylum-seekers and refugees are excluded from public health programmes.
The impact of such exclusions is now playing out. COVID-19 illustrates how refugees, asylum seekers, internally displaced people and migrants are being left out of pandemic preparedness plans, including national vaccination programmes.
Evidence shows that the vast majority of migrants are currently excluded from state-based COVID-19 vaccine rollout programmes. These forms of exclusion are likely to have far-reaching public health implications. To effectively reduce the spread of COVID-19, everyone must be vaccinated. Otherwise the virus will continue to spread while new variants emerge.
The African continent has the lowest COVID-19 vaccination coverage globally. Just 2% of the population has received at least one vaccine dose. But beyond this is the issue of how countries implement their own COVID-19 vaccination programmes and who they leave behind.
Some countries do include migrant populations. But the International Rescue Committee (IRC) reported in May 2021 that 60% of countries receiving their vaccines through COVAX had excluded refugees or internally displaced populations from their national plans.
We have been conducting research exploring access to COVID-19 vaccines across the continent. Our findings and a case study of South Africa highlight the issues of vaccine nationalism, vaccine exclusion and hesitancy and their likely effect at the population level.
Exclusion and violation of rights
Restricted access to vaccines is one clear example of discrimination against migrants. Not all migrants are undocumented and not all who are undocumented are vulnerable. But the exclusion of specific groups on the basis of citizenship, immigration or documentation status violates their human right to health, and affects the success of any vaccination programme.
Our investigation highlighted how migrants and refugees are being excluded.
First, migrant populations have simply not been included or have been ignored in vaccination rollout plans of many states. Few vaccine programmes across Africa make it explicit whether – and how – various migrant groups will fit into the rollout. For example, an internal WHO report in May 2021 noted that in Nigeria, there are concerns that over 2.7 million internally displaced people are at risk of being completely ignored in the current vaccine plans.
Second, even where non-nationals are explicitly included in plans, such as in Kenya and Senegal, they may face barriers. For example, in Kenya, refugees are fearful of coming forward and accessing state services such as public healthcare. The same WHO report noted that Kenya might exclude hundreds of thousands of refugees through a disconnect between policy and practice.
The risks of arrests, detention and deportation are significant in many states. If people don’t feel safe, COVID-19 vaccination programmes will be less effective.
There are nonetheless notable exceptions on the continent – Rwanda, Cameroon and Senegal being three. For example, Senegal and Cameroon are allowing refugees to register in designated health facilities and city councils. Rwanda was one of the first 20 countries worldwide to begin vaccinating refugees and asylum seekers alongside citizens. The national response plan prirotises asylum-seekers and refugees alongside healthcare workers and key civil society and community members.
The case of South Africa
Exclusion, barriers to access and discrimination can be seen clearly in southern Africa, and specifically South Africa. The region has diverse historical and contemporary migration patterns. South Africa has the highest rates of cross-border migration. Only 7% of the South African population is estimated to have been born in another country.
Due to an increasingly restrictive immigration regime and a seriously compromised Home Affairs Department, many migrants in South Africa struggle to regularise their stay. As a result, those who start off with work permits or asylum-seeker permits often find themselves – through no fault of their own – without valid documents.
Where the vaccination rollout requires an identity number, passport number or refugee permit to register there is no option for those who do not have these. Furthermore there is no clear directive of how people who are undocumented – including South African citizens – can register for vaccination.
The South African government has included refugees and asylum-seekers with documentation in the country’s vaccination rollout.
Vaccine hesitancy
Finally, a response to vaccine hesitancy within local communities and migrant groups on the continent demands collective action between states, international humanitarian organisations and civil society. In addition to a mistrust of vaccinations themselves, hesitancy can take the form of a fear of being treated badly due to anti-foreigner attitudes, or fear of arrest or deportation.
For example, in the Central African Republic, rumours have been circulating about “foreigners” spreading the virus and even fears that international aid agencies are creating the virus as a way to make money. In Rwanda, rumours and the spread of misinformation have gained traction in certain areas.
More strategic thinking is needed to raise awareness, build trust and outline measures of protection for those who fear coming forward for the vaccine. As the International Organisation for Migration has emphasised, reaching out to migrant communities, in tailored languages and through relevant communication channels, is central to creating vaccine demand.
One approach would be to include civil society organisations, community groups and religious leaders in vaccine rollout programmes.
A clear way of improving the safety of everyone is through firewalls. These provide legal protection for undocumented people, ensuring they face no penalties when accessing state health services. Any information collected is used by the health system only.
Not only does the continent need more vaccine doses, but countries must also include all migrant populations. Failure to ensure access for all undermines national responses to COVID-19. The consequences spread far beyond those nations.
There is no place for hypocrisy. The international community cannot be called out on vaccine nationalism if states do not plan for an inclusive national response themselves. Without vaccinating everyone, nobody is safe.
Six myths about vaccination for Covid-19 put to rest
- Neelaveni Padayachee and Varsha Bangalee
The circulation of misinformation about the Covid-19 vaccine poses the danger of hampering the government’s efforts to control the pandemic.
South Africa’s COVID-19 vaccine rollout programme, outlined by the Ministry of Health, had three phases, starting with the most vulnerable population.
Phase one included all the frontline healthcare workers. They received the Johnson and Johnson vaccine. Phase 2 vaccinated people over 60 years old and those in congregate settings. The third and final phase, now under way, covers the remaining South African population.
The programme got off to a shaky start in February 2021. It encountered a number of setbacks such as supply, logistics and governance issues, but has gained momentum in recent weeks. As many as 200,000 doses are being administered daily. By the end of July 2021, almost 2.9% of the South African population had been fully vaccinated and 7.5% had their first of the two Pfizer doses.
Despite this uptake, many South Africans are still hesitant to take the vaccine. The circulation of misinformation about it poses the danger of hampering efforts to control the pandemic.
In this article, we aim to dispel some of the myths surrounding the COVID-19 vaccines.
Myth 1: The COVID-19 vaccine will affect a woman’s fertility
This myth was sparked when a social media post was shared in December 2020 by Dr Wolfgang Wodarg, a physician and former chief scientist for allergy and respiratory therapy at Pfizer, and Dr Michael Yeadon, a pulmonologist. They claimed that the spike protein on the coronavirus was the same as the spike protein that is responsible for the growth and attachment of the placenta during pregnancy. The fear was that, as a result of the vaccine, the immune system would not be able to differentiate between the two spike proteins and would attack the placental protein.
This is untrue. The overall makeup of the placental protein is very different from the coronavirus spike protein.
Additionally, during the Pfizer vaccine tests, 23 women volunteers became pregnant after taking the vaccine.
Furthermore, the benefits of being vaccinated outweigh the risks of infection for pregnant women.
Myth 2: I’ve had COVID-19, so I don’t need a vaccine
Reinfection with SARS-CoV-2, the virus that causes COVID-19, can occur even in individuals who have previously contracted the virus. But receiving the vaccine can provide protection against severe COVID-19 complications.
The level of protection that is achieved from natural immunity after being infected by the virus is unknown. But scientists believe that the vaccine provides better protection than natural infection.
Myth 3: COVID-19 vaccine side-effects are dangerous
Several studies have been conducted since the start of the pandemic that have measured South Africans’ perceptions of vaccine issues. A recent study by the University of Johannesburg and the Human Sciences Research Council of South Africa found that of the respondents who did not want to be vaccinated, 25% were concerned about side-effects.
Most of the side effects of the COVID-19 vaccine are mild. They include low grade fever, sore arm and fatigue, and these usually subside after one to three days.
Rare side effects such as blood clots have been reported from the Johnson and Johnson vaccine. The chances of experiencing this side effect are low. The risks of blood clots as a result of COVID-19 infection are 8-10 times higher than risks associated with the vaccine. Doctors are aware of this concern and are trained to identify and treat the condition quickly.
A recent article by Healthline – a medically reviewed and fact checked website – compared the benefits and risks of being vaccinated with those of contracting COVID-19. Lung damage is a complication of COVID-19 while muscle fatigue can be a side effect of the vaccine. This risk-benefit decision is left to the individual to make, but vaccinations have been proven to be safe.
Myth 4: Vaccines have a microchip that will track and control an individual
This conspiracy theory has been propagated by anti-vaxxers who believe that the American business magnate, investor and philanthropist Bill Gates will implant microchips to track people’s movement, using the vaccine as the method of delivery. This is untrue and has been clarified by Gates in the media.
This myth gained traction when a video was shared on Facebook making false claims about the optional microchip on the syringe’s label of the COVID-19 vaccine. This microchip’s purpose is to confirm that the injectable and the vaccine are not counterfeit and haven’t expired. It will also confirm if the injection has been used.
People commenting on the video appeared to have misinterpreted the technology as an injectable. But the microchip is part of the syringe label and not the injectable substance itself.
Myth 5: The COVID-19 vaccine development was rushed, so it may not be effective
The vaccine was developed very quickly. This was possible because the vaccine technology had been in development for many years. When the genetic information of SARS-CoV-2 was identified, the process could begin quickly. There were sufficient resources to fund the research and social media made it easier to recruit participants for the clinical trials. Because SARS-CoV-2 is contagious, it was easy to tell whether the vaccine worked or not.
Myth 6: The COVID-19 vaccine can alter my DNA
The messenger RNA vaccine (Pfizer) and the viral vector vaccine (Johnson and Johnson) cause your body to develop protection, so that when you are infected by SARS-CoV-2, your body is prepared to fight the virus. DNA is located in the nucleus of your cells and the vaccine material does not enter the nucleus. So it does not alter the DNA.
Social media plays a huge role in propagating myths and conspiracy theories. Before you share any information, you should ensure that it is from a scientific and reputable source.
Pasha 118: We need to learn to live with COVID-19.
In the first year of the COVID-19 pandemic the phrase “herd immunity” was bandied about a lot by heads of state as well as health officials. This ideal end state was described as the moment when the virus had been beaten, and everyone could return to a normal life.
But a great deal has changed in the intervening months. Firstly, the virus has mutated in ways that make it spread more quickly, and in ways that make it potentially more resistant.
In addition, the unequal distribution of vaccines, combined with slow rollouts in a great many countries as well as vaccine hesitancy, has thrown initial planning off course.
So what’s the alternative?
We must learn to live with the virus. To do this, reaching high levels of vaccination is crucial. This will minimise the number of people being hospitalised and dying from COVID-19. It does not mean that COVID-19 will be gone but it means clusters of outbreaks will be smaller and less damaging to countries. Health facilities will be able to cope better.
In today’s episode of Pasha, Shabir A. Madhi, Dean of the Faculty of Health Sciences and Professor of Vaccinology at the University of the Witwatersrand, discusses the problems with herd immunity and how to deal with COVID-19 in the long term.
Covid-19 herd immunity is not going to happen, so what next?
- Shabir A. Madhi
When politicians and others speak about herd immunity, unfortunately, they are under the misconception that the current tools that we’ve got are adequate.
Any notion that COVID-19 was going to last for just a few months was very much misplaced in 2020. Especially after it was recognised that the SARS-CoV-2 virus was largely spread through the airborne route, all indications were that it would cause repeat bouts of waves. This is what happened in the flu epidemic of 1918.
In addition very few scientists predicted that we would see the type of mutations that occurred over such a short period of time. This has resulted in the virus becoming both more transmissible and more able to evade immune responses.
The evolution of the virus has been so rapid that the Delta variant, which is currently dominating the world, is at least twice as transmissible as the ancestral virus that was circulating.
What this means is that herd immunity is no longer a discussion the world should be having. We should start to avoid using that term in the context of SARS-CoV-2, because it’s not going to materialise – or is unlikely to materialise – during our lifetimes.
When politicians and others speak about herd immunity, unfortunately, they are under the misconception that the current tools we’ve got are adequate to eliminate the virus. It’s not what we have at hand right now.
Instead we should be talking about how to live with the virus. The tremendous success that’s materialised with COVID-19 vaccines allows us to do this, without actually getting into the herd immunity threshold.
Peddling the concept of herd immunity creates a misconception that we are actually going to get to a stage where this virus is going to be eliminated. That’s unlikely to happen. It will continue circulating.
There are a number of dangers in continuing to make people believe it’s possible.
Firstly, it could dent confidence in vaccines. Even if South Africa gets to its target of 67% of the population being vaccinated – as set out by the Department of Health – there will still be outbreaks of COVID-19. The result will be that people begin to doubt the benefits of being vaccinated. Also, for the now dominant Delta variant, immunity against infection (not only COVID-19 illness) would need to be closer to 84% for the “herd immunity” threshold to be reached.
Secondly, failing to face up to the reality that herd immunity can’t be achieved will mean that countries like South Africa will continue to believe that ongoing restrictions will get them there. That will compromise the lives of people on multiple fronts – including education and livelihoods.
What is herd immunity?
Herd immunity is when someone infected by the virus won’t, on average, infect another person. So you reach a state where the immunity in the population against infection by the virus is such that there are too few people in the environment for sustained onward transmission to take place to others.
This is because they’ve developed immunity against being infected, or at least have developed immunity to the extent where even if they were infected, they would be able to clear the virus very quickly and wouldn’t be able to transmit it to other people.
So herd immunity essentially means that you have brought about an absolute interruption in the chain of transmission of the virus in the population in the absence of other interventions that too could interrupt virus transmission such as wearing of face masks.
But some changes have forced a shift in our thinking about herd immunity. It’s now viewed much more as an aspiration rather than actual goal.
What’s changed
Firstly, the evolution of the virus and the mutations that have occurred.
One set of mutations made the virus much more transmissible or infectious. The Delta variant is just such an example. Initially we thought the SARS-CoV-2 reproductive rate was between 2.5 and 4. In other words, in a fully susceptible population every one person infected would on average infect about two and a half to four other people. But the Delta variant is at least twofold more transmissible. That means that the reproductive rate of the Delta variant is probably closer to six rather than three.
The second change is that the virus has shown an ability to have mutations that make it resistant to antibody neutralising activity induced by past infection from the original virus, as well as antibody responses induced by most of the current COVID-19 vaccines.
The third big issue centres on the durability of protection. Our memory responses are lasting for at least six to nine months at the moment. But that doesn’t mean that they will protect us against infection from variants that are evolving, even if such memory responses do assist in attenuating the clinical course of the infection leading to less severe COVID-19.
The fourth issue conspiring against us being able to reach a herd immunity threshold any time soon is the inequitable distribution of vaccine across the world, the slow uptake and the sluggish rollout. Unfortunately, this provides fertile ground for ongoing evolution of the virus.
No country is going to lock its borders perpetually. This means the entire global population needs to reach the same sort of threshold round about the same time. At the moment just 1% of the populations of low-income countries have been vaccinated. And 27% of the global population.
With the Delta variant, we would need to get close to 84% of the global population developing protection against infection (in the absence of non-pharmacological interventions) in as brief a period of time as possible.
Next steps
The only sustainable solution is to learn to live with the virus.
This will require ensuring that we get the majority of individuals, especially adults, and particularly those at a higher risk of developing severe COVID-19 and dying, vaccinated as quickly as possible. In my view this could be achieved in South Africa with 20 million people vaccinated – not the 40 million target set by the government. But the 20 million would need to include 90% of people above the age of 60, and 90% of people above the age of 35 who have co-morbidities.
If South Africa achieved this milestone, it could get back to a relatively normal lifestyle even with the virus continuing to circulate and causing the occasional outbreak. It would also ensure a threshold that guaranteed its healthcare systems weren’t going to be overwhelmed, and that people were not going to die in large numbers.
We are simply going to have to become comfortable with the idea that SARS-CoV-2 is going to be like one of the numerous other viruses that circulate that cause respiratory illness each day. Usually mild infections, and less often a severe disease.
So people will, unfortunately, continue dying of COVID-19, but certainly not at the magnitude that’s been seen over the past 18 months. A major advance would be for COVID-19 to be no more severe than what is seen every influenza season (10,000 to 11,000 deaths) in South Africa.
The UK experience is where we should be heading. That is getting back to a relatively normal lifestyle, provided that we’ve got a adequate number of people vaccinated, and particularly people who are at higher risk of developing severe COVID-19.
The UK is currently close to 85% of adults that have already received at least a single dose of the vaccine. As a result they’re able to remove almost all restrictions.
The UK is seeing an increase in number of cases of the Delta variant. But they’ve seen very nominal changes when it comes to hospitalisation and death. The vast majority of people (97%) who still end up being hospitalised and dying of COVID-19 in the UK are those who decided not to be vaccinated.
Shabir A. Madhi, Dean Faculty of Health Sciences and Professor of Vaccinology at University of the Witwatersrand; and Director of the SAMRC Vaccines and Infectious Diseases Analytics Research Unit, University of the Witwatersrand. This article is republished from The Conversation under a Creative Commons license. Read the original article.
Variants, the fourth wave, vaccines and the unlikelihood of herd immunity
- The Scientists Collective
What might happen in South Africa?
The rise of the scary-sounding variants, a South African third Covid-19 wave that was much worse than the first or second for most of the country, and the introduction of multiple vaccines has confused many of us. Uncertainty about the future is always frightening. This is especially so when scientists don’t explain things clearly, or where there is disagreement around ideas like ‘herd immunity’, whether the new variant makes you sicker than the previous ones, and speculation about how the virus will evolve further.
First, some key points in our article (below) about SARS-CoV-2 (the virus)/Covid-19 (the disease) in South Africa:
South Africa, like much of the African region, has experienced a devastating third wave, made worse by the very small number of people who were vaccinated when the super-infectious Delta variant arrived.
The phrase “herd immunity” is used incorrectly by senior advisers to government, and unfortunately has entered popular vocabulary among politicians, commentators and the media, when it is extremely unlikely to occur.
Ongoing mention about vaccinating to reach herd immunity threatens to undermine messaging on the actual value of vaccines,which is primarily to prevent severe disease and death.
Our immune system seems unable to stop SARS-CoV-2 infection in everyone, even after vaccination or previous infection.
However, the vaccines (and immunity produced by a previous infection) seem excellent (not 100%, but very close) at stopping severe illness — the kind that puts you in hospital and kills you.
Understanding that the primary role of Covid-19 vaccines is to protect against severe disease and death helps us to decide how best to use current vaccines, future possible combinations or “boosters”.
A better understanding will also better inform how we use masks, and apply social distancing and lockdowns, to get our society, schools and other institutions back to normal as quickly and responsibly as possible.
Experts are cautious about firmly forecasting the future of the Covid-19 pandemic as there are many uncertainties. But we know if a fourth wave arrives towards the end of the year (as previous waves have been roughly five to six months apart), vaccinations for as many people as possible are our #1 priority, as well as preparing and stocking health facilities, and ensuring safeguards against rapid spread are in place in places where people gather in large numbers.Lessons need to be learnt from the experience of the first three waves.
In the short term, it is impossible to over-emphasise how important it is to get the vast majority (90% or more) of vulnerable people (those over 60, and those with comorbidities) vaccinated before November 2021.
Deal with it! Masks and physical distancing are here to stay until there is high penetration of Covid-19 vaccines among the groups most vulnerable for severe Covid-19.
If we get the majority of adults vaccinated, (like the 88% of adults in the UK), especially the most vulnerable, there is a future (maybe a year away) where we may be able to get back to a normal lifestyle and start regarding this virus like the seasonal influenza virus — something that we have to live with and manage.
In this article, we try to explain the current scientific understanding, and, more importantly, some scenarios that may evolve as we stare down a fourth wave, and how you should plan your life.
But first, a few concepts:
What is ‘herd immunity’? (and why is it unlikely to materialise for SARS-CoV-2)
Herd immunity, simply put, is where even individuals without immunity enjoy protection from an infectious disease because so many people around them have immunity (either from prior infection or vaccine), and do not transmit the infection, in this case the coronavirus SARS-CoV-2. While the unPC term “herd immunity” makes us sound like a bunch of animals rather than humans, it’s become a popular phrase used in the media and by scientific advisers quoting it alongside statistical formulas, which mislead and falsely reassure the public and policy makers alike.
So let’s unpack the term so we know what we mean when we use it in this article.
The term herd immunity, sometimes called population immunity, has been around for about 100 years, and implies we can protect the vulnerable from infection by getting immunity in the people around them, enough to mean they are unlikely to be exposed.
It was rapidly applied to SARS-CoV-2 in early 2020, with some scientists, politicians and other real and self-proclaimed experts advocating that a more or less uncontrolled spread of the infection was a way to get society back to normal. This is a reckless approach in our view.
The reality is that herd immunity does not apply to SARS-CoV-2. This is because the virus is very widespread, highly infectious, and mutates relatively easily. As a result of its characteristics, people who have been vaccinated or infected can still get infected and spread the virus, meaning everyone will get the virus eventually.
SARS-CoV-2 is a coronavirus; several different coronaviruses are widely circulating among human beings, causing mostly common colds every year. Every person reading this article has had infections with these coronaviruses dozens of times in their life, their immune system primed for repeat challenges when they had their first infections during the early years of life.
Everything we see about SARS-CoV-2 suggests it will do the same with time — simply become one of the circulating viruses causing mild illness that we all deal with every season. The current dreadful illness mainly occurs in those witholderor compromised immune systems who have not encountered this virus before, although we are seeing significant severe illness even in younger populations.
Organisms always evolve towards greater transmissibility, though the effect on virulence (the ability to cause harm) is much less clear — virulence can decrease even as transmissibility increases.
Developing full-blown herd immunity for SARS-CoV-2 would require either an evolution in the virus against its own “interests” (infecting as many of us as possible), or a level of immunity as yet unseen from the currently available vaccines; we think both are scientifically improbable.
So, we can’t have herd immunity and shouldn’t use the term.
We strongly suggest advisers to government or politicians stop using this term, as it creates a misleading idea of what to expect with Covid-19 in the future, and risks creating doubt about the value of vaccines. Perhaps a better term is “population effective protection’’ — how many people have been vaccinated or infected in the population and enjoy protection from severe illness (but not necessarily infection).
This makes it easy to see why vaccines are our only solution out of the pandemic without old and vulnerable people getting sick and dying in large numbers. It also makes it easy to understand that future “booster doses’’ or changes in the pattern of vaccine administration may be needed.
If immunity reduces over time or proves insufficient, for example in immunocompromised people, we may need further jabs (as with flu), or we may find that a certain combination of vaccines confers optimal or even life-long protection against disease. Some people may not need these add-on vaccines — the circulating virus may act as a natural booster, after an initial vaccine or infection.
There is a fortune of research going on in the field of booster vaccine doses — watch this space.
Protection from Covid is available, one way or another. Get it through the vaccine rather than natural infection!
In a substantial proportion of people, especially the elderly and those with comorbidities like diabetes, but sometimes even in younger and otherwise healthy people, the virus unleashes a serious immune reaction that damages the lungs and other organs. Natural infection seems to be much less severe when you are younger, but it is still bad enough for public health experts to recommend vaccination (this is partly because the vaccines are very safe when compared to the unpredictable risk of developing severe Covid).
We also don’t yet know what the long-term consequences of long Covid will be, which can affect any age group. Natural infection will come your way eventually, but this may be much later than your vaccination date, so by waiting for natural infection you won’t be able to stop the spread of the disease through the population.
Bottom line: getting infected is ultimately inevitable if you engage with other human beings — and being vaccinated when that time comes provides you with maximal protection. Getting protection from illness from a vaccine is very, very safe compared to getting it from experiencing SARS-CoV-2.
Variants are often more infectious:
Viruses mutate as a natural phenomenon, so the news that this happened isnot surprising to scientists. Everyone has heard of the “South African’’ (now named “Beta’’) and the current “Delta’’ variants, and there are others from Brazil and the UK.
So-called “variants of concern”, either have mutations that confer advantage in evading our immune response and/or transmit more easily than the original version of the virus — in the second wave, the Beta variant was responsible for the vast majority of infections in South Africa. In the third wave, the Delta variant caused massive waves of infection in Africa, Europe, Asia and North America. It is inevitable that further variants will still develop.
The variants vary as to how lethal they are or how sick people get. It is important to remember that viruses are not necessarily out to kill you — the goal of any living organism is to reproduce, and so a virus will do this by infecting as many people as possible to spread as far as it can. Your immune system is designed to try to stop or limit the infection before it damages the body.
Vaccines are a wonder of modern science. Even the ones that do not fully prevent infection.
There are actually only three questions we need to ask, concerning how vaccines work:do they protect you from infection? If not, do they stop you getting sick? And finally, will they make you less likely to pass infection along if you get infected?
To the first question, the answer is “mostly” — the virus is less likely to cause infection in the vaccinated, certainly less symptomatic infection, although the variants have shown that some vaccines may be better than others at this.
Should we worry that several of the vaccines are not as good at preventing infection?
Every current vaccine significantly reduces the chances of hospitalisation and death (and probably long Covid) remarkably well. Currently, in some cases, vaccinated individuals do experience what health professionals call“breakthrough infections”, where the virus finds its way past the body’s initial defences, and illness occurs (usually it feels like a cold), but the rest of the immune response will prevent any spread and severe harm.
Indeed, this kind of partial protection is likely to happen eventually with ALL the current crop of vaccines. We do not need to worry about this, so long as the vaccines continue to prevent the serious consequences of Covid-19.
This is excellent news — none of us lives in fear of the common cold apart from germaphobes.
Finally, will it prevent transmission?
Preliminary data suggest there are fewer people infected in households where more members are vaccinated. This makes sense, aspeople who are vaccinated tend to shed less virus when they get infected. However, it has been shown that the Delta variant makes you shed far more virus than other variants.
The research question here is critical to us getting back to normal society — does being vaccinated make you less infectious to others? Again, too early to know for sure. Watch this space, but we are hopeful.
Will there be a fourth wave, and when?
Frustratingly, this is not clear. We are guessing any time from October/November, because it seems to be following a cyclical pattern in many places, every six months, here and elsewhere. But the surges in different places, even between South African provinces, vary widely, with the peaks differing by two to three months, as well as in severity.
Many countries, like ours, had a worse second and far more intense third wave; others have had two waves but with high levels of infection in between, and in some, the second wave wasn’t as bad. Portugal had a third wave just a few weeks after the second. India’s third wave was devastating. So, wait and see and be prepared. In highly vaccinated countries, almost all the deaths are in unvaccinated people, which is why South Africa should single-mindedly focus on this.
So, what scenarios await us? Based on the understanding we have of SARS-CoV-2 so far (set out above) we have detailed some possible scenarios below:
Scenario 1 (and the one we think most likely)
The infection becomes more like a common cold or like seasonal flu.
After several further epidemic waves, the virus continues to circulate indefinitely in a series of smaller waves, infecting people (vaccinated and unvaccinated) repeatedly every year or two, like the other circulating human coronaviruses. We may see more major waves if a new more transmissible variant similar to Delta emerges, but it is likely the most transmissible versions are fighting it out (keep an eye on the Lambda variant in South America).
For people with prior infection or who have been vaccinated, every subsequent infection means on average less severe illness. For instance, a first infection can range from no symptoms at all, to a severe illness putting you in hospital or to giving you long Covid (which we explained in aprevious article) after even initial mild infection, but subsequent infections are less and less severe.
Why do we think this scenario is possible?
Large studies, including in health workers, show that once you have had it the first time, subsequent infections are almost always far less severe. We see the same with vaccines — when you get infected, it’s usually minor or asymptomatic. Some people still get sick the second time, but severe illness is very unusual. There is a theory (read here) that this is how one of our endemic coronaviruses arose, in the 1890s — it surged through the world, killed lots of people, and those who survived developed immunity and thus adapted to it.
What are the implications of this scenario?
Paradoxically, this is the happiest scenario, but ONLY with mass vaccination. If we don’t quickly vaccinate a large number of people who have not been infected yet, then the elderly, and those with comorbidities in particular, will still be at risk of severe illness and death.
Some poorly thought-through commentaries have called for “natural infection’’ to accelerate this process, arguing that getting as many young people infected as possible will speed us towards herd immunity. If the scientific scenarios above are valid, this is a dreadful option, as herd immunity in the context of Covid-19 is such flawed thinking. If they are wrong and we are right, and this is allowed to happen, a huge number of people will get sick (even young people have a small chance of severe illness), potentially have chronic illness (long Covid), and die for nothing.
In summary, it’s a race: you get the virus or you get the vaccine. If you gamble on the virus, as some anti-vaxxers will, you put yourself and others at risk of all the Covid-19 consequences, and if lucky, will survive and be immune. You will also put others at risk, even if your own infection remains without symptoms or runs a mild course. If you get the vaccine, you fast-track your immunity at a far lower risk of illness.
Immunity to SARS-CoV-2 may prove to be transitory, and reduce to next to nothing over a few years, much like with flu. With flu, getting the disease or getting the vaccine protects you, but immunity is lost quickly, which is why we have to vaccinate annually. The best-case scenario is that natural infection or vaccines provide permanent protection; the “flu’’ scenario the worst, and again there are variations where we may have to “boost’’ in more vulnerable populations every so often.
We think that if the above scenario is in play, and mass vaccination occurs quickly, we can be back to almost or total normal within a year, provided 80% or more of adults are vaccinated. In this scenario, vaccinated or previously infected people can probably congregate as normal, with little or no restrictions.
Until large numbers of people are infected or get vaccinated, though, and we see that subsequent infections are shrugged off like the common cold, the masks and physical distancing will need to stay — to protect the unvaccinated. There are variations of this scenario, where the virus mutates to a more benign form, or even spontaneously disappears (we think this is highly implausible), or we get a super-vaccine that totally protects from repeat infections (also unlikely) — but means the same thing — life gets back to a normal.
Scenario 2: Not much changes
The virus continues to circulate indefinitely, evolving as it goes to escape our efforts at becoming immune, and continuing to cause lots of severe disease as it’s doing now. We think this is not likely because both natural and vaccine-derived immunity would have to fail to be significantly protective against severe disease for the new variants, and that’s not what we’re seeing. Our immune system is incredibly sophisticated, and the virus likely has a limited number of options of evading it while causing severe disease.
Scenario 3: Eradication
We include this here, even though as we explain above, we think this scenario is frankly impossible.
Some commentators continue to advance an eradication/control option. In this scenario, lockdowns, public health interventions and contact tracing with aggressive quarantining brings the virus under control to the point of eradication, as they have done in New Zealand and Iceland. This isn’t feasible since society is then perpetually vulnerable to having the virus run through its immunologically ill-prepared population and undoing all your hard work (see Australia at the moment).
Obviously, eradication would be ideal, but the level of societal change required, especially in the context of a global travel network and porous borders, combined with the fact that the seeding of the virus is so widespread (and rare patients continuing to excrete the virus for months), that it seems incredible. As we describe above, herd immunity approaches to eradication using infections and vaccines are impossible.
We are aware we are putting our heads on the block with these scenarios somewhat, but South Africans need to start thinking about the possible futures that await them and prepare for these different scenarios. The health, economic and social costs that the pandemic has had on our society have been exacerbated by inadequate strategy and poor planning. We also need to understand why vaccines are critical to any normal future, including reviving our economy. If the vaccines continue to work as well as they have, a vaccinated future holds hope of a return to normality.
The following scientists have contributed to this article:
Prof Shabir Madhi, Respiratory and Meningeal Pathogens Research Unit, University of Witwatersrand; Dr Jeremy Nel, University of Witwatersrand; Prof Marc Mendelson, University of Cape Town; Prof Lucille Blumberg, National Institute of Communicable Diseases; Dr Nomathemba Chandiwana, Dr Samanta Lalla-Edwards, Taylor Johnson, Prof Francois Venter, Holly Fee, Dr Chelsea Kruger, Dr Karlien Moller, Dr Simiso Sokhela, Dr Joanna Woods, all of Ezintsha, University of Witwatersrand; Dr Regina Osih, The Aurum Institute; Prof Glenda Gray, Medical Research Council; Prof Yunus Moosa, Department of Infectious Diseases, UKZN; Prof Wolfgang Preiser, University of Stellenbosch; Prof Lucy Allais, Department of Philosophy, University of the Witwatersrand; Prof Shaheen Mehtar, University of Stellenbosch; Prof Vinodh Edward, The Aurum Institute; Dr Fareed Abdullah, SAMRC and Steve Biko Academic Hospital; Prof Imraan Valodia, Faculty of Commerce, Law and Management, and Director of the Southern Centre for Inequality Studies, University of the Witwatersrand; Dr Aslam Dasoo, Progressive Health Forum; Prof James McIntyre, Anova Health Institute; Prof Eric Decloedt, University of Stellenbosch; Prof Colin Menezes, University of the Witwatersrand; Prof Guy Richards, University of the Witwatersrand; Dr Jantjie Taljaard, University of Stellenbosch; Prof Morgan Chetty, KZNDHC and IPA Foundation.
You can book for your vaccination at any vaccination site across South Africa.
Steps to receiving your COVID-19 vaccine:
Register for the Covid-19 vaccine on the government’s EVDS system.
Visit the confirmed vaccination site on the date and time of your booking.
Take your EVDS SMS as proof of registration and your proof of identity (South African ID or passport) to the vaccination site.
OR
Walk-in to any vaccination site to register and vaccinate.
You can go to any vaccination site or sites close to Wits such as the Liberty site in Braamfontein, the Charlotte Maxeke Academic Hospital in Parktown, the Yeoville Recreational Centre or the Hillbrow Clinic. Wits is working to secure dedicated spots for staff and students at the Liberty site in Braamfontein. More information to follow.
Book a seat on the Wits bus departing from all Wits bus stops (see schedule below)
Bring proof of identity (South African ID or passport) with Wits staff/student card to the vaccination site
Get vaccinated.
Transport
The University has made buses available (with Covid-19 protocols in place) to transport staff and students across campuses to the Liberty vaccination site. This service comes at no cost to staff and students. Use the staff and student link above to book your vaccination date and to book for a bus.
The bus will depart from the Amic Deck, Braamfontein Campus East every 30 minutes at 13:45, 14:15 and 14:45, and from the Parktown Education Campus, Wits Junction and EOH residences every 30 minutes at 13:45, 14:15 and 14:45. Staff and students can also self-drive or walk to the vaccination site.
Vaccinations sites close to Wits
You can also vaccinate at any site of your choice or a site close to Wits such as the Liberty site in Braamfontein, the Charlotte Maxeke Academic Hospital in Parktown, the Yeoville Recreational Centre and the Hillbrow Clinic. Register on EVDSand take your ID or passport with you.
3. Book a seat on the Wits bus departing from all Wits bus stops (see schedule below)
4. Bring proof of identity (South African ID or passport) with Wits staff/student card to the vaccination site
5. Get vaccinated
Don’t hesitate. Vaccinate.
Transport to the SABC vaccination site
The University has made buses available (with Covid-19 protocols in place) to transport staff and students across campuses to the SABC vaccination site on Thursday, 26 August and Friday, 28 August 2021. This service comes at no cost to staff and students. Use the staff and student link above to book your vaccination date and to book for a bus.
The bus to the SABC vaccination site will depart from Wits Junction, Parktown Education Campus, EOH and Amic Deck, every two hours from 09:00, 11:00, 13:00 and 15:00 and return. Staff and students can also self-drive or walk to the vaccination site.
- Prof. Wolfgang Preiser, Cathrine Scheepers, Jinal Bhiman, Marietjie Venter, Penny Moore and Tulio de Oliveira
We are being cautious about the implications for vaccine efficacy and transmissibility while we gather more data to understand this lineage.
As a team of South African researchers we have identified a new lineage of SARS-CoV-2, the virus causing COVID-19. A lineage represents a genetically distinct virus population with a common ancestor. This virus may be designated as a variant in future, based on significantly altered properties, but first we need to understand it better. Our findings so far are set out in a non pre-peer reviewed paper.
The new lineage, assigned the name C.1.2, has been found in all provinces in the country. While it shares some mutations with other variants, it is different in some respects.
Viruses mutate all the time. Sometimes the mutations result in an added benefit for the virus, such as increased transmissibility. But often mutations don’t do anything beneficial for the virus. So more mutations do not always mean trouble for us, its host.
For C.1.2, a lot is still unknown. For example, it’s too early to tell whether these mutations will affect transmissibility or vaccine efficacy.
The Network for Genomics Surveillance in South Africa has been monitoring changes in SARS-CoV-2 since March 2020. South Africa was one of the first countries globally to introduce systematic and coordinated genomic surveillance, sequencing genomes of SARS-CoV-2 from patient samples representative of different geographic regions and over time.
Its findings have provided insights into how and when SARS-CoV-2 was introduced into the country, and into its early spread. The Network has also been sequencing virus genomes to identify newly developing viral lineages of particular concern.
Later in 2020 the network detected what is now called the Beta variant of concern and more recently observed, almost in real-time, the arrival and rapid “take-over” of the Delta variant in South Africa.
What’s known, and what’s not known
We select patient samples from diagnostic laboratories throughout the country and perform sequencing to analyse the virus genomes. We then compare these sequences to those seen before and elsewhere. It’s very much like the game where you spot the difference between nearly identical pictures.
We’re playing spot the difference with SARS-CoV-2. When we find many differences – or differences in certain particularly important places like the spike of the virus – we pay special attention. We then look to see how often we see this particular virus and where – in one region of the country or in multiple regions, only in South Africa or also in other parts of the world. We also monitor whether it increases over time, which would suggest that it is replacing previous versions of the virus.
When we sequence the virus and compare it to other SARS-CoV-2 viruses it gets assigned a name based on the closest matching virus. We then look at the virus and the one that it matches to see how similar they are to each other. If we see a lot of differences that could be an indication of a new lineage.
In May 2021 we first detected a mutated group of related SARS-CoV-2 viruses in South Africa which has been assigned the lineage, C.1.2. So far, from May to August 2021, C.1.2 has been detected in all provinces. Yet it occurs at relatively low frequency and though we see small increases in this lineage overtime they remain very low.
This lineage possesses mutations within the genome that have been seen in other SARS-CoV-2 variants.
The network alerted the World Health Organisation (WHO) and the South African National Department of Health to this lineage in July. The two months between our first discovery and the notification comes from the lengthy process of sequencing and analysis. In addition, mutated viruses appear from time to time – but many disappear again. Therefore we needed to monitor this particular one to see if it would be detected in additional regions. Only when we started detecting it in other provinces and when it was reported also from other countries did we feel we had sufficient evidence to suggest a new lineage.
The surveillance network is continuing to monitor the frequency of the lineage across the country, and helping other African countries do the same. Also, tests to assess the functional impact of the mutations it harbours are under way – for example, how well do antibodies in people who have been vaccinated or infected previously neutralise the new virus, how well does it multiply in cell cultures compared to other virus variants, and so on.
The virus has not yet fulfilled the WHO criteria to be classified as a variant of interest or variant of concern. A variant of interest has genetic changes affecting important virus characteristics (transmissibility, disease severity, immune, diagnostic or therapeutic escape) and epidemiological impacts suggesting a risk to global public health. A variant of concern is the worst category – it’s a variant with proven increased transmissibility and/or virulence and/or decreased effectiveness of public health or medical tools such as vaccines, therapeutics and tests.
Delta is a good example of a variant of concern that rapidly came to dominate the epidemic globally, causing major waves in many countries including those with advanced vaccination roll-out programmes.
The C.1.2 lineage shares a few common mutations with all other variants of concern, including the Beta, Lambda and Delta variants. But the new lineage has a number of additional mutations.
The implications
We are still gathering more data to understand the impact of this lineage on transmissibility and on vaccines.
SARS-CoV-2, like all viruses, mutates with time, usually in a way that affords the virus some kind of advantage. Some of the mutations in the C.1.2 lineage have arisen in other SARS-CoV-2 variants of interest or concern. But we still don’t have a full picture. It will take a combination of ongoing thorough surveillance (especially to see whether it perhaps displaces the currently prevalent delta variant) and laboratory-based studies to characterise its properties.
Based on our current understanding of the mutations in this particular lineage, we suspect that it might be able to partially evade the immune response. Despite this, however, our view based on what we know now is that vaccines will still offer high levels of protection against hospitalisation and death.
We expect new variants to continue to emerge wherever the virus is spreading. Vaccination remains critical to protect those in our communities at high risk of hospitalisation and death, to reduce the strain on the health system, and to help slow transmission. This has to be combined with all the other public health and social measures.
We therefore advise the public to remain vigilant and continue to follow COVID-19 protocol by including good ventilation in all shared spaces and wearing masks that cover your nose, mouth and chin. These non-pharmaceutical interventions are still shown to be preventing the spread of SARS-CoV-2 irrespective of the variant.
We are also of the view that the mutated lineage is unlikely to affect the sensitivity of PCR tests. These tests typically detect at least two different parts of the SARS-CoV-2 genome, which serves as a backup in the case of a mutation arising in one of them. Studies are ongoing to assess any implications for diagnostic testing.
Why vigilance is needed
The Network for Genomic Surveillance in South Africa links National Health Laboratory Service and private COVID-19 testing laboratories to academic sequencing centres. This collaboration has allowed South African experts to rapidly generate and analyse sequence data to inform regional and national responses.
As of late August 2021 the delta variant accounted for over 90% of sequences in Southern Africa. But virus evolution is ongoing, as long as the virus can spread from person to person, multiply, and be passed on. It is thus necessary to continue monitoring its evolution, to detect new problematic properties early and institute countermeasures, where possible.
Covid-19 Update 72: Netcare vaccination site at Wits
- Wits University
Wits staff and students can now get their Covid-19 vaccine at the Netcare site on campus.
The University has collaborated with Netcare to make Covid-19 vaccines easily accessible for members of the Wits community. Wits staff and students will be able to get their Covid-19 vaccination in the Wits Sport Multipurpose Hall, Braamfontein Campus East from 6 September until 23 September 2021.
The Netcare vaccination site is available to staff and students, their immediate family members and household members who are 18 years and older.
All persons accessing the Wits campus and receiving a vaccine must complete the Covid-19 screening tool on the day via the Logbox app. Staff and students can alternatively dial *134*8627# and visitors can dial*120*8501# to complete the Covid-19 screening.
The vaccination site is available as follows:
Date: 6 - 23 September 2021 (Mondays to Fridays)
Time: 08:00 – 16:00
Venue: Wits Sport Multipurpose Hall, Braamfontein Campus East
Parking: Visitor parking is available at the Planetarium visitor parking area.
3. Bring proof of identity (South African ID or passport) with Wits staff/student card and booking confirmation to the vaccination site. People on medical aid will be required to provide their medical aid number. The vaccine is for free for everyone including those on medical aid.
4. Get vaccinated.
Netcare will administer the Pfizer vaccine 1st or 2nd shot. One must be 2 weeks post COVID if recently tested positive, or 42 days post 1st Pfizer shot to receive 2nd Pfizer shot.
Vaccinate at any other site
If you are 18+, you can go to any vaccination site or sites close to Wits such as the Liberty site in Braamfontein, the Charlotte Maxeke Academic Hospital in Parktown, the Yeoville Recreational Centre or the Hillbrow Clinic.
Staff and students choose to protect each other as they receive their Covid-19 vaccination on campus.
Covid-19 has disrupted student activities and Wits’ buzzing campus life. As vaccinations gather momentum across the country, Witsies are rolling up their sleeves in the quest to return to normalcy and revive the vibrant campus life.
Wits University, in partnership with Netcare, launched a vaccination site on campus today, 6 September 2021 in the Wits Sport Multipurpose Hall, Braamfontein Campus East.
The Netcare vaccination site is an initiative to make Covid-19 vaccinations easily accessible to members of the Wits community and their household members. It will operate weekdays between 08:00 and 16:00 until 23 September 2021.
The University has been at the forefront of the fight against Covid-19 through scientific research into vaccines and its involvement in vaccine trials, has now brought vaccines to staff, students and alumni.
Vaccines reduce transmissions
Professor Shabir Madhi, Dean of the Faculty of Health Sciences and Professor of vaccinology said while vaccines may not completely protect people from being infected, they reduce transmission of the virus by 50% and reduce Covid-19 cases.
“The vaccine is the only sustainable manner in which we can go back to a normal lifestyle. It is to ensure that we can protect people, not only preventing people from being infected, but also protecting them from developing severe disease and dying of Covid-19. The only thing that is available to us to achieve that goal is vaccines despite what others may say on social media,” said Madhi.
Vaccinating back to normalcy
Jerome September, Dean of Student Affairs called on the student community to vaccinate, stating that vaccination is a broader responsibility to society.
“While they may not be in the highest of the risk groups, it is protecting themselves that will ensure that the broader society is protected.. The sooner our community gets vaccinated, the sooner we can go back to normalcy.”
The vaccination site on campus will make it easier for students to vaccinate in between their lectures, said September.
Students taking the lead with vaccination
Mpendulo Mfeka, President of the Wits Student Representative Council (SRC), led by example as one of the first few students to vaccinate today. He appealed to students to get their vaccination so they can enjoy the full student experience.
“This is about lives and livelihoods. Even the SRC could not have socials for first years this year. We could not attend classes. A lot of the academic programme has been disturbed by Covid-19. The campus experience has been taken away by Covid-19. We want to encourage students to get vaccinated,” said Mfeka.
Mongezi Sibanda, a third year Bachelor of Science student was the first student to receive the Covid-19 vaccination. He vaccinated because he wants to see Covid-19 over, he said.
“I am tired. I would like to get Covid-19 behind us. We need to do this collectively and vaccinate,” he said.
First year Bachelor of Commerce student, Dipuo Mabasa who was among the students who vaccinated said the site was convenient for her. Mabasa, who is in the University’s netball team, said she took the jab so she can participate in the upcoming netball tournament.
Jacque Du Plessis, Managing Director of Netcare attested to the effectiveness of the vaccines adding that infection rates have decreased among Netcare healthcare workers who vaccinated.
“We need to make sure that we limit the transmission with all the different variants. Even if we can do 100 vaccinations a day, we are moving in the right direction towards normalcy.”
The vaccination site accepts walk-in’s in order to leave no one behind. People will be assisted with the registration process at the site.
How Messenger RNA works in nature and in making vaccines
- Kristie Bloom
Thanks to the collaborative efforts, the large-scale manufacturing of mRNA drug products is becoming a reality.
Vaccines have long been an integral part of public health programmes around the world, reducing the spread and severity of infectious diseases. The success of immunisation strategies to protect children from diseases like polio, hepatitis B, and measles, and adults from influenza and pneumococcal disease, can be seen globally.
The COVID-19 pandemic created an urgent need for an effective vaccine. This is where messenger RNA (mRNA) vaccines, which are classified as a next-generation technology, gained prominence. Decades of research and clinical development into synthetic mRNA platforms for cancer treatments and vaccines for infectious diseases like influenza, malaria, and rabies, finally paid off as both Moderna and Pfizer/BioNTech’s COVID-19 mRNA vaccines received emergency use authorisation. As a result, mRNA technologies have been catapulted into the public spotlight.
Developing synthetic mRNA into vaccines
Ribonucleic acid (RNA) is a natural molecule found in all our cells. There are many types of RNA, each with distinct functions. As the name implies, mRNA acts as an important messenger in human cells. These molecules carry unique codes that tell our cells which proteins to make and when to make them. The code is copied from a strand of DNA in the nucleus of the cell, in a process called transcription. The mRNA is then transported into the cytoplasm (the solution contained in the cell) where the message is ‘read’ and translated by the cell’s protein production machinery. The result is an important protein, such as an enzyme, antibody, hormone, or structural component of the cell.
Nearly 40 years ago scientists found that they could mimic transcription and produce synthetic mRNA without a cell. The process, known as in-vitro transcription, can generate many mRNA molecules from a strand of DNA in a test tube. This requires an enzyme (called RNA polymerase) and nucleotides (the molecules that are the building blocks of DNA and RNA). When mixed together, the polymerase reads the strand of DNA and converts the code into a strand of mRNA, by linking different nucleotides together in the correct order.
When in vitro transcribed mRNA is introduced into a cell, it is ‘read’ by the cell’s protein production machinery in a similar manner to how natural mRNA functions. In principle, the process can be used to generate synthetic mRNA that codes for any protein of interest. In the case of vaccines, the mRNA codes for a piece of a viral protein known as an antigen. Once translated, the antigen triggers an immune response to help confer protection against the virus. mRNA is short-lived and does not change the cell’s DNA. So it is safe for the development of vaccines and therapies.
A major advantage of in vitro transcription is that it does not require cells to produce the mRNA. It has certain manufacturing advantages over other vaccine technologies – rapid turnaround times and reduced biological safety risks, for example. It took only 25 days to manufacture a clinical batch of Moderna’s lipid nanoparticle mRNA vaccine candidate, which in March 2020 became the first COVID-19 vaccine to enter human clinical trials.
Importantly, as in vitro transcription is cell-free, the manufacturing pipeline for synthetic mRNAs is flexible and new vaccines or therapies can be streamlined into existing facilities. By replacing the DNA code, facilities can easily switch from producing one kind of mRNA vaccine to another. This not only future-proofs existing mRNA production facilities but could prove vital for rapid vaccine responses to new pandemics and emerging disease outbreaks.
How do mRNA vaccines work?
The mRNA vaccines we are familiar with today have benefited from many years of research, design and optimisation. Understanding how synthetic RNA is recognised in cells has proven essential in developing effective vaccines. Typically, the mRNA codes for a known viral antigen. In the case of COVID-19 mRNA vaccines, sequences coding for the SARS-CoV-2 spike protein or the receptor-binding domain have been used. These antigen-encoding mRNA molecules are incorporated into very small particles made primarily of lipids (fats). The lipid particle has two main functions: it protects the mRNA from degradation and helps deliver it into the cell. Once in the cytoplasm, the mRNA is translated into the antigen which triggers an immune response.
This process is essentially a training exercise for your immune system, and it normally takes a few weeks for your adaptive immunity to mature and synchronise. mRNA vaccines have been shown to stimulate both arms of the adaptive immune response, which are important for establishing protection. Humoral (B cell) immunity produces antibodies while cellular (T cell) immunity helps to detect infected cells. The current mRNA COVID-19 vaccine schedule uses a two dose (prime-boost) approach, which aims to strengthen your adaptive immune response towards the SARS-CoV-2 virus.
Another type of mRNA vaccine, referred to as self-amplifying RNA, may only require a single low dose to achieve the same level of protection. In a cell, these self-amplifying RNA vaccines can copy the mRNA code. This means that more antigen can be produced from less RNA. Several COVID-19 RNA vaccines currently in clinical trials are exploring self-amplifying RNA technologies.
mRNA vaccines beyond COVID-19
It is an exciting time for mRNA technologies. Thanks to the collaborative efforts of governments, funding agencies, academia, biotech and pharmaceutical companies, large-scale manufacturing of mRNA drug products is becoming a reality. The success of Moderna and Pfizer/BioNTech’s COVID-19 vaccines has helped re-energise ongoing mRNA research.
Both mRNA and self-amplifying RNA have shown potential as vaccines for multiple infectious diseases including influenza, respiratory syncytial virus, rabies, Ebola, malaria and HIV-1. Coupled with therapeutic applications, most notably as immunotherapy for the treatment of cancers, mRNA technologies will continue to improve and expand, forming an integral part of future drug development.
Covid fallout: Vulnerability and signs of recovery in Gauteng
- Gauteng City-Region Observatory
There is no doubt about the enormous scale of the shocks South Africa has experienced over 2020-21.
New survey resultslaunched on 9 September by the Gauteng City-Region Observatory (GCRO)reveal just how much socioeconomic fallout the Covid-19 pandemic has caused for Gauteng. A full 11% of all adults in the province have lost a job since March 2020, while 4% were forced to permanently close a business. Of those who lost a job or closed a business, only 44% subsequently found new employment. There are, however, also indications of positive responses from both the government and society as a whole. Almost one quarter of households in Gauteng included an adult who received the Covid-19 Social Relief of Distress grant, while 13% received food support, while levels of community trust have risen dramatically.
These numbers from the GCRO’s sixth Quality of Life Survey capture contradictory household experiences of what is undoubtedly an epoch-defining moment in our history.
The Covid-19 pandemic has brought two new kinds of threat to survival. First, the virus itself has caused enormous loss of life. At the time of writing excess deaths across South Africa stood at about 250,000 since the start of the pandemic, and these continue to grow at more than 5,000 each week.
Second, large parts of the economy and society have been constrained or suspended altogether. Ordinarily people survive and thrive in cities precisely because urban living enables them to move around and interact. While no doubt a necessary response to the public health shock of Covid-19, the injunction to stay at home has triggered extensive socioeconomic shocks. Jobs have been whacked, along with education and many urban amenities – including local libraries, restaurants and train services – that we used to take for granted. As we all understand well, these health and socioeconomic shocks landed in a context where the ability of a significant portion of the population to survive was already extremely precarious.
When societies are hit by an unexpected shock – drought, flood, earthquake or pandemic – households may be cut off from their means of survival. Those that have something to fall back on – savings, social networks, a “plan b” – can absorb shocks and re-establish themselves once it is possible. Since poor households typically have very little to fall back on they arevulnerable,and may not be able to make it to the other side of the crisis without help. In such contexts, it cannot be expected of all households to be independently resilient. Instead, responsibility for the resilience of individuals is in the hands of society at large, through its ability to provide the means of survival to the vulnerable. As we pick up the pieces from the crisis, we need to ask hard questions about whether we have done enough to ensure both individual and collective resilience, and what other mechanisms could be established for a better post-crisis future. To answer these questions we need more nuanced insights into how different kinds of households and parts of society have been differentially affected in the crisis. Here, data from large-scale socioeconomic and attitudinal surveys can be crucial.
From October 2020 to May 2021, Quality of Life Survey fieldworkers visited each of the province’s 529 wards, interviewing a total of 13,616 adults who were carefully sampled to be representative of the inhabitants of the province. Comparing these results to those from the five previous surveys in this series allows us to see both continuities and changes in the wake of the pandemic. The survey is wide ranging, with more than 200 questions on a wide variety of topics, providing evidence of the multidimensional knocks the province has taken over the past year.
First, the survey results show the ways in which everyday behaviour in Gauteng has changed since the arrival of Covid-19. For example, nine out of 10 respondents stated that their households had avoided public spaces and gatherings. One-third of households changed where or how they bought groceries. Trips out of the home are now less likely to be for work, and are more likely to be shorter than in the past. Some changes, initially required by regulations, did not snap back immediately to pre-pandemic norms once regulations were lifted. For example, two-fifths of households with children kept them away from school evenafterthey were allowed to return.
The impact of children being kept out of school is compounded in many of these households by limited access to home internet and computers. Three out of every five households with children under the age of 18 do not have a working computer, and four out of every five of these households do not have a home internet connection. This would have severely constrained options for children’s learning at home, even though families and schools have adapted in different ways to learning and teaching in the pandemic. School closures and the health crisis in general have also disproportionately impacted women, 40% of whom spent more time than usual looking after children or other family members since March 2020, compared with only 18% of men.
The survey shows the scale at which people lost work in Gauteng, whether due directly to lockdown restrictions, or a more general loss of demand. Over and above the 4% of all adults who had closed a business permanently, and the 11% who lost a job, 19% took a cut in salary and working hours since March 2020. Importantly, of those who had lost a job or closed a business, 50% have been unable to find new work, and 7% have dropped out of the labour market altogether. However, white respondents, and those with higher levels of formal education, were notably more likely to have found new jobs than black African respondents, or those with lower levels of education. This provides a stark example of the differential ability of people to “bounce back” from shocks.
Other variables also illustrate the variations inability to cope, with some households and individuals more vulnerable than others. For example, the percentage of low-income respondents who recently missed a debt repayment went up, while the percentage of high-income earners who missed a debt repayment decreased.
In a context where the proportion of Gauteng’s households living below the average poverty line has risen to 36%, from 25% in 2017/18 (the last time the Quality of Life Survey was run), how have vulnerable households been able to survive? Here the role of the state is crucial, not only in continuing to provide the infrastructure and services that make urban life possible, but also through safety nets to help households meet their needs in the absence of sufficient work. In total, almost half of all Gauteng respondents (48%) said that someone in their household received a social grant of some kind. This was up from 42% in 2017/18. In May 2020, the Covid-19 Social Relief of Distress grant was introduced for people who were unemployed. Almost a quarter (23%) of survey respondents indicated that someone in their household was receiving this R350 grant. While grants are no doubt essential to those who receive them we should note that R350 is one-tenth the minimum wage, and as such is not a replacement for decently paid employment.
We also see evidence of broader social support in the survey data. More than one in 10 respondents received food support, whether from the government or an NGO, since March 2020. Levels of community trust have increased substantially since 2017/18, continuing an upward trend from 2015/16. However, community trust levels remain notably lower for black African and coloured respondents than for Indian/Asian and white respondents. Participation in organised social activities such as church, stokvels or sport actually increased very slightly relative to 2017/18, despite lockdown regulations limiting in-person gatherings for much of 2020. Participation increased most substantially among individuals reporting extremely low household incomes, suggesting that these activities might have provided an element of support for Gauteng’s poor during the pandemic.
Despite various forms of support, results from the survey show that the pandemic has taken a toll on people’s physical and psychological wellbeing. Self-reported health, overall satisfaction with life, and mental health have all worsened relative to 2017/18. Using a screening tool for depression, our data show that 14% of Gauteng’s residents are at high risk of depression. This is an increase from 12% in 2017/18. Those who experienced at least one of the five economic impacts highlighted above are far more likely than the average to be at high risk of depression. Mental health services must be prioritised in Gauteng’s recovery, although the overburdened public healthcare system is struggling to cope with the pandemic, and even basic healthcare needs are going unmet: 7% of adults in Gauteng have struggled to access healthcare since March 2020, and more than 2% have been turned away when requesting a Covid-19 test.
Since the survey interviews were concluded in May 2021, Gauteng has experienced a particularly brutal third wave of Covid-19 infections and extreme civil unrest. Our data cannot reflect how these additional shocks have affected Gauteng’s residents. However, the results from the Quality of Life Survey 6 (2020/21) speak to the context in which these events occurred: one in which many more households are more broadly vulnerable, across multiple socioeconomic fronts. We can only anticipate that more recent events have intensified the vulnerability of many households.
Analyses of disasters show that shocks can set vulnerable households back well beyond the duration of the crisis itself. The fact that some households have been less able to cope with the multifaceted shocks triggered by Covid-19 underscores the importance of collective responses. As the geographer Neil Smithargued, it is not inevitable that some people should struggle to survive – to leave vulnerable people stranded is a societal choice. Given the reach achieved through social grants, and the fairly widespread provision of food support, there is no doubt that positive steps have been taken. These measures have gone at least some way in helping vulnerable households and individuals survive. But looking back we can ask whether additional support might not have softened the blows for the many still not coping. And looking to a post-crisis future we need to consider seriously how we might institutionalise systems of care for those who have been disproportionately affected, and are unable to achieve resilience on their own.
The writers are with theGauteng City-Region Observatory: Dr Richard Ballard (specialist researcher); Dr Julia de Kadt (senior researcher); Graeme Gotz (director of research strategy); Christian Hamann (researcher); Sthembiso Pollen Mkhize (research intern); Yashena Naidoo (junior researcher); Dr Alexandra Parker (senior researcher); Rashid Seedat (Executive Director).
Details on vaccination and the return of staff members to campus.
President Cyril Ramaphosa announced on Sunday evening that South Africa has moved to Adjusted Alert Level 2, thereby easing several regulations, which impacts on members of the Wits community, as detailed below.
At the outset, the Senior Executive Team (SET) strongly recommends that all staff members get vaccinated as soon as possible – it is our collective responsibility, and it is in the best interests of our community and society. It is also our best chance at minimising the impact of another resurgence of the virus, and getting back to normal as soon as possible. For these reasons we are working on a vaccination policy, which will be circulated in the coming days.
The Wits Netcare Vaccination Site has been established in the Multipurpose Hall on the Braamfontein Campus to vaccinate the broader Wits community (including family members and friends). The site is open Mon-Fri from 08:00 – 16:00 until 23 September 2021. Walk-ins are welcome, and everyone above 18 years of age can be vaccinated.
Staff and students can also vaccinate at any convenient site, including the Liberty Vaccination Site in Braamfontein and the Charlotte Maxeke Johannesburg Academic Hospital in Parktown.
Academic Staff
The teaching and learning programme will continue as per the respective faculty timetables, and in the modes determined and specified by faculties. Academics and researchers are required to be accessible for academic and research purposes, and for postgraduate supervision.
All staff, postgraduate students and postdoctoral fellows can continue with research on campus, and must adhere to all Wits’ COVID-19 protocols when on campus. The same applies to students serving on clinical training platforms, students attending in-person lessons, and those requiring access to studios and laboratories, as determined at the faculty level. Libraries will open in line with regulations issued by government.
Professional and Administrative Staff
All University entities are required to be fully operational as we strive to fulfil our mandate to deliver academic, research and service excellence in the 2021 academic year.
Professional and administrative staff are accordingly required to report for duty on campus, in line with the directives of their respective senior executive member, who is authorised to determine and approve the level of staff required in their faculty or division. Line managers and Heads of School are also required to act in accordance with the directives of their respective faculty dean or senior executive member.
Workplace Safety
The health and safety of every member of the Wits community is paramount, and again, it will require our collective effort to keep everyone safe.
Staff members are required to:
Complete the self-screening form via the Wits LogBox Screening App every day before entering campus;
Wear a mask over the mouth and nose, and especially when in close proximity to others;
Refrain from gathering in spaces that are not adequately ventilated and to rather hold meetings outdoors (no gatherings are allowed in tearooms and canteens); and
Abide by all Wits’ COVID-19 policies and protocols.
Responsibilities for Line Managers
Line managers must update the Occupational Health and Safety risk assessment for their respective entity and must implement the risk mitigation measures before staff members return to the workplace.
Line managers must work with their assigned human resources officers, health and safety officers and representatives, PIMD, Services, and other relevant entities, to ensure the safety of staff members, and especially that the following measures are in place:
the physical distancing of staff members in the workplace;
the regular cleaning of venues and work spaces;
the provision of personal protective equipment for specialised areas (and ensuring that it is correctly worn); and
the adherence to Wits’ COVID-19 protocols to prevent the spread of infection.
Conclusion
Let us take the necessary precautions to ensure our own personal health and safety and that of our colleagues, students and friends, as we return to campus. We strongly advise that the most sustainable manner by which to protect yourself and reduce your chances of infecting others is to be vaccinated against Covid-19.
Please speak to your line manager or relevant executive should you have any further queries about the return to campus plans.
Millions of children miss routine vaccinations amid the chaos of Covid-19
- Wilmot James, Lawrence Stanberry and Jeffray Tsai
Urgent catch-up plans are needed.
Countries need to develop strategies to re-establish routine childhood vaccination programmes and develop catch-up programmes for those children who have missed their routine childhood vaccines.
Wilmot James is a Senior Research Scholar, Lawrence Stanberry a Professor of Pediatrics and Jeffray Tsai a research assistant at Columbia University. James is also an Honorary Professor of Public Health at the University of the Witwatersrand
In April 2020, the World Health Organization warned that postponing vaccinations due to the imposing urgency of the Covid-19 pandemic will result in children dying from utterly preventable diseases. The world’s focus on Covid-19 is understandable, but the tragic result is the neglect of many other health challenges officials have laboured on for years.
Vaccination is a mainstay of preventing illness and reducing mortality in low- and middle-income countries, particularly in children under five years of age, but, regrettably, routine childhood vaccinations have fallen behind since the beginning of the pandemic, making children more susceptible to preventable diseases such as measles and tetanus.
In 2020,23 million childrenwere not able to meet their routine immunisation services, 3.7 million more than in 2019. On specific vaccinations, when comparing numbers to 2019, 3.5 million more children missed theirDTP-1 vaccineand three million theirfirst measles shot. This is a significant number of children that missed their routine vaccinations in 2020.
United Statesdata indicated that childhood and adolescent vaccinations were substantially lower during March-May 2020 compared with the average administered during the same period in the previous two years. Although the number of children and adolescents vaccinated between June and September 2020 rebounded and approached pre-pandemic levels, the increase was not enough to achieve the catch-up vaccinations needed, leaving large numbers of children still susceptible to vaccine preventable diseases.
Most countriesreported at least some disruptions to essential health services, with routine immunisation interference among the most frequent. Reasons for disruptions included restrictions placed on movement and travel; the closure of facilities due to the redeployment of health workers to Covid-19 wards; inadequate supply of personal protective equipment and the postponement of non-urgent medical care because of concerns about viral exposure.
Inparts of the United States, increasing Covid-19 vaccine hesitancy has spilled over to impact attitudes about the safe and effective vaccines that have been used for decades in routine immunisation programmes. Countries have been placed on alert for this insidious vaccine hesitancy creep that could undo years of progress in driving down childhood mortality.
The numbers are concerning, but they did not drop as much as initially assumed.
The CEO of the Bill and Melinda Gates Foundation, Mark Suzman, has said that vaccination ratesdid not drop as low as the 14%predicted by the Institute for Health Metrics and Evaluation. Still, that is still enough to backtrack on years of progress.
High-income countries are able to make progress despite the backtracking, but middle-income countries may not be as fortunate.Middle-income countrieshave an increasing number of children unvaccinated against preventable diseases. Similar to Covid-19 vaccine accessibility, there needs to be equal access to vaccines in general to be able to prevent all diseases.
With the more concerning variants of SARS-CoV-2, there is likely to be continued disruption of childhood vaccinations.
Countries need to develop strategies to reestablish routine childhood vaccination programmes and develop catch-up programmes for those children who have missed receiving their routine childhood vaccines. These include:
Ensuring the safety of all vaccine workers by placing them among the top tier of people receiving the Covid-19 vaccines.
Restoring vaccination campaigns with special emphasis on catch-up vaccinations and identifying communities that are under-vaccinated.
Ensuring all routine vaccination sites are open and adequately staffed.
Providing transportation fees to ensure parents can take children to vaccination appointments.
Redoubling efforts to reduce vaccine hesitancy.
Children’s health delayed may well become children’s health denied, which, given the capability of today’s medicine and public health, is simply unforgivable.
James is a Senior Research Scholar, Stanberry a Professor of Pediatrics and Tsai a research assistant at Columbia University. James is also an Honorary Professor of Public Health at the University of the Witwatersrand.
Next week, daily between 27 September and 1 October, Columbia University and the University of the Witwatersrand will host a virtual symposium on “Effective ways to Increase Vaccination Rates”. You can find the daily programme and registration detailshere.
Yet hesitancy may be a significant barrier to the success of South Africa’s vaccine programme — a survey by the Human Sciences Research Council in June and July this year showed that28% of the 8 000 respondents were reluctant to be vaccinated.
The raging question for South Africa is not so much aboutwhetherthe government should consider a COVID-19 vaccine mandate, but rather whether theycan. And the short answer is yes.
Leveraging the law: How to mandate vaccines
The government could call on two laws that would allow them to make getting a COVID-19 vaccine compulsory, if it ever came to that.
Every doctor or nurse in both the public and private health sector who diagnoses a patient with a notifiable condition has to report it to the National Institute of Communicable Diseases — failure to do so is a criminal offense.
Under the Notifiable Medical Conditions Regulations, a healthcare provider would be allowed to administer a vaccine even if a person refuses to accept it. But this is not as totalitarian as it sounds: a court has to decide whether this would be a justified action. The process is complicated, because the head of the provincial department of health would have to apply for a court order and then the court must assess – on a case-by-case basis – whether compelling the person to take a vaccine without their consent is justified.
Another route that could be used to justify mandatory vaccination is theregulations issued under the state of disaster declared in March 2020, which are used to regulate South Africa’s COVID-19 response. Under these regulations, a person can be compelled to undergo COVID-19 testing, isolate if infected — and potentially also be vaccinated. It would still have to be a court order, but the process is slightly easier as such an application can be lodged by people from a wider range of sectors — for example, healthcare workers, government officials or certain ranks of police officers — and the order can be granted by a magistrate’s court.
Both these avenues have been used in the past to institutemandatory isolation and quarantineor evento enforce treatmentfor conditions that pose a significant public health risk. But in the context of making COVID-19 vaccination compulsory, they are unlikely to be feasible options.
Keeping our options open: How to incentivise mass vaccination
When authorities look to introduce vaccine mandates, they generally try to incentivise people to get vaccinated. This means being vaccinated can be a requirement to do certain things, while non-adherence may result in some form of penalty.
For example,US Federal Policynow requires that government workers either be vaccinated or submit to weekly testing. The City of New York also recently instituted theKey to NYC– a pass granting people access to indoor activities such as restaurants, performances and gyms provided they have been vaccinated against COVID-19. The use of similar vaccination certificates has recently also been announced inIsrael, theEuropean Unionandsome provinces in Canada.
The practice is not new, and South Africa already has some mandates in place to encourage specific vaccinations.
For example, the department of basic education requires parents to submit their child’s immunisation cardwhen applying for Grade 1 enrollment, to prove that the child has been vaccinated against vaccine-preventable childhood diseases such as measles, polio and whooping cough. Although admission currently cannot be refused if a child is not vaccinated, the department isin the process of introducing a policythat would prevent unvaccinated children from being admitted to public schools.
Another example is theyellow fever vaccine passport, which was instituted in line with the World Health Organisation’sInternational Health Regulations. Anyone who wants to travel to an area with a high risk of yellow fever must prove that they have been vaccinated against the disease before being allowed to enter that country or to re-enter South Africa. Those who do not want to be vaccinated are not forced to take a vaccine, but are prohibited from travelling.
To vax or not? Workplaces may not give you the option
Internationally, a number of private companies are moving towards making COVID-19 vaccines mandatory for their employees, and South Africa is already following suit.
On 2 September 2021, Discovery announced thatCOVID-19 vaccination will be mandatory for all stafffrom 1 January 2022. Adrian Gore, CEO of Discovery, explained that the decision was motivated byboth a moral and a legal obligationto provide a safe working environment for their employees. Since Discovery’s announcement, a number of other organisations, includinguniversitiesand private companies, have implemented similar policies, or are considering them.
The Constitution vs COVID: A balancing act of rights
Some legal commentary argues that making the COVID-19 vaccine compulsorywould be a violation of constitutional rights, including the rights to bodily integrity, freedom of religion, and dignity. And although it is true that mandatory vaccination may limit these rights, it is important to recognise the flip side: no constitutional right is absolute.
This means that any right in the bill of rights can be limited if justified under section 36 of the Constitution. For example, if the prosecution needs an accused’s blood as evidence to support their case, the person’s right to bodily integrity can be limited and he or she can be compelled to have a blood sample drawn.
What has also often been overlooked in citing individual rights in the argument against mandatory vaccination is that the courts have found far-reaching limitations to be justifiable during the COVID-19 pandemic. For example, the High Court in Pretoria found thatclosing mosques as part of lockdown measureswas a justifiable limitation of the right to freedom of religion. The argument was that the measure would assist in controlling the pandemic, and the court specifically recognised the concept of ubuntu — calling on citizens to make sacrifices to their individual rights for “the greater good” of curbing the pandemic.
Similarly, the Supreme Court of Appeal recognised the “trade-off” between individual liberties and curbing the spread of COVID-19 in a judgment that found theregulations of the state of disaster to be largely constitutional. The ruling came down to the court saying that limiting individual liberties such as the right to freedom of movement and the right to dignity was justified because it protects the right to life of people who may otherwise have been vulnerable to dying from COVID-19.
Responsibility and rights: A legal roadmap for vaccine mandates
Although the law allows for potential mandatory COVID-19 vaccination in South Africa, what this looks like in practice will depend not only on the government but also on the private sector. Arguably, vaccines are more invasive than closing mosques or preventing the sale of alcohol. And as there are no specific cases testing the constitutionality of vaccine mandates, prior court rulings can provide only a guide to the approach.
The complex, multilayered practicalities of enforcing COVID-19 vaccination mean that vaccine mandates will have to be developed responsibly. In some contexts, such as frontline healthcare, a hardline approach may be warranted and the limitation of individual rights could be justified.
But it might not apply in all contexts. Some individuals may have valid, medical reasons for not being able to take a COVID-19 vaccine; others may be objecting on religious grounds or work in low-risk environments where their decision not to be vaccinated poses little risk to others. Outside of work environments, vaccine mandates could be used to incentivise rather than enforce vaccination, without significant incursions on individual rights.
In the end, decisions about mandatory COVID-19 vaccination may ultimately be informed by our individual actions. Because with every right also comes a responsibility.
Safura Abdool Karim is a public health lawyer at the University of the Witwatersrand (Wits). She also consults for a health policy research unit funded by the South African Medical Research Council and Wits, the Centre for Health Economics and Decision Science (Priceless).
Wits-educated billionaire launches R3-billion vaccine development project in SA
- Wits University
It will help to establish two research centres to boost cancer and vaccine research at the University of the Witwatersrand.
Wits University alumnus and South African-born biotech billionaire, Dr Patrick Soon-Shiong, has officially launched the ambitious R3-billion initiative to build capacity for advanced health care in Africa.
Wits is one of the leading universities to benefit from this partnership that will focus on the rapid clinical development of next generation vaccines for infectious diseases, including Covid-19 vaccines, and cancer at centres of excellence across the country.
Wits has already identified the establishment of a new Centre of Excellence in Oncology and the Wits Infectious Diseases Research Institute in the Faculty of Health Sciences.
The initiative is driven by NantAfrica, a division of NantWorks which is Soon-Shiong’s multinational, California-based conglomerate that is leading the digital revolution in healthcare, technology and media through the harnessing of science, digital infrastructure, supercomputing and communication.
“Wits University is honoured to partner with NantWorks to advance the research and clinical development of vaccines, and training and technological innovation in oncology, infectious diseases, immunology, molecular medicine, and related disciplines, in Africa. This will ultimately result in improving the lives of many people,” says Dean of the Faculty of Health Sciences, Professor Shabir Madhi, a vaccinologist, and world-leader in his field.
“This collaboration will provide further growth in the world-class research undertaken by Wits scientists in the field of infectious diseases, and provide opportunities for cutting edge research in the field of immunotherapy in the management of cancer.”
Professor Zeblon Vilakazi, Wits Vice-Chancellor and Principal, welcomed the collaboration, saying this relationship is “particularly special as both Dr Soon-Shiong and his wife Michelle are Wits alumni, who met on our campus.”
“This collaboration speaks directly to the priorities of Wits University as we approach our centenary – to improve health care using the latest technology and innovation, to benefit broader society, and to advance the public good. We look forward to working with the team to conduct research at the frontiers of science, that addresses the pressing challenges of the 21st Century, and that ultimately advances better healthcare for humanity,” says Vilakazi.
Professor Shabir Madhi had a discussion with Dr Soon-Shiong in March 2021 about COVID-19, his thoughts and ideas on vaccine development in South Africa, and how scientists can be engaged.
NantAfrica also wants to tap South African medical expertise in treating diseases that are prevalent in the country such as HIV, tuberculosis, human papillomavirus and cervical cancer.
South African President Cyril Ramaphosa it’s an opportunity to address the public health challenges experienced in South African and the continent and leapfrog to cutting edge technology.
“It is a game changer for our country. This technology transfer, including manufacturing biologics, will reinforce vaccine equity sorely needed globally,” he said during the online media conference.
NantAfrica also wants to tap South African medical expertise in treating diseases that are prevalent in the country such as HIV, tuberculosis, human papillomavirus and cervical cancer.
Head of UNAIDS unpacks the knock-on effects of Covid-19
- Imraan Valodia
Greater urgency is needed in the response to pandemics, to end AIDS and to end COVID-19.
The COVID-19 pandemic has deepened global inequities. The world’s poor have bore the brunt of national lockdowns and will struggle to recover and poorer countries have been unable to rollout comprehensive vaccination campaigns because of a grossly unequal distribution of vaccines. On top of this COVID-19 has also derailed progress against diseases that affect poor people. Imraan Valodia sat down for a conversation with Winnie Byanyima, the Executive Director of UNAIDS.
Imraan Valodia: What impact has COVID-19 had on the fight against HIV in countries, particularly those in the global South, carrying the biggest burden of the disease and with significantly weaker healthcare systems?
Winnie Byanyima: Firstly, we must recognise the successes of the AIDS response. We have achieved what many once said was impossible. Of the 38 million people living with HIV, 27.5 million are accessing lifesaving antiretroviral therapy. We have cut the rate of new HIV infections by more than half and averted 16.6 million deaths.
Hundreds of thousands are still dying of AIDS and 1.5 million people were newly infected last year. AIDS remains a crisis and COVID-19 is making it worse.
Even before COVID-19, we were off track in meeting the global AIDS targets and the COVID-19 pandemic has pushed us back even further. COVID-19 related restrictions have hurt the most vulnerable, including marginalised and stigmatised communities and has disrupted access to HIV services.
Since COVID-19 hit, the Global Fund to Fight AIDS, TB and Malaria estimate that the number of mothers receiving prevention of mother to child transmission services dropped by 4.5%, people reached with HIV prevention programmes declined by 11%, HIV testing declined by 22% and medical male circumcision to prevent HIV dropped by 27%.
In very high prevalence settings in Africa, it is estimated that the effects of COVID-19 could contribute to a 10% increase in HIV deaths over five years.
Amid unprecedented global disruptions, we must act urgently to prevent a resurgent global AIDS pandemic and to quickly recover our progress toward ending AIDS. To get fully back on track on HIV we absolutely have to get on top of COVID-19.
Imraan Valodia: COVID-19, like HIV, has deepened inequalities in society and disproportionately affected women while widening the long-existing gender pay gap. How do we begin to address this gender economic and inequality pandemic?
Winnie Byanyima: Both COVID-19 and HIV are feeding off inequalities: women whose rights are not respected; women who do not have economic security or access to the most basic health or education services. These are the people that pay the heaviest price of our inaction on inequality. They pay the price in insecurity, in poverty, in sickness, and too often in death.
Five in six African adolescents newly acquiring HIV are girls. The reason is power. Research shows that completion of secondary education reduces a girl’s risk of acquiring HIV by up to half, and by even more if this is complemented by a package of rights and services. Yet as countries struggle with the current fiscal challenges, education and girls’ empowerment are among sectors that are suffering the biggest budget cuts.
Governments also have a responsibility to shift the burden of care away from women’s invisible unpaid labour. Affirmative action is essential to counteract the legacy of discrimination against women.
Economic interventions are needed to overturn the gross imbalance of wealth. But ending the age of inequality requires the strengthening of emancipatory social and cultural forces to overturn the gross imbalance of power in all its interconnecting forms.
Imraan Valodia: You say that extreme inequality is not inevitable – it’s a policy choice – explain what you mean by this? What roles can individuals, communities, and nations play to end it?
Winnie Byanyima: There is a pandemic of inequality – between men and women, between the South and the North; between dominant and marginalised communities, between the elite and the majority – which hold back our enormous potential.
Inequalities are perpetuated by laws, by informal rules (social norms), by national social and economic policies and resource allocation, and by global policies and finance. And key to determining all those outcomes are inequalities of voice and power.
In the face of the colliding crises, it has become clear that we need bold new approaches to how we survive and thrive. Action is needed at all levels – not to build a perfect world but to enable a resilient one.
The answers are being articulated by activists and organisers, particularly young people from the most marginalised communities. They are showing how to build societies able to overcome any crisis and to unleash the potential of all. They have done so because the people most impacted are those who understand it best.
As a UN leader, I have experienced the power of the pressure of communities, women’s groups and grassroots movements, pushing us; at times that pushing is uncomfortable for us; but my message to you is:
Keep pushing!
Imraan Valodia: What lessons can we learn for the management of future pandemics from the triangle of science, government and communities that was in place in dealing with HIV?
Winnie Byanyima: We have learned a lot about how to fight pandemics. This year marks 40 years that we have been fighting AIDS and our successes and failures have taught us that we cannot successfully conquer a pandemic without working together to end inequalities, promote people-centred approaches, engage communities, and respect human rights.
This is one of the most challenging moments in the history of HIV and global health. We need greater urgency in our response to pandemics, global solidarity behind a data-driven global plans to end AIDS and to end COVID-19, and partnerships to prepare to respond to the next threat.
We need to draw from the collective experience, brilliance and value set of the AIDS response. If we apply the hard-earned lessons of AIDS up front, we will increase our odds of winning.
This article is part of a media partnership between the Southern Centre for Inequality Studies and The Conversation Africa for its 2021 annual Inequality Lecture, which is being presented on Thursday, 30 September. Register for the lecture here.
Palliative care and Covid-19: A patient’s quality of life and dignified death are paramount
- Desia Colgan, Nicola GunnClark and Emmanuel Kamonyo Sibomana
Calls to permit nurses in South Africa, Kenya and Tanzania to prescribe morphine to help ease patient's suffering and give them a dignified death.
Human beings have a right to live a life with dignity which is free of suffering, pain and stigma, no matter how short their life may be. When it comes to people who are living with a serious condition or illness the question is,how can quality of life be ensured?
The reality is many seriously ill patients, particularly in Africa, struggle with ever-increasing pain, finally dying without relief while immediate carers, often loved ones, stand by helpless and emotionally broken. This suffering is as a result of limited access to oral liquid morphine, a situation exacerbated by the lack of knowledge on how to administer pain-relieving medicine. It is unfortunate that governments overlook the fact that greater access to pain relief and wide training of healthcare workers would mean that, for people who are seriously ill, pain relief, control of symptoms and a good quality of life are possible.
In southwest Uganda, things are a little different. Patients with advanced illness are served by a palliative care unit atKitagata Hospitalreaching a catchment population of almost 40,000 people in greater Bushenyi District.
Between April and May 2020, when the global Covid-19 crisis struck, hospital services were disrupted worldwide. For the newly established palliative care unit, inpatient palliative care consultations were interrupted, and visits to patients at home severely limited or even discontinued. Appointments were postponed due to the risk of infection, so patients could not come to hospital and could not send family members or carers to collect drug refills.
Mukazi battled breast cancer alone
This is the situation faced by 48-year-old Brigit Mukazi (not her real name), who has advanced breast cancer.
Mukazi lives in Ntungamo District, which is outside the hospital catchment area. For more than five days she called for pain relief and was cut off from palliative care assistance at the hospital due to the high cost of hiring special transport during Covid because there was no public transport available due to the restrictions. Mukazi was facing the prospect of ever-worsening quality of life with escalating pain, increasing symptoms of her breast cancer and within a few months, the inevitability of a miserable, painful end to her life.
This situation is the reality for most seriously ill patients in developing countries across the world today.
What happened to Mukazi?
To answer this question we have to go back to the years before Covid-19 struck, when thePalliative Care Association Uganda (PCAU)sent a nurse to be trained in palliative care. Once qualified this nurse, Catherine Nakasita, set up the first palliative care unit at Kitagata Hospital. The hospital management provided a double-entry cupboard system for the palliative care unit to store oral morphine, and also allowed Nakasita access to the national medical stores which ensures a continuous supply of morphine and other essential palliative care drugs.
When Covid-19 struck, palliative care unit services were severely disrupted and Nakasita witnessed a crisis of need unfolding. The calls for drug refills, by patients and their carers, fell on deaf ears. When Nakasita contacted the district officials for help, she was told the government only supported pregnant mothers, leaving cancer patients to languish in pain without support. Mukazi was one of these patients (Read “The Right way to say goodbye: Quinton’s Story” (2018) and “Why are we failing to protect the rights of children like Kivumbi?” (2019).
Nakasita knew there were hundreds more like Mukazi and could not ignore their suffering. She initiated the process by using her personal cellphone and her vehicle, and also contactedbodaboda(motorbike) drivers to deliver drugs to patients and bring critically ill patients to hospital – essential during a severe lockdown.
Collaboration and cooperation meant care continued
Because she knew her funds were insufficient to reach the many patients in need of pain relief and transport, Nakasita wrote to the Palliative Care Association Uganda for further support. She knew there were many children and adults living with cancer who, after chemotherapy, needed follow-up visits to hospital but they lacked the financial means to make the trip.
Nakasita was aware of this silent suffering hidden away in homes, across many districts, so she raised the alarm. The association recognised her call for help and provided her with the necessary financial assistance to deliver drugs and pay drivers to transport patients to and from hospital. Support from the association and others, such as District Health Authority, meant that the holistic approach to palliative care and access to this service could continue uninterrupted during the pandemic.
It was Nakasita who initially set up the palliative care unit at Kitagata Hospital and who personally travelled five hours to reach Mukazi in a remote area in Ntungamo District, bringing her oral morphine and antibiotics. Without a trained palliative care nurse such as Nakasita, the many patients in Mukazi’s position would have been forgotten.
Nurse prescribes morphine
As a qualified palliative care nurse, Nakasita was allowed to administer morphine in place of a medical practitioner.
In order for Nakasita to legally access morphine for her patients, she must keep accurate records which justify the further ordering of morphine. In addition Nakasita must send quarterly reports to the National Medical Store (NMS) thus ensuring the collection of data reflecting the needs for pain relief and the response. The NMS gathers and analyses data to establish the true extent of the problem. Through this analysis there is a potential to develop plans tailored to meet local needs of communities.
At a more personal level, Nakasita also cleaned Mukazi ’s wound and offered emotional support to the family, this same support or similar support was provided for 600 more patients and families in the Greater Bushenyi District. Through both the work and the compassion displayed by Nakasita the dignity and rights of patients such as Mukazi are ultimately realised and upheld.
Palliative care improves quality of life
Palliative care is important because it affords patients pain relief and symptom management, thus improving a patient’s quality of life while still pursuing curative measures. Palliative care not only controls a patient’s distressing symptoms, but also addresses and supports a patient’s emotional, psychological and spiritual needs whilst also offering care for their families.
As a nurse Nakasita found the palliative care training worthwhile because she learned to manage the patients’ pain and other distressing symptoms of a life limiting illness. Previously she thought morphine weakened patients, which is a common misconception shared among many of her fellow health workers. As a result of her training she realised this misconception meant patients were not offered the pain relief they so desperately needed.
These early laws continue to drive suspicion and fear, including many in the medical profession, about the utilisation of opium as a form of pain relief, which denies the right of many to adequate health care and to a dignified end to life. Uganda’s nurse prescribing has shown that with safeguards in place, including secure morphine storage, and adequate record-keeping by nurses, there have been no recorded cases of drug misuse.
Viruses and pathogens will come and go but as human encroachment on the environment, and on wildlife, increases, so too will the frequency of these new diseases. As scientists accept the reality of future pandemics and develop tools to predict these threats, global health experts will have limited time to find innovative remedies to these pandemics of the future.
This is the time, as leading scientists and innovators scurry to respond to the call for relief, where people with palliative care skills like Nakasita, are a necessity. Health practitioners and carers, with palliative care training, are already in place to provide the necessary and humane care for those many who are suffering.
Unfortunately, while in the storm of a pandemic, humane and gentle medicine often goes unrecognised and the rights of many patients are undermined. In the haste to stop the spread or cope with increasing numbers of patients, inclusive healthcare is non-existent with many older or seriously ill patients being left to die alone (Read: “Dying Alone Due to Covid-19: Do the Needs of the Many Outweigh the Rights of the Few – or the One?”).
If palliative care is not included in pandemic preparedness, when the next pandemic rolls around, many more will die in unnecessary suffering, watched over by their helpless traumatised families, who will be scarred forever. Pandemics by their nature cause death but we can at the very least relieve suffering prior to death. Health systems that continue to chase cures for each future pandemic, and continue to ignore palliative care that relieves suffering, do their citizens a huge disservice.
Dr Desia Colgan is a senior law lecturer at the University of Witwatersrand. She oversaw the Wits Street Law programme for over 20 years, working extensively on social justice issues and the rights of children. For the past 14 years she has been involved with palliative care for adults and children. Nicola GunnClark previously worked at the National Hospice Association in South Africa (HPCA) on legal projects including publication of Legal Aspects of Palliative Care (2012) which led to the rollout of law training to hospices, and linked indigent hospice patients & families to pro bono legal help, and later was appointed advocacy officer to HPCA. For six months she worked at the national children’s palliative care network, Patch SA assisting to set up a high-level meeting with government highlighting the need to implement the national policy on palliative care particularly so children’s right to palliative care can be realised, and for palliative care to be integrated into the health system. Her day job is in conveyancing in the United Kingdom. Emmanuel Kamonyo Sibomana is a member of Quebec Bar (Membre du Barreau du Québec) who previously worked as Health Rights Officer for Open Society East Africa. Sibomana is a strong proponent for justice and has been involved, for many years, in supporting strategies that advance the health and human rights of all marginalised people.
The authors would like to acknowledge Catherine Nakasita for her input and feedback during the writing of this article. Without her help this article would not have been possible. For questions on this story please contact the co-authors: Dr Desia Colgan desia.colgan@wits.ac.za; Nicola GunnClark gunnclarknicky@gmail.com; Emmanuel Kamonyo Sibomana healthrightseafrica@gmail.com.
Online teaching and learning: Towards a realistic view of the future
- Greig Krull and Danie De Klerk
The shift to emergency remote teaching and learning enabled academics to start questioning some long-held assumptions about in-person teaching and learning.
South African universities are currently considering the future of teaching and learning after the rapid shift to emergency remote teaching and learning in 2020 and 2021. During this time, two narratives have (re)emerged. One implies that teaching and learning online is more difficult or demanding than in-person education. The other that it’s not as good as in-person teaching and learning.
In the South African higher education context these concerns seem to be closely tied to staff burnout and to the inequities and complexities of the sector, which were amplified by emergency remote teaching and learning.
There were many equity and inequality issues in South Africa higher education prior to the pandemic. Strategies have been designed to create a more equitable higher education system. Still, as the COVID-19 pandemic has so starkly reminded us, challenges remain. Now is the time to continue focusing on addressing inequities rather than citing them as a reason not to change.
Our argument is based on our work in the field of online teaching and learning and informed by our experiences of moving to emergency remote learning at a South African university during the pandemic. We developed a support strategy for staff and students and this gave us insight into their challenges and needs.
Online teaching and learning before COVID-19
Open distance learning and online learning in higher education are nothing new. Pedagogically sound curricula had been delivered in fully online modes long before 2020. But integrating technology into teaching and learning has long been a point of contention in contact universities globally. Part of the reason is the way online tools were sold to higher education institutions, with little consideration to managing the associated changes.
Academics were often “thrown in at the deep end” with little pedagogical training or guidance on the use of the technology. Online and blended learning became the province of the early adopters and those brave enough to persevere. And expectations created by software companies weren’t always met.
Emergency remote teaching and learning
COVID-19 forced the rapid upskilling of academics and students to teach and learn remotely in ways unfamiliar to most. Emergency remote teaching and learning is by no means the same as authentic online or blended teaching and learning. The latter is usually carefully planned and designed over a long period, before the launch of carefully crafted learning experiences. And students have the choice to sign up for that mode of delivery. In contrast, in an emergency mode, some curricula were reduced to a bare minimum.
Nonetheless, the emergency shift enabled academics to begin to question some long-held assumptions about in-person teaching and learning. It raised questions about the role of the classroom, the lecturer and the way students learn. This can lead to improved practices in the sector.
The change undoubtedly placed immense strain on academics and students alike. And this came on top of many systemic factors that have been increasing the pressures experienced by academics over the last two decades. However, it is not online learning that led to this strain, but the transition to a different way of teaching and learning during a pandemic.
Student realities
A Department of Higher Education and Training survey of nearly 49,000 students from 24 higher education institutions in South Africa found that 96% of those who responded had learning devices in 2020, of whom 89% had smartphones. But half of all respondents found a smartphone difficult to use for learning.
More shocking are the findings of another survey of just over 13,000 students which revealed that just over 40% of respondents could not buy their own food during the pandemic, about 30% didn’t have a suitable study space, 6% reported not having electricity, and more than 40% felt socially isolated.
Yet these realities were not new. Emergency and remote teaching and learning has brought them to the fore.
While some may cite pedagogical reasons for returning to the classroom, it’s likely to shift focus away from these uncomfortable truths once more. Reverting to pre-pandemic ways could simply dim the spotlight and allow for a continuation of what had been. Rather, we argue for developing more inclusive and better teaching and learning practices as the sector moves beyond emergency mode.
Towards a realistic view of the future
Now is the time to use the lessons learned from this disruption, while being realistic about the sector’s context. First, there’s a need to untangle conflated perceptions of emergency and authentic teaching and learning. Academics must reflect and learn from what has been developed over the last 18 months. They must guard against silencing a conversation about entrenched inequalities.
Second, academics must remember that social learning doesn’t only occur on campus. It can happen in online spaces. The sector should aim to enhance student learning experiences.
Third, the fact that emergency and remote teaching and learning has introduced new (or at least previously undervalued) ways of engaging with students must be acknowledged. This enhances academics’ ability to respond to the expressed needs of students. Now is the time to have uncomfortable conversations, grapple with the realities laid bare by unusual times, and imagine new possibilities.
Fiona MacAlister, the project manager for online learning at the Faculty of Commerce, Law and Management in the University of the Witwatersrand, also contributed to this article.
Covid-19: Should South Africa be vaccinating 12-17 year olds
- Shabir A. Madhi
The focus of the government seems to be about how many people can get vaccinated rather than ensuring the greatest protection against severe disease and deaths.
South Africa is one of the leading countries in Africa in terms of COVID vaccine rollout, along with Mauritius, Tunisia and Morocco. It has, however, had it’s fair share of challenges. Shabir Madhi has been a key player in shaping the country’s response. Ina Skosana and Ozayr Patel asked him for an assessment of plans to vaccinate adolescents, and next steps.
Should South Africa be vaccinating adolescents?
I don’t believe this is the most efficient use of the vaccines. In a country like South Africa, we’d be much better off offering a third dose of the Pfizer/BioNTech vaccine to the 65% of adults above the age of 65 who have been vaccinated, and intensifying efforts at vaccinating the elderly and high risk groups who have not yet received even a single dose.
We shouldn’t be using these vaccines to give to children between 12 to 17 years a single dose.
Young children rarely get severe disease from COVID-19. Vaccinating children with a single dose of the Pfizer vaccine is unlikely to provide much value to the child in terms of individual protection, unless they have underlying medical conditions pre-disposing them to severe COVID-19. If this is the case they should receive the full two dose schedule. A single dose also doesn’t work too well in reducing the ability of a person to transmit the virus.
This is the main reason being given for vaccinating 12 to 17 year olds.
South Africa might be banking on the fact that a large percentage of the population – estimates are between 70% to 80% – might have been infected already. In that context, a single dose of vaccine is probably all you require to protect against severe COVID-19.
This hybrid immunity, where you start off with your immune system being primed by natural infection followed by a vaccine, induces quite potent immunity. Consequently, people that have passed infection probably only require a single dose of any vaccine. That’s the only way South Africa can really justify using a single dose of vaccine in the 12 to 17 year old age group. Needless to say, waiting to get infected and risking developing long-COVID, being hospitalised for COVID-19 or dying from COVID-19 is not really a bright idea.
The liberal rollout of COVID-19 vaccines in South Africa to low risk groups, such as young children, appears to be more about chasing after numbers rather than deriving the maximal protection against severe disease and deaths.
I’m not saying that you shouldn’t vaccinate children. There’s a time and place. But that time and place is not right now in South Africa, or globally in the context of the tragic inequity of vaccine access.
Starting to vaccinate children against COVID-19 (and use of booster doses in healthy adults) is more than just a country specific decision. Most countries on the continent have less than 5% of the adult population vaccinated, and in fact, less than 10% of people above the age of 60 are vaccinated.
This is being perpetuated by countries with access to vaccines using them liberally.
Would you recommend a booster for the general population?
Absolutely. For certain groups of adults.
We now understand that the first two doses of vaccine provide good protection against severe disease in people above the age of 65 and those with other underlying medical conditions. However, it is also apparent that people older than 65 or with underlying immunosupressive medical conditions require a third dose of the mRNA vaccines, such as by Pfizer/Biontech. This is required to boost their immune response and enhance their protection even against severe COVID-19.
The primary goal of vaccination therefore needs to be on reducing severe disease and death. This requires targeted strategies on who to prioritise.
Evidence from the US is that a two dose schedule of the Johnson & Johnson vaccine is superior in protecting against hospitalisation than a single dose. And if you want durability of protection, you need to boost, which can be done with another dose of Johnson & Johnson.
My own preference is to boost with one of the messenger RNA vaccines. In South Africa this is the Pfizer vaccine. The evidence is clear that the type of immune responses from this approach is superior to two doses of the J&J vaccine and possibly even two doses of the Pfizer vaccine.
Is vaccine coverage high enough to justify boosters?
Absolutely. If we can justify providing vaccines to the 12 to 17 year old age group, it means we’ve got vaccines that we don’t know what to do with.
In my view it would be much better offering these doses to boost adults above the age of 55. In particular, people older than 65 do require an additional dose of the Pfizer vaccine after they’ve had two shots. The same thing goes for other risk groups such as people with kidney transplants, or people with cancer and on chemotherapy, people with any other sort of underlying immunosuppressive condition.
South Africa is, once again, going against the World Health Organisation which is recommendating booster doses of such high risk groups, and instead vaccinating young children.
Is South Africa in a stable position vis-a-vis another surge?
The main thing that’s going to determine how well the country manages another resurgence is the percentage of people above the age of 50 who have been vaccinated. We need to get 85% to 90% of this age group vaccinated and 80% of those with underlying medical conditions.
If we don’t reach those marks, when we do have a resurgence – and we will have a resurgence in the next two to three months – it will end up with hospitals coming under pressure once again.
What’s in South Africa’s favour is the high percentage of the population that’s been infected with the virus. Natural infection does seem to confer protection against severe disease.
So this combination of natural immunity – probably 75% to 80% of the population has now have developed some level of natural immunity – coupled with vaccine induced immunity and a hybrid of the two probably puts South Africa in a relatively stable position in relation to severe cases likely to be lower with a future resurgence than experienced in the past. This could, however, change if there are new major immune-evasive mutations in the virus.
What’s been learnt from the vaccine roll-out in South Africa?
We’ve learned that rolling out a vaccine is as complex as securing supplies. And we’ve missed some targets.
For example, we were meant to have vaccinated the majority of people above the age of 60 by July this year. Currently we’re sitting at around about 62% to 63% of people above the age of 60. In the 50 to 59 year age group we are looking at just over 50%.
The reasons are multiple. But part of it speaks to the issue of planning and rollout, not just in South Africa, but in many countries. People don’t appreciate what it entails, starting from community engagement, adequate communication around what the vaccines are about, what the purpose of the vaccine programme is, and then finally being able to implement.
The other challenge was that the initial planning for the rollout was top down. The expectation was that people were going to rush forward to register on the electronic vaccine data system without really understanding how adaptable it was for South Africa. The system was inaccessible to most people.
There was a quick escalation in coverage once walk ins were set up for targeted age groups. Also, the use of pop up facilities is beginning to play a big part in increasing vaccine coverage rates.
This also speaks to the issue of community sensitisation and engagement of community structures. Unfortunately resources set aside for this purpose were siphoned off by corruption.
Also, South Africa hasn’t had enough champions across the spectrum of society. In other countries support this has been a major contributor to success.
On the plus side, South Africa secured adequate supplies of vaccine. That in itself was quite an achievement, considering the poor planning until Government came under pressure early in January 2021. The challenge now is being able to use the doses wisely before they expire.
Shabir A. Madhi, Dean Faculty of Health Sciences and Professor of Vaccinology at University of the Witwatersrand; and Director of the SAMRC Vaccines and Infectious Diseases Analytics Research Unit, University of the Witwatersrand. This article is republished from The Conversation under a Creative Commons license. Read the original article.
The proposed Framework has been developed and will be shared with staff, students, senior managers, organised labour, and other constituencies for comment.
Please send your comments to vco.news@wits.ac.za by Monday, 11 October 2021.
SUMMARY OF THE WITS MANDATORY VACCINATION FRAMEWORK
Wits is a contact teaching university and the mandatory vaccination of staff and students will enable optimal access, the holistic delivery of the teaching and learning programme, and research to continue. A mandatory vaccination policy protects the health and safety of the University community, members of the public, and advances the public good.
POLICY STATEMENT
All staff and students, including applicants for study or employment, as well as visitors and service providers will be required to be vaccinated against COVID-19 before accessing campus.
GENERAL PRINCIPLES
- Staff and students will be required to produce their digital vaccine passport or vaccination cards, which will be linked to their access cards to enable them to enter Wits’ premises.
- Staff will be given paid time-off to get vaccinated, and sick leave should they experience any side-effects associated with the vaccine.
Exemptions:
- Students under the age of 18 are exempted (until laws change).
- Staff or students may be exempted on medical grounds (on confirmation from a medical professional that it poses a significant medical risk), Wits may send staff/students for further medial assessment if required. A Committee will be set up to decide on any exemptions based on reasonable accommodation, in line with labour directives.
Students who elect not to be vaccinatedon constitutional grounds will be required to:
- undertake daily health screening prior to being allowed entry to Campus;
- buy and always wear an N95 mask, including in lectures, laboratories, during tutorials, and/or during assessments, and on buses; and
- undertake weekly testing (at their own cost) for SARS-CoV-2 infection irrespective of whether they have COVID-19 symptoms or not.
These students will also not be allowed:
- into common areas where social engagements take place;
- to stay in Wits’ residences; and
- to attend in-person graduation ceremonies.
Staff members who elect not to be vaccinatedon constitutional grounds will be required to:
- undertake daily health screening prior to being allowed entry to Campus;
- buy and always wear an N95 mask; and
- undertake weekly testing for SARS-CoV-2 infection (at their own cost) irrespective of whether they have COVID-19 symptoms or not.
These staff will also not be allowed into common areas where social engagements take place and may not refuse to return to work on account of not being vaccinated. They can apply for reasonable accommodation from the Wits Mandatory Vaccination Committee. In instances where reasonable accommodation cannot be provided, the University may exercise its rights to terminate the employee’s services based on incapacity in line with the relevant processes and procedures.
Service Providers and Visitors
These rules apply to service providers, the employees of service providers, and visitors who will not be permitted access to Campus or any University facilities unless they are vaccinated.
Wits Mandatory Vaccination Committee
This committee of experts will consider:
- applications for exemption on medical grounds and cases where students are under 18;
- requests for reasonable accommodation by staff members who have been exempted on medical grounds or who have elected not to be vaccinated on constitutional grounds; and
- monitor compliance with the University’s vaccination policy.
Q&A ON VACCINES
We asked Wits scientists, some of the best in the world in their fields, the following questions about vaccines:
Q: Are vaccines safe?
A: COVID-19 vaccines have been proven to be safe and highly effective in reducing the risk of becoming infected with SARS-CoV-2 (the coronavirus that causes COVID-19), in preventing serious illness and death from COVID-19, and in limiting the spread of the virus.
Q: What if it is my personal choice not to get vaccinated?
A: If you do not get the vaccine, you put your health, and the health of others at risk. Scientific evidence has shown that vaccines are the most critical and effective intervention for COVID-19 prevention. When a large proportion of people are vaccinated, there is greater community protection against transmission of the virus, which allows the University community to safely return to on-site teaching, learning, research, operations, and other in-person activities.
At Wits, where most of the teaching and learning takes place in large groups and where students and some staff live in communal housing, a risk of infection and outbreaks exist and can be significantly reduced by ensuring that all members of the University community are vaccinated. In this vein, and in balancing the collective right of the broader University and surrounding community to health and safety, against individual rights to bodily integrity; freedom of religion; belief and opinion, the prevailing view is that the collective right takes precedence. This is in the broader public interest and is reasonable, justifiable, and rational.
Q: How were COVID-19 vaccines developed so quickly? How do I know if they are injecting me with the virus instead?
A: There is no reason to distrust vaccines just because you do not know what is in it. The COVID-19 vaccines were also developed and approved quickly because scientists already knew and understood much about the coronavirus. Speak to your healthcare professional, someone at Campus Health and Wellness, or a Wits expert.
Q: Is Wits’ mandatory vaccination policy a breach of South African labour laws?
A: All Wits’ policies will comply with South African legislation and labour laws. South African labour law puts primacy on the collective rights of people when upholding the rights of any one individual is going to put the collective at risk.
"We will also continue to engage with the broader Wits community on the proposed policy in the coming weeks."
The Senate, the highest academic decision-making body of the University of the Witwatersrand, considered the proposed mandatory vaccination policy at its final regular meeting of the year on 4 November 2021 and expressed its overwhelming support to recommend the proposed policy to Council.
We welcome this affirming support from Senate and thank all Senators for their insightful comments, robust opinions, and meaningful contributions to the policy. We will incorporate the suggestions made by Senators as may be appropriate, before the policy is presented to Council for approval.
We will also continue to engage with the broader Wits community on the proposed policy in the coming weeks. Staff members and students will have another opportunity to engage on the proposed policy through webinars which will take place in the next 10 days. Several Wits experts will be online to address any concerns that you may have. Details will be shared via Wits News on Monday.
We would also like to express our deep appreciation to all members of the Wits community who have already commented on the proposed mandatory vaccination policy framework. Hundreds of email comments were received and considered, and recommendations and suggestions were incorporated where appropriate.
For now, we strongly encourage all members of the Wits community to get vaccinated as soon as possible.
[WATCH] an animation that answers many vaccination questions based on information from the Scientists Collective.
- Sara Cooper, Alison Swartz, Bey-Marrié Schmidt, Charles Shey Wiysonge, Christopher J Colvin, Evanson Z Sambala, Natalie Leon
Unpacking parents’ reasons for not vaccinating their children: why it matters
For many of us, the case for childhood vaccination seems self-evident. Every year, this powerful public health intervention protects billions of children from deadly and debilitating infections like polio and measles. Yet worldwide, many parents are reluctant – if not outright refusing – to vaccinate their children. This includes parents who have access to vaccines, are well-educated, and have enjoyed the benefits of having their children grow up in a world free of many vaccine-preventable diseases.
This phenomenon is now referred to as vaccine hesitancy. It’s not new. Public concerns about vaccination, and controversies surrounding it, are as old as vaccines themselves. Yet with the recent global outbreaks of diseases such as measles and diphtheria, and more recently COVID-19, vaccine hesitancy has been placed firmly on the global public health agenda.
In a recently conducted Cochrane review we analysed qualitative studies of parents’ views, experiences, and practices around routine childhood vaccination.
We included 27 studies in our analysis. Studies were conducted in Africa, the Americas, South-East Asia, Europe, and the Western Pacific, and included urban and rural settings, as well as high-, middle-, and low-income settings.
We found that vaccination uptake, as with so many health interventions, is influenced by many factors and carries a variety of meanings – social, political, economic, ideological, moral as well as biological. Through their vaccination choices, parents are often communicating not just what they think about vaccines, but also who they are, what they value and with whom they identify.
We found that parents’ vaccination views and practices are shaped by factors like:
their broader worldviews surrounding health and illness
the vaccination ideas and practices of their social networks
wider political issues and relations of power and particularly the impact these have on parents’ trust (or distrust) in those associated with vaccination programmes
access to and experiences of vaccination services and their frontline healthcare workers.
Our findings suggest that childhood vaccination, whatever stance is taken, is a complex social process. It is deeply embedded in the wider social worlds in which people live. Understanding these social worlds, and placing them at the centre of public health interventions, is critical.
Reasons for vaccine hesitancy
Vaccine hesitancy is not a single problem. The way it manifests and why it occurs varies considerably across place, time, and even vaccines. Local contexts and framing matter. Yet we found certain overarching patterns across the studies that help to explain why parents may be hesitant about routine vaccines for their children.
The first reason relates to the view that healthcare is a matter of personal risk, choice, and responsibility. Many parents, across the spectrum of vaccination attitudes, hold this worldview. Yet some parents see this worldview as being in conflict with vaccination promotion messages. These messages emphasise population-level risk and community health. This perceived tension may lead some parents to be hesitant about vaccination for their children.
The second reason relates to the impact of social exclusion. Exclusion can take many different forms: economic, political, and cultural. All these forms can lay the foundation for distrust, alienation, resentment, and demotivation. Parents who are socially excluded may be hesitant about vaccination because they distrust vaccines and those delivering them. Or it may be a form of resistance or a mechanism to bring about change. It may be that vaccination takes time and comes with opportunity costs for these parents.
An alternative approach
Parents who resist vaccines for their children are commonly portrayed as ‘ignorant’, ‘misinformed’ or ‘irrational’ – or selfish or evil. It is often assumed that the attitudes of these parents can be corrected with biomedical education and advanced risk communication strategies. The findings from our review suggest that a more nuanced and less clinically oriented approach may be needed.
Such an approach involves taking seriously, on their own terms, the complex factors and meanings shaping parents’ vaccination choices. It means recognising that parents’ values and priorities, and their responses to these, do not always align with the goals of vaccination programmes.
“Hesitancy” does not only have negative connotations, as seminal work published over two decades ago demonstrated. In fact, for many parents, “hesitancy” may also be about a striving for or desiring something: to protect their child’s health, to be part of healthcare decision-making, to belong and feel included among peers, to feel confident that expert systems have their best interests at heart, to have their own priorities recognised and basic needs met.
Approaching hesitancy with this understanding is unlikely to translate into one-dimensional and “quick-fix” interventions. Yet we believe it could provide avenues for the development of more sensitive and effective strategies for engaging with parents who decide against vaccination for their children.
Covid-19 Update 76: Council approves Wits Covid-19 Mandatory Vaccination Policy
- Senior Executive Team
Read the full statement, the policy, and the Q&A information document wherein Wits experts answer questions about vaccination, legal, ethical, and more.
The Council of the University of the Witwatersrand discussed and approved the Wits COVID-19 Vaccination Policy at its meeting on 25 November 2021, following engagements with the Wits community over several weeks. These engagements will continue as the course of the pandemic becomes clearer. The Policy will be implemented from 1 January 2022 and will be reviewed regularly. Staff and students will have from 1 January 2022 to 1 March 2022 to either vaccinate or apply for reasonable accommodation. An implementation plan is being developed and this information will be shared with the Wits community as soon as it is available.
Summary of the Wits Covid-19 Vaccination Policy
Policy Statement
All members of the University community will be required to vaccinate against COVID-19 in order to access the University’s precincts, aside from those who have been granted reasonable accommodation.
Purpose
The purpose of the Policy is to enable the return of employees and students to the University’s precincts whilst protecting the health and safety of the University community, and all others who work, live, learn, and/or participate in activities on campus.
Context
The vaccination of employees and students will enable optimal access and the functioning of the University, including the delivery of teaching and learning, and the conducting of research. This is particularly pertinent for students who, due to their socioeconomic circumstances, benefit more readily from learning on campus, and those whose learning programmes require in-person engagement for pedagogic and professional reasons, in line with the 2022 Blended Teaching and Learning Plan.
Wits also plans to re-invigorate the student experience in 2022 by enabling more on-campus social engagement.
The Wits COVID-19 Vaccination Policy will help to protect the health and safety of the University community and the broader public. The University will make provision for the vaccination of employees and students on campus and at dedicated sites in 2022.
COVID-19 vaccinesare proven to besafe and highly effective in reducing the risk of becoming infected with SARS-CoV-2 (the coronavirus that causes COVID-19), in preventing serious illness and death from COVID-19, and in reducing the spread of the virus.
In balancing the collective rights of the broader Universityand surrounding community to health and safety, against individual rights to bodily integrity, freedom of religion, belief and opinion which may be limited in terms of Section 36 of the Constitution, our view, supported by experts, is that the collective right takes precedence. This is in the broader public interest and is reasonable, justifiable and rational.
Principles
All members of the University community must be vaccinated regardless of whether they have been diagnosed with COVID-19 in the past. Everyone will be required to comply with the relevant national and Wits COVID-19 safety protocols, including the wearing of masks. A vaccination site will also be established on campus.
Those who are not vaccinated and have been granted reasonable accommodation will be required to comply with additional protocols like daily health screening and weekly antigen testing for SARS-CoV-2 infection, irrespective of whether they are symptomatic or not (Wits will cover costs of those unable to pay for the first few months).
Staff and students who are not vaccinated and who have been granted reasonable accommodation, may also be limited from participating in certain University activities. For example, they may not be allow to participate in activities in common spaces where social engagements occur; to attend certain academic activities and/or graduations; and will not be allowed to secure accommodation in any University-owned residences.
Implementation of the Wits Covid-19 Vaccination Policy
A Wits COVID-19 Vaccination Policy Implementation Committee is being established. The Committee will develop an implementation plan that will include details of how the Policy will be effected, how access to campuses will work, how to apply for reasonable accommodation, etc. This information will be shared with the Wits community as soon it becomes available. There will also be ongoing engagement with staff and students to clarify aspects of the Policy and its implementation.
Access to Campus
The University can refuse access to campus to any person who has not been vaccinated and/or who has not been reasonably accommodated. Vaccinated members of the University will provide proof of their vaccination status, which will be linked to their staff or student profile to enable seamless access to the University’s precincts. Visitors will have to produce their EVDS certificate confirming their vaccination status before being permitted access to campuses.
Reasonable Accommodation
Employees and students who cannot be vaccinated on medical grounds, or choose not to be vaccinated on Constitutional grounds, must apply for, and be granted reasonable accommodation between 1 January 2022 and 1 March 2022. If reasonable accommodation is denied, staff and students can appeal to the Mandatory Vaccination Appeals Committee.
Should these appeals be denied, the University reserves the right not to register students, to defer studies, and in respect of staff to address the matter in line with the University’s policies and procedures, and relevant labour laws. Employees will not be entitled to refuse to return to work on the basis of not having been vaccinated.
Two webinars and several dedicated meetings were held in recent weeks to engage on the Wits COVID-19 Vaccination Policy. A panel of experts, including a vaccinologist, scientists, clinicians, lawyers and ethics specialists responded to questions from members of the Wits community on vaccines, the proposed policy, and other areas. The questions and answers have been clustered and can be viewed on the Wits COVID-19 portal or via this Q&A link. Experts did not respond to questions from anonymous sources.
Watch this video that may help to answer some vaccination concerns.
Thank you
SENIOR EXECUTIVE TEAM
26 NOVEMBER 2021
The hunt for coronavirus variants
- Wolfgang Preise, Cathrine Scheepers, Jinal Bhiman, Marietjie Venter and Tulio de Oliveira
Covid 19: How the new one was found and what we know so far.
Since early in the COVID pandemic, the Network for Genomics Surveillance in South Africa has been monitoring changes in SARS-CoV-2. This was a valuable tool to understand better how the virus spread. In late 2020, the network detected a new virus lineage, 501Y.V2, which later became known as the beta variant. Now a new SARS-CoV-2 variant has been identified – B.1.1.529. The World Health Organisation has declared it a variant of concern, and assigned it the name Omicron. To help us understand more, The Conversation Africa’s Ozayr Patel asked scientists to share what they know.
What’s the science behind the search?
Hunting for variants requires a concerted effort. South Africa and the UK were the first big countries to implement nationwide genomic surveillanceefforts for SARS-CoV-2 as early as April 2020.
Variant hunting, as exciting as that sounds, is performed through whole genome sequencing of samples that have tested positive for the virus. This process involves checking every sequence obtained for differences compared to what we know is circulating in South Africa and the world. When we see multiple differences, this immediately raises a red flag and we investigate further to confirm what we’ve noticed.
In addition, South Africa has several laboratories that can grow and study the actual virus and discover how far antibodies, formed in response to vaccination or previous infection, are able to neutralise the new virus. This data will allow us to characterise the new virus.
The beta variant spread much more efficiently between people compared to the “wild type” or “ancestral” SARS-CoV-2 and caused South Africa’s second pandemic wave. It was therefore classified as a variant of concern. During 2021, yet another variant of concern called delta spread over much of the world, including South Africa, where it caused a third pandemic wave.
Very recently, routine sequencing by Network for Genomics Surveillance member laboratories detected a new virus lineage, called B.1.1.529, in South Africa. Seventy-seven samples collected in mid-November 2021 in Gauteng province had this virus. It has also been reported in small numbers from neighbouring Botswana and Hong Kong. The Hong Kong case is reportedly a traveller from South Africa.
The World Health Organisation has given B.1.1.529 the name Omicron and classified it as a variant of concern, like beta and delta.
Why is South Africa presenting variants of concern?
We do not know for sure. It certainly seems to be more than just the result of concerted efforts to monitor the circulating virus. One theory is that people with highly compromised immune systems, and who experience prolonged active infection because they cannot clear the virus, may be the source of new viral variants.
The assumption is that some degree of “immune pressure” (which means an immune response which is not strong enough to eliminate the virus yet exerts some degree of selective pressure which “forces” the virus to evolve) creates the conditions for new variants to emerge.
Despite an advanced antiretroviral treatment programme for people living with HIV, numerous individuals in South Africa have advanced HIV disease and are not on effective treatment. Several clinical cases have been investigated that support this hypothesis, but much remains to be learnt.
Why is this variant worrying?
The short answer is, we don’t know. The long answer is, B.1.1.529 carries certain mutations that are concerning. They have not been observed in this combination before, and the spike protein alone has over 30 mutations. This is important, because the spike protein is what makes up most of the vaccines.
We can also say that B.1.1.529 has a genetic profile very different from other circulating variants of interest and concern. It does not seem to be a “daughter of delta” or “grandson of beta” but rather represents a new lineage of SARS-CoV-2.
Some of its genetic changes are known from other variants and we know they can affect transmissibility or allow immune evasion, but many are new and have not been studied as yet. While we can make some predictions, we are still studying how far the mutations will influence its behaviour.
We want to know about transmissibility, disease severity, and ability of the virus to “escape” the immune response in vaccinated or recovered people. We are studying this in two ways.
Firstly, careful epidemiological studies seek to find out whether the new lineage shows changes in transmissibility, ability to infect vaccinated or previously infected individuals, and so on.
At the same time, laboratory studies examine the properties of the virus. Its viral growth characteristics are compared with those of other virus variants and it is determined how well the virus can be neutralised by antibodies found in the blood of vaccinated or recovered individuals.
In the end, the full significance of the genetic changes observed in B.1.1.529 will become apparent when the results from all these different types of studies are considered. It is a complex, demanding and expensive undertaking, which will carry on for months, but indispensable to understand the virus better and devise the best strategies to combat it.
Do early indications point to this variant causing different symptoms or more severe disease?
There is no evidence for any clinical differences yet. What is known is that cases of B.1.1.529 infection have increased rapidly in Gauteng, where the country’s fourth pandemic wave seems to be commencing. This suggests easy transmissibility, albeit on a background of much relaxed non-pharmaceutical interventions and low number of cases. So we cannot really tell yet whether B.1.1.529 is transmitted more efficiently than the previously prevailing variant of concern, delta.
COVID-19 is more likely to manifest as severe, often life-threatening disease in the elderly and chronically ill individuals. But the population groups often most exposed first to a new virus are younger, mobile and usually healthy people. If B.1.1.529 spreads further, it will take a while before its effects, in terms of disease severity, can be assessed.
Fortunately, it seems that all diagnostic tests that have been checked so far are able to identify the new virus.
Even better, it appears that some widely used commercial assays show a specific pattern: two of the three target genome sequences are positive but the third one is not. It’s like the new variant consistently ticks two out of three boxes in the existing test. This may serve as a marker for B.1.1.529, meaning we can quickly estimate the proportion of positive cases due to B.1.1.529 infection per day and per area. This is very useful for monitoring the virus’s spread almost in real time.
Are current vaccines likely to protect against the new variant?
Again, we do not know. The known cases include individuals who had been vaccinated. However we have learnt that the immune protection provided by vaccination wanes over time and does not protect as much against infection but rather against severe disease and death. One of the epidemiological analyses that have commenced is looking at how many vaccinated people become infected with B.1.1.529.
The possibility that B.1.1.529 may evade the immune response is disconcerting. The hopeful expectation is that the high seroprevalence rates, people who’ve been infected already, found by several studies would provide a degree of “natural immunity” for at least a period of time.
Ultimately, everything known about B.1.1.529 so far highlights that universal vaccination is still our best bet against severe COVID-19 and, together with non-pharmaceutical interventions, will go a long way towards helping the healthcare system cope during the coming wave.
This article was updated following the World Health Organisation’s announcement on the new variant.
The new variant – identified as B.1.1.529 has been declared a variant of concern by the World Health Organisation and assigned the name Omicron.
The mutations identified in Omicron provide theoretical concerns that the variant could be slightly more transmissible than the Delta variant and have reduced sensitivity to antibody activity induced by past infection or vaccines compared to how well the antibody neutralises ancestry virus.
As vaccines differ in the magnitude of neutralising antibody induced, the extent to which vaccines are compromised in preventing infections due to Omicron will likely differ, as was the case for the Beta variant.
However, as vaccines also induce a T-cell response against a diverse set of epitopes, which appears to be important for prevention of severe COVID, it is likely that they would still provide comparable protection against severe COVID due to Omicron compared with other variants.
The same was observed for the AstraZeneca vaccine. Despite not protecting against the mild-moderate Beta COVID in South Africa, it still showed high levels of protection (80% effective) against hospitalisation due to the Beta and Gamma variants in Canada.
In view of the new variant, there are a few steps that governments shouldn’t be taking. And some they should be taking.
What not to do
Firstly, don’t indiscriminately impose further restrictions, except on indoor gatherings. It was unsuccessful in reducing infections over the past 3 waves in South Africa, considering 60%-80% people were infected by the virus based on sero-surveys and modelling data. At best, the economically damaging restrictions only spread out the period of time over which the infections took place by about 2-3 weeks.
This is unsurprising in the South African context, where ability to adhere to the high levels of restrictions are impractical for the majority of the population and adherence is generally poor.
Secondly, don’t have domestic (or international) travel bans. The virus will disseminate irrespective of this – as has been the case in the past. It’s naive to believe that imposing travel bans on a handful of countries will stop the import of a variant. This virus will disperse across the globe unless you are an island nation that shuts off the rest of the world.
The absence of reporting of the variants from countries that have limited sequencing capacity does not infer absence of the variant. Furthermore, unless travel bans are imposed on all other nations that still allow travel with the “red-listed” countries, the variant will directly or indirectly still end up in countries imposing selective travel bans, albeit perhaps delaying it slightly.
In addition, by the time the ban has been imposed, the variant will likely have already been spread. This is already evident from cases of Omicron being reported from Belgium in a person with no links to contact with someone from Southern Africa, as well as cases in Israel, UK and Germany.
All travel bans accomplish in countries with selective red-listed countries is delay the inevitable. More could possibly be accomplished by rigorous exit and entry screening programmes to identify potential cases and mandating vaccination.
Third, don’t announce regulations that are not implementable or enforceable in the local context. And don’t pretend that people adhere to them. This includes banning alcohol sales, whilst being unable to effectively police the black market.
Fourth, don’t delay and create hurdles to boosting high risk individuals. The government should be targeting adults older than 65 with an additional dose of the Pfizer vaccine after they’ve had two shots. The same thing goes for other risk groups such as people with kidney transplants, or people with cancer and on chemotherapy, people with any other sort of underlying immuno-suppressive condition.
South Africa shouldn’t be ignoring World Health Organisation’s guidance which recommends booster doses of high risk groups. It should de-prioritise, for the time being, vaccinating young children with a single dose.
Fifth, stop selling the herd immunity concept. It’s not going to materialise and paradoxically undermines vaccine confidence. The first generation vaccines are highly effective in protecting against severe COVID-19, but less predictable in protecting against infection and mild COVID due to waning of antibody and ongoing mutations of the virus. Vaccination still reduces transmission modestly, which remains of great value, but is unlikely to lead to “herd-immunity” in our lifetimes.
Instead we should be talking about how to adapt and learn to live with the virus.
There is also a list of things that should be considered in the wake of the Omicron variant, irrespective of whether it displaces the Delta variant (which remains unknown).
What to do
Firstly, ensure health care facilities are prepared, not only on paper – but actually resourced with staff, personal protective equipment and oxygen, etc.
There are 2000 interns and community service doctors in South Africa waiting for their 2022 placement confirmation. We cannot once again be found wanting with under-prepared health facilities.
Provide booster doses of J&J or Pfizer to all adults who received a single dose J&J. It’s needed to increase protection against severe COVID. A single dose of the J&J vaccine reduced hospitalisation due to Delta variant in South Africa by 62% in South African healthcare workers, whereas two doses of AZ and mRNA vaccines in general had greater than 80%-90% protection against severe disease from the Delta variant.
Studies confirm a two dose schedule of the Johnson & Johnson vaccine is superior in protecting against hospitalisation than a single dose. And if you want durability of protection, you need to boost, which can be done with another dose of Johnson & Johnson or a dose of mRNA vaccine.
The evidence is clear that the type of immune responses from a heterologous approach of AZ or JJ followed by a mRNA vaccines such as Pfizer/Biontech induces superior neutralising and cell mediated immune responses than two doses of the non-replicating vector vaccines.
Thirdly, implement vaccine passports for entry into any indoor space where others gather, including places of worship and public transport. Vaccination might be a choice currently, however, choices come with consequences. Even if vaccines only reduce transmission modestly, over and above the infections they prevent, a breakthrough case in a vaccinated individual poses less risk of transmission to others than infection in an unvaccinated and previously uninfected individual.
Fourth, continue efforts at reaching out to the unvaccinated and under-immunized. This should include the use of pop up facilities where people are likely to gather and other targeted community outreach programs.
Fifth, immediately boost high risk groups older than 65 and others who have immunosuppressive conditions. The primary goal of vaccination therefore needs to be on reducing severe disease and death. This requires targeted strategies on who to prioritise.
Sixth, encourage responsible behaviour to avoid re-imposing alcohol and other restrictions to punish all due to irresponsibility on part of a minority.
Seventh, monitor bed availability at regional level to help decide on regional action to avoid overwhelming of facilities. Higher levels of restrictions need to be tailored for when we expect overwhelming of health facilities. As hospitalisation usually lag behind community infection rates by 2-3 weeks, keeping an eye on case rates and hospitalization rates could predict which facilities in which regions may come under threat.
This would allow for a more focused approach to imposing restrictions to relieve anticipated pressure on health facilities 2-3 weeks before expected. This will not change the total number of hospitalisations. But it will spread it out over a longer period of time and make it more manageable.
Eighth, learn to live with the virus, and take a holistic view on the direct and indirect effects of the pandemic on livelihoods. The detrimental indirect economic, societal, educational, mental health and other health effects of a sledge-hammer approach to dealing with the ongoing pandemic threatens to outstrip the direct effect of COVID in South Africa.
Ninth, follow the science and don’t distort it for political expediency.
Tenth, learn from mistakes of the past, and be bold in the next steps.
Shabir A. Madhi, Dean Faculty of Health Sciences and Professor of Vaccinology at the University of the Witwatersrand; and Director of the SAMRC Vaccines and Infectious Diseases Analytics Research Unit, University of the Witwatersrand. This article is republished from The Conversation under a Creative Commons license. Read the original article.
Omicron data: more transmissible but less severe
- Harsha Somaroo
Early data show that Omicron is dominating new COVID-19 cases in Gauteng province.
Gauteng is the smallest of South Africa’s nine provinces but home to a quarter of the country’s population. It is also the country’s economic power house. These factors have contributed to it becoming the epicentre of the COVID-19 epidemic. Gauteng’s COVID-19 surveillance aims to provide an understanding of the province’s experience. This also serves as an early warning system for other parts of the country. Public health medicine specialist Harsha Somaroo is part of the team analysing data for the Gauteng Department of Health and told The Conversation Africa what it’s showing so far.
What’s your data showing about COVID-19 in Gauteng?
In the four epidemiological weeks (13 November to 4 December, 2021), there was an exponential rise in new COVID-19 cases. The province officially entered its fourth COVID-19 wave on 1 December.
During this period South African scientists announced they had identified a new variant of SARS-CoV-2, which the World Health Organisation went on label a variant of concern and named it Omicron. Current data show that the Omicron variant is dominating new COVID-19 cases in the province.
The rate of increase in new cases in Gauteng has been significantly higher compared to any other period in the epidemic in the province. The weekly rates of increase in new infections, when compared to the previous week, were 71%, 341%, 379% and 272%.
That’s reflected by the steep incline in the curve for COVID-19 cases (Figure one).
The COVID-19 test positivity rate (the number of tests done that have a positive result) for the past four weeks, were 1.4%, 5.0%, 19.0%, and 33.9%. This reveals a rapid rise, and now widespread community transmission, of SARS-CoV-2 in Gauteng.
What does your data tell us about Omicron?
The recent exponential rise in new COVID-19 cases, associated with the detection and domination of the Omicron variant in the province, suggests that this SARS-CoV-2 variant of concern is highly transmissible.
It is also possible to understand the severity of illness better by monitoring trends and outcomes among hospitalised patients. There are two sets of data that provide insights – hospitalisations and excess deaths. Excess deaths are deaths above the number expected in a region for that point in time, and give an indication of the COVID-19 related deaths in a region.
Compared with previous periods during which the numbers have spiked the latest numbers show that new daily COVID-19 hospitalisations and excess deaths have been lower than the rate of increase in new COVID-19 cases, suggesting that the variant may cause less severe illness.
The weekly rates of new hospitalisations have been significantly high for the past three weeks (120%; 166%; and 125%). But this was still lower compared to previous periods in which infection numbers rose. Also, the current increase came off a very low base as admission numbers had fallen after the last COVID-19 waves in Gauteng (Figure two).
Another caveat, is that some patients have been admitted for other conditions, and were diagnosed with COVID-19 due to routine testing protocols in hospital, and not because they showed symptoms. Due to the number of patients for which this information is available, this proportion could lie between 7.4% and 52.1% of new COVID-19 admissions.
Another difference the data are showing is that there’s a change in the age profile of admissions. Younger age categories of patients (0-9, 10-19, and 30-39) accounted for higher proportions of hospital admissions during the past month than previously.
A significant proportion of these admissions might be due to asymptomatic COVID-19 infections which were incidental diagnoses due to routine testing for COVID-19 on admission to hospital (between 7% and 46%).
The average length of stay in hospital, for all age categories of patients, was lower in the past month compared to overall. Additionally, fewer patients were admitted into Intensive Care Units (5.6% versus 9%), and a lower proportion of patients required supplemental oxygen therapy (19.4% versus 43.1%) or ventilation (1.4% versus 8.2%) in the past four weeks compared to cumulatively (Table one).
In-hospital mortality rates were also lower in the past four weeks compared to cumulatively (2.6% compared to 22%). However, there was still higher mortality among those over 50 years old.
The early findings suggest less severe COVID-19 infections, though they should be correlated with clinical pictures and monitored closely over the next few weeks to better understand the clinical manifestations and outcomes related to the Omicron variant.
What do people need to do in the light of this information?
These early surveillance findings give us some idea of the transmission dynamics and virulence of the Omicron variant in Gauteng. Trends will need to be monitored closely over the next few weeks to fully understand the impact of this new variant.
The recent high rates of COVID-19 transmission, and continued higher death rates among older patients hospitalised with COVID-19, have important implications for public health measures. The following are critical to decrease the number of new COVID-19 cases:
physical distancing
avoidance of gatherings and poorly ventilated spaces
wearing of masks at all times when around other people
ensuring good hand and respiratory hygiene.
All eligible people, especially those aged over 50, should be fully vaccinated against COVID-19, to protect themselves against severe illness and death. They should also avail themselves for booster shots where indicated.
From bathrooms to buses and public areas on campus, the unsung heroes in the Services Department wage a daily battle against the virus.
The people behind the Services Department, who have played an integral role in the implementation of Covid-19 protocols and preventative measures at the university, are celebrated as Wits Heroes.
Contribution during Covid-19 pandemic
When the Minister of Higher Education, Science and Technology, Dr Blade Nzimande announced that students were to begin a process of returning to campus and that universities should be ready for their return – Services responded positively. With a clear mandate to train staff on new protocols; source sanitisers; secure PPE and chemicals and disinfect buildings, the Services team sought to prepare campus for the return of students and staff.
Working day and night including weekends, the team distinguished themselves in service delivery under the ‘new normal’.
The Director of Services Israel Mogomotsi says that “despite the risks involved in the cleaning and hygiene sector and waste management, staff continued to deliver on their mandate.”
“They worked hard, regardless of the competing demands coming their way. They teamed up and focused on the job and delivered. Along the way we lost one of the Operations Manager to Covid-19” added Mogomotsi.
Twelve members of the management team and 30 staff members have tests positive since the start of the pandemic. One member, Magnath (Mags) Baijnath, a West Campus Operations Manager: Cleaning and Hygiene, unfortunately succumbed to the virus.
Drivers, cleaners and management
The Services team comprises of multiple members, from the cleaning to the management staff. The entirety of the group numbers 1188 employees from different sectors within the services department.
Mogomotsi says that each member has an equally important functioning to play.
“The role of cleaning and hygiene became recognised as a critical skill. Cleaning is a thankless job, and it requires continuous motivation of team members.”
Dining hall catering staff continued to prepare and serve meals in the residences, while intercampus bus drivers shuttled students around campus. The Department ensured the functionality of Wits’ campuses, handling the invisible and lack-luster detail that goes with the job.
To stay within the law, staff worked on a rotational timetable, which allowed them to finish work early to arrive at home in time for lockdown curfew. There was a prompt adaptation period to the new methodology of staff rotations with no conflicts or hesitancy within the group.
For the staff to adapt, it was not an individual task but a team-based and dependent system, explains Mogomotsi about the critical role of team work. The team is driven by the Department's strategic values known as Tads (Building Teams; Accountable; Quality Service Delivery; System integration).
“Services Department management team members displayed higher levels of determination, flexibility and they worked hard. The different units pulled together and worked as a collective to ensure that we achieve the expected service delivery.”
Looking ahead to 2022, Mogomotsi hopes that the virus will be well managed as staff and students return to campus. “We look forward to contributing and supporting the activities towards centenary events celebrations.”
The managers in the Services Department recognised for outstanding work and leadership are: Leah Mathabe, Veliswa Mbolekwano, Nicholas Matthes, Cristina Tomas, Jeane-Pierre Tollemache, Thapelo Musekwa , Connie Tshimangadzo, Chris Ziyambi, The late Magnath Baijnath, Cameron Watt, Veronica Mbonani, Rueben Chaibva, Timothy Mudau, Karen Du Plessis, Lebogang Maila, Ricardo Fernandos , Nodumo Buso, Janice De Gouvela and Haqiqat Ismail.
About Wits Covid-19 Heroes
The Wits Heroes Series celebrates staff and students who went beyond the call of duty at the onset of Covid-19 in 2020. Wits Heroes were nominated by members of the Wits community. Discover other Heroes.
South Africa has changed tack on tackling Covid: why it makes sense
- Shabir A. Madhi, Fareed Abdullah and Jonny Myers
The South African government has chosen a pragmatic approach that balances the potential direct and detrimental indirect effects of Covid.
In the final days of 2021 the South African government eased its COVID regulations. On December 30th the government scrapped a curfew that had been in place since March 2020. It also initially announced an easing around quarantines and contact tracing but subsequently reversed these plans. Nevertheless, its approach sets a new trend in how countries are choosing to manage the pandemic. Shabir Madhi and colleagues reflects on the boldness – and the risks.
What are the main elements of its new approach?
The South African government has decided to take a more pragmatic approach while keeping an eye on severe COVID and whether or not health systems are imminently under threat. This reflects an acceptance that governments will increasingly be looking for ways to live with the virus cognisant of the detrimental indirect effects that restrictions have been having on the economy, livelihoods and other aspects of society. This is particularly pertinent in resource-constrained countries such as South Africa.
The latest announcements mark a significant departure in the way forward. They mark a pragmatic approach that balances the potential direct and indirect detrimental effects of COVID.
Our hope is that the government continues to pursue this approach and doesn’t blindly follow policies that are not feasible in the local context, and ultimately yield nominal benefit.
The new, more nuanced approach is in stark contrast to reflexively imposing higher levels of restrictions as case rates increased. This suggests that the government has taken note of commentary that has provided suggestions to focus on whether the health facilities are imminently under threat, rather than simply going to higher levels of lockdowns.
The main element of the new approach arises from a high level of population immunity. A sero-survey done in South Africa’s economic hub, Gauteng, just prior to the onset of the Omicron wave indicated that 72% of people had been infected over the course of the first three waves. Sero-positivity was 79% and 93% in COVID-19 unvaccinated and vaccinated people older than 50 years a group that had previously made up a high percentage of hospitalisations and deaths.
The sero-survey data show that immunity against severe Covid in the country has largely evolved through natural infection over the course of the first three waves and prior to the advent of vaccination. This has, however, come at the massive cost of 268, 813 deaths based on excess mortality attributable to Covid-19.
The presence of antibodies is a proxy for underlying T-cell immunity which appears to play an important role in reducing the risk of infection progressing to severe COVID. Current evidence indicates that such T cell immunity, which has multiple targets and even more so when induced by natural infection, is relatively unaffected even by the multiple mutations in Omicron and is likely to persist beyond a year. This sort of underpinning T-cell immunity that reduces the risk of severe disease should provide breathing space for at least the next 6-12 months, and possibly beyond that.
Even though Omicron is showing heightened anti-spike protein antibody evasiveness relative to even the Beta variant, vaccine and natural infection induced T-cell immunity has been relatively preserved.
This could explain the uncoupling of the case rate compared with the hospitalisation rate, and even more pronouncedly, with the death rate. In addition, other changing characteristics of the Omicron variant caused by the mutations appear to make it more efficient in infecting and replicating in the upper rather than the lower airway. This could also be contributing to lower likelihood of progressing from infection to severe diseases.
Source: Jonathan Elliot Myers and Fareed Abdullah.
In the meantime it’s crucial that a number of steps are taken.
The drive to ensure higher uptake of vaccines, including booster doses for high-risk groups, needs to continue.
Also, considering that only 10% of infections are actually documented in South Africa because so few people are being tested, a more pragmatic approach to isolation is warranted, mainly if people are symptomatic. This also means that quarantining won’t bring about any major reduction in transmission.
There also needs to be recognition that contact tracing in South African and other similar settings is unlikely to be of any value. This is because the average person in South Africa will possibly have 20 close contacts per day. And even symptomatic infected individuals are most infectious in the pre-symptomatic and early symptomatic phase.
The ineffectiveness of contact tracing and quarantine in limiting the spread of the virus in South Africa is corroborated by three quarters of the population having been infected over the course of the first three waves.
In our view, there is also room for the gradual relaxing of non-pharmacological interventions. In particular, token gesture “hand hygiene” and superficial thermal screening should be scrapped. And there is little reason not to be allowing events such as attendance to outdoor sports events.
Instead, at least for the immediate future, the government should continue focusing on interventions like masking in poorly ventilated indoor spaces and ensuring adequate ventilation.
The issue of mandatory vaccinations is still on the radar, as it extends beyond the added risk that unvaccinated poses to others. And the greater pressure they place on the health systems when they are hospitalised for Covid.
Attention also needs to be given to how incidental COVID infections – people diagnosed with Covid when they’re admitted for a non-related medical issue – are managed in hospitals. The Department of Health guidance needs to be adapted to manage these patients with the appropriate level of skill and resources for the primary reason they were admitted. And patients with severe COVID-19 disease require additional care and expertise to improve their outcomes.
Finally, an evaluation of both vaccination status and underlying immune deficiency needs to become a key element of the workup of hospitalised patients with severe COVID.
Is it clear what the goals are?
The goal has to be minimising hospitalisation and death. It is unnecessary to be stressing out the economy, other health services and livelihoods in South Africa. The death rate with Omicron wave in South Africa is on track to be approximately one-tenth compared to the Delta wave. This means it possibly on a par with deaths caused by seasonal influenza pre-Covid – 10,000 to 11,000 per annum.
It’s impossible to say what the characteristics of future variants would be over time. But the experience with the Omicron wave in South Africa provides some comfort that immunity against severe disease and death will continue tracking downward, particularly if vaccine coverage can be increased to 90%, particularly in the >50 year age group. The high force of infection that has likely transpired with Omicron will also further contribute to enhancing protection against severe COVID-19 in the immediate future.
What are the risks?
The major risk is the unpredictability of new variants that evade all aspects of past infection and vaccine-induced immunity. But this is likely to be the result of the evolution of the virus rather than any changes in policy.
Another risk is failure to change the pandemic mindset and failure to appreciate that with Omicron the epidemic phase of COVID-19 is coming to an end. The country and all its institutions and people need to prepare to get back to a previous life – most notably the health services.
The South African government appears to have come to appreciate that the past practices have had limited success in preventing infections, and fully appreciates the detrimental effects that restrictions have had on the economy and society. In addition, it has run out of road to continue with what has unfortunately not yielded much benefit. Despite all the severe lockdowns South Africa still ranks high with a Covid death rate of 481 per 100,000.
Covid-19 Update 77: Wits Covid-19 Vaccination Implementation Plan
- Wits MVAX Policy Implementation Committee
Wits Universit's Mandatory Vaccination Policy (MVAX Policy) will be implemented in January 2022.
Wits University adopted a Mandatory Vaccination Policy (MVAX Policy), which will be implemented from 1 January 2022. The Policy states that all members of the University community will be required to vaccinate against COVID-19 in order to access the University’s premises, aside from those who have been granted Reasonable Accommodation. Members of the Wits community will have until 1 March 2022 to get vaccinated or be granted Reasonable Accommodation.
All persons accessing Wits campus or premises will need to upload their Vaccination Certificate or apply for Reasonable Accommodation on the Wits Vaccine Implementation Portal.
The Policy is for everyone’s protection to reduce transmission and severity of the SARS-CoV-2 virus, allowing us to get back to campus for teaching and learning.
PLEASE NOTE: Access to upload your vaccine certificate or to apply for Reasonable Accommodation will ONLY OPEN IN MID-JANUARY 2022. The date will be communicated in the New Year.
Step 3: Upload your Vaccination Certificate or Vaccination QR Code:
Students: Upload to the Student Self-Service Portal (Link will be active mid-January 2022)
Staff: Upload to the Wits Staff Intranet Portal (Link will be active mid-January 2022)
You will need to log in with your student/staff number and Wits password before 1 March. (You can still upload your certificate and gain access to campus if you have only one shot (Pfizer), but will need to upload the certificate for your second shot within 60 days to continue to have access to campus). Students registering in person or without internet will be assisted to upload their certificate manually.
Step 4: Once verified, you will receive confirmation via email
Step 5: Your access card will be activated to enter Wits campuses, buildings and Wits buses because you have been vaccinated
As of 1 March, all students and staff entering campus via the pedestrian gates or in vehicles will be required to present their access card confirming vaccination status. Handheld card reader devices will be available to accommodate people who are carpooling.
How to Apply for Reasonable Accommodation
Members of the Wits community who are unable to vaccinate due to medical or Constitutional reasons, may apply for Reasonable Accommodation (RA).
Step 1: Log into the Student Self-Service Portal or Wits Staff Intranet Portal (Links will be active mid-January 2022)
Step 2: Complete the online Reasonable Accommodation Application Form and upload supporting documents (doctor’s letter or an affidavit with motivation)
Step 3: You will receive an email confirming receipt of your application
Step 4: Your Department/Line Manager or Faculty Registrar/Committee will consider the request and approve or deny the application
If your RA is approved, you will receive email confirmation and your access card will be activated so that you can enter campus as you have been provided Reasonable Accommodation. You will need to abide by all Wits’ COVID-19 Protocols (see below), and take and upload a weekly negative antigen test result from an accredited service provider to the Student Self-Service Portal or Wits Staff Intranet Portal (Links will be active mid-January 2022).After verification of the antigen test result, your access card will be activated for seven days only. Thereafter, you need to repeat the steps each week, uploading a negative antigen test to be provided with seven days of access to campus.
If your RA is denied, you will be advised via email. You may choose to accept the decision and get vaccinated (See Step 1 - How will it Work?) or may choose to appeal the decision (See Step 5).
Step 5: You can appeal to the Mandatory Vaccination Appeals Committee by logging into the Student Self-Service Portal or Wits Staff Intranet Portal (Links will be active mid-January 2022). Complete the online Reasonable Accommodation Appeal Application Form and upload supporting documents (doctor’s letter or an affidavit with motivation)
If your Appeal is approved, you will receive email confirmation and your access card will be activated so that you can enter campus. You will have to abide by all Wits’ COVID-19 Protocols (see below), and take and upload a negative antigen test result from an accredited service provider to the Student Self-Service Portal or Wits Staff Intranet Portal (Links will be active mid-January 2022) every week. After verification of the antigen test result, your access card will be activated for seven daysonly. Thereafter, you need to repeat the steps each week, uploading a negative antigen test to be provided with seven days of access to campus.
If your Appeal is denied, you will be advised via email. You may choose to accept the decision and get vaccinated (See Step 1 – How will it Work?) or you may need to put your studies in abeyance or deregister (students) or resign (staff). There is no further appeal process.
Abide by Wits’ COVID-19 Campus Protocols
Everyone must abide by all national regulations and Wits’ COVID-19 protocols when on campus.
Wits will have a Pop-Up Vaccination Site on campus from mid-January 2022 and will provide COVID-19 antigen testing on-site (Students/staff may apply to qualify for free testing when they apply for Reasonable Accommodation for those who can’t afford it).
Covid-19 Update 78: Implementation of Wits Mandatory Vaccination Policy
- Wits MVAX Operations Committee
Wits University adopted a Mandatory Vaccination Policy (Mvax Policy), which will be implemented from 1 January 2022.
This communication serves to provide operational information on the Wits’ Mandatory Vaccination Policy (MVax Policy) which came into effect from 1 January 2022. The Policy seeks to enable the return of employees and students to the University’s precincts whilst protecting the health and safety of our community, and all who work, live, learn, and/or participate in activities on campus.
Get vaccinated or apply for reasonable accommodation
The Policy states that all members of the Wits community are required to vaccinate against COVID-19 in order to access Wits’ premises, aside from those who have been granted reasonable accommodation. Most members of the University Community have until 1 March 2022 to get vaccinated or be granted reasonable accommodation. Please note however, that in terms of the MVax Policy, students will not be provided with housing in any University-owned or managed residences if they are not vaccinated. All students who have applied to Wits residences must therefore be vaccinated before they will be granted housing accommodation in Wits residences. The reasonable accommodation process does not apply to this cohort of students. In addition and given that they start earlier than other cohorts of students, first-year students in the Gateway to Success Programme will need to show proof of vaccination or be granted reasonable accommodation before 5 February 2022.
How it works – Staff and Students upload your Vaccine Certificate
Step 1: Get vaccinated at any vaccination site nationally or visit the Wits Vaccination and Testing Site in the Wits Sports Hall on the Braamfontein Campus (opens 1 Feb 2022).
Step 3: Upload your Vaccine Certificate with its QR Code to the Wits Vaccine Implementation Portalfrom 20 January 2022. Log in with your student/staff number and Wits password.
Step 4: Once verified, you will receive confirmation via email. Your access card will be activated to enter Wits’ precincts, campuses, buildings and buses because you have been vaccinated.
Please note: You can gain access to campus if you have received the Johnson and Johnson vaccine or one shot of the Pfizer vaccine, but you will need to upload the certificate for your Pfizer second shot within 90 days to continue to have access to campus. Persons will also need to get a booster shot as and when recommended by the national Department of Health and the National Institute of Communicable Diseases.
OR
Apply for Reasonable Accommodation
Wits staff and students may apply for reasonable accommodation (on medical or Constitutional grounds) from 25 January 2022. Log in with your student/staff number and Wits password.
Wits' Vaccination and Testing Site
Wits will host a Vaccination and Testing Site in the Wits Sports Hall on the Braamfontein Campus from 1 February 2022, which will offer access to vaccines and boosters, and provide antigen testing on-site. Students and staff who cannot afford it may qualify for free antigen testing when they apply for reasonable accommodation.
How does the MVAX Policy affect you?
Students
Students are required to vaccinate or apply for and be granted reasonable accommodation before 1 March 2022.
Students in Wits Residences
All students who apply to live in Wits residences will need to be vaccinated due to the close living configuration, level of occupancy and associated risks in residences. Only students with proof of vaccination will be able to apply for and live in Wits residences as per the MVax Policy. No exceptions will be made.
Staff
Employees are required to vaccinate or apply for and be granted reasonable accommodation before 1 March 2022. Staff cannot refuse to return to work on the basis of not having been vaccinated.
Service providers and contractors
Personnel of service providers and contractors are required to be vaccinated by 1 March 2022 to access campus. No service provider will be allowed on campus without proof of identification and proof of vaccination. Contractors, suppliers and vendors can read more on the Wits Vaccine Implementation Portal.
Visitors
Visitors to Wits’ campuses will be required to show proof of identification and proof of vaccination by 1 March to enter Wits’ premises. Visitors read more on the Wits Vaccine Implementation Portal.
Covid-19 Campus Protocols
All persons entering the Wits campus are expected to follow the COVID-19 Protocols of 1M + 2V + 3Ss: Wear a face Mask, stay in Ventilated areas, Vaccinate, complete the COVID-19 Screening Tool, keep a Social Distance of 1.5m and Sanitise hands regularly.
Covid-19 Update 79: You can now upload your vaccine certificate
- Wits Mvax Operations Committee
Mandatory vaccination: The link to upload your vaccine certificate is now live.
You can access it via the Wits Vaccine Implementation Portal. Please be advised that all those who uploaded certificates yesterday to the test site will need to upload it again to the live site. Due to a slight technical delay, staff and students will only be able to apply for reasonable accommodation from 25 January 2022.
How to upload your Vaccine Certificate (staff and students)
Step 1: Get vaccinated at any vaccination site nationally or visit the Wits Vaccination and Testing Site in the Wits Sports Hall on the Braamfontein Campus (opens 1 Feb 2022).
Step 3: Upload your Vaccine Certificate with its QR Code to the Wits MVax Implementation Portal from today, 20 January 2022. Log in with your student/staff number and Wits password.
Step 4: Once verified, you will receive confirmation via email. Your access card will be activated to enter Wits’ precincts, campuses, buildings and buses because you have been vaccinated.
Please note: You can gain access to campus if you have received the Johnson and Johnson vaccine or one shot of the Pfizer vaccine, but you will need to upload the certificate for your Pfizer second shot within 90 days to continue to have access to campus. Persons will also need to get a booster shot as and when recommended by the national Department of Health and the National Institute of Communicable Diseases.
Remember that all students who apply to live in Wits residences will need to be vaccinated due to the close living configuration, level of occupancy and associated risks in residences. Only students with proof of vaccination will be able to apply for and live in Wits residences as per the MVax Policy. No exceptions will be made.
OR
Apply for Reasonable Accommodation from 25 January 2022
Due to a slight technical delay, Wits staff and students may apply for reasonable accommodation (on medical or Constitutional grounds) from 25 January 2022. Log in with your student/staff number and Wits password
If you are experiencing glitches in uploading your certificate, this information might help. You can also log technical queries via ithelp@wits.ac.za.
Over 7 500 staff and students uploaded their vaccine certificates to the Wits MVax upload portal yesterday. Thank you!
Some people have received communication indicating that their vaccination status could not be verified for various reasons. Thank you to those who have brought it to our attention – we are doing our best to troubleshoot the glitches. The information below may help.
The Government Vaccination Certificate System website URL: https://vaccine.certificate.health.gov.za/ is not accessible when using Internet Explorer. Please try using the Chrome, Firefox, Edge or Safari browsers.
International students and staff, or persons who have international vaccination certificates/cards will be able to upload their vaccination certificate or vaccination card from 25 January 2022 to the Wits Wits MVax Upload Portal. Choose the option for “International Vaccination Certificate” from the drop-down menu.
Persons who were part of a Vaccine Trial or Vaccine Study will be able to upload their vaccination documents from 25 January 2022 to the Wits MVax Upload Portal. Choose the “Vaccination Trial/Study Certificate” from the drop-down menu.
The MVax Helpdesk to assist with the manual uploads of vaccination certificates or any other queries will be set up on the ground floor of Solomon Mahlangu House from 25 January 2022. There will also be an MVax Helpdesk at the Assisted Registration area at Sturrock Park starting from 27 January 2022. Please visit the MVax Helpdesk for assistance or log technical queries via ithelp@wits.ac.za.
Let us vaccinate to congregate!
End SA’s national state of disaster
- Francois Venter, Marc Mendelson, Jeremy Nel, Lucille Blumberg, Zameer Brey and Shabir A Madhi
Covid-19: On 15 March 2020, President Cyril Ramaphosa declared a national state of disaster in terms of the Disaster Management Act.
Almost two years on, we are entering a new phase of the pandemic. All over the world, including within the WHO, there is an assessment taking place of the measures that will be most suited to this phase. Top of the list is vaccination, good indoor ventilation, and close monitoring of the SARS-Cov-2 virus and other possible pandemic threats.
South Africa needs to do this too. As scientists, our current understanding of the science, the building of immunity protecting against severe Covid-19, and experience with policy renders most state of disaster measures still in place unfit for purpose and requires tailoring of others.
Being on permanent “Code Red” affords little protection against a hyper-transmissible SARS-CoV-2 variant such as Omicron and entails unacceptable societal costs.
SARS-CoV-2 has been a devastating virus, killing friends, family and colleagues, as well as leaving many people with symptoms oflong Covid. We are not suggesting ignoring it, but the risk is changing for South Africa and our response needs titrating against the risk it poses.
We have no truck with Covid-denialists or anti-vaxxers.
But change is needed now. The focus on Covid-19 has set back many other health programmes and broader socioeconomic and educational programmes.
Finally, the continued lack of accountability and transparency the act affords to politicians for unscientific and irrational decision-making on issues of public health is long past justification.
Further evolution of SARS-CoV-2 may generate more variants, but the foundation of protection from severe disease, hospitalisation and death that is our immune response — whether by prior infection (now, very conservatively, an estimated three quarters of South African inhabitants) or by vaccination (for about a third) — has been consistently exhibited across the three waves caused by the Beta, Delta and now Omicron dominant variants.
The decoupling of infections and severe disease and death from Covid-19 has been most stark in the waning Omicron-dominant wave in South Africa, despite earlier theoretical concern about the spectrum of mutations identified in the variant.
Omicron, a variant that causes many millions of infections (possibly infecting half the South African population), did not result in significant stress on the country’s health system through hospitalisations andexcess deaths (see here).
Consequently, despite formal case numbers probably equating to the combined total of both the first and second Covid-19 waves, immunity derived from prior infection and vaccination protecting against severe Covid-19 won the day.
We believe that this is likely to continue in future waves, barring the unlikelihood of mutations affecting all aspects of immune responses, which would be analogous to a completely “new” type of virus having evolved from an immunological perspective.
In such an unlikely scenario, as would be the case for the immediate emergence of another novel pandemic-causing virus, containment measures could be reconsidered. But we can’t proceed as if this is the likely scenario — it isn’t, and the costs of pretending it is too high.
The vast majority of South Africans now have immunity, meaning Covid-19 in 2022 is likely to have a similar death rate to seasonal influenza (10,000-11,000 deaths a year) in the pre-Covid era, as opposed to the290,000 Covid- related excess deathsover the past 22 months of the pandemic, and much lower than the projected58,000 annual TB-related deaths.
Hence, as the beginning ends, we believe the time is now to immediately end those measures that serve no purpose, some of which are detrimental, and progressively enable a return to normal.
End the state of disaster
We see no reason for the continued use of this legislation, nor for the National Coronavirus Command Council.
In terms of SARS-CoV-2 the government should be single-mindedly focused on the vaccine programme and protecting health facilities from the impact of large numbers of admissions.
Our suggestions below do not require continued centralised, secretive and unaccountable decision-making for this to occur. Arguments that the state of disaster is required to enforce interventions like masks or limits on social gatherings are unconvincing, as most restrictions need to be lifted anyway;improved communication, together with conventional legal and social persuasion mechanisms can be used to ensure that the very limited number of interventions required are executed.
We know the vital Covid Social Relief of Distress (SRD) grant is linked to the Disaster Management Act, and it is vital for millions of people’s livelihoods that this continues.The Department of Social Development Expert Panel on Basic Income Supporthas provided clear guidance regarding how this can be continued under the Social Assistance Act, which we support.
We are advocating that Covid be seen as another health priority, with rapid decision-making led by the Department of Health consulting other departments through inter-ministerial or other existing legislative structures. There is a multiplicity of examples of where health collaborates closely with other departments, and these can be employed.
Stop school restrictions
The impact on education has been severe, and we are now at the point where every resource should be focused on making 2022 a “back to normal” year.
Unfortunately, the Minister of Education has announced further rotational learning —a huge mistake.
Children experience only a very small chance of harm from infection with SARS-CoV-2, except for those under one year of age or in the presence of underlying medical conditions. Children suffer illnesses from influenza and a range of other viruses and infections too, and we sent them to school prior to this pandemic, understanding the massive benefits to child health and development.
Furthermore, keeping children out of schools inflicts harmto the social/financial fabric of the household when carers have to stay home to mind the kids (anyone doubtful about the huge consequences of these school disruptions should readthis Unesco documentcapturing the harms in detail).
Schooling needs to happen again as normal. Vaccine mandates are appropriate for all educational staff, for their own health and to protect children by avoiding further disruptions to teaching. Teachers or other educational workers should be assisted with attention to ventilation and encouraged to wear masks indoors if they are in high-risk groups.
With the very high levels of asymptomatic transmission and community immunity present, there is no reason to continue restricting class sizes or children playing. Enforcing physical distancing measures in classrooms, such as requiring students to be 1.5 metres apart from each other, is impractical and not likely to substantially reduce transmission in the face of these new variants. Also, considering that for every one documented Covid-19 case in South Africa there are nine other undiagnosed cases due to limited testing, there is no place for school closures when cases of Covid-19 are identified.
Reform how Covid is handled in healthcare facilities
The ongoing restrictions on allowing family visitors in hospitals are unnecessary and cruel.
Testing asymptomatic patients for Covid indefinitely is a waste of money and resources — even in hospitals, in most instances. Testing of people with respiratory symptoms, especially when there is a resurgence, should continue into the immediate future as it could assist in management of the person.
As for educators, vaccine mandates for healthcare workers make sense, to protect them at an individual level, and the health system from sickness-related absenteeism.
Also, healthcare workers, being more susceptible to being infected because of the nature of their work, might require annual booster doses of vaccines to enhance protection even against mild disease. Also, booster doses to healthcare workers could reduce the risk of them transmitting the virus to vulnerable patients.
Finally, meaningful managerial support to facilities — ensuring the mundane, but crucial everyday issues such as staffing, compliance with general infection prevention measures, oxygen and drug supply, and ambulance services, which was found wanting despite plenty of warning, especially during the first three waves — should be a primary focus of the Department of Health.
Furthermore, masks should no longer be compulsory outdoors. Vulnerable people may elect to wear a mask outdoors in crowded circumstances, while understanding that vaccinations will provide the greatest protection to their health.
What about indoor restrictions?
We must eventually accept that indoor restrictions will have to end too. As an intermediate step, vulnerable people may be advised to avoid crowded indoor venues when the Covid caseload is high, and/or wear a mask for added protection.
As medical veterans of mask-wearing, we have no patience with arguments around discomfort, health or misguided infringements of freedoms. However, we can’t keep wearing masks in all indoor circumstances forever, and more so now that the risk of severe Covid-19 is greatly diminished compared with earlier stages of the pandemic when there was little immunity against severe Covid-19.
Masks, especially high-quality masks, work when fitted well, but we have to anticipate that — for all but the most vulnerable patients — our immune systems are going to be enough to protect us (vaccines!).
There may be places where masks stay mandated (on densely packed public transport), but overall, the indoor mask-wearing mandate should eventually fall away.
End routine sanitising (and taking of contact details)
We think having routine foot-pump hand sanitisers at the entrance to bathrooms, food markets and crowded venues is good hygiene, and one of the few things we want left over from the pandemic — not for the prevention of Covid-19, but for all the other nasty bugs killed by handwashing.
However, the “hygiene theatre” at many workplaces, venues and restaurants, with the spraying of hands repeatedly with alcohol sprays combined with thermometry, both of uncertain quality, and recording of names and cell numbers with no intention of following up, is a waste of time and distracts from things that make a difference —opening windows and encouraging ventilation.
End routine thermometry and daily screenings
It is a useless waste of time and money. Always was. Many infections are asymptomatic, and even when they’re not, a fever is only present in a small minority of cases. Most of the readings of less than 35oC imply the person is dead or rapidly becoming so!
Also asking people to complete a questionnaire on whether they have any symptoms of Covid-19 is meaningless, since a large majority of infections would be asymptomatic. If individuals are symptomatic for respiratory illness (and not only due to Covid-19), they shouldalwaystake precautions of not infecting others by limiting their social engagement and wearing a face mask when in public. This message needs reinforcing: it is a basic of public health and infection control.
Stop fogging — yesterday
Another waste of time and money, but this time it can be harmful. This holiday, several of us stayed in places proudly advertising that they “fogged” between guests. We also note that government departments, despite their own guidelines from early 2020, persist in shutting down police stations, grant offices and schools, at massive cost.
Fogging is potentially harmful to health, using damaging chemicals, and is only used in highly focused infection outbreaks in health facilities.Cut it out.There is no scientific basis for the fogging and closure of any venue, including police stations and other government buildings following the diagnosis of an infected case.
Stop all PCR and antigen testing at borders
There is no reason for insisting on this when the virus is circulating so widely. Requiring testing for a plane trip from Gaborone to Joburg, but not Cape Town to Joburg, or for people driving in a private vehicle from Mozambique, makes no sense. It does not stop variants and even if someone with the virus slipped over the border, the contribution to existing infection rates is negligible.
This testing requirement, pervasive across the world, has created a massive money and time-wasting international industry, with no health benefits.
South Africa, a victim (and previous proponent) of baseless travel bans, should take a public and widely communicated step that the ONLY requirement to enter the country is proof of vaccination (or medical reason for not having vaccination), mainly to protect our hospitals and ICUs.
Instead, redirect these resources towards vaccinating at borders for those leaving and those coming into South Africa, recognising many of our neighbouring countries continue to have constrained vaccine supply.
Stop routine testing mild and asymptomatic cases
There is nothing to offer people who are positive that you wouldn’t offer for any mild respiratory infection. Routine testing of asymptomatic patients should stop. Staff should be vaccinated and theatre staff should use high-quality masks. PCR testing protocols (with gaps between testing and actual surgery) are far from perfect, and asymptomatic infection probably adds minimal risk to surgery.
Hospitalised symptomatic people should be tested, as we have treatments, but for mild disease, testing really only makes sense for those at high risk (so we can watch them closely, and for possible future access to new drugs that seem to work well at keeping this group out of hospital).
You can make a case for testing yourself if visiting granny or someone vulnerable, but understand that the tests are not perfect (they can give a false negative result) and that unless the person you are visiting is living as a hermit, their risk of exposure to someone else who isn’t testing and infected is very high.
Again, vaccines are the best protector of the vulnerable, including the need for a third dose of vaccines which the government needs to make available with fewer restrictions.
End quarantine and contact tracing
On 23 December 2021, the Ministerial Advisory Committee on Covid-19 issued revised protocols on contact tracing, quarantine and isolation, eliminating the need to contact trace and quarantine the contacts of people who tested positive. Five days later, the Department of Health rescinded the advisory.
Put simply, only a tiny percentage (~10%) of people who are infected with the virus will have been tested and found to be positive. Very high rates of asymptomatic infection, high levels of protective immunity against severe disease, and the social barriers stopping most of the population from effectively quarantining, makes the practice redundant.
For similar reasons — plus a lack of feasibility to contact trace even the people who have been in contact with a known case of Covid-19 due to the extreme numbers (remember, Omicron may have infected almost half the country) — it would make contact tracing an entirely moot point.
Reduce isolation
Currently, confirmed Covid-19 cases are asked to isolate for 10 days from their test (if no symptoms), or from the beginning of symptoms. Ten days came from original data which suggested that peak infectiousness was from one to three days pre-symptoms until eight days post the onset of symptoms. Recently, a number of countries, including the US, have shortened the isolation period to five days from test or symptom onset.
We believe theUS CDC’s more pragmatic approachof five days isolation, with a return to work and society using a mask for the next five days, is sound.
Even more pragmatic is to limit isolation only if a person is symptomatic.
Stop all curfews
The only reason for this was to protect health facilities from trauma-related hospital and ICU admissions. Our facilities coped with the last wave, so this reason no longer holds. The government would do much better to run high-profile education campaigns on alcohol harm and better policing and punishment of traffic and alcohol-related crime. Glad to see that all current curfews have been lifted.
Replace the current vaccination programme with something radically better
If we are called upon to suddenly boost the conservatively estimated 30% of the population that is vulnerable (the elderly and those with diabetes and obesity, the major readily identifiable risk factors for severe illness), at current rates it would take another year to get anywhere close — for Omicron, we perhaps had two weeks before the wave was firmly upon us.
The current system simply does not move quickly enough, and vaccine hesitancy is a convenient shroud to hide behind a system that is currently unable to deliver vaccines efficiently or conveniently.
Vaccines are our major protector — everything else is a mitigator — and we need a radical new strategy that makes getting vaccines as easy as buying milk and bread.
The main focus of the vaccine drive should be to achieve >90% vaccine coverage in people older than 50, and to provide third doses to very high-risk groups.
In addition: Replace the cumbersomeEVDS system’s registration requirements with a simplified guideline; allow the private sector to separately procure and distribute vaccines and start a proper seamless door-to-door campaign that aims to reach the millions of poor and undocumented (there are excellent Eastern Cape and other models); offer vaccines at routine medical queues and chronic medicine pick-up points, grants and pension queues, and central taxi vaccination distribution programmes.
For people needing certification so that they can cross borders, special sites can administer and provide digital certificates.
If we listen to individuals in communities (as done in the most recent Covid-19 Vaccine Survey), we will hear many people who are ready to be vaccinated asking for an easier, more convenient process. For example, 34% of the unvaccinated in the survey would get vaccinated as soon as possible, and of those, 70% would take the vaccine if offered at home or place of work.
Furthermore, messaging and administrative processes around EVDS leave much to be desired, with only a quarter understanding that pre-registration is no longer a requirement for vaccination.
We have never made electronic registration a requirement for any social or health programme, and introducing it in a pandemic is risky, even in well-resourced, high-income countries.
Arguments about duplication (“people getting more vaccines than they should”) are weak, with only a third of the country vaccinated.
Where data on specific demographics is available (perhaps captured retrospectively into the EVDS or similar system), it should be made public, so community-wide efforts to reach under-vaccinated populations can be made.
Vaccine mandates?
Some countries (like Greece and Austria) have made vaccines mandatory for vulnerable populations, with fines for noncompliance, reasoning that this is required to protect precious hospital and ICU resources.
Vaccination mandates have been implemented very effectively in many countries, including places with strong histories of individuality, such as France, and in many workplaces in South Africa.
We have no patience with the wilful misportrayal of vaccine side-effects by anti-vaxxers on social media, and the use of this argument against mandates.
The authors acknowledge the programmatic complexity and feasibility of vaccine mandates. The current vaccines work best in protecting against severe Covid-19 and are somewhat less predictable in preventing infections due to some antibody-evasive variants such as Beta and Omicron.
Nevertheless, Covid-19 vaccines still result in a quicker decrease in the viral load and lessen the duration of shedding, even due to Omicron, which would reduce the infectiousness of a person (seehere).
In the context of safeguarding healthcare systems from avoidable hospitalisations, as well as using whichever tools are available to us to safeguard people in high-risk indoor environments, mandatory vaccination should be considered, particularly when people are involved in indoor gatherings.
Dropping all these restrictions: what if we are wrong?
The virus has caught us off-guard on several occasions, especially regarding the remarkable transmissibility of Delta and Omicron, and theantibody-evasiveness of Omicron, and it may happen again. But we feel there are two extremes in the debate — a “we must stay on Code Red until we are certain’’ extreme (which does not acknowledge that we have a wealth of knowledge and experience now), and a “let-it-rip’’ extreme (which is a spectrum from understandable exhaustion and frustration with a lack of seeming progress on relaxing restrictions, to a range of over-confident pundits).
So what are we recommending?
In summary, we are recommending a risk-adjusted approach where scarce resources are much more targeted and the negative consequences of increasingly irrelevant measures, best described as Covid theatre, are discarded.
We are advocating for a strong focus on those at risk of severe infection by increasing vaccination, masks being worn when indoors and maybe avoid indoors during a wave. In the long term, vaccination is by far the greatest priority over other measures (including boosters, as needed).
It is quite possible to responsibly open society rapidly while maintaining early monitoring systems — something South Africa is blessed with.
Remember that all the current vaccines, as well as immunity from past infections, maintained high protection against severe Covid and death against ALL the variants, across the globe, and probably will work against the next one.
A cautious approach would be to get rid of the above measures, while monitoring and sounding any early alarms such asongoing sentinel wastewater surveillanceto detect an increase in virus load in the community.
Once there is a suggestion of a new surge of infections, increasing attention to new vaccination requirements (by fast-tracking vulnerable people to boosters, if the science suggests this), while monitoring and ensuring health facilities are prepared, makes sense.
At the same time, communicating carefully and transparently regarding any escalating risk, especially to vulnerable populations, may allow them to take additional measures to protect themselves: they may temporarily want to pay more attention to distancing and masking indoors, as much as they are able.
Government support to vulnerable populations thus far has been poor, and unfocused, so attention to this group — delivery of medication at home, food security, home vaccinations and other assistance — should receive priority. Many of the innovations that healthcare workers have developed in this vein should remain part of the health system in perpetuity as they take us closer to patient-centric care.
Finally, there is as great a chance that we are at risk of another pandemic virus in the future, as of the evolution of this one. TB and seasonal influenza were major killers pre-Covid and will remain so, as we have not addressed social determinants of infection.
We call on the South African government to set up a permanent pandemic preparedness body, be it a Ministerial Advisory Committee on Emergency Preparedness or Strategic and Technical Advisory Group, to monitor global threats, ensure that the policies and procedures are in place to rapidly move the country into pandemic mode (if needed), and that supply chain requirements are met.
Finally, we all need to reflect on the fact that there are also several current pandemics that continue to kill tens of thousands of people every year in South Africa — TB, pneumonia, HIV, antibiotic-resistant infections — which never went away. Many are prevented by vaccines or treatment — and greater attention needs to be focused on those, too.
Francois Venter, Ezintsha, Faculty of Health Sciences, University of the Witwatersrand. Marc Mendelson, head of Infectious Diseases and HIV, University of Cape Town. Jeremy Nel, Head of Department, Infectious Diseases, University of the Witwatersrand. Lucille Blumberg, Right To Care and University of Stellenbosch. Zameer Brey, health systems adviser and Groote Schuur Hospital board member. Shabir A Madhi, Dean, Faculty of Health Sciences and Professor of Vaccinology, University of the Witwatersrand.
The Gender Commission has failed women
- Ames Dhai, Helen Rees, Glenda Gray, Aslam Dasoo, Mike Sathekge, Angelique Coetzee, Priya Soma-Pillay, Yasmin Adam, Lee Fairlie
Scientists say the Commission’s statement against mandatory vaccinations is offensive, irresponsible and misleading.
Scientists call on the Gender Commission to withdraw its statement, engage with the relevant institutions, societies and experts and replace it with one that truly addresses Covid-19 reproductive health concerns.
On 16 January, the Commission for Gender Equalityissued a statementtitled “Gender Commission on imposing mandatory Covid-19 vaccination”, in which it noted a study published in theJournal of Obstetrics and Gynaecologyearlier in the month that found vaccines cause a small, but temporary change in menstrual cycle length. In the article, the commission misinterprets the paper and also fails to consider the many other harmful impacts associated with Covid-19 disease and reproductive health that make immunisation a priority for women of childbearing age.
In theObstetrics and Gynaecologyarticle (onlinehere) cited by the Gender Commission,the authors found that in women using Pfizer-BioNTech (55%), Moderna (35%) or Johnson & Johnson/Janssen (7%), Covid-19 vaccination was associated with a less than a one-day change in cycle length for both vaccine-dose cycles compared with pre-vaccine cycles (first dose 0.71 day-increase, second dose 0.91 day-increase). The overall conclusion of the study was that theirfindings were reassuring in that there was no population-level clinically meaningful change in menstrual cycle length associated with Covid-19 vaccination and that Covid-19 vaccination was not associated with changes in menses length.
Using this study as justification and ignoring the study’s reassuring conclusions, the Gender Commission cautioned businesses and institutions against forcing employees to vaccinate and recommended against imposing sanctions against them if they did not vaccinate against Covid-19.
It furtherwarned that mandatory vaccination mandates do not supersede South Africa’s Constitution and its provisions and that“Maintaining public health, reaching herd immunity, and preventing mutating Covid-19 variants are noble acts but should not be achieved by trampling the basic human rights that are enshrined in the Constitution.”
The commission specifically noted that the large numbers of young females employed as cashiers and cleaners in South Africa’s retail sector were unable to negotiate with their employers, should they not wish to vaccinate.
In addition, it called for institutions of higher learning to “afford the same respect to students and workers who may not wish to vaccinate”. It further stated that many students and workers were not empowered to negotiate with big corporates and institutions and attributed this shortcoming to the country’s legacy of oppression, economic inequality and limited access to information.
The commission underscored that section 12 (2) of the Constitution on the rights to bodily and psychological integrity, which include the rights to make decisions concerning reproduction; to security in and control over their body; and not to be subjected to medical or scientific experiments without informed consent could not be infringed.
However, the Gender Commission, in its misunderstanding and hence misrepresentation of the study’s findings, asserts thatdue to possible long-term effects from what it describes more broadly as a scientifically established connection between Covid-19 vaccinations and women’s reproductive health, many women may not be comfortable taking vaccines.
In so doing, the Commission ignores the fact that, as explained below,Covid-19 itself poses an enormous threat to women’s reproductive health, and that addressing the low vaccine uptake among women of child-bearing age is both ethically imperative and a human rights obligation for the protection of their reproductive health in the ongoing pandemic.
Unfortunately, such messaging compounds young peoples’ concerns regarding fertility and Covid-19 vaccination, which isunfounded in published literatureand undermines vaccination efforts. Low uptake of Covid-19 vaccination in pregnant and breastfeeding women in public health facilities remains a concern and frequently stems from healthcare workers themselves not following recommended guidance due to their own beliefs and misperceptions.
In publishing an article like this, the Gender Commission seems oblivious of the danger of the assertions made in its statement — that “the enthusiasm of women of reproductive age for receiving a Covid-19 vaccine may be negatively curbed especially in light of currently circulating anecdotal claims of the vaccines adversely affecting fertility and pregnancy”.
Rather than debunking these contentions and reassuring the women, it claims that there is no available scientific evidence to support such assertions, it causes further harm to them by issuing cautions and warnings based on false information and a misreading of the science.
It is unclear how the commission has come to the conclusion that reproductive health is negatively affected withregard to a less than one-day change in cycle length that corrects itself the following cycle. While some studies have noted menstrual changes after mRNA and adenovirus vectored Covid-19 vaccinations, menstrual lengths return to normal with the following cycle. Moreover, in a study of menstruating women, it was found that a quarter of those that had been infected with SARS-CoV-2 experienced menstrual disturbances.There is no evidence that the use of Covid-19 vaccines adversely affects women’s long-term reproductive health.
Of note, there is currently no evidence that Covid-19 vaccinations cause infertility (see Association of Reproductive and Clinical Scientists, British Fertility Society, Covid-19 vaccines and fertility, 2021here, an article in theJournal of Obstetrics and Gynaecologyhere) and in clinical trials, unintended pregnancies occurred at the same rate in both the vaccinated and unvaccinated women.
Studies (seehereandhere) have also found that being unvaccinated is a huge risk to women in the reproductive age group as being infected with Covid-19 starkly increased pregnancy complications, including stillbirths and critical care admissions among the unvaccinated groups.
Sahpra’s current guidance is that Covid-19 vaccines for women of childbearing age and pregnant women are recommended.Using evidence generated by robust scientific studies, theCDC (US),WHO,NHS (UK), other internationally recognised authorities and the SA Vaccine Ministerial Advisory Committeehaveissued guidelines and advisoriesemphasising the importance of Covid-19 vaccination for women in this age group.
It is disconcerting that the Gender Commission, a Chapter 9 Institution of the SA Constitution and an organ of state, would stray from its constitutional mandate as set out in section 187(2).
The commission must promote respect for gender equality and protect, develop and attain gender equality. In realising its mandate, it has the power to monitor, research, educate, lobby, advise and report on issues concerning gender equality as regulated by the Commission for Gender Equality Act 39 of 1996.
The drafters of the Constitution judged it to be necessary to create a separate independent institution to deal with the distinctive needs of women, considering the unfair discrimination South African women were subjected to during the colonial and apartheid eras, and the patriarchal nature of society in our country.
Given the history of South Africa and the reason the commission was established, it is unfortunate and unacceptable that the commission seems to have lost its way and muddled the issues emanating from the mandatory vaccination debates with women’s reproductive health and rights. In addition, similar to theinitial utterances from the Human Rights Commission (SAHRC)(also a Chapter 9 Institution), it is clutching at the wrong end of the stick and missed the point on individual rights versus public health needs when it uses section 12 of the Constitution to admonish employers and institutions regarding the “trampling” of human rights.
Notwithstanding the entitlements to rights, most rights in the Constitution may be limited, provided the limitation is of general application, and is “reasonable and justifiable” — which means that it is rational, proportional and the least restrictive in terms of achieving its objective (section 36). It is argued that, where backed by scientific evidence and the rights of all people to a safe environment, (both at work and educational institutions), it would be “reasonable and justifiable” to compel workers and students to take a vaccine that is available and approved for use by the Sahpra.
Fortunately, the SAHRC reviewed its communication and in September last year, while strongly encouraging voluntary vaccinations, recognised that theexistential crisis caused by the pandemic affected all human beings and also that there were implications on both rights and responsibilities. Itstated, therefore, that it was highly likely that a general law mandating vaccination would pass constitutional muster.
The purpose of Chapter 9 Institutions is to support and protect our constitutional democracy. It is essential that they monitor the government and assist us in holding the government accountable. They need to ensure that South Africa transforms into a society in which social justice prevails. Social justice includes gender justice. The Gender Commission has failed the women it is mandated to protect by failing in its responsibility to make certain that prior to communicating with the public, its statement was well researched and based on robust scientific evidence.
On the contrary, its statement is offensive and diametrically against women’s education and empowerment, and an impediment to attaining gender equality.
We call on the Gender Commission to withdraw its statement, engage with the relevant institutions, societies and experts and replace it with one that truly addresses Covid-19 reproductive health concerns. Instead of misconstruing science to justify a stance against mandatory Covid-19 vaccinations, it would bode well for it to use the available evidence to build up and strengthen vaccine confidence among women. Surely, in this way, its mandate to promote and protect reproductive health and rights of women will be realised.
Ames Dhai is Chairperson Bioethics Advisory Panel (SAMRC) and Unesco International Bioethics Committee, Visiting Professor Bioethics, Wits School of Clinical Medicine, Faculty of Health Sciences.
Helen Rees,Executive DirectorWits Reproductive Health and HIV Institute,Faculty of Health Sciencesand Chairperson, Board of the South African Health Products Regulatory Authority.
Glenda Gray, president and CEO, SAMRC.
Aslam Dasoo, Progressive Health Forum.
Mike Sathekge, professor and head of the Nuclear Medicine Department, University of Pretoria and Steve Biko Academic Hospital.
Angelique Coetzee, chairperson, South African Medical Association
Priya Soma-Pillay, head of department, Obstetrics and Gynaecology, University of Pretoria and Steve Biko Academic Hospital, president of The College of Obstetricians and Gynaecologists of South Africa.
Yasmin Adam, head of the Department of Obstetrics and Gynaecology, Chris Hani Baragwanath Academic Hospital, University of the Witwatersrand.
Lee Fairlie is director of Wits Reproductive Health and HIV Institute.
The limits of “lawfare” as a political tool
- Julian Brown
Covid-19 in South Africa shows the limits of using courts to fight political battles.
The Covid-19 pandemic has changed many aspects of our daily lives. Some of these changes are immediately visible in the everyday wearing of face masks, in the bottles of hand sanitiser found on shop counters, and in the careful spacing of long queues. Others, though, are less obvious. They take place in the structures of the legal system that shapes our relationships to one another and to the state.
In the recent past, as I’ve argued in my book, South Africa’s Insurgent Citizens the post-apartheid constitution’s emphasis on the need for state action to be both rational (in the legal sense) and grounded in the fundamentals of the Bill of Rights, has meant that the law and legal activism have become political tools. These tools have often been used by poor communities and civil society bodies to pursue their goals. Attempts such as these to pursue political ends through legal means have been described as “lawfare”, and have become common in South Africa.
In the current pandemic, this history of “lawfare” has inspired a new series of legal challenges to the new legal rules and structures that govern the country.
The mechanism through which these new rules are implemented is the Disaster Management Act of 2002. This Act enables the President and the executive to declare a national state of disaster and – so long as the disaster persists – to bypass some of the legal constraints ordinarily placed on the exercise of government powers.
The Act gives the President the power to govern by making regulations that then have legal and binding force on the nation. The President can do so without following the slow processes of passing new legislation.
On 15 March 2020, following the President’s lead, the Minister of Cooperative Government and Traditional Affairs declared such a state of disaster and, shortly afterwards, published the first of several sets of regulations. These regulations established the framework within which South Africa has since been governed.
They were almost immediately challenged in the country’s courts.
These challenges took several forms. Some of the first cases disputed the legality of the initial declaration, while others questioned specific aspects of the new regulations – such as the decision to ban the sale of alcohol, or the sale of tobacco.
I wrote about these challenges in a recent paper in the South African Journal on Human Rights, and considered what the successes and failures of these cases might mean for civil society politics during the Covid-19 pandemic. In essence, I argued that the relative failure of these cases has shown the limits of “lawfare” as a political strategy in the context of a widely-recognised disaster. In a time of uncertainty, the courts are more likely to give the executive branch of the state more discretion, reducing the possibility of public oversight of its actions.
Covid-19 response and lawfare
In the first six months after the declaration of a state of disaster, a wide range of civil society organisations and political parties challenged the legality of the declaration itself, of the regulations that governed trade, and human movement through curfews and restrictions on national travel.
Although some of these challenges achieved limited success in the courts, the majority failed. The courts proved themselves reluctant to interfere in the exercise of the executive’s power to promulgate and enforce regulations in terms of the Act. In doing so, the courts tacitly accepted that standards of judicial oversight that mark the separation of powers in ordinary times might not be appropriate during the exceptional circumstances of a state of disaster.
It is tempting to explain at least part of this trend by reference to the inept way in which some of the early challenges were argued. The very first case, for example, argued that the state of disaster should not have been declared because
Covid-19 … cannot be harmful to Africans.
But comparable statements were also made in another case - De Beer v Minister of Cooperative Affairs that was partially successful. In this case, the “Liberty Fighters Network”, a relatively-unknown civil society organisation, argued that the President should not have declared a state of disaster to respond to Covid-19 because a number of other serious diseases were already endemic in South Africa.
The successes and failures of this case – and other cases – revolved around the standard of legal rationality that could be required of the government. The applicants were successful because the judge held that each of the specific regulations had to be justified as ‘rational’ – and that he could therefore strike down isolated aspects of the regulations piecemeal.
But in the majority of the other cases the executive was held to a different standard: most other judges were reluctant to pick apart the threads of the regulations to determine the individual rationality of each one. Instead, they held that the regulations ought to be examined as a whole. If the entire scheme was rationally connected to the purpose of containing and managing the Covid-19 disaster, then the regulations would withstand scrutiny as a whole.
The limits of lawfare
Although the De Beer judgment received a great deal of press attention at the time, the standard it applied did not persist. It is the other standard – of overall rather than specific rationality – that went on the shape the jurisprudence. And it is the regular use of this standard that best explains the failures of pandemic “lawfare”.
It is obvious that it is much harder to argue that the entire fabric of the regulations is wholly irrational than it is to argue that a specific thread within that fabric – the decision to ban the sale of alcohol, for example – should not have been taken.
It is thus unsurprising that the prospects of “lawfare” by civil society organisations during the first six months of the disaster were bleak. And in the almost 18 months since, little has happened to change that assessment.
Indeed, the willingness of the executive to pre-empt criticism by amending the regulations has arguably strengthened its position. The overall rationality of the links between the regulations, their amendment, and the changing events of the pandemic seems clear – even if a court might be persuaded to doubt the logic of a specific ban or requirement. The regulations are almost immune to challenge.
Overall, this has meant a reduction in the effectiveness of civil society politics. Even as many of the physical spaces in which public gatherings and activism could take place were being closed, the grounds on which organisations could challenge the legal regimes under which South Africa is governed were being steadily narrowed.
I do not know how this will affect the ways in which politics will continue to develop once the pandemic ends. But I think it is fair to suggest that the past two years have shown the limits of “lawfare” as a political tool in this context.
- Herkulaas MvE Combrink, Benjamin T H Smart, Scott Hazelhurst and Vukosi Marivate
Covid-19: Scientists without quality data are like unarmed soldiers in a war zone.
Some of the most important lessons for public health from the COVID pandemic are about how the government should share data with the public, how updates about responses should be clearly articulated, and how important the sharing of the insight, the information, and the full relevant data are to the public.
The pandemic brought these issues into focus. But the challenge extends beyond the boundaries of COVID-19 to all diseases.
Mistakes made during the pandemic when it came to the collection, management and distribution of data must be recognised. And lessons must be learned and shared about efficiently navigating public health data.
We looked at the effectiveness of lockdown in South Africa and how data were used during the pandemic. We concluded that data collection and dissemination could have been much more efficient. And that if it had been it would have determined better outcomes.
For example, if more detailed, localised data had been publicly available throughout the country it would have been possible to quantify and contrast the spread of the disease between cities, towns and rural areas. In turn, this would have meant that those making policy decisions were better informed.
Our analysis and findings underscored that quality data is the cornerstone of good science. Without it, scientists given the job of informing the public about vital public health issues are like unarmed soldiers in a war zone.
We cannot emphasise enough the importance of epidemiological data, and how relevant it is in managing the early stages of a disease outbreak. However, as a disease progresses, so too must the underlying data and reporting improve to manage the progression of the outbreak.
About more than just data
Sharing information is not just about sharing any data with the public.
Take the issue of aggregate reporting. Limited inferences can perpetuate public bias. Aggregate reporting presents data in a way that illustrates a cumulative number or a time series progression of the total sum of data. These World Health Organisation graphs are a good example of both good and bad practice. Good because data are shared, bad because only one variable perspective is shared at a time.
Another challenge is that underlying data aren’t made available for other scientists to use easily. So even though comprehensive and well presented epidemiological reports are released by South Africa’s National Institute of Communicable Disease (NICD) and it now has a very usable dashboard, the underlying data are not available for any other visualisations or analyses by others.
A further problem with aggregate reporting is that it abstracts the nuances and public healthcare interventions and changes over time. This includes things like modification in patient follow-up guidelines, introduction of a new treatment regimen (as was the case with HIV/TB) and innovative clinical surveillance strategies.
Members of the public need to have comparisons of the state of the current outbreak in relation to previous outbreaks of a similar nature. This would be contextually relevant and can help people to assess the insight as well as the data and move toward evidence-based decision making.
The time frames can be adjusted from these dashboards. But the way the data are presented means that it’s hard to contextually compare different infectious disease surges (or clusters of outbreaks of a specific disease) and the impact on the healthcare system.
Reflecting changing realities
Disease outbreaks aren’t static. A disease can lose epidemic-status and become endemic, as it becomes a constant and more predictable presence at a particular location. For example, both the contagiousness and harmfulness of a disease can change as a result of an actual intervention, such as an effective vaccine or effective non-pharmaceutical interventions.
In the initial stages of an outbreak, three primary data points are useful to everyone and should be shared routinely: time, place, and number.
Typically, after any outbreak, government or health authorities take steps to share basic data and infographics with the public that purport to justify any interventions they may recommend.
This was the case during COVID.
But we identified some immediate problems with this approach.
Firstly, much of the information is released only in formats like infographics that are not computer readable. This makes further analysis impossible without research groups and members of society manually transcribing, collecting, and sharing data. This causes a trust issue with the data: there might be multiple sources of the same information and the process is error-prone.
Secondly, data shared over time and subsequent visualisations became less frequent (in the case of data sharing) and remained aggregate (in the case of dashboards and infographics). An unfortunate consequence was that there wasn’t transparency or a clear correlation between the underlying evidence and decisions being taken.
So how can public health decision making stop being treated like a state secret? Aren’t there simply ways for the required data to be openly shared, and platforms created that enable engagement with the numbers?
We think it is indeed possible.
The way forward
Disaggregated data. In a country with inequities such as South Africa, aggregated data can hide disproportionate effects of an event on specific communities. Making the raw disaggregated data available can enable evidence-based advocacy and interventions to meet the needs of marginalised communities more effectively.
Accessible data. Information should be shared with the inclusion of indices, metrics, and simplified computer readable data types. This would allow wider use and add a layer of transparency. It would also create an opportunity for community-led monitoring and evaluation outside the government.
Choosing appropriate visualisations. We strongly recommend representing the data as a relative number (in other words such as percentages or per population size) in addition to absolute numbers. This would make it more accessible. Ordinary citizens would be able to understand better where things stand and how they are changing. It would also help inform changes they may choose to implement to keep themselves safe.
Also, previous outbreaks of a similar or the same pathogen should also be displayed. This would enable people to contextually assess the similarities and differences at a glance. Here’s a good example.
Flaws to overcome
COVID-19 exposed the fragmented way in which data is released, and how insufficient data sharing can be if it’s not done at a local area level.
In some instances, data quality issues also compromise the trust the public has in the system. Trust is also affected by the frequency with which data are shared. Inconsistencies in terms of time and date for data sharing seems to be a universal problem. This breeds public distrust.
From COVID-19 we learned that there are multiple opinions around a specific issue. Some of these opinions have been badly informed. But one cannot blame people who are uninformed when important decision-making information is not freely and easily accessible. Without the required supporting information, citizens will continue to make assumptions or believe misinformation and disinformation that are not evidence-based. Their spread may be unavoidable. But the lack of access to quality data is not.
Nompumelelo Mtsweni, data visualisation developer, Elizabeth Cornelia Greyling, strategy manager at Columbus Stainless, and Emmanuel A. Simon, digital strategic consultant, also contributed to this article.
Covid-19 Update 81: Vaccination and testing site now open
- Wits Mvax Operations Team
Apply for reasonable accommodation and upload your international vaccine certificate.
It has been wonderful to see staff and students returning to our campuses this week, as registration commenced. It has been especially gratifying to learn that to date over 16 700 staff and students (about a third of the Wits community), have uploaded their vaccination certificates via the Wits MVax Upload portal. Thank you! It is anticipated that this number is likely to increase given that staff and students have until 1 March 2022 to upload their certificates.
Upload WHO-approved International Vaccination Certificates
We are pleased to announce that all World Health Organization-approved international vaccination certificates can now be uploaded. Read more about how to do this on the Wits MVax Implementation Portal.
How to Apply for Reasonable Accommodation
Wits staff and students may apply for Reasonable Accommodation if they cannot be vaccinated on medical grounds or may elect not to be vaccinated on Constitutional grounds through the exercise of their rights to privacy, bodily integrity, freedom of religion, freedom of belief and/or freedom of opinion. It is noted that these rights are not absolute and may be limited to give effect to the Wits Vaccination Policy. The granting of Reasonable Accommodation is not automatic, and any decision will be based on the University’s policies and procedures, return to campus plans, risk assessments, and operational requirements, amongst others. Persons granted Reasonable Accommodation will have to agree to and abide by additional Covid-19 safety protocols and limitations. Click here to Apply for Reasonable Accommodation. The portal to apply is now open.
Wits COVID-19 Vaccination and Testing Site opens 1 February 2022
The Wits COVID-19 Vaccination and Testing Site opens tomorrow, 1 February 2022 in the Wits Multipurpose Sports Hall on the Braamfontein East Campus (next to the swimming pool). It will run from 08:00 – 15:00 on weekdays and will include a Vaccination Help Desk. You do not need to make a booking – just walk in with your identity document or passport and get vaccinated. Services include free vaccinations including boosters, COVID-19 antigen tests and a Help Desk. All staff, students, alumni, contractors, family members and household persons are welcome as walk-in patients. No bookings are needed.
We thank you for walking this journey with us and look forward to welcoming you back to campus soon.
Covid-19: New tracker for shopping malls
- Wits Enterprise
Wits team develops social distancing and shopper behaviour tracker for malls.
Wits University innovators have developed a novel Wi-Fi-based solution for managing and monitoring foot count, social distancing and consumer behaviour in shopping malls. The solution uses Artificial Intelligence (AI) to allow retail managers to make future predictions, improve security and deliver intelligence to stores about shopper behaviour.
Its inventor, Dominique Adams has been awarded R100 000 worth of support from Wits Enterprise towards developing the business so as to take the innovation to the next stage. This award was for the winning pitch of the latest Prospector@Wits course run by Wits Enterprise. Development of the Wi-Fi-based, AI-enabled solution began in 2020, shortly after the Covid-19 pandemic emerged in South Africa, triggering the concept for the social distancing tracking tool.
Adams explains; “Our innovation stemmed from an existing product for Wi-Fi signals to monitor social distancing in public spaces. We engaged with stakeholders in the retail space to determine whether there was a need for a solution that, with the application of AI technology, would give them valuable insights into consumer behaviour and help them make predictions.
“Combining Wi-Fi technology with AI, our tool allows mall managers to monitor the complex behaviour of people in real-time as well as predict their future behaviour. This gives stores data-based intelligence while providing mall management teams with an additional tool for enhancing security. Our tool also allows shopping malls to monetize from the deployment of Wi-Fi, and importantly obtain intelligent foot count and other data for strategic planning and evidence-based decision-making.”
As an example, Adams says mall managers can measure the overall popularity of stores and see the length of time a shopper spends at a particular store. The data gathered from these measurements are valuable for establishing shopper behaviour and for informed decision-making and planning.
Adams’ DataConvergance team is developing the solution under the leadership of Professor Bruce Mellado from Wits University’s School of Physics. Mellado is also part of iThemba LABS at the National Research Foundation, and leads the Technology Innovation Platform in Artificial Intelligence, which is a collaboration between Wits and iThemba LABS.
The team, consisting of data scientists and AI specialists, includes Xifeng Ruan, Kentaro Hyashi, Finn Stevenson and Benjamin Lieberman.
In developing the tool from scratch, they had to learn how to harness the large amount of data available from Wi-Fi systems and solve challenges around Wi-Fi signals bouncing off walls, the distortion of positioning of people and the complexity of terrains. In adapting the tool for shopping mall application, Adams recalls the biggest challenge being the reluctance of mall managers to assist with the market and needs analysis.
“It has been a huge team effort. Being awarded the seed funding is a huge achievement for me as well as our team, a great reward for all the long hours spent. The knowledge gained through the Prospector@Wits course and the valuable guidance from my mentor, Dineo Masokoane, were critical contributions to the successful outcome of the project proposal.”
Commenting on the solution’s potential, Mellado says: “Given the small number of businesses contemplating or already adopting AI, there is a huge opportunity for this solution to be successful in the retail environment. If the solution is successfully implemented, DataConvergence could be a trailblazer in the deployment of AI in the retail sector.”
Ela Romanowska, Director of Innovation Support at WITS Enterprise says that this is another example of Wits University’s response to providing solutions to societal needs, and is a worthy winner of the Prospector@Wits end of course pitch session.
Dineo Masokoane, Innovation Support Manager at Wits Enterprise, says: “The solution will enhance data collection by exploiting and deriving greater benefits from the Wi-Fi availability in malls. This approach enlarges the scope of information available to management and planners to monetise their investment in Wi-Fi as well as optimise in-store strategy development.”
The next steps for Adams and his team are to refine the prototype for the retail environment and develop a pilot in a real retail environment before full- and large-scale deployment in shopping malls.
The inside story of discovering the Omicron variant
- The Conversation Weekly podcast
The Conversation Weekly podcast: What South African scientists' experience offers the world about future variants.
What is it like to discover a new coronavirus variant? In this episode of The Conversation Weekly podcast, we hear the inside story from one of the South African scientists who first alerted the world to the omicron variant. And a South African vaccine expert explains what lessons the country’s experience can offer the rest of the world about future variants. We’re joined by Ozayr Patel, digital editor for The Conversation based in Johannesburg for this story.
Plus, new research finds a person’s emotional reaction to music has a lot to do with their cultural background – we speak to the musicologist behind it.
It was nine o'clock on a Friday evening in late November 2021 when Jinal Bhiman and her colleagues at the National Institute for Communicable Diseases first saw the sequencing data for the omicron variant. “We hadn’t seen those many mutations before,” says Bhiman, a principal medical scientist at the institute. The sequencing data came from a small group of eight samples from South Africa’s Gauteng province where an unusual cluster of cases had been spotted.
Over the following week, scientists across South Africa’s network for genomics surveillance swung into action to sequence more samples, before Bhiman and her colleagues alerted the South African government to their discovery. “Things exploded from that week on,” says Bhiman.
The World Health Organization quickly classified the discovery as a variant of concern and called it omicron. As countries around the world began closing their borders to travellers from southern Africa, Bhiman and some of her colleagues received death threats. “That was really scary,” she remembers. Scientists were targeted because of the travel bans. “They felt that scientists shouldn’t be raising the alarm – that this is not benefiting us in any way,” she says. Bhiman believes that the travel bans were irrational, because of the speed at which the variant moved around the world.
Shabir Madhi, Professor of vaccinology at the University of Witwatersrand, is a vaccine expert who’s worked on a couple of South Africa’s COVID-19 vaccine trials. He recalls that when he first saw the sequencing data on omicron, he was “fairly optimistic” that the immunity built up by vaccines and past waves of infections would protect against severe disease. And he was right. “We’ve seen a dramatic decoupling of infections, hospitalisations and death,” says Madhi.
But Madhi criticises the scepticism scientists in the northern hemisphere had about the early omicron data coming out of South Africa. “It’s a manifestation of cultural imperialism, where we will not believe anyone else unless we show the same first,” he says. He believes South Africa’s experience can offer lessons to scientists in other countries who may discover another coronavirus variant, particularly when it comes to travel bans. “I think the global community needs to make a stance that when countries start reporting data, they’re not going to be penalised for it,” he says. Madhi also thinks countries need to be careful about using “computer modelling about the potential effects of the mutations and extrapolating that this is what will happen from a clinical perspective”.
In our second story, we explore whether a person’s emotional response to music and harmony is innate or shaped by culture. George Athanasopoulos, COFUND/Marie Curie junior research fellow at Durham University in the UK, travelled to a remote region of northwestern Pakistan to spend time with the Kalash and Kho people who live there. His research is revealing that music considered “happy” to western listeners, for example in a major key, isn’t necessarily perceived that way by others. “After hours and hours of experimenting with the two tribes in northwest Pakistan,” he explains. “We found that actually for them, it’s the minor chord which conveys happiness.” (Listen from 34m15s.)
And Laura Hood, politics editor for The Conversation based in London, recommends some expert analysis on the political pressures facing the British prime minister, Boris Johnson, over parties held during the lockdowns. (Listen from 47m10s)
This episode of The Conversation Weekly was produced by Mend Mariwany and Gemma Ware, with sound design by Eloise Stevens. Our theme music is by Neeta Sarl. You can find us on Twitter @TC_Audio, on Instagram at theconversationdotcom or via email. You can also sign up to The Conversation’s free daily email here.
You can listen to The Conversation Weekly via any of the apps listed above, download it directly via our RSS feed, or find out how else to listen here.
Covid-19 Update 82: Changes to isolation protocols and FAQs
- Wits MVax Operations Team
The South African government released new Covid-19 regulations as at 31 January 2022, pertaining to changes to isolation protocols.
Below are four scenarios regarding whether you should come to campus or not following a positive Covid test, if you have symptoms, or come in close contact with a positive Covid-19 case.
What to do if…
You test positive for Covid-19 (PCR or antigen test) with NO symptoms
You test positive for Covid-19 (PCR or antigen test) AND you have symptoms
You develop symptoms of Covid-19
You have been in close contact with someone who has tested positive for Covid-19
If you test positive and do not have symptoms then you do not need to isolate and you can come to campus. Continue to follow the standard Covid-19 protocols: 1M+2V+3Ss – Wear a Mask; stay in well-Ventilated areas; Vaccinate; Complete the Covid-19 Screening tool; maintain a Social distance of 1.5m; and Sanitise hands often.
If you test positive and show symptoms, you need to isolate for seven days. Do not come to campus. Return to campus after seven days with a sick note as required by Faculty/Line Manager. If you have moderate or severe Covid-19 illness, please submit a medical certificate to anna.moloi@wits.ac.za in order to return to campus.
If you have symptoms of Covid-19, please do not come to campus. You do not have to isolate, but monitor your symptoms and seek medical advice as needed. You may return to campus when you have recovered, with a sick note as required by Faculty/Line Manager.
If you have been in close contact with someone who tests positive for Covid-19 and you do not have symptoms then you need not isolate and you can come to campus. Continue to monitor yourself for symptoms and follow the routine Covid-19 protocols 1M+2V+3Ss in (1.) above.
More than 20 000 staff and students have uploaded their vaccination certificates to the MVax Upload and RA Portalsince the process opened in January. Please view the Frequently Asked Questionsabout the process and the procedure until 1 March 2022, the date by which all Witsies must vaccinate or have applied for reasonable accommodation. Visit Wits Vaccination Policy Implementation to learn more.
LogBox App is being streamlined to make it easier for you to complete the questions.
We would like to thank all members of the Wits community who have uploaded their vaccine certificates to the COVID-19 MVax portal. More than 22 000 certificates have already been uploaded and the numbers are increasing daily. Thank you!
The Wits Vaccination and Testing Site in the Wits Sports Multipurpose Hall (located on the Braamfontein East Campus next to the swimming pool) is also very busy – thanks to all who are vaccinating! Open Monday to Friday, 08:00-15:00. There is also the MVAX Helpdesk.
This is a reminder that it still remains a regulatory requirement for every person to be screened before entering any Wits campus. This is done by completing the daily screening tool via the LogBox Mobile App or the SMS-USSD service. To expedite access to Wits’ campuses, only visitors will have their daily Screening Tool checked at the entrance (including contractors, service providers and suppliers).
All persons with a Wits access card who wish to enter our campuses must complete the daily screening before arriving at the entrance. The LogBox App is being streamlined to make it easier for you to complete the questions in under 15 seconds. We urge you to complete the screening tool before you arrive at Wits. Spot checks for staff and students may be conducted from time to time, or at the entry to a specific venue.
The Screening Tool result must permit you to enter the campus. If the result is not favourable, please do not come onto campus. If you have symptoms, seek assistance from a healthcare professional. If you test positive for COVID-19 with symptoms, you need to isolate for 7 days. More information in the Wits COVID-19 Handbook.
It is our collective responsibility to protect ourselves, as well members of our community by complying with the above requirements and being considerate of our fellow colleagues, students, and friends.
Covid-19 Update 84: Over 30 000 vaccination certificates uploaded
- Wits MVax Operations Committee
The academic programme began in earnest today and it was fantastic to see students in class again and staff back on campus.
Our objective is to ensure that our community is protected as far as possible from COVID-19, and one way in which to do so is by ensuring that people are vaccinated as quickly as possible.
Thank you to all members of the Wits community who have uploaded their vaccination certificates – we surpassed the 30 000 mark over the weekend (almost 70% of students and about 75% of staff uploaded their certificates). The uploads continue to roll in, as we approach 1 March. Our vaccination site has also been incredibly busy, with hundreds of vaccinations administered every day. We predict that over 500 people will be vaccinated on-site tomorrow.
Members of the Wits community who elect not to vaccinate on Constitutional or medical grounds, must apply for reasonable accommodation via the Wits MVax Portal. Some applications are still being processed at the faculty and other levels, and others are serving before the MVax Appeals Committee. Staff and students who have applied for reasonable accommodation and who are awaiting the outcome of their applications will have access to campus pending the outcome of the applications or appeals process. Reasonable Accommodation does not apply to students and staff living in Wits’ residences.
Everyone is required to complete the revised LogBox COVID-19 screening application every day, which takes only seconds to complete. Campus Protection Officers will conduct spot checks at entrances to ensure that people continue to complete the screening tool.
Continue to abide by Wits’ COVID-19 protocols – wear a mask, stay in well-ventilated areas, vaccinate, complete the LogBox screening form on the app, keep a social distance of at least 1,5 metres and sanitise regularly.
South Africa has arrived at the recovery stage of the pandemic
- Shabir A. Madhi
South Africa is in a new phase of the COVID pandemic. But vaccination remains crucial.
A recently published South African study set out to determine sero-positivity against SARS-CoV-2 before the fourth wave of COVID-19, in which the omicron variant was dominant. Sero-positivity measures the presence of antibodies against the virus; it indicates past infection. The study focused on Gauteng, the country’s economic hub. Ozayr Patel asked Shabir Madhi to unpack the results and explain why the findings suggest that South Africa has reached a turning point in the pandemic.
What we found
The results show the levels of sero-positivity – in other words what percentage of people have antibodies to the virus – among just over 7,000 people from whom samples were taken. From these results the following rates were calculated:
In those under 12 years of age, none of who received a COVID-19 vaccine, 56% showed presence of antibodies to SARS-CoV-2
In those over 50 it was 80%, including 70% if unvaccinated and 93% if vaccinated
In high density inner city areas the sero-positivity prevalence was 85%
Using the seroprevalence data, together with COVID-19 attributable deaths using excess mortality data from the South African Medical Research Council, the study was also able to impute the risk of dying following infection by SARS-CoV-2 prior to the Omicron wave in South Africa. This infection fatality risk for COVID-19 was 0.57% pre-omicron in Gauteng. This is substantially higher than 0.019% imputed for seasonal flu, which infected one-third of the population each year pre-COVID, calculated using similar methods.
Vaccination coverage: We discovered high levels of hybrid immunity: that is immunity gained from a combination of previous infections plus vaccinations.
At the time of the onset of the omicron wave, 36% of people in Gauteng had at least one dose of the vaccine. This was higher – 61% – in those over the age of 50. (This cohort was responsible for more than 80% of deaths pre-omicron.)
Based on sero-survey, 70% of vaccinated people were also infected pre-omicron. Hence they would have had substantial hybrid immunity, which has been shown to induce a broader repertoire of immune responses against the virus. Such hybrid immunity in South Africa has, however, come at the cost of loss of 300,000 lives based on South African Medical Research Council excess mortality estimates. These are three-fold higher than the official recorded number of deaths.
Based on another study, the hybrid immunity is expected to confer greater protection against infection and mild COVID-19 compared with immunity only from vaccine or natural infection.
Hospitalisations and death rates: Our study also analysed the temporal trends in COVID-19 cases, hospitalisations and deaths (recorded and COVID attributable from excess mortality) from the start of the pandemic up until the tail end of the Omicron wave. The study found a massive decoupling between the number of people becoming infected with the virus relative to COVID hospitalisation and death rates during the course of omicron compared with earlier waves. This was true across all adult age groups.
The omicron wave was associated with 10% of all hospitalisations since the start of the pandemic, whereas 44% of hospitalisations had transpired during the course of the Delta variant wave. More impressively, only 3% of COVID deaths since the start of the pandemic occurred during the omicron wave, compared with 50% during the delta dominant wave.
The findings of decoupling of infections and severe or fatal COVID-19 were similar in the 50-59 year age group. In this group the omicron wave contributed to 15% of recorded COVID hospitalisations and 2% of deaths since the start of pandemic. This compares with 46% of hospitalisations and 53% of deaths occurring in the third wave, dominated by delta. The data for people over 60 years old was similar.
The survey also found that 58% of children under 12 years of age (all unvaccinated) were sero-positive. They were not more heavily affected during the Omicron wave.
The delta dominant wave which was the most severe in South Africa, coincided with South Africa’s belated COVID vaccine rollout. The high death rate during that wave is an indictment of the missed opportunities that could have prevented a large percentage of the deaths which transpired. In particular, the delayed procurement and roll out of COVID-19 vaccines in South Africa, as well as the ill-informed decision to against the WHO recommendation on the continued use of the AstraZeneca vaccine which was available to in South Africa when the Beta variant was circulating in South Africa.
In summary, the omicron wave contributed to less than 5% of all COVID-19 deaths in Gauteng. Since the start of the pandemic, the delta variant wave contributed to 50% of all of the deaths. The balance is split roughly equally between the first and second waves caused by ancestry and the beta variant.
Our findings also show that natural infection has been high and is playing a major role in how the pandemic has unfolded especially in countries with low to moderate COVID-19 rollout. These high levels of infections have, however, resulted in a massive loss of lives; which to date is likely under-estimated in low and middle income countries as shown from the South African data.
What the findings tell us
The findings indicate that South Africa is moving into the convalescent phase of the COVID pandemic – the recovery phase. This is likely to be the same in other countries with low or modest vaccine uptake, but high force of past infections. As such, South Africa needs to recaliberate its approach to the pandemic and to start managing it as we would do for other respiratory infections which too cause large number of hospitalisations and deaths.
There are still a few unknowns. Another resurgence is likely, and there might well be another variant. But it would be very surprising if further variants are able to evade the T-cell arm of the immune system which is stimulated by vaccines and natural infection. The T-cell (cell mediated immunity) arm of the immune system, appears to be the main mediator of protecting against severe COVID-19, even when there are breakthrough infections in vaccinated people or reinfections.
So why do I believe that we are at the tail end of this pandemic? It depends what metric you use. If it’s about infections, we’re not at the tail end. If it’s about the number of deaths that will transpire from COVID-19 during 2022, relative to the number of deaths that will transpire from other preventable causes of death in countries such as South Africa, then I believe the country has pretty much arrived towards the end of this pandemic.
In South Africa about 10,000 to 11,000 people die of seasonal influenza every year. In 2019 tuberculosis killed 58 000 in 2019. But we are not declaring an emergency in South Africa to deal with flu or tuberculosis. Deaths from HIV, and complications from HIV, are about 70,000. But South Africa isn’t shutting down the country to prevent deaths and infections from these diseases.
Now what?
Only 12% of people across the continent have received one dose of vaccination. The implications of our findings are that:
Vaccine coverage must be enhanced by ensuring that adequate booster doses are given to those who require it. We might need to continue boosting. This might need to be on an annual basis for the next two to three years, especially for high risk individuals. The time line for this is until we have more experience on the durability of protection of vaccines, particularly in settings with a high prevalence of hybrid immunity (where protection may be even longer lasting. )
Campaigns should be focused primarily on high risk groups, including getting over 90% of people over 50 years of age vaccinated before the next resurgence anticipated. This should be the focus rather than the current arbitrary target of vaccinating 40%-70% of the population.
It’s still beneficial to expand vaccinations in settings with high sero-positivity. Studies on hybrid immunity show this delivers more robust and broader repertoire immune responses that could heighten protection against infection, and reduce the magnitude of future resurgences.
It’s also important that key non-pharmacuetical interventions are kept in place. This includes wearing masks in crowded poorly ventilated indoor places, and particularly high risk individuals when there is an increase in virus transmission activity.
Our findings support the optimism expressed at the beginning of 2022 in South Africa that a turning point had been reached in the pandemic. Many in high income countries dismissed this view as not applicable to their settings despite high vaccine coverage. But their experience has since generally aligned with South Africa’s.
Lastly, better COVID vaccines are required. But the world is no longer at “code red”. And it’s time to rebuild livelihoods, economies and all other facets of life that were affected over the past two years. This is particularly true in fragile low and middle income countries.
Shabir A. Madhi, Dean Faculty of Health Sciences and Professor of Vaccinology at University of the Witwatersrand; and Director of the SAMRC Vaccines and Infectious Diseases Analytics Research Unit, University of the Witwatersrand. This article is republished from The Conversation under a Creative Commons license. Read the original article.
Omicron doesn’t need its own custom vaccine
- Simone Richardson and Penny Moore
The Omicron variant of the SARS-CoV-2 virus was discovered in South Africa and emerged in November 2021.
Scientists have already learned a lot about Omicron. One of the key questions that remains is how well our immune systems deal with infection by this variant.
This is important for two reasons. Firstly, Omicron is highly infectious and has swept across the world. Thus, many people have been exposed to Omicron and we need to define how well such people are protected from future re-infections by emerging variants.
Secondly, several vaccine manufacturers have started to incorporate Omicron into their vaccines. Understanding how well our immune system responds to Omicron will tell us how well such vaccines might work.
Our latest study begins to answer these questions. But first, let’s review what’s known.
Omicron and the immune system
Omicron bears more than 30 mutations in the spike protein – more than any other variant of the virus previously described. Many of these mutations are in parts of the spike that are immune “hot-spots”. These are the parts that antibodies most frequently recognise. Antibodies are the infection-blocking proteins that the body makes when triggered by vaccines or previous infection.
These neutralising antibodies, which prevent infection if present at high enough levels, are 20-fold less effective against Omicron compared to the ancestral SARS-CoV-2 variant. This has translated into much lower protection rates from symptomatic infection caused by Omicron after two vaccinations. Twice vaccinated people are only 20% less likely than unvaccinated people to become infected with Omicron, which is why we have seen Omicron infections even in people who have received a COVID-19 vaccine.
The good news is that this protection is rescued by three vaccine doses (to 60-75% protection). This means you are 70% less likely to become infected by Omicron if you have received three doses of the vaccine, compared to unvaccinated people.
However, vaccines work in multiple ways. Protection from infection is just one aspect, and actually, many scientists feel it’s not realistic to expect that COVID-19 vaccines can completely prevent infection. To do this would require that high antibody levels are maintained for long periods of time, but in reality antibody levels wane.
Crucially, the vaccines we already have, after even two doses, do a very good job at protecting us from severe disease caused by Omicron (providing 70% less chance you will become severely ill if you catch Omicron).
This continued effectiveness against hospitalisation has largely been attributed to a second arm of the immune system, called T cells. T cells are much less focused on the “hot-spots” favoured by neutralising antibodies. They recognise many more parts of the spike, beyond those mutated in Omicron or any other variant.
Also, antibodies don’t just neutralise viruses – they can destroy already infected cells. They can do this with all variants, and it may play a role in preventing severe disease.
Omicron and hybrid immunity
In the first part of our study, we asked how strong people’s immune response was to Omicron infection after previous vaccination, termed a “breakthrough infection”. We found that infection following vaccination results in an extremely strong neutralising antibody response, regardless of which vaccine you received. This is because the vaccine has primed your immune system to be ready to respond to a second exposure, in this case through infection. These high antibody levels mean that your chance of being reinfected, after a breakthrough infection, is likely lower.
In contrast, people infected with Omicron who had not previously been vaccinated make excellent neutralising antibodies against Omicron itself. However, when we test these antibodies against other variants of concern such as Beta, Delta and the ancestral virus, these Omicron-triggered antibodies show substantially reduced activity. Thus, these antibodies are good at recognising the variant that triggered them, but less good at recognising other variants.
This study and our previous data indicate that people who have been vaccinated and suffered breakthrough infections have excellent antibodies and are likely protected from future infection until these antibodies wane.
We have previously shown that the reverse is also true: people vaccinated after infection also show extremely good antibodies.
In South Africa, where as many as 70-80% of people have been infected, and 40% vaccinated, it is likely that many people now have this “hybrid immunity”. This will likely translate into future variants showing reduced ability to cause severe disease.
The bottom line? Vaccination is a great way to make sure your immune system can fight new variants.
Variant-specific vaccines
These data are also key to telling us whether future vaccines need to be adjusted to match Omicron. The risk of this strategy is potentially endless “variant-chasing”, which would require us to update our vaccines constantly.
Our study shows that Omicron is highly immunogenic, but that it triggers neutralising antibodies that preferentially recognise parts of the spike specific to Omicron. These antibodies may not provide particularly good protection against emerging variants, with no guarantee that these future variants will evolve from Omicron.
This also means that new vaccines based on Omicron may not be better than those we already have. That’s a finding supported by early pre-clinical data from Omicron-based vaccines in a study in a study from the US.
Ultimately, rather than focusing on new variant-specific vaccines, the emphasis should continue to be firmly on deploying existing vaccines as fast as possible to as many people as we are able to reach.
New Covid-19 regulations are the real state of disaster
- Scientists Collective
The incoherent and illogical new government Covid-19 regulations are the real state of disaster
These draft regulations are seemingly an ill-conceived and misdirected attempt to continue preventing SARS-CoV-2 infections and appear to be oblivious to the new realities of Covid-19, two years into a pandemic.
Despite the low coverage of Covid-19 vaccinations in South Africa and failure to vaccinate the targeted 40 million people (or administer 40 million doses of vaccine) by the end of 2021, there has been evolution of widespread population immunity and resultant protection, particularly against severe Covid-19 and death in South Africa.
Even before the Omicron-driven fourth wave that started in late November 2021, up to 70% of the population had been infected at least once, which has since likely increased to >80% after the fourth wave due to Omicron’s high transmissibility.
The high force of SARS-CoV-2 infections in SA, and the 300,000 excess deaths that have been mostly attributed to Covid-19, is indicative of the failure of the government-enforced regulations to prevent significant numbers of infections in South Africa.
These regulations, such as lockdown strategies, limits on gatherings, curfews, social distancing and mask mandates, at best drew out the initial period over which roughly the same number of infections would have occurred.
These regulations may have assisted in relieving the pressure on healthcare facilities when the population was generally not immune. However, large scale immunity from those surviving infection and moderate vaccine coverage will probably continue to contribute to the decoupling of cases from severe disease and death seen during the Omicron wave in future waves.
Consequently, it is not conducive for economic recovery and inappropriate to continue pursuing policies and imposing regulations aimed at trying to prevent SARS-CoV-2 infections, as opposed to primarily focusing on enhancing population immunity through vaccination to prevent severe disease and death from Covid-19.
An update and review of the current regulations are certainly critical at this time, when the landscape has changed in relation to the risk to the integrity of the health service from Covid-19 and given the increasing need to balance public health measures, the new reality of high levels of immunity, and regulations that have limited civil liberties, restricted movement and challenged the economy.
What was hoped for was a mature, thoughtful set of regulations that considered these new realities. What was published, however, was an inconsistent, incoherent and illogical set of draft regulations firmly rooted in 2020 when knowledge about Covid-19 was more rudimentary.
The first thing to appreciate is the context of these regulations.
Until now, the regulations governing the Covid-19 restrictions have stemmed from the Disaster Management Act, the powers for which kicked in when the state of disaster was declared in early 2020. The government has recently announced that it at least intends to end the state of disaster. However, in the government’s view, new regulations are required to be promulgated via other acts (largely, but not exclusively, the National Health Act), so that Covid-19 restrictions can be continued in some form when the state of disaster ends.
One big challenge with the draft regulations is that they mostly appear to be written in a general way that would apply to all notifiable medical conditions(NMCs) and not just Covid-19. Perhaps that will be amended, but regardless, it’s worth remembering that the intention behind these draft regulations was to accommodate Covid-19. This makes many of the details even more baffling.
Four sets of draft regulations were released for public comment on 15March. A thorough review of these is beyond the scope of an article like this, but we do feel strongly that they contain several large conceptual errors that are worth pointing out. For instance:
The regulations contain numerous mentions of quarantining. But the reason for this is unclear, as quarantine following a contact with a case of Covid-19 is no longer a requirement in South Africa. And rightfully so, as some of us have pointed out previously.
The regulations list criteria for self-isolation that are unrealistic and untenable in the context of most of the South African population.
Stipulating that persons wishing to self-isolate or self-quarantine, must “have access to the internet and a phone that allows the daily reporting of symptoms” and must “have access to a private physician” is ludicrous and not a reality for most people in South Africa, nor is the requirement that the facility for self-isolation/quarantine “must be a separate well-ventilated bedroom with bathroom and toilet”.
The writers of these regulations seem to remain out of touch with the realities of the daily lives of the South African population.
The regulations strengthen the ability of the government to mandate “prophylaxis, treatment, isolation and quarantine”. There is less recourse for patients to refuse any of these than previously. Yet, apart from the other problems with isolation and quarantine above, the only current “prophylaxis” for Covid-19 is vaccination.
This is not currently mandatory in SA, nor is it proven to alter the natural history of a recent contact or acute case of Covid-19 if given directly after a high-risk contact or during the incubation period of the infection.
The draft guidelines contain an entire section on establishing a national database for contact tracing. The fact that the government continues to believe that contact tracing for Covid-19 is a viable and realistic option, when fewer than 10% of infections are ever diagnosed, shows that their thinking is firmly rooted in 2020. The reasons for this have been outlined elsewhere.
Many of the general measures to contain the spread of NMCs that can be transmitted through droplets or aerosols, detailed in section 16 of the above regulations, lack logic or ability to enforce.
“No person may be allowed to use any form of public transport… if they do not wear a mask.” A fair objective, but it lacks enforcement, particularly on trains and taxis. Furthermore, experience with the highly transmissible and infectious Omicron variant indicates that the type of cloth mask most worn by the public (which rarely provides a good seal around the nose and mouth) provides little-to-no protection against being infected and does not meaningfully reduce transmission.
Physical distancing at work and in queues is also detailed in the regulations. But this ignores the fact of aerosol spread of infectious virus particles, which can comfortably exceed distances of the recommended one metre. The notion of physical distancing to reduce risk of infecting others is firmly rooted in an era prior to realising that spread of SARS-CoV-2 is mainly via the airborne route, and most efficient in poorly ventilated indoor spaces irrespective of distancing between people.
Besides which, as pointed out, prevention of infections by SARS-CoV-2 is no longer an attainable objective as it may have seemed two years ago. Adequate ventilation is key to prevent transmission and requires emphasis.
For travellers exiting South Africa, screening is continuously referenced. We know that temperature screening is useless, missing >50% of symptomatic persons and all those who are asymptomatic, and superficial thermal screening is scientifically flawed in detecting fever.
No one is going to volunteer symptoms at the border if the consequence is forced isolation or being forcibly restricted from leaving.
The proposed regulations for people entering South Africa are even worse. Travellers would need proof of full vaccination, or else a recent negative PCR test. There is great value in ensuring that visitors to our country are vaccinated before entry and considerations to achieve this will be welcome – as they would for other communicable diseases such as influenza that are also not currently mandatory. Several other potential restrictions are then listed.
But consider: If a thousand, ten thousand, a hundred thousand or a million people have Covid-19 at any point in time in South Africa, what impact will a handful or even hundreds of cases of Covid-19 coming into the country make on the epidemic in that country? None, particularly as so many people already here who have Covid-19 are transmitting whilst asymptomatic.
Furthermore, PCR tests aren’t sensitive enough to ensure that travellers who test negative 72 hours before travel won’t be carrying the virus and able to transmit.
If vaccinated passengers do not have to perform a PCR test, but may still be infected, these transmitters will not be stopped at the border. In addition, PCR tests tend to stay positive for weeks or even months after the infectivity is over, leaving travellers trapped trying to enter South Africa.
These half-arsed, pointless and bureaucratic testing rules for travellers entering South Africa are of no benefit, harm tourism, confer huge and unplanned costs on travellers with no health benefits and hurt the economy.
The proposed regulations advise that mandatory quarantine may be required for inbound travellers (even though South Africans in-country who are contacts no longer require quarantine). They further suggest that “a person who wishes to be placed under self-quarantine must submit a written application, 72 hours prior to intended date of entry into the Republic, to the Director-General: Health to obtain approval”. When has this, or would this, ever happen? As well as a spectacular waste of a senior official’s time, by the time they got a reply, the person applying would probably officially have long-Covid!
Most perplexing of all is the proposal that “All unvaccinated travellers will be offered vaccinations”, an intervention that will serve no value in influencing the trajectory of the pandemic in South Africa. As people who think vaccines are important, we love the idea, but why are we forcing all this testing and everything else on people, and THEN vaccinate them at the end? Why not just offer them vaccines before they travel?
The list of inconsistencies and confusing logic goes on throughout the four sets of draft regulations. From emphasis on cleaning and disinfection of public spaces – knowledge has moved on, i.e. the contribution of fomites from surfaces is negligible – to again regulating for mandatory prophylaxis (relevant to some other NMCs), which, apart from vaccination, does not currently exist.
There is another issue worth considering too, and that is whether Covid-19 should be a notifiable medical condition at all, as it currently is. According to the National Institute for Communicable Diseases, an NMC is a condition – most of them communicable – of public health importance.
“Surveillance of NMCs involves the systematic collection, analysis and use of epidemiologic data to provide scientifically proven and accurate information to detect and act against public health threats rapidly.” In other words, it allows timeous detection and response to public health threats in order to prevent disease outbreaks, estimates burden of said NMC and identifies populations at risk, monitors trends and helps direct public health interventions and informs policy decisions.
Most NMCs relate to communicable diseases with epidemic capability or those that are nearing elimination and thus critical to survey and control new cases, such as acute flaccid paralysis caused by poliomyelitis.
On the list of NMCs under the National Health Act, 2003 (Act No. 61 of 2003) and published under Government Notice No. 1434 of 15 December 2017, is “respiratory disease caused by a novel respiratorypathogen”, with the example of Middle Eastern Respiratory Syndrome coronavirus (MERS-CoV), which, like SARS-CoV-2, has epidemic potential. SARS-CoV-2 clearly fell into this category at the time of its recognition in 2020, and adding it to the list of NMCs was undoubtedly the right thing to do at that time.
The problem now, as highlighted above, is that South Africa, like almost every country in the world, has proven itself incapable – through little fault of its own – of undertaking the sort of surveillance, contact tracing, quarantine and isolation of cases that is required for containment of a respiratory spread NMC, to meaningfully alter the course of a pandemic.
Hence, the regulations now out for review will not meaningfully alter the course of the epidemic of Covid-19 in South Africa.
If we accept that current surveillance misses 90% of infections, how is continuing that surveillance going to change public health interventions?
All laboratory confirmed tests for SARS-CoV-2 – be they PCR or rapid antigen test (in future) – can simply be reported to a central database and nationally (as they are now) without being an NMC. It’s simple laboratory reporting. Similarly, wastewater surveillance for SARS-CoV-2, which is a very useful predictor of community transmission levels, does not necessitate Covid-19 being an NMC.
Genomic surveillance continues to be critical in understanding the evolution of the virus and requires ongoing investment and support. Such strategies would continue to allow surveillance of the epidemic in South Africa and optimise efficiencies.
Alternatively, as for influenza, we could move to incorporating SARS-CoV-2 into a sentinel surveillance programme such as is undertaken both in the community (influenza-like illness – ILI) and in hospital (severe acute respiratory illness – SARI) surveillance.
Influenza is not an NMC, and like the “swine flu” (H1N1pdm09) pandemic influenza virus of 2009, the way forward for Covid-19 is to be considered in the same light now that extensive population immunity has evolved against severe illness and development of herd immunity or elimination of SARS-CoV-2 are no longer realistic goals.
In conclusion, the current proposed regulations are confusing, inconsistent and illogical in the face of advancing science of Covid-19 and vaccine roll-out.
Part of the reason for this is that by lumping Covid-19 in with standard NMCs, a mockery is being made of advancing understanding of the pandemic.
Surveillance and reporting of the small percentage of Covid-19 cases that we confirm can easily continue, and should, but Covid-19 should be removed as an NMC, and these regulations should be rewritten to consider the knowledge gained through science over the past 26 months.
We recommend that SARS-CoV-2 be removed from the list of notifiable medical conditions and that the following regulations be put in place:
Existing wastewater surveillance and laboratory confirmed cases of Covid-19 should continue to be reported monthly.
SARS-CoV-2 monitoring should be added to the current influenza community and hospital surveillance programmes.
Continued genomic based sentinel surveillance to track viral evolution.
Public health interventions – optimising ventilation of indoor spaces and avoiding whenever possible and masking should be recommended for during a Covid-19 and/or any other respiratory virus (including influenza should the winter influenza seasons return) waves and particularly for high-risk individuals.
Mandatory performance of hand hygiene should be stopped at points of entry to public spaces, BUT for reasons of general risk reduction of transmission of contact-related infections that are not Covid-19, alcohol-based hand rub should remain available for personal choice.
All border restrictions entering and leaving the country regarding SARS-CoV-2 should be removed with immediate effect.
And that the focus of South Africa’s efforts in this third year of the Covid-19 pandemic should be on repairing:
The damage done to children’s education.
The damage done to non-Covid-19 health priorities, including childhood vaccination, HIV, TB, antimicrobial resistance and chronic care programmes.
The public health of vulnerable populations such as the elderly and those with comorbidities and who lack social protections. A clear plan is required for protection for future SARS-CoV-2 waves, that ensures mitigation measures have substance.
The collapse of hospital services such as in the Eastern Cape, which occurred during each wave with depressing regularity. Services in prior waves in many provinces were characterised by late managerial reaction, something that is in sharp relief currently in Gauteng as hospitals fail to meet their most basic service standards. The poor accountability of health service senior managerial services across the country requires focused attention in 2022.
We are frustrated at the seeming unwillingness to break with two years of behind-the-doors decision-making and are now presented with a poorly written policy document for comment, with the deadline for these comments timed for the exact moment the State of Disaster will simply be renewed.
It is incompetence and South Africa deserves better.
Marc Mendelson is Professor of Infectious Diseases at Groote Schuur Hospital and the University of Cape Town. Shabir A Madhi is the Dean, Faculty of Health Sciences and Professor of Vaccinology at University of the Witwatersrand. Jeremy Nel is an infectious diseases expert, University the Witwatersrand. Glenda Gray is the President & CEO of the South African Medical Research Council). Regina Osih is an Infectious Diseases Specialist. Francois Venter is Professor of Medicine, University of the Witwatersrand. This article was first published in the Daily Maverick.
Covid-19 risks remain
- Harsha Somaroo
At this point it’s pragmatic to integrate COVID-19 management into routine health practices.
In early April South Africa ended most of the mandatory measures it put in place to curb the spread of SARS-CoV-2. The country terminated its “state of disaster” and moved to a transitional phase. For 30 days certain measures will remain in place. These include wearing face masks in indoor public spaces, restrictions on gatherings as well as proof of vaccination or a negative PCR test for people travelling to the country. To find out more about the implication of this decision and the reasoning behind it, The Conversation Africa’s Ina Skosana spoke to Harsha Somaroo, who has been supporting COVID-19 surveillance in South Africa’s economic hub, Gauteng province.
Has South Africa turned the COVID corner?
I believe so. South Africa has navigated the unpredictable trajectory of the COVID-19 pandemic for over two years now. The country has reached a point of understanding which COVID-19 preventive measures work. In addition, effective treatment approaches are accessible, and the development and availability of COVID-19 vaccines has been a game changer.
A decision to lift most restrictions was also informed by the fact that there has been a discernible decoupling of the COVID-19 case numbers from severe cases and deaths. In other words, the number of severe cases and deaths is low despite high numbers of new cases. This suggests that there are high levels of population protection against severe illness and death from COVID-19, due to a combination of naturally-acquired and vaccine-acquired immunity.
At this point it’s pragmatic to integrate COVID-19 management into routine practices and adopt risk-appropriate approaches based on individual vulnerabilities and the prevailing SARS-CoV-2 transmission risk and dynamics in different settings.
The transitional measures announced by President Cyril Ramaphosa attempt to reduce risk factors for SARS-CoV-2 transmission. They:
mandate face masks in indoor public spaces
recommend restrictions on public gatherings
monitor COVID-19 vaccination and test status at events and of travellers
maintain the social relief of distress grant.
A number of factors will help people manage their COVID-19 risks. These include being up to date with COVID-19 vaccination schedules and adherence to related preventive measures. Sustained communication about these measures remains important, especially for the most vulnerable groups. These continue to be: those over the age of 50, those who have a comorbid illness, those attending crowded environments and frontline healthcare workers.
What has informed the government’s decision?
In March 2020 the president declared a national state of disaster, and subsequently a national lockdown. This was in response to the uncertainty around an unprecedented global COVID-19 pandemic as well as the anticipated impact of transmission on the country’s health and the healthcare system. The aim was to trigger rapid responses for social, economic and medical preparedness.
The state of disaster allowed the government to put in place public health measures nationally to slow viral transmission. It also allowed for access to disaster funds that provided essential economic support. This included boosting medical preparation and hospital capacity, and economic support for workers and businesses during the lockdown period.
Over the following months the government adopted an incremental approach to adjusting lockdown restrictions. The country has been at the lowest level of lockdown for the past six months, following a decline in COVID-19 related morbidity and mortality numbers and sufficient health system capacity. This was the case even during the high COVID-19 transmission rates observed with the omicron variant.
The provisions of the Disaster Management Act are no longer warranted.
What are the risks?
A risk is that people associate the end of the disaster management regulations with the end of SARS-CoV-2 transmission and COVID-19 health risks. This might, in turn, mean that they take less care in managing their individual risks of acquiring COVID-19 – and its potential effects.
Thus public health messaging has a critical role to play in reinforcing the transmission and outcome risks. Hopefully keeping the transition measures in place for 30 days will empower people and communities to manage the continued risk.
Another risk is that we might see the emergence of more transmissible and virulent SARS-CoV-2 variants. But ongoing surveillance will allow for early detection and prompt management of potential resurgences.
Even if there is a resurgence, the country is unlikely to have to rely on the Disaster Management Act again. This is because revisions are being made to the National Health Act to allow for emergency interventions to be implemented if they’re needed.
Has South Africa managed the pandemic well?
South Africa – and the global community – was manoeuvring through uncharted territory with the COVID-19 pandemic. Under the circumstances the country did well.
The early declaration of a national state of disaster allowed for a rapid response that wasn’t possible under existing legislation at the time. This helped slow down rapid viral transmission and gave the health system time to prepare. It also gave the government time to try and balance the risks to health and the economy.
The government also set up a national command council. This included an expert advisory committee, to monitor the rapidly evolving pandemic and advise the government on the best evidence-based approaches as these emerged.
Another major factor was that incredible social solidarity emerged at the outset. This helped the country navigate the trajectory and uncertainty of COVID-19 waves.
However, constraints that challenged routine healthcare management – internal and external to the health system – were also magnified during management of the pandemic. This provides further motivation to strengthen the existing governance, operations, and performance of the health system, and to improve collaboration between sectors that support public health.
If we get this right the country will be able to better manage its response to future pandemics.
Covid-19 Update 85: Over 90% of those accessing Wits' campuses are vaccinated
- Senior Executive Team
It is with great appreciation that we thank you and members of our wider Wits community for vaccinating and in so doing, making Wits a safer place for all.
Over 90% of staff and students who access Wits’ campuses and precincts on a daily basis are now vaccinated (about double the national average). Just over 1% of our total population have applied for and have been granted reasonable accommodation. Well done!
We would like to thank the MVax Operations team as well as the Faculty Committees for their tremendous effort in achieving this milestone. This includes the staff at the Wits Vaccination and Testing Site where over 4 300 staff and students have received their vaccines. For those who are still not vaccinated, and who have not yet been granted reasonable accommodation, please do so as soon as possible.
Relocation of the Wits Vaccination and Testing Site
The Wits Vaccination and Testing Site will be relocating to a permanent site in the Campus Health and Wellness Centre in the Matrix Student Centre on the Braamfontein Campus as from 5 April 2022.
A pop-up vaccination site will also be established from 5 April 2022 on the Wits Education Campus to service persons on the Parktown campuses for one month. The Wits Vaccination and Testing Site at the Sports Multipurpose Hall will be closed on 4 April for the relocation to the two new sites.
For those who need booster vaccination shots, take note of the following:
Changes to the COVID-19 Vaccination Schedule
There has been a recent change to the COVID-19 Vaccination Schedule which allows for a much earlier second shot and booster for Pfizer recipients, as well as a second booster shot for persons who received the Johnson & Johnson shots.
Persons who received the Pfizer shot can get their second shot 21 days after the first shot, and booster shot 90 days after the second shot. Persons who received the Johnson and Johnson (J&J) first shot can receive their first booster 60 days later, choosing either the J&J or Pfizer vaccine. They will receive their second booster 90 days after the first booster, again this can be either J&J or Pfizer. In addition, any person with an internationally approved WHO vaccine, can register on the EVDS and receive their booster shot for either Pfizer or J&J.
Services offered at the Wits Vaccination and Testing Site
The Wits Vaccination and Testing Site offers all vaccines and provides COVID-19 antigen testing at a cost of R100. The Site is open from 08:00 to 15:00 on weekdays. Walk-ins are welcome.
New project will examine Covid-19 vaccine acceptance in southern Africa
- Wits University
A new project will examine Covid-19 vaccine acceptance in SA and Zimbabwe and recommend strategies to promote vaccination.
The project will aim to fill critical information gaps in South Africa and Zimbabwe.
The University of the Witwatersrand and its partners announced the launch of a new study on Covid-19 vaccine acceptance in South Africa and Zimbabwe, with the goal of better informing efforts to promote vaccination in the two countries.
The project is funded by Schmidt Futures, the Bill & Melinda Gates Foundation and Aspen Pharmacare.
Joining Wits University in the project consortium are Columbia University in the USA, RTI International, Charles River Medical Group in Zimbabwe, the Rhodes Trust based at the University of Oxford, the Atlantic Institute, and the Schmidt Science Fellows.
Together, this consortium comprises the Vaccine Information Network (VIN), part of the VacSafe Working Group at Columbia University.
VIN aims to increase COVID-19 vaccination rates through data-driven confidence building messages from trusted community leaders and partnerships with governments.
Madhi says, “Wits VIDA welcomes the opportunity to host this critical and timeous study to promote vaccine uptake in South Africa and Zimbabwe. African countries increasingly bear the burden of SARS-CoV-2 infection due to both misinformation and access to life-saving vaccines. The study makes an important contribution to our unique African context and to saving lives through vaccination.”
Associate Professor Janan Dietrich will lead the study in South Africa, through a partnership between Wits VIDA and the African Social Sciences Unit of Research and Evaluation (ASSURE) – a new research syndicate co-founded by Dietrich and Dr Nellie Myburgh, via the Wits Health Consortium.
Dietrich says, “I am very excited to be doing this work through ASSURE, which aims to support health research through conducting African-led social and behavioural sciences studies. The VIN study is a timely social and behavioural sciences study that places people at the centre of local efforts to promote vaccination.”
Dietrich is director of bio-behavioural research at the Perinatal HIV Research Institute (PHRU) and Myburgh is Head of Anthropology at Wits VIDA.
The project will follow a three-phase approach in both countries, beginning with focus group discussions to understand the nature and drivers of vaccine hesitancy.
In the second phase, the research team will recruit and interview a cohort of 2,000 COVID-19 vaccine recipients three times over six weeks to understand the motivations, barriers, safety perceptions, side effects and other experiences of COVID-19 vaccination.
In the final phase, the researchers will draw on their findings to co-design a strategic communications framework with local influencers, including religious leaders, community leaders and media.
“The drivers of vaccine hesitancy vary from country to country and even locality to locality,” said Dr. Larry Stanberry, Associate Dean for International Programs and Director of the Programs in Global Health at Columbia University Vagelos College of Physicians and Surgeons.
“Without a better understanding of the local reasons behind vaccine hesitancy and how people overcome their hesitancy, it is challenging to build a strong local plan to promote vaccination.”
Dr. Tariro Makadzange, M.D., Ph.D., Founder and CEO of Charles River Medical Group in Zimbabwe added: “This project will equip governments and local influencers with the critical data and information needed to create effective messaging.”
The Vaccines and Infectious Diseases Analytics (VIDA) Research Unit of the University of the Witwatersrand is an internationally recognised, African-led research unit in the field of epidemiology of vaccine preventable diseases and clinical development of life-saving vaccines. Wits VIDA conducts cutting-edge medical research, with the objective of saving lives across Africa and low and middle-income countries (LMIC). Founded in 1995, the unit’s work informs local and global policy recommendations on infectious diseases and the use of next-generation and novel vaccines. For more information, visit https://wits-vida.org/
About Columbia University’s VacSafe Working Group
The Vaccine Safety and Confidence-Building Working Group (VacSafe WG) convened by Wilmot James PhD, Senior Research Scholar at Columbia University’s Institute for Social and Economic Research and policy (ISERP) and co-convened by Joshua Nott at Schmidt Futures, will catalyze and support projects that generate, scale and analyze actively-collected vaccine safety surveillance and pharmaco-vigilance data in Africa. For more information, visit https://vacsafe.columbia.edu/.
Race and class fears amplified on Twitter when Covid-19 hit
- Job Mwaura and Ufuoma Akpojivi
Study of tweets in Kenya and South Africa shows online rage towards white communities and privileged classes can be read as fatigue with the postcolonial state.
It’s common in both Kenya and South Africa for there to be everyday conversations about inequalities in power relations and between “races”, classes and ethnic groups. Kenya, in East Africa, and South Africa, in southern Africa, share a history of British colonial divisions. In both countries, social movements and protest have sought to address these social injustices – like #FeesMustFall, #MenAreTrash, #SabaSabaMarchForOurLives, #OccupyParliamentKE.
Socio-economic and political divides were further exacerbated by the global COVID-19 pandemic and the responses of the Kenyan and South African governments. As countries went into lockdowns, citizens used social media platforms to voice their concerns.
During the first weeks of COVID-19 cases reported in Kenya and South Africa, there were hundreds of thousands of tweets posted by distressed citizens. Our study of these tweets was undertaken in order to see what kind of conversations were happening – and if they reinforced postcolonial social inequalities in the countries.
Over 129,541 tweets were collected from Kenya and 237,528 from South Africa between 5 March and 31 March 2020 using Twitter Archiving Google Sheet (TAGS). The tweets, from ordinary citizens, were then grouped into themes and the major themes were used to produce a research report.
Our study revealed several issues raised. These were divided into four themes: racialised politics, classism, privilege and panic buying, and ethnicity and ‘othering’ (or prejudice against certain groups). These themes, outlined below, echoed issues of discrimination that have characterised postcolonial states.
In short, we found that the first recorded cases of COVID-19 in South Africa and Kenya in March 2020 spawned a maelstrom of tweets reflecting fears and anxieties about the virus, as well as other deeply rooted prejudices. The rage towards white communities and the powerful and privileged class can be read as fatigue with the existing postcolonial issues.
Racialised politics
Power and the racialised politics of the pandemic dominated the Twitter conversations in both countries. At the beginning of 2020, media reports had indicated that black communities in the US were hardest hit by the pandemic due to continued institutionalised discrimination.
The first cases of COVID were reported on 5 March and 13 March 2020 in South Africa and Kenya, respectively. These first reports indicated the virus had been brought into both countries by “privileged” citizens.
The first case of COVID in South Africa was a white South African from KwaZulu-Natal province, who had travelled back from Europe. In Kenya, 239 passengers who had arrived from China were blamed for bringing in COVID. This resulted in a strong resentment in South Africa towards the white communities, and resentment towards the Chinese in Kenya.
Racial conversations worsened when some Kenyans and South Africans regarded COVID-19 as a foreign disease. As one South African tweet stated:
Imagine dying from an overseas disease when you don’t even own a passport, let alone being in a plane or ship, except for a relationship. Watseba these travellers di na le mahlale (You know, these travellers are silly) #COVID19SouthAfrica
And another, in Kenya:
We can confidently report that part of China mega loans agreement (initially negotiated by Raila as PM) was to allow illegal infiltration of Chinese into KE (Kenya), that’s why these despots continue to allow coronavirus infected Chinese to enter KE. #UhuruKenyatta #coronavirusInkenya"
Classism, privilege and panic buying
When the World Health Organization (WHO) declared COVID-19 a pandemic on 11 March 2020, it led to drastic changes in public and social life. These were accompanied by perceived and sometimes real shortages of resources. There were reported cases of long queues in the stores with individuals stockpiling essential goods.
Class issues dominated the conversations on panic buying in both Kenya and South Africa. While privileged white communities in South Africa were accused of participating in panic buying, Kenyan tweeters regarded those who participated in panic buying as a selfish and ignorant middle class:
The only people who have panicked and started panic buying of goods are the wannabe middle class. The rest of us live on FAITH. One day at a time #StayHome #lockdown #COVID19KE
Those who could panic buy had the resources to do so. Those who could not afford to, as Twitter users noted, could only panic:
To the selfish assholes black and white. Stop hoarding stock on retail shops, just because you can afford to purchase 15 loaves of bread doesn’t mean the rest of us don’t want to eat. You have clearly demonstrated if there was a deadly epidemic, you’d do the same #COVID19SouthAfrica
Ethnicity and othering
Propagation of ‘othering’ in Twitter conversations was also noticed in both South Africa and Kenya. Apart from the resentment towards white and Chinese communities, ethnic stereotyping was evident in online conversations. These were linked to the ability to survive the pandemic due to behaviours associated with certain ethnic stereotypes. Ethnic stereotypes and prejudices are divisive and generally show an unfavourable attitude towards certain groups. As one Kenyan Twitter user put it:
BREAKING NEWS! We need 2 Kikuyu’s to go to China waibe dawa ya coronavirus, 2 Kalenjins watoroke nayo mbio, 2 luos warushe mawe in case kuharibike, 2 maasai waruke nayo border, 2 kamba and 3 kisii for supernatural powers for protection and 2 Luyhas wakule evidence #covid19kenya’
(We need two individuals from the Kikuyu community to go and steal medicine from China, two from the Kalenjin communities to run with it, two from the Maasai community to cross the border with it, two from Kamba and Kisii communities to use their supernatural powers for protection and two from the Luhya community to eat the evidence afterwards)
And a South African tweet read:
Worry yam is watching all those rich South Africans (majority white) who bought more than they needed throw these away once the outbreak is brought under control on the back of many preventable deaths. #COVID19SouthAfrica"
The colonial lives on in the postcolonial
These Twitter conversations in the first few weeks of the COVID-19 pandemic in Kenya and South Africa reveal a range of unique experiences and biases shaped by postcolonial legacies of power. They represent ongoing racial and ethnic issues that are highly contested and deep-seated in the historical antecedents of both countries.
In building a post-COVID society, government policies must systematically address these postcolonial issues and legacies of power and racial and ethnic identity in order to shape a society that is responsive to the needs of all its citizens.
Please take note of rising infections in the country and particularly in Gauteng. Please get vaccinated if you have not done so yet.
Get vaccinated
Thank you to the majority of staff and students who have vaccinated – you are protecting yourself and helping to protect our broader community from serious illness. Covid-19 infections are on the increase nationally, and particularly in the province. We encourage everyone who has not yet vaccinated to do so as soon as possible. If you are due for your booster shot, please get it.
Upload your certificates
Remember to upload your vaccination certificates to the Wits portal. If you have been granted reasonable accommodation, you must upload your weekly antigen or PCR tests to the site. Email mvaxhelpdesk@wits.ac.za if you need help.
Wits Vaccination and Testing Site
A permanent Vaccination and Testing Site with a Help Desk is open at the Campus Health and Wellness Centre (CHWC) in the Matrix on Braamfontein Campus East. It is open Monday to Friday, from 08:00 to 15:00. Vaccines are free, whilst antigen tests cost R100. We have had some supply constraints this week, but will be back on track from Monday, 9 May 2022 – we apologise for any inconvenience caused by the temporary interruption. Please note that the pop-up vaccination sites in Parktown have now been closed – please come to the CHWC in the Matrix for assistance.
Please do not come onto campus if you have Covid-19 symptoms or if you test positive.
If you test positive for Covid-19 (PCR or antigen test) with NO symptoms, do not come to campus, avoid social gatherings for 5 days,
If you test positive for Covid-19 (PCR or antigen test) AND you have symptoms, do not come to campus, isolate for 7 days,
If you develop symptoms of Covid-19, do not come to campus until you seek medical advice and test for Covid-19,
If you have been in close contact with someone who has tested positive for Covid-19, you can come to campus but monitor for symptoms.
Remember to:
Wear a mask properly over your mouth and nose when indoors,
Stay in well-ventilated areas,
Vaccinate,
Maintain a social distance of at least 1.5 meters, and
the wearing of masks is no longer compulsory, although high-risk individuals are encouraged to continue wearing masks, especially when infections start to increase, and
all venues, including work spaces, can now be filled to capacity.
Until further notice, the University’s restrictions on student gatherings and events, particularly during the examination period, remain. The July graduation ceremonies will now return to the Great Hall.
Return to Campus Plans
The relaxing of the national regulations removes all restrictions that prevent professional and administrative staff from returning to work. Therefore, unless approved by their line manager, all professional and administrative staff are required to return to their respective workspaces on campus.
Schools are required to update and submit their blended teaching and learning plans to accommodate increased face-to-face contact with students for the second semester, after consultation with their respective Heads of Departments, Heads of Schools, and Faculty Deans.
Going Forward
These protocols may change as the virus evolves, as regulations change, and as the science develops. We will review our policies, rules and regulations, and in particular our Mandatory Vaccination Policy, based on the best scientific evidence on hand, and following engagements with the relevant structures within the University.
We will also monitor the power supply situation on campuses and in the City of Johannesburg over the next few weeks, to ensure that it does not compromise our return to campus plans.
Keep warm during these cold winter days.
Senior Executive Team
Covid vaccines and pregnancy: a review of the evidence shows they are safe
- Marta C. Nunes
In all the research reviewed, none found any safety concerns regarding COVID vaccines during pregnancy.
COVID vaccines have been contentious ever since they were developed in response to the coronavirus pandemic, though the evidence is that they are safe and effective. One of the concerns has been whether the vaccines were safe for pregnant women. A recent review looked at the evidence available from North America, Israel and Europe. The Conversation Africa’s Ozayr Patel asked vaccine specialist Marta C. Nunes to sum up the findings.
How did you gather the evidence?
Current COVID-19 vaccines were not tested in pregnant women in the initial clinical trials. But in many countries, pregnant women did get the vaccine. Observational studies have been done since the vaccines became available, to generate information on the vaccines’ safety and how well they work.
We reviewed more than 30 studies from a number of different countries that had data on pregnant women and COVID vaccines.
What did you find?
We divided our review into three components: safety; immunogenicity (strength of immune response); and protective effects.
The question was whether it was safe to vaccinate pregnant women with COVID vaccines. None of the studies found any safety concerns regarding these vaccines during pregnancy. The reactions to the vaccine that were reported by pregnant women were similar to the reactions that were reported by other adult people who got the vaccine. There was no difference between pregnant women and the general population as regards safety.
The second component was immunogenicity: how well the immune system of the pregnant women mounted a response to the vaccine. Pregnant women’s immune response to the vaccine was similar to the response of women who were not pregnant. Basically they had the same level of antibodies after vaccination. And these antibodies could cross the placenta. The antibodies could be found in the cord blood of the newborn, probably conferring some protection to the baby during the first few months of life.
The third part of the review focused on the protective effects of vaccines. It looked at whether vaccines protected pregnant women against COVID-19. There are not many studies yet exploring this. But existing studies found that mothers who received the COVID vaccine were protected against disease and so were their babies. Vaccinating pregnant women is much like vaccinating other adults. The big advantage is that it protects babies too.
Should women take the vaccines?
We recommend it. This is because multiple studies, including a study by our research unit in South Africa which hasn’t been published yet, show that women who are pregnant and get infected with COVID have a higher risk of preterm births. Some studies have also shown that women who get COVID during pregnancy have a higher risk of stillbirths. So it’s really important to protect pregnant women against COVID-19.
Which vaccines are the best for pregnant women?
Most of the studies in our review looked at mRNA vaccines. This is because most of the studies were in countries that mostly use those vaccines. That’s why the World Health Organization currently recommends mRNA vaccines. Not many studies looked at the vector based vaccines, for example the Johnson & Johnson and AstraZeneca vaccines. Studies that included the AstraZeneca and Johnson & Johnson vaccines did not find any problem with them. There are studies in progress that are also looking at other vaccines.
What other vaccines do pregnant women get?
Vaccinating pregnant women is not a new concept. In South Africa, pregnant women receive the tetanus vaccine. The influenza vaccine is also recommended for pregnant women. They are also given the pertussis (whooping cough) vaccine in the private healthcare system in South Africa and many other countries. It is definitely not a new concept to give pregnant women vaccines and they have been shown to be safe and protective.
Data from low and middle income countries is scarce, though. It is important to get data from these countries because populations are different in some ways. We know that women in the African region may have some comorbidities that women in the US tend not to have. It would be valuable to have studies and observations from African countries or other low and middle-income countries where the situation could be different.
- Caroline Southey with Miriam Maina and Sarita Pillay
Pasha Podcast: When SARS-CoV-2 emerged, the country took measures to restrict people’s movements and activities, to slow the spread of infections.
There were various levels of restrictions, the most severe being in place in March and April 2020.
During this “hard lockdown”, many people in South Africa really struggled. Not only did they have financial difficulties but the lockdown took an emotional and mental toll. The common themes, no matter where people lived, were feelings of anxiety, frustration and isolation. And as lockdown went on, those feelings got worse.
In today’s episode of Pasha, Sarita Pillay, a PhD student at the University of the Witwatersrand, and Miriam Maina, a research associate at the University of Manchester, take us through their research on this lockdown toll.
The researchers got their information from multimedia diary entries made during the “level 5” lockdown. Their informants were people living in a variety of dwelling types, households and urban neighbourhoods. The entries recorded participants’ daily experiences, concerns and feelings.
Much of the anxiety people felt came from the fact that it was an unknown virus. People didn’t know how it would affect them. They also worried about people breaking lockdown regulations. The economic impact of the lockdown was a concern; food security was a big issue.
Feelings of isolation and frustration came from being alone. It didn’t help that people were separated from their daily routines.
Regular physical activity may boost effectiveness of Covid-19 jab
- Wits University
A new study by a team of South African researchers shows the more you exercise, the more protective Covid vaccination seems to be.
Regular physical activity may boost the effectiveness of the Covid-19 jab, with the level of protection afforded against serious infection rising in tandem with the amount of physical activity done, suggests research published online in the British Journal of Sports Medicine.
The research done by team of South African scientists, including from Wits Sport and Health (WiSH), a Research Group at Wits University in Johannesburg, South Africa, shows convincing evidence that regular physical activity helps ward off the consequences of serious Covid-19 infection, reducing the risk of hospital admission, intensive care, assisted ventilation or death. Similarly, vaccination also minimises these risks.
Previously published research, also by WiSH using Discovery Health data, on the additive effects of physical activity on vaccination against various infections, suggests that it enhances the body’s immune response. Up until the recent study, it was not known whether this might also apply to SARS-CoV-2, the virus responsible for Covid-19 infection.
For the study, researchers drew on anonymised Discovery Health medical records and wearable activity tracker data for healthcare workers belonging to a medical insurance scheme as well as a health promotion and behavioural change programme.
Participants were mapped to physical activity categories using their average monthly levels in the two years preceding the start of the study: under 60 minutes of a week (low); at least 60-149 minutes (medium); and 150 minutes + (high).
Covid-19 swab test results were analysed for 53,771 participants with low levels of physical activity, 62,721 with medium levels, and 79,952 with high levels.
Complete health, Covid-19 vaccination and physical activity data were obtained for 196,444 adults who tested negative for SARS-CoV-2. The study participants were vaccinated between mid-February to the end of October 2021 with a single dose of the Johnson & Johnson vaccine.
Vaccine effectiveness against Covid-19 among fully vaccinated people in the low physical activity category was 60%. In other words, the risk of hospital admission was reduced by 60% in this group.
Comparable risk reductions for those in the medium and high physical activity groups were, respectively, 72% and 86%.
“Those who were fully vaccinated and who clocked up high weekly levels of physical activity were nearly three times less likely to be admitted to hospital than those who were vaccinated but in the low physical activity category,” says Professor Jon Patricios from Wits Sports and Health.
Similarly, those in the medium physical activity category were nearly 1.5 times less likely to be admitted to hospital with Covid-19 infection.
“The findings suggest a possible dose–response where high levels of physical activity were associated with higher vaccine effectiveness,” says Patricios.
“This substantiates the WHO recommendations for regular physical activity — namely, that 150–300 minutes of moderate intensity physical activity per week has meaningful health benefits in preventing severe disease, in this context against a communicable viral infection.”
As this is an observational study, the researchers were not able to establish the reason for the increased effectiveness of the vaccine. However, it is suggested that it may be because of a combination of enhanced antibody levels, improved T cell immunosurveillance, and psychosocial factors.
The researchers also warn that the results cannot be generalised to other populations, virus variants, or other types of Covid-19 vaccines.
“The protective effect of physical activity appears to result from exercise’s powerful effect at many levels of the body’s physiology that impact almost every organ system including the immune system,” says Patricios.
“Public health messaging should encourage physical activity as a simple, cost-effective way of enhancing vaccine effectiveness to mitigate the risk of severe Covid-19 illness requiring hospital admission.”
The Wits Institute for Sports and Health received a boost earlier this year when the family of Brian and Dorothy Zylstra pledged R80 million towards the Institute in their name. This donation from the Skye Foundation was announced at the launch of the Friends of Wits in Australia in May as part of the centenary campaign.
Covid disrupts traditional rituals of mourning
- William Gumede
We need to find ways to grieve as individuals, and collectively as a nation, or we risk grief becoming chronic, unleashing psychological and physical illnesses.
Although many South Africans have experienced so much grief that they often assume they did not have the time, the luxury, or the money to grief, stoically soldiering on with life after devastating losses, they will have to find ways to grief as individuals, and also collectively as a nation, or risk grief becoming chronic, unleashing new emotional, psychological, and physical illnesses.
I suffered the devastating loss at the end of May 2021, of a very close friend, Thashnee Padiaychee, who was in the prime of her life, not of Covid-19, but of breast cancer. Like many, following a bereavement I felt intense sadness, struggled to let go and trying to make sense of her death, wondering whether there could have been other therapies available around the world to treat her cancer that we may not have been aware of.
The devastation wreaked by Covid-19 caused many South Africans wretching grief, their lives shattered by the death or illness of a loved one, either because of Covid-19 or because of other critical illnesses aggravated by the impact of Covid-19.
Heartbreakingly, many Covid-related deaths could have been prevented. There was government incompetence in not procuring vaccines earlier. Some ANC government leaders made decisions to buy vaccines based on ideology, rejecting supposedly “Western” manufactured vaccines, for developing country manufacturing ones – in the process delaying the delivery of vaccines to the ill.
There was corruption in the misappropriation of funds intended for protective equipment. There was an ill-considered delay in allowing the private sector to roll out vaccines. Harmful myths were and are still spread about vaccines. Quack remedies were often proffered – and still are.
The public health service has been crippled by patronage appointments of incompetent politically connected cadres, the capture of procurement of critical supplies and ideological decision-making and corruption, resulting in healthcare, medicine, and facilities not available for Covid suffers, but also for those struggling with critical illnesses such as cancer. The loss of lives under circumstances of government corruption, mismanagement, and lack of care, is even harder to bear.
Covid-19 disrupted many of the rituals of mourning and grief – because of the lockdown restrictions on funerals, communal singing, and social distancing. Many were deprived of saying final farewells, giving a last touch or holding a hand of those who have died during this Covid-19 epidemic. Pursuing face-to-face reconciliation, forgiveness, and closure with those on their deathbeds which is so crucial for post-grief healing has been impossible during Covid-19.
It is crucial that especially black South Africans find time, space, and support to grief, not only for Covid-19 grief, but all other losses, traumas, and deaths. The cumulative grief of lives lost many black South Africans experienced before Covid-19, now combined with Covid-19, could lead to what specialists call “prolonged grief disorder”, in which grief symptoms, without active intervention or treatment, may persist indefinitely.
Self-care is going to be crucial to overcome grief. The loss of someone close may shake one’s sense of self. Life may feel meaningless. Numbing oneself emotionally to deal with the shock as is often the case in particularly black communities that have experienced so much trauma, is not healthy.
One has to accept that “bad things happen at random”. Successfully rebuilding one’s life after the passing of a loved one is to try to find a new sense of purpose in the tragedy, to continue to care about others and to stay engaged with one’s surroundings. Given the fragility of life it is important that we live more intentionally, engage more consciously and caringly with the ones we love and feel gratitude for being alive. And that we love consciously – whether intimate partners, family, or friends.
Toxic relations whether in intimate partners, personal friendships or with toxic political parties one supports should be jettisoned.
The fragility of life underscored by Covid-19 must compel us to increase the frequency of use keeping in contact with family members, friends, co-workers, and neighbours. It must also end the culture of secrets within families, for us to become more accepting of differences and different beliefs.
As I grew older, I have come to appreciate the cultural, religious, spiritual, and communal rituals during apartheid that helped many of us recover from the death of loved ones, misfortune, and trauma. The community fragmentation in the post-apartheid-era, partially because of state failure, corruption, and the corruption in many instances of many traditional grief rituals, means that it may be necessary for some of the rituals to be adapted for present times and new more relevant and appropriate ones fostered. New individual, family and community memorials are crucial to celebrate those who died in symbolic and spiritual ways and in memories.
Black South Africans, because they are generally poorer, have been unequally hit by dead, chronic illnesses, and post-traumatic trauma because of Covid-19 or because of critical illnesses aggravated by the impact of the virus. Because of South Africa’s segregated past, South Africa does not have collective mournings, rituals and memorials, as these are also segregated along race, ethnicity, and political affiliation. Covid-19 is an opportunity for the country to foster a national ritual of mourning around the illness that can cut across ethnic, colour or political affiliation.
If all South Africans, use the Covid-19 experience to work towards restoring solidarity, empathy and caring for others, across colour, ethnicity and political affiliation for those who are grieving, the devastation of Covid-19 could be turned into a new sense of common national spirit.
A national memorial for those who died of Covid-19 across colour, ethnicity and political affiliation, in which the names and the pictures of all those who died of Covid-19 should be considered. In this way, Covid-19 could be something South Africa can unite around – even if in grieving.
William Gumede is Associate Professor, School of Governance, University of the Witwatersrand, and author of Restless Nation: Making Sense of Troubled Times (Tafelberg). This article was first published in TimesLive/Sunday Times.













-600x300.jpg "Professor Lynn Morris received the Harry Oppenheimer Fellowship Award in June 2017")











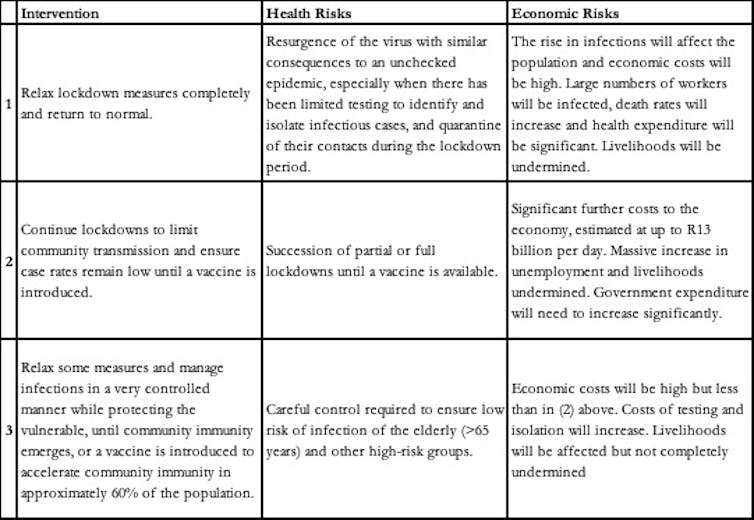

 The grant award supports COVID-19-related visualisation and analytics for Southern Africa. The nature of the project is interdisciplinary, where medical data and expertise need to be combined with the wealth of methodologies and algorithms used in advanced analytics, Big Data and Data Science. Assumptions used in the project revolve around our current level of understanding of advanced analytics driven by Data Science and other disciplines. Both main-stream statistical frameworks, frequentist and Bayesian are an underlying assumption to model development. Input from the different medical, virology and custodians of static data pertaining to populations, social and medical vulnerabilities, access to medical infrastructure, prevalence of various relevant pre-existing conditions are also underlying assumptions.
The grant award supports COVID-19-related visualisation and analytics for Southern Africa. The nature of the project is interdisciplinary, where medical data and expertise need to be combined with the wealth of methodologies and algorithms used in advanced analytics, Big Data and Data Science. Assumptions used in the project revolve around our current level of understanding of advanced analytics driven by Data Science and other disciplines. Both main-stream statistical frameworks, frequentist and Bayesian are an underlying assumption to model development. Input from the different medical, virology and custodians of static data pertaining to populations, social and medical vulnerabilities, access to medical infrastructure, prevalence of various relevant pre-existing conditions are also underlying assumptions. 
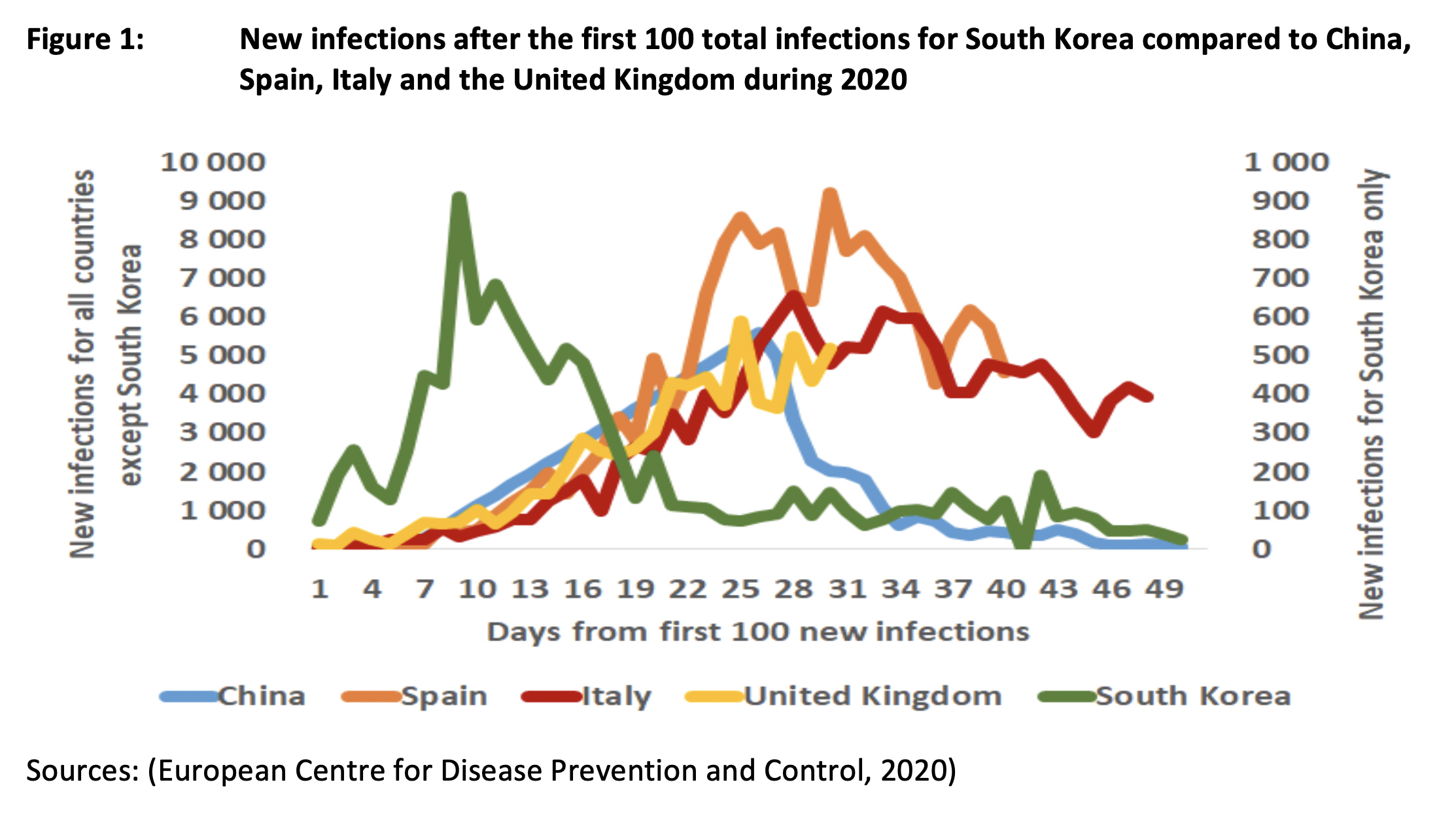
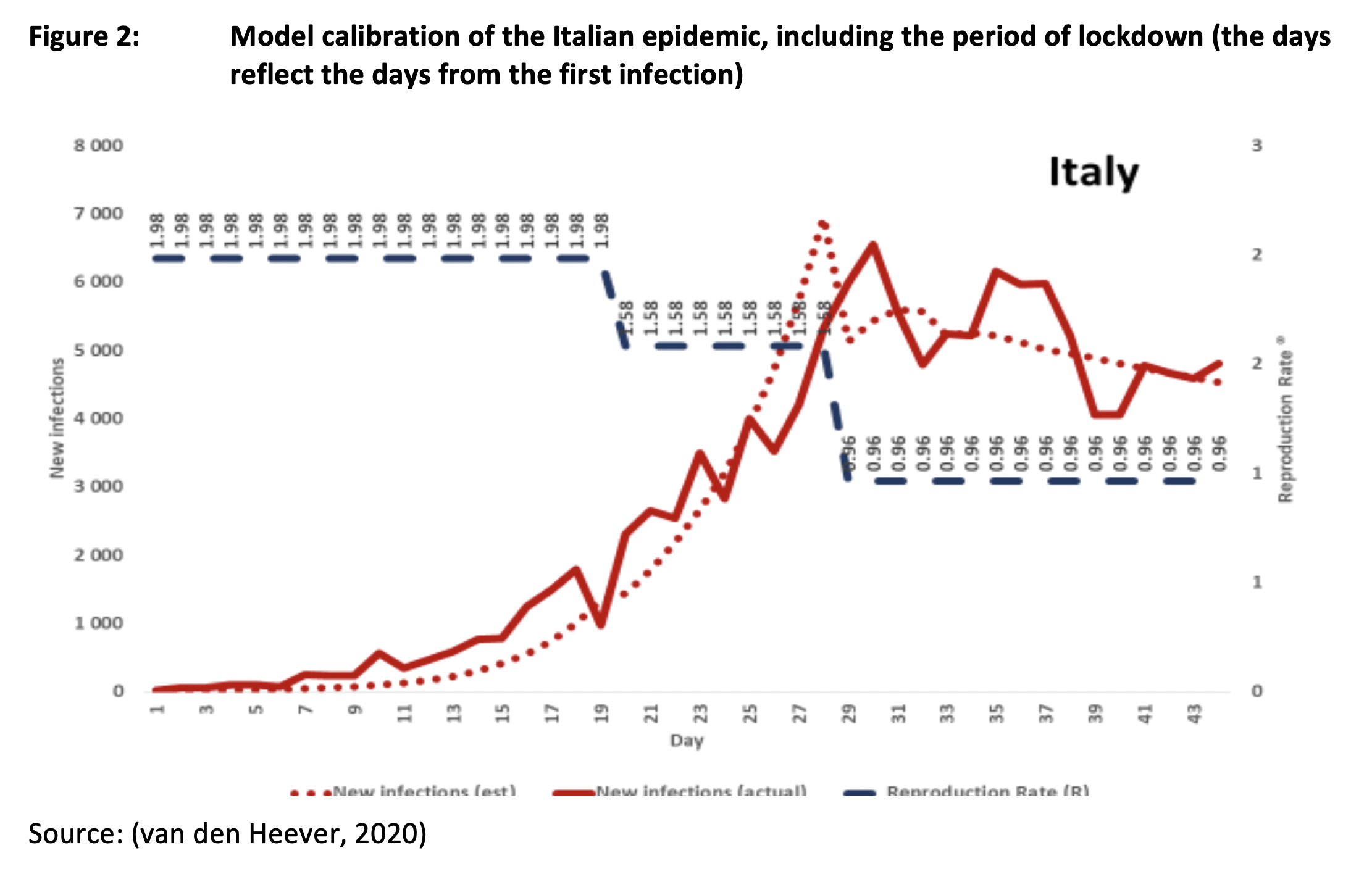
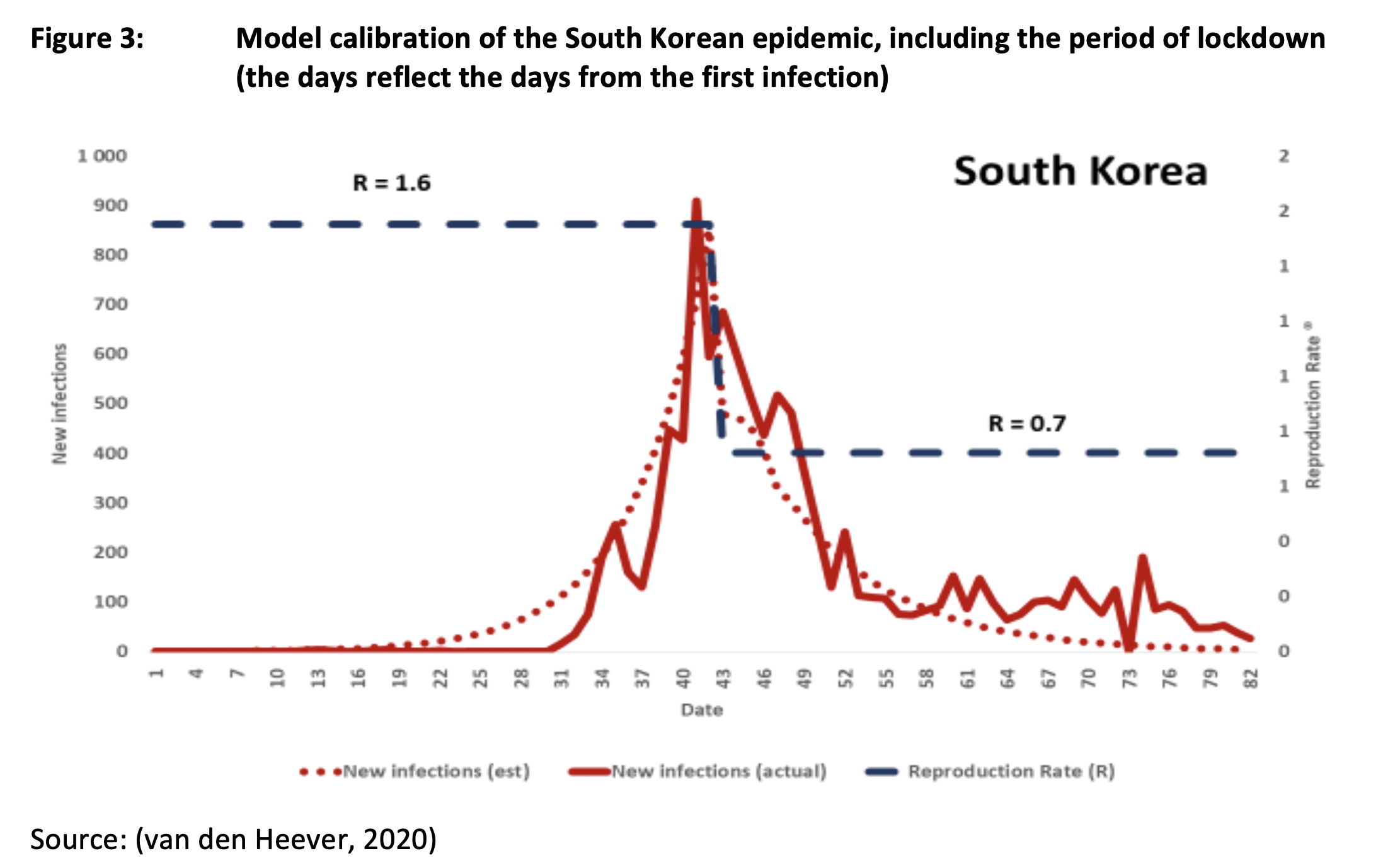
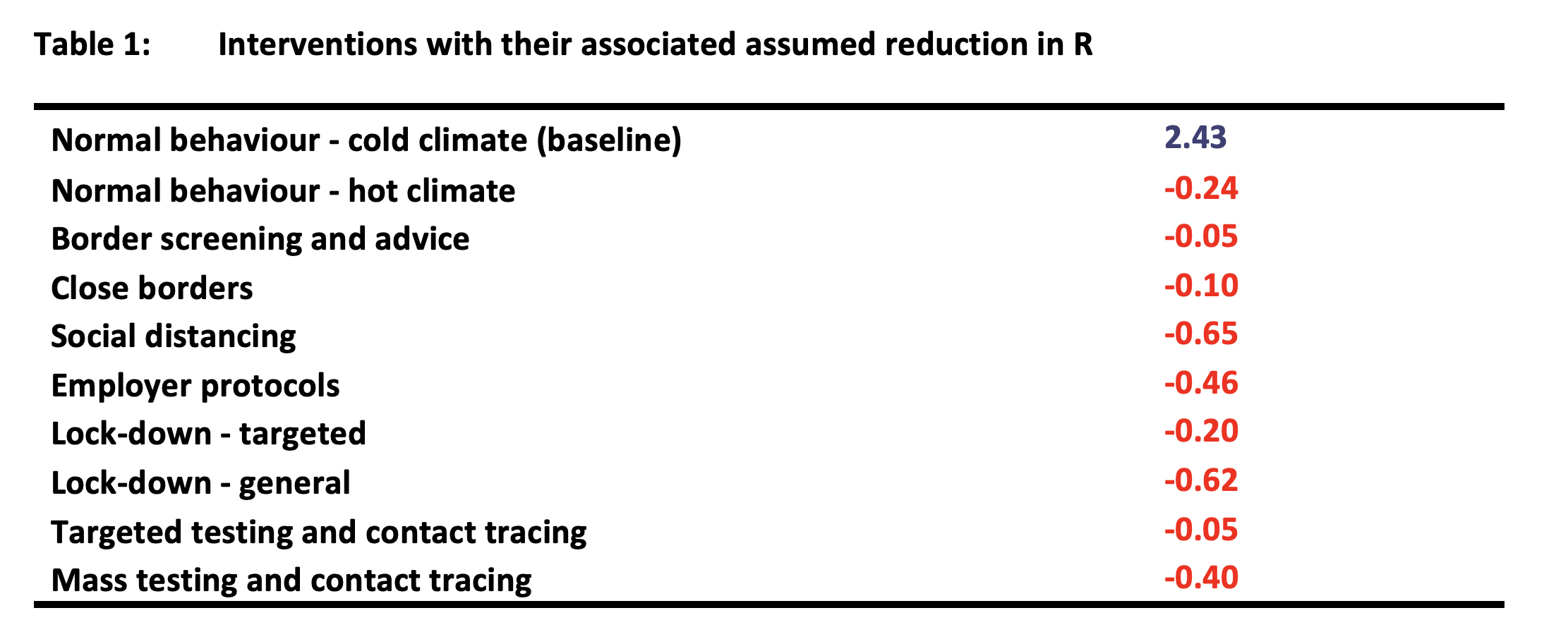

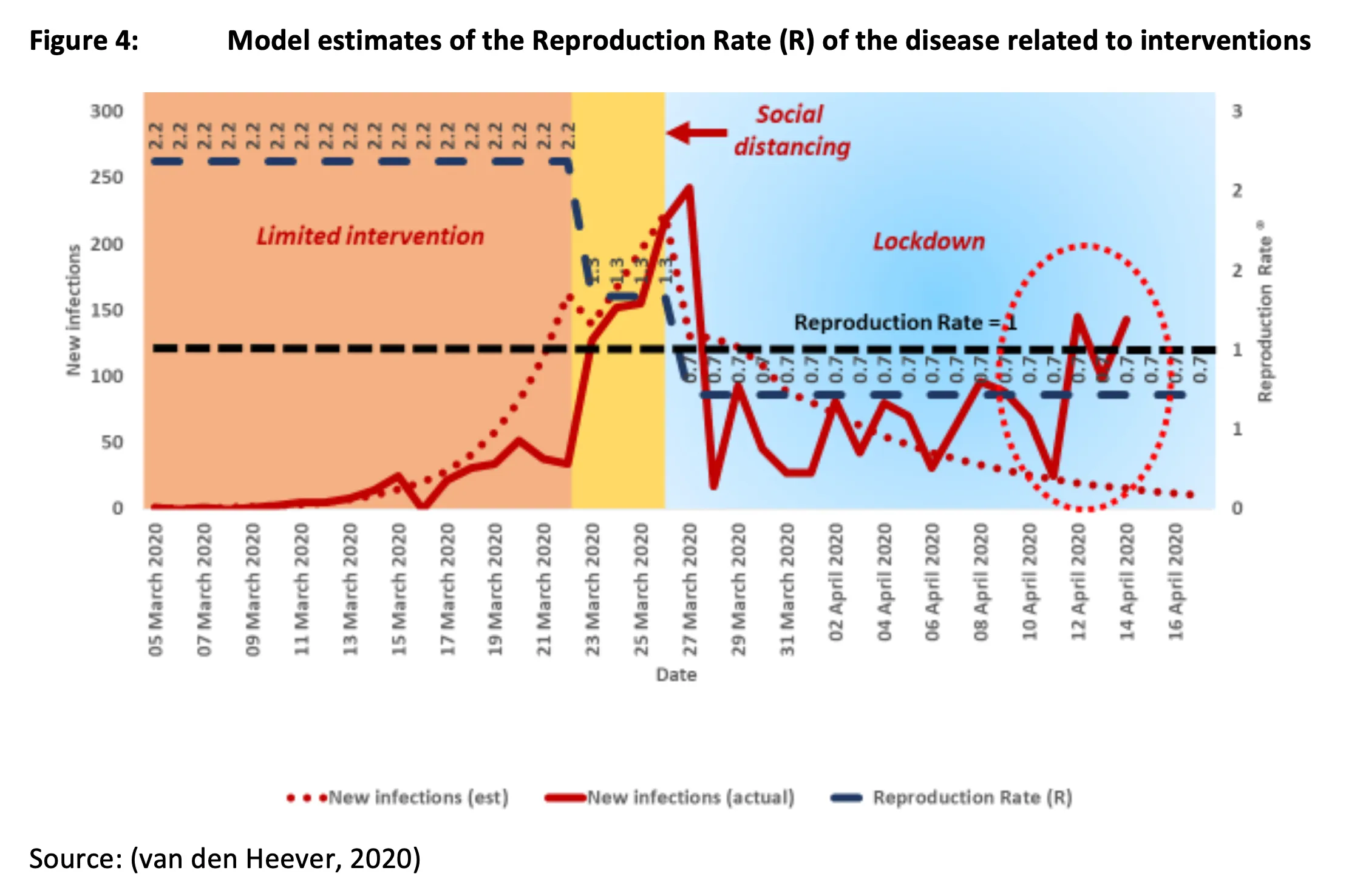
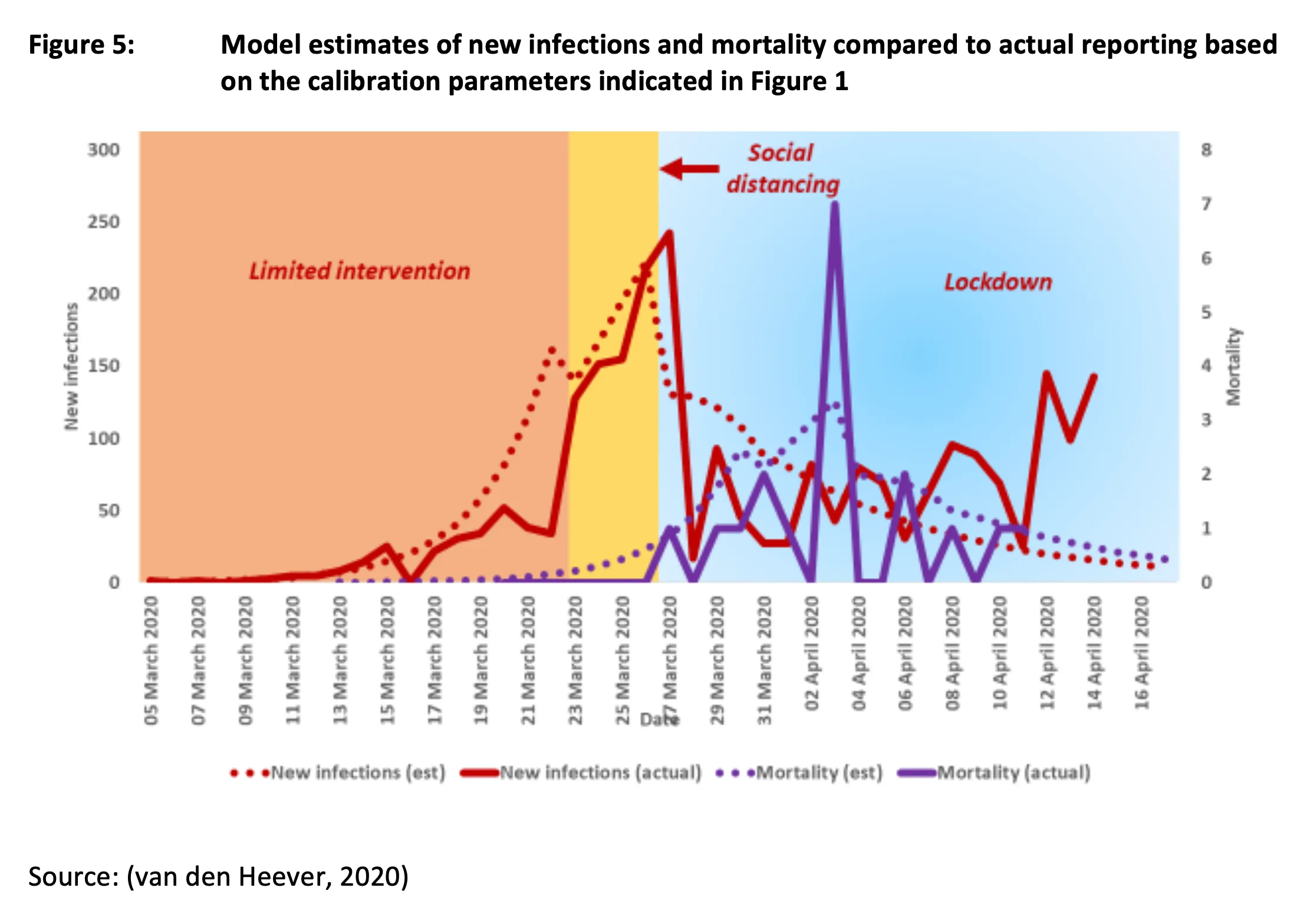
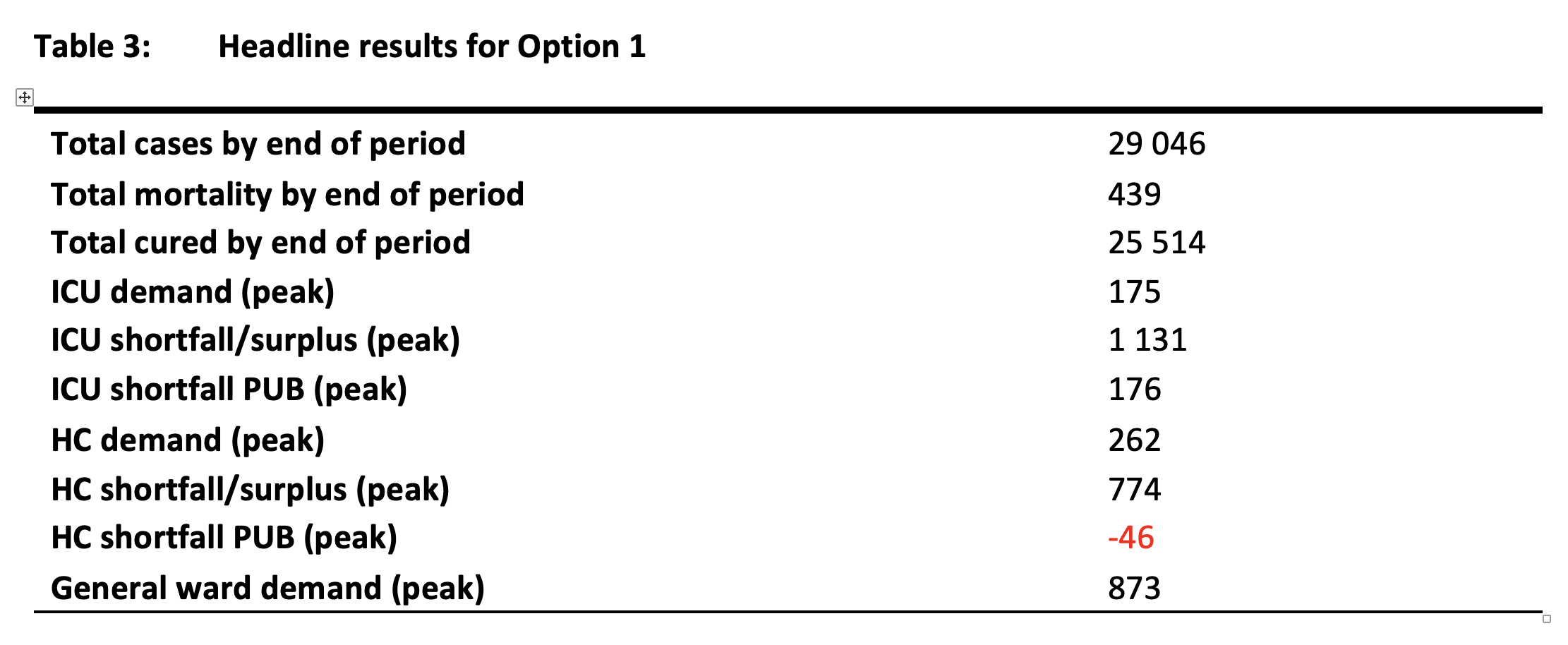
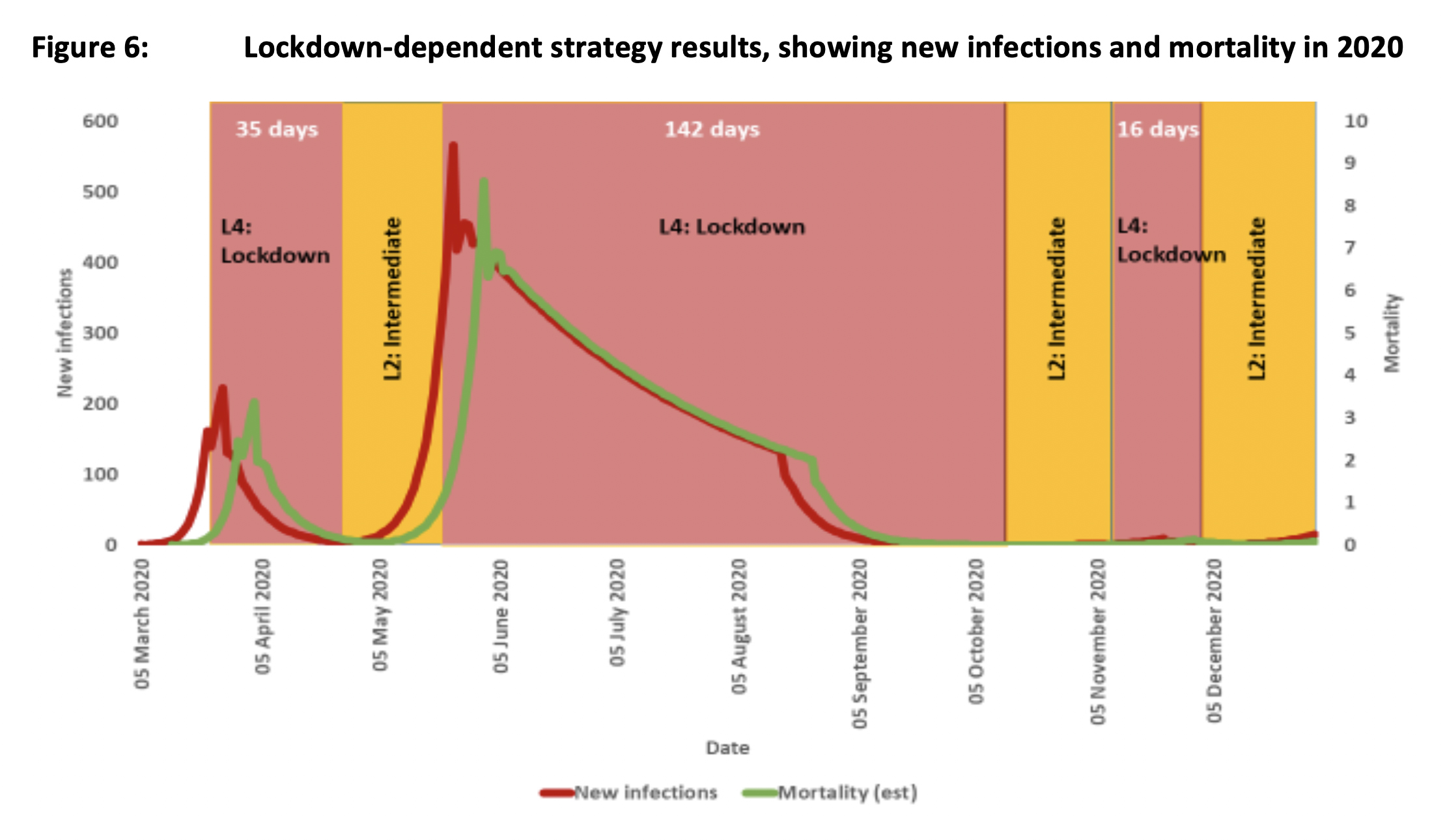
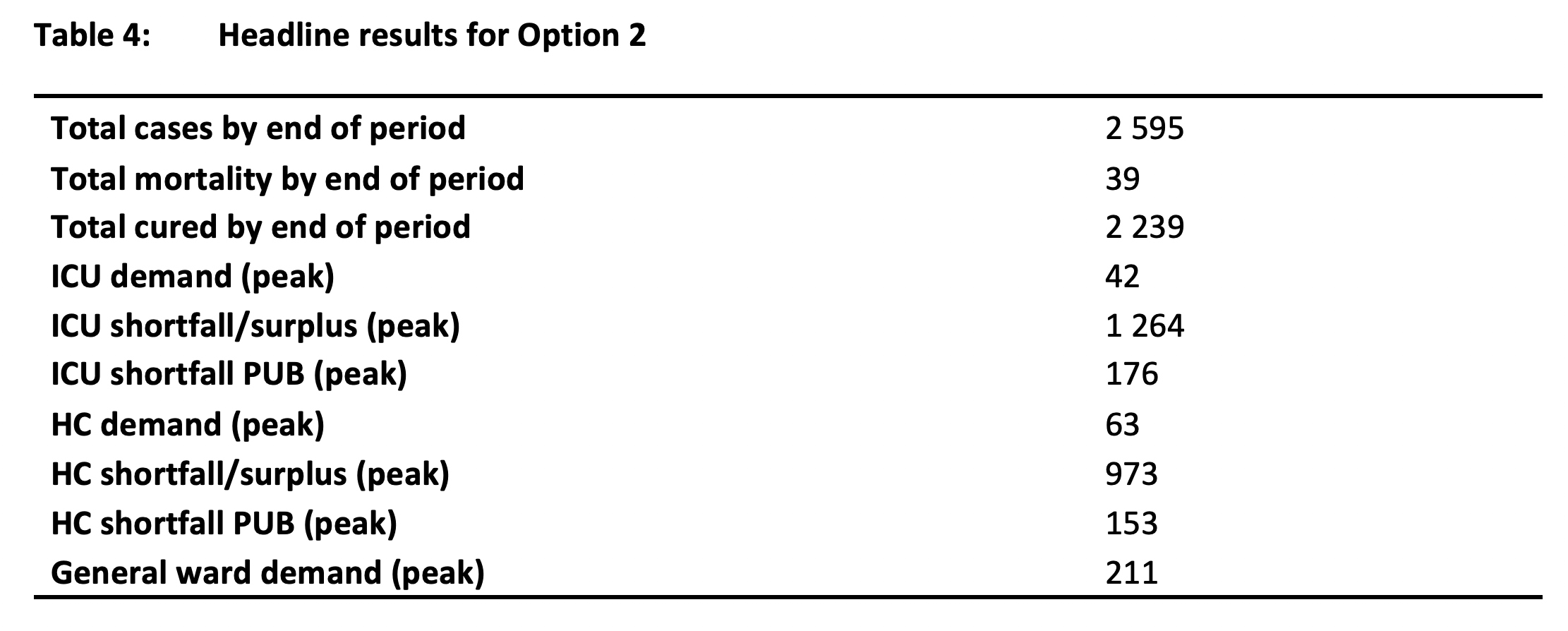
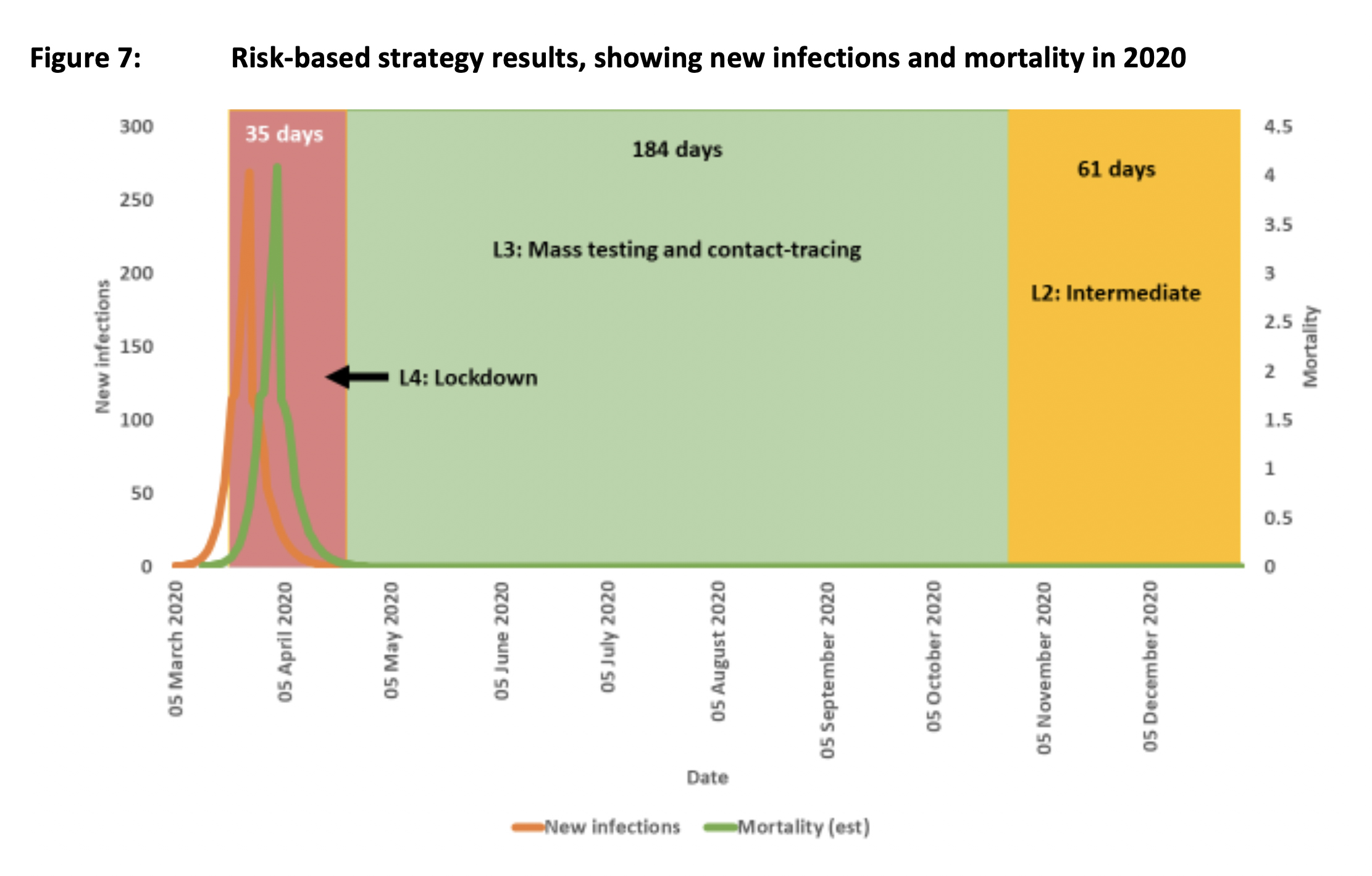










 Vaccines and Infectious Diseases Analytics Research Unit (VIDA), leads the South African Ox1Cov-19 Vaccine VIDA-Trial. ©WITS UNIVERSITY")
.")

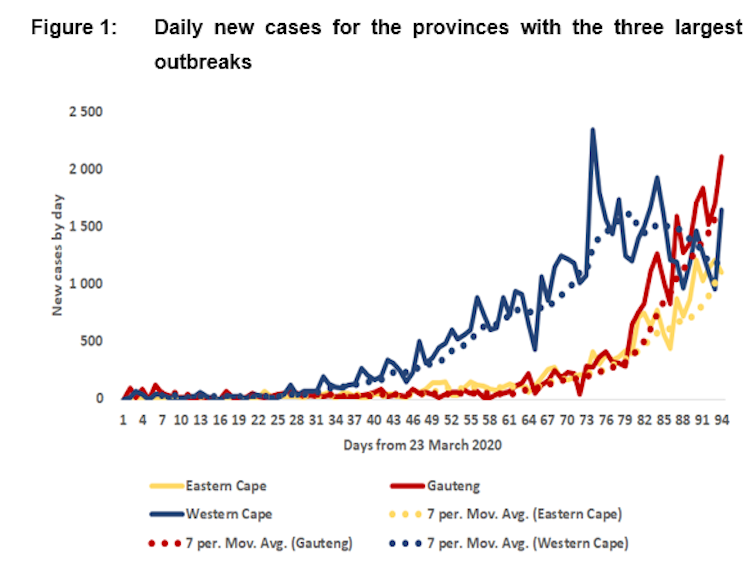
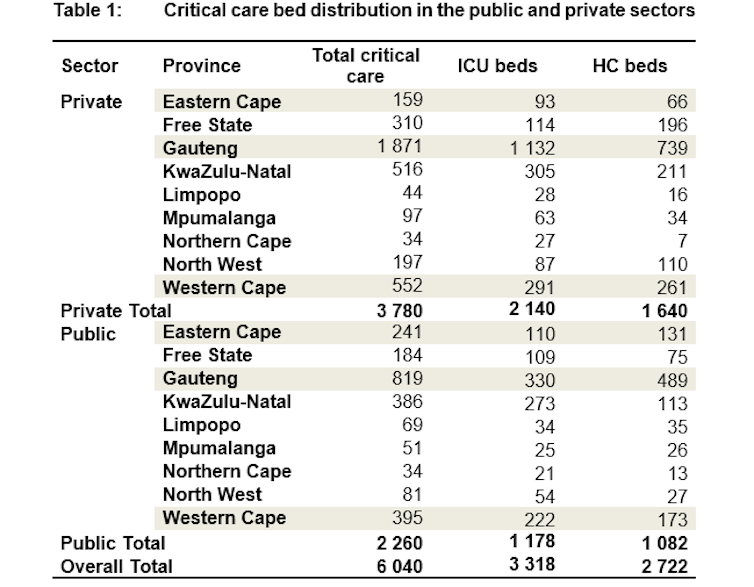










-600x300.png "Wits Agincourt nurse Olivia Khosa tests a child in rural Bushbuckridge for COVID for the PHIRST study")
-600x300.png "Nurse Thandy Nyalungu with a participant in the PHIRST study in Agincourt")



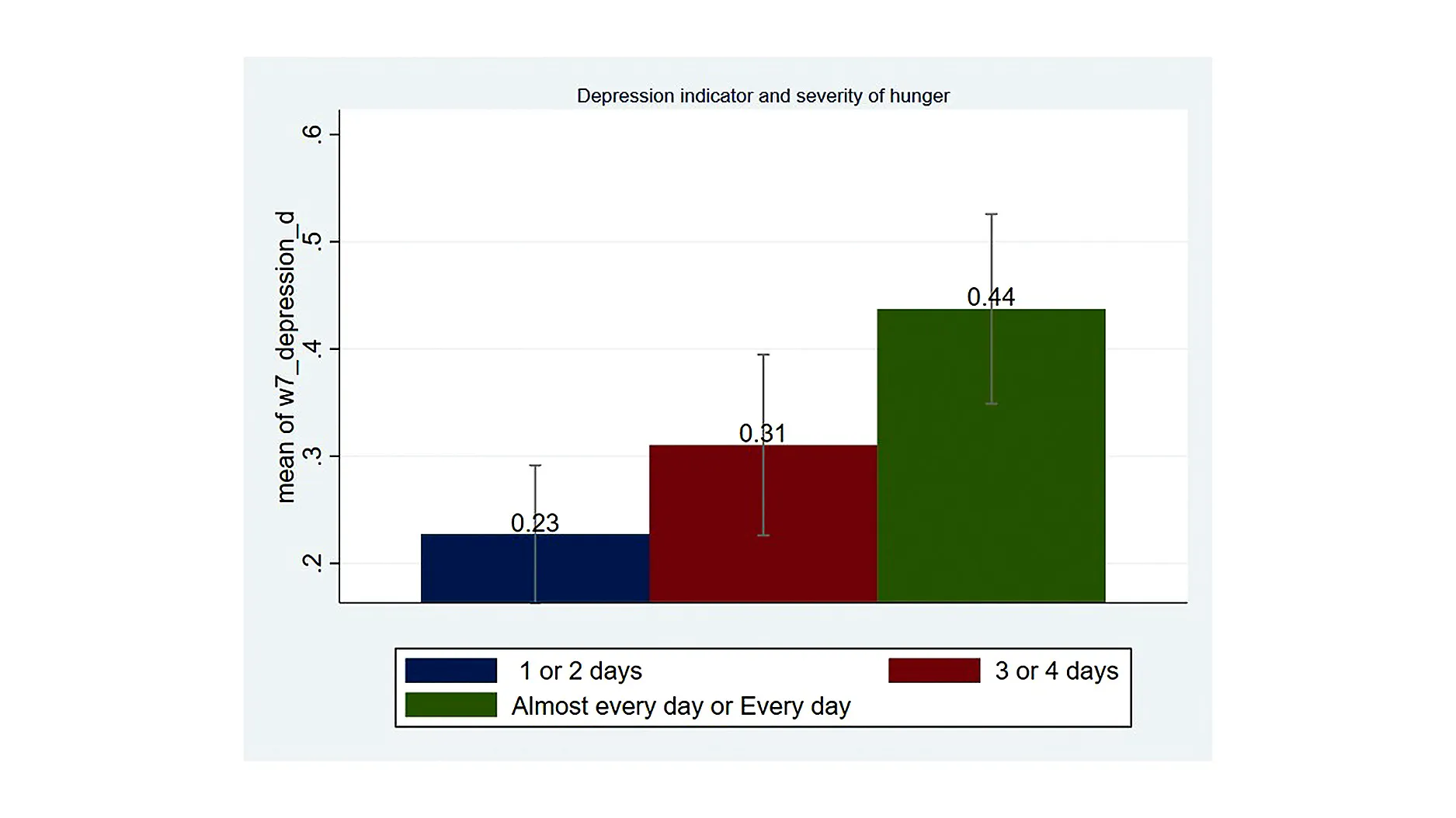






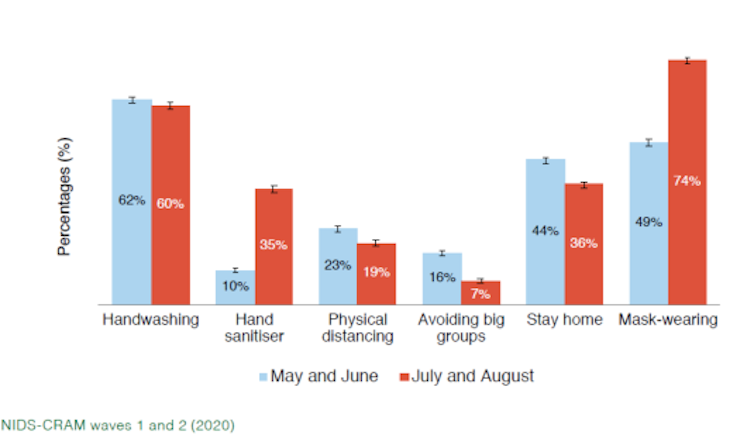
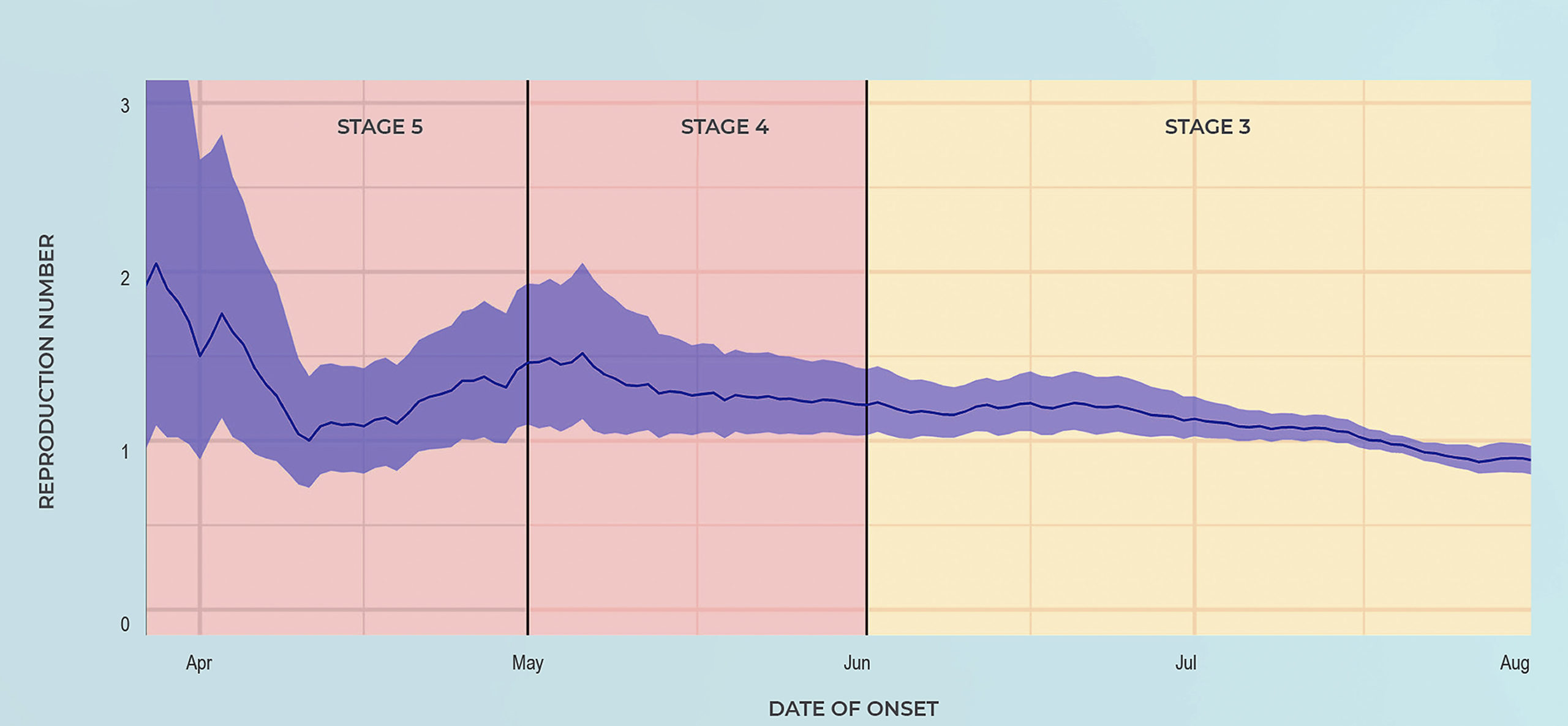
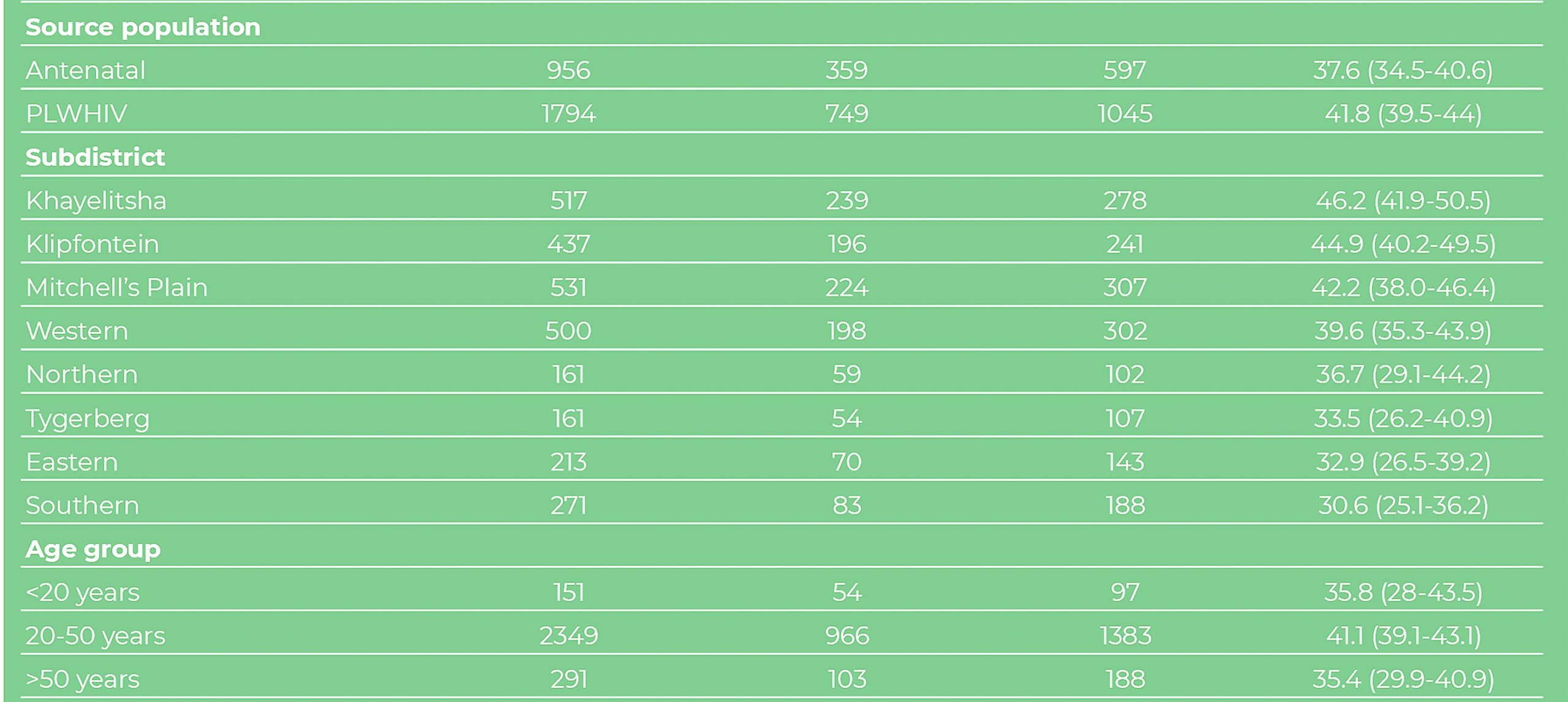



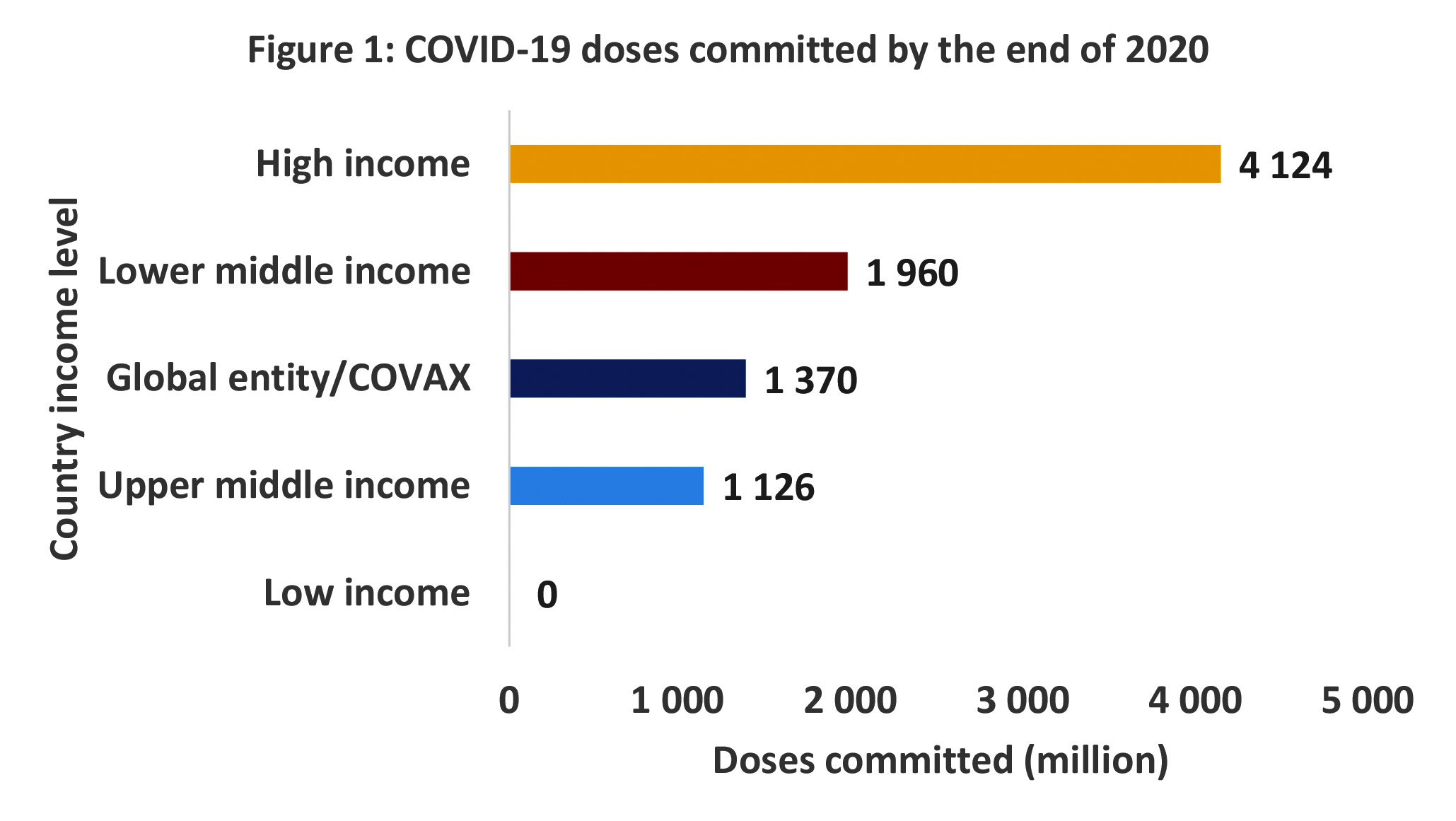
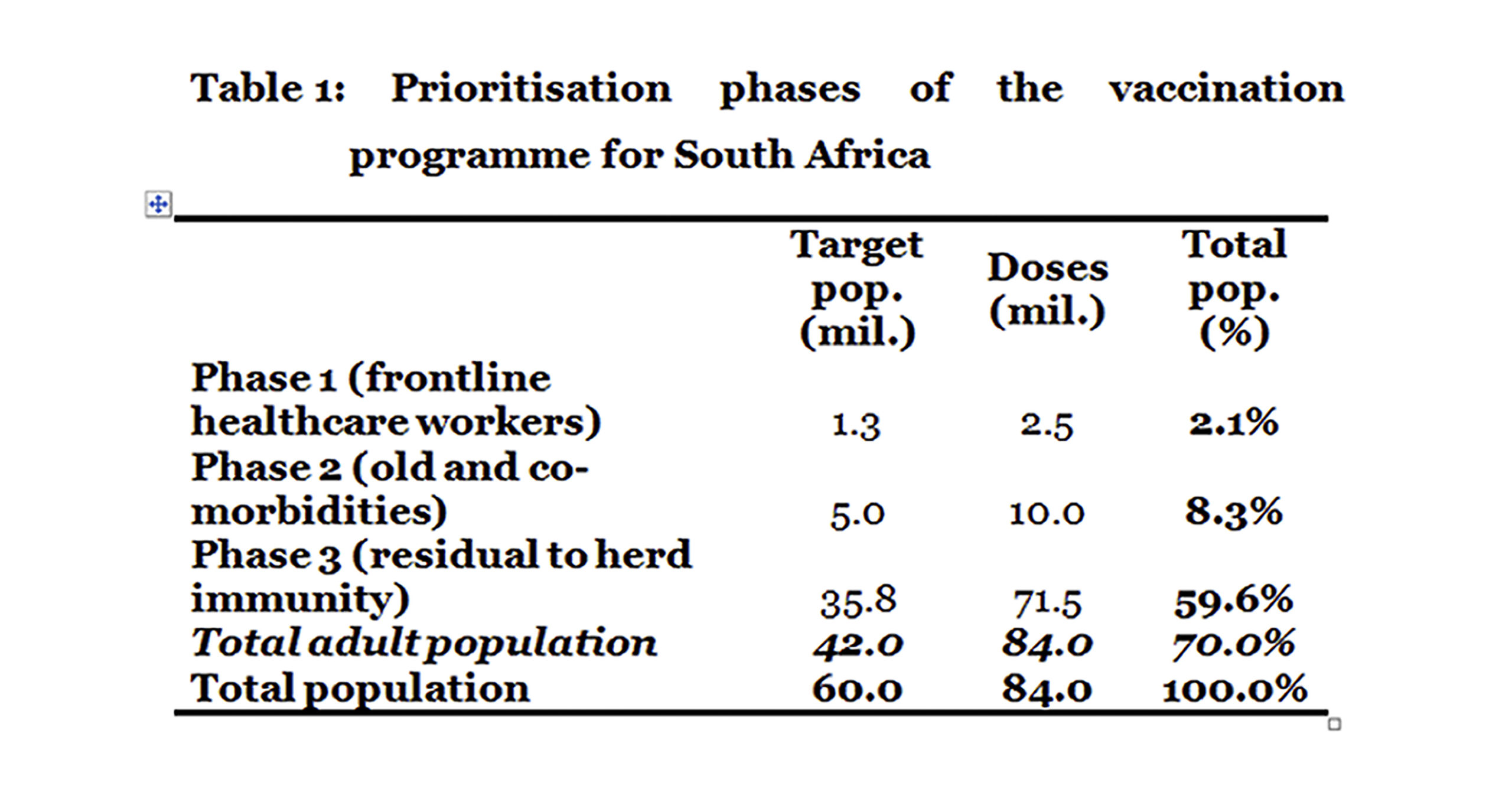
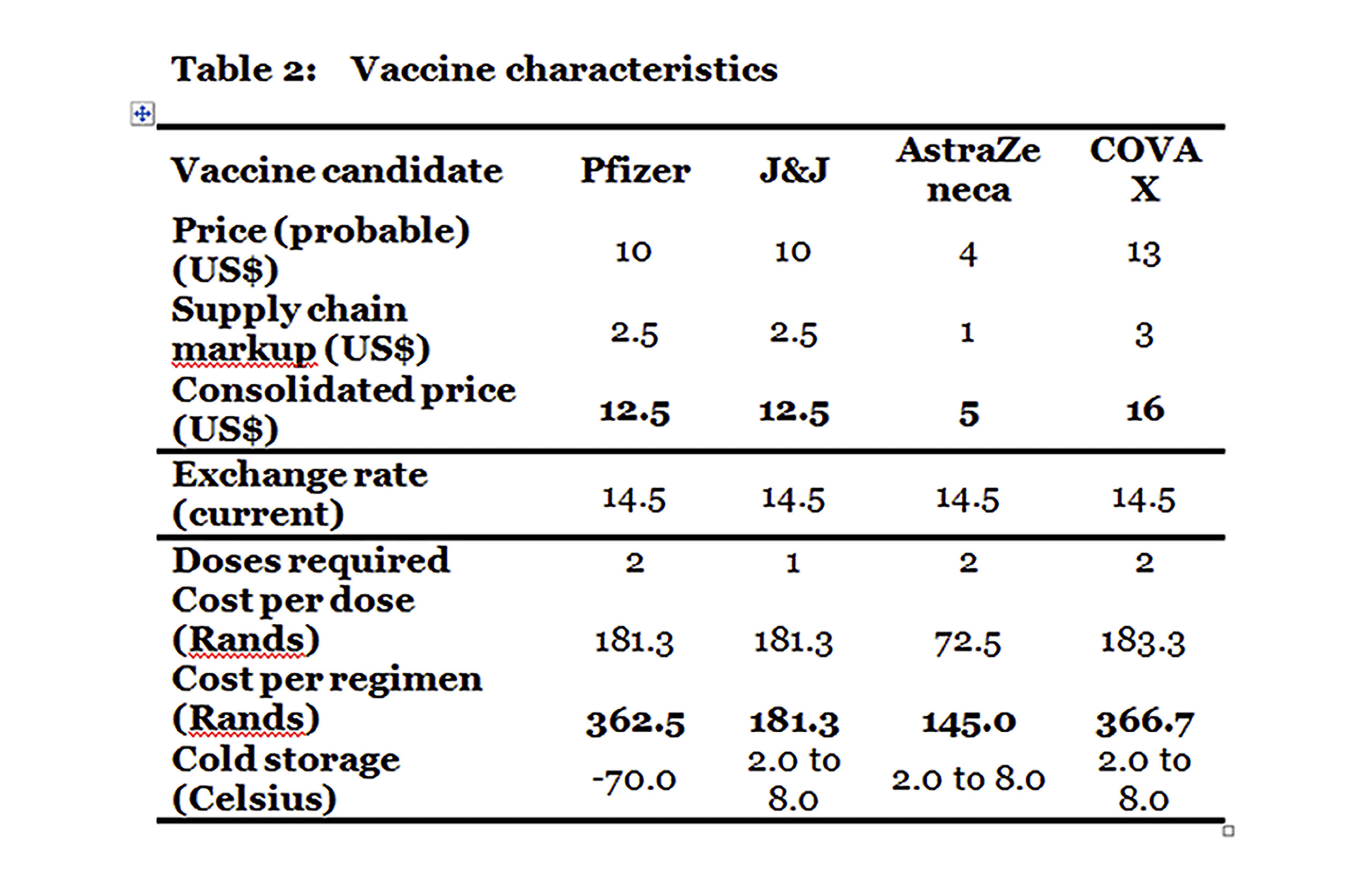
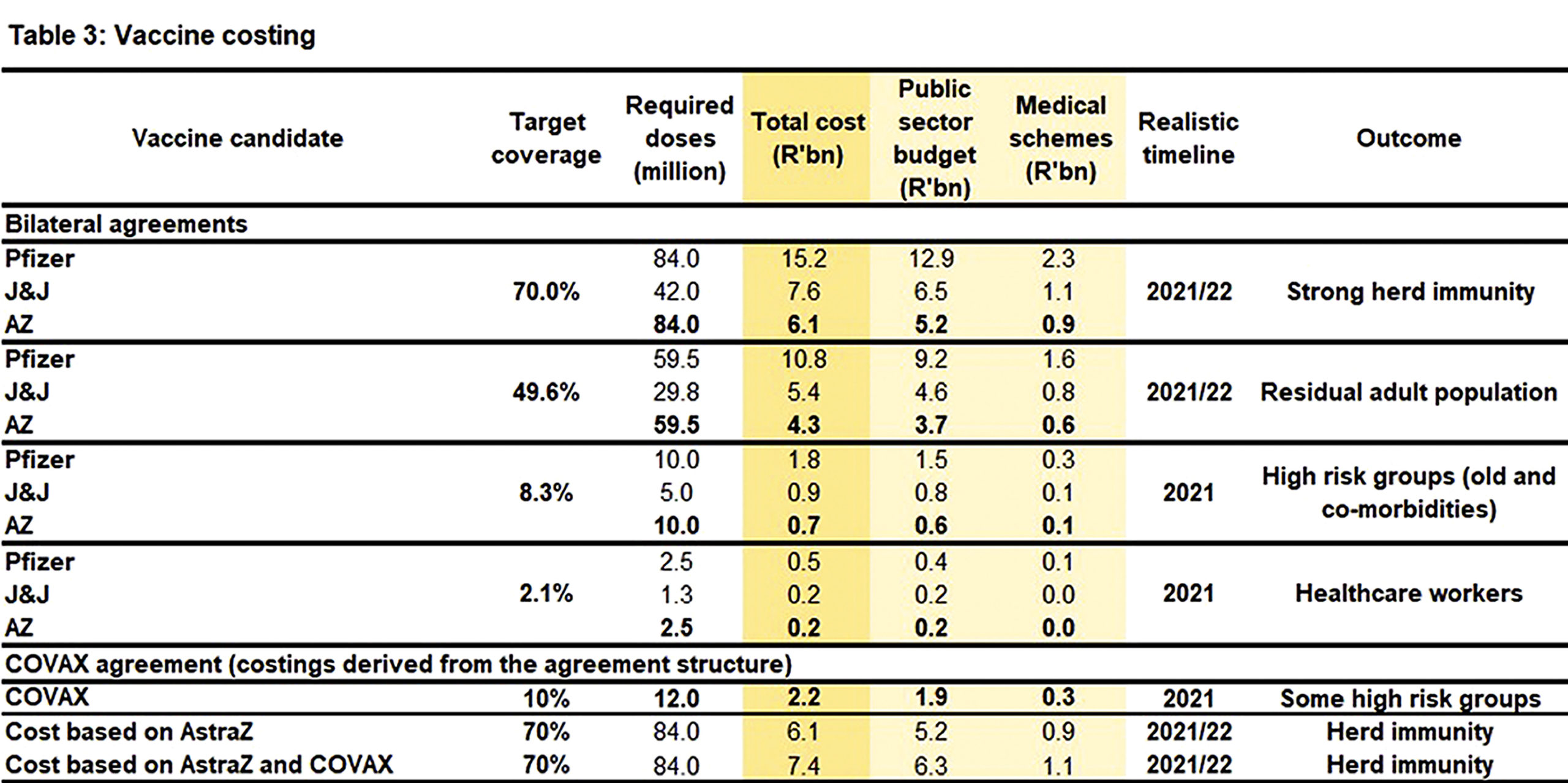



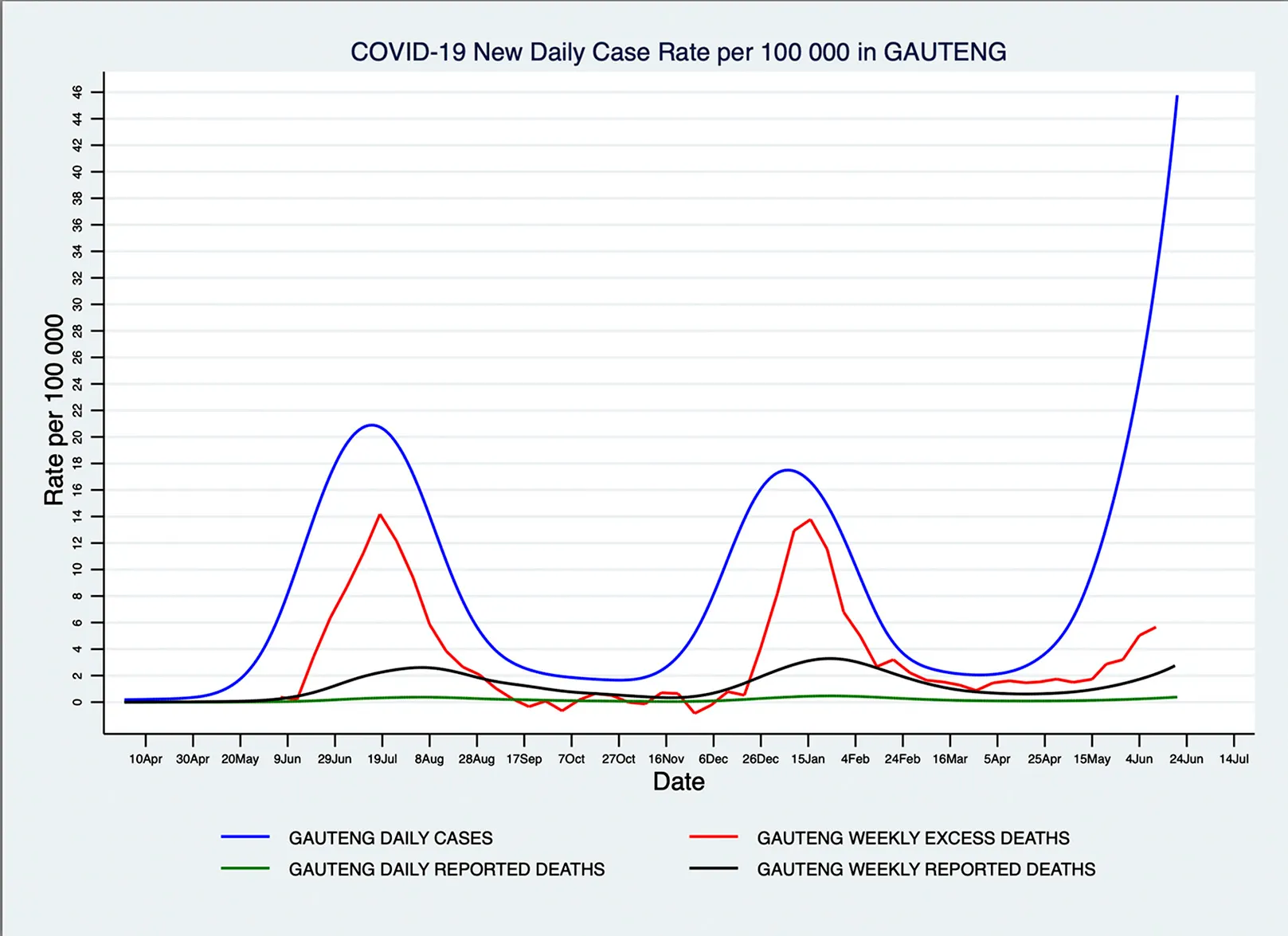
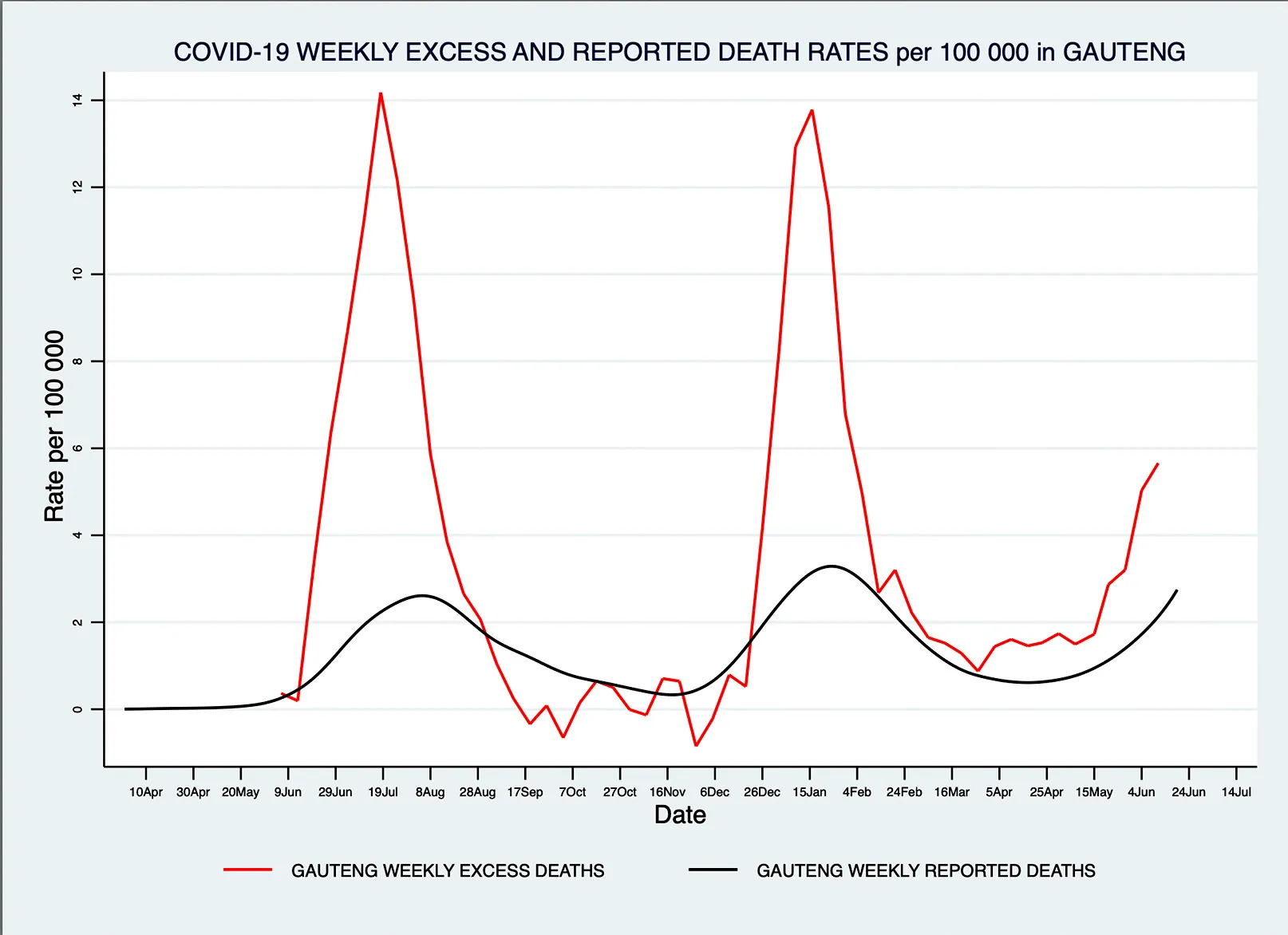




 Centre entrance wall that was vandalised to gain entry to the clinic. (Photo: Anusha Nana)")



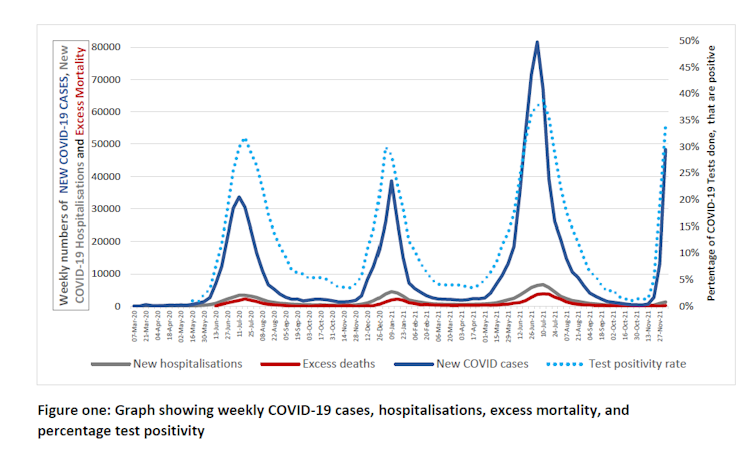
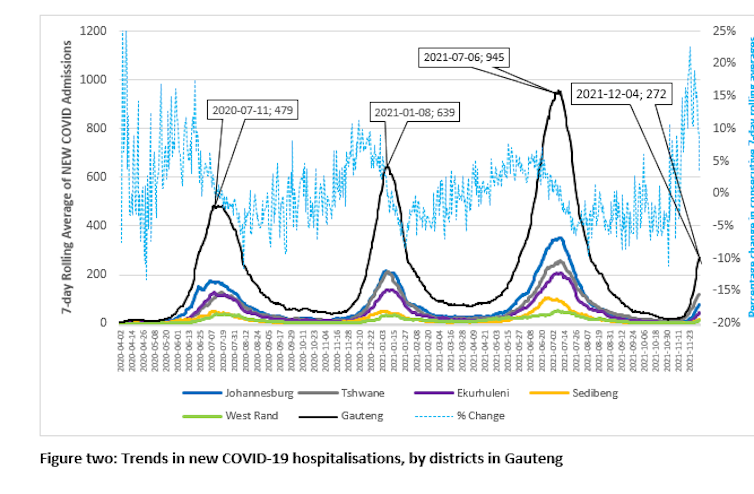
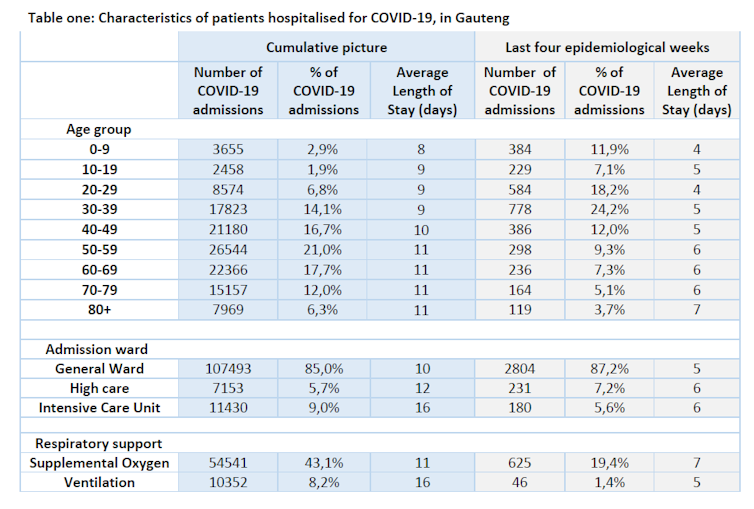

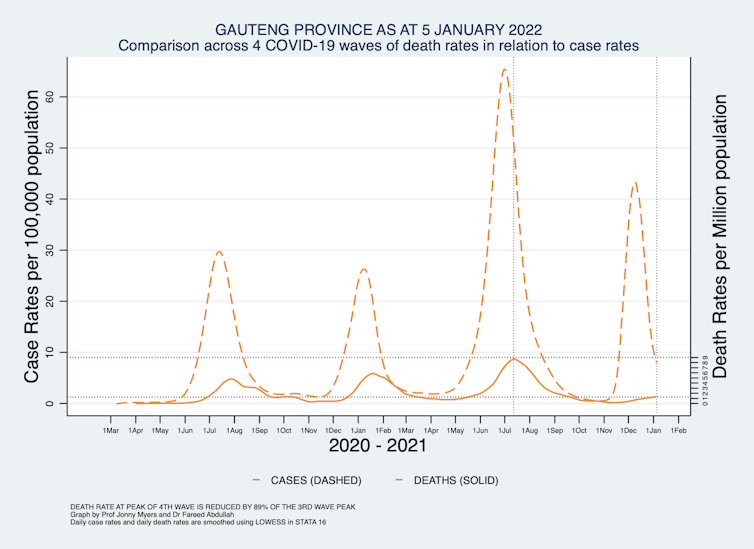





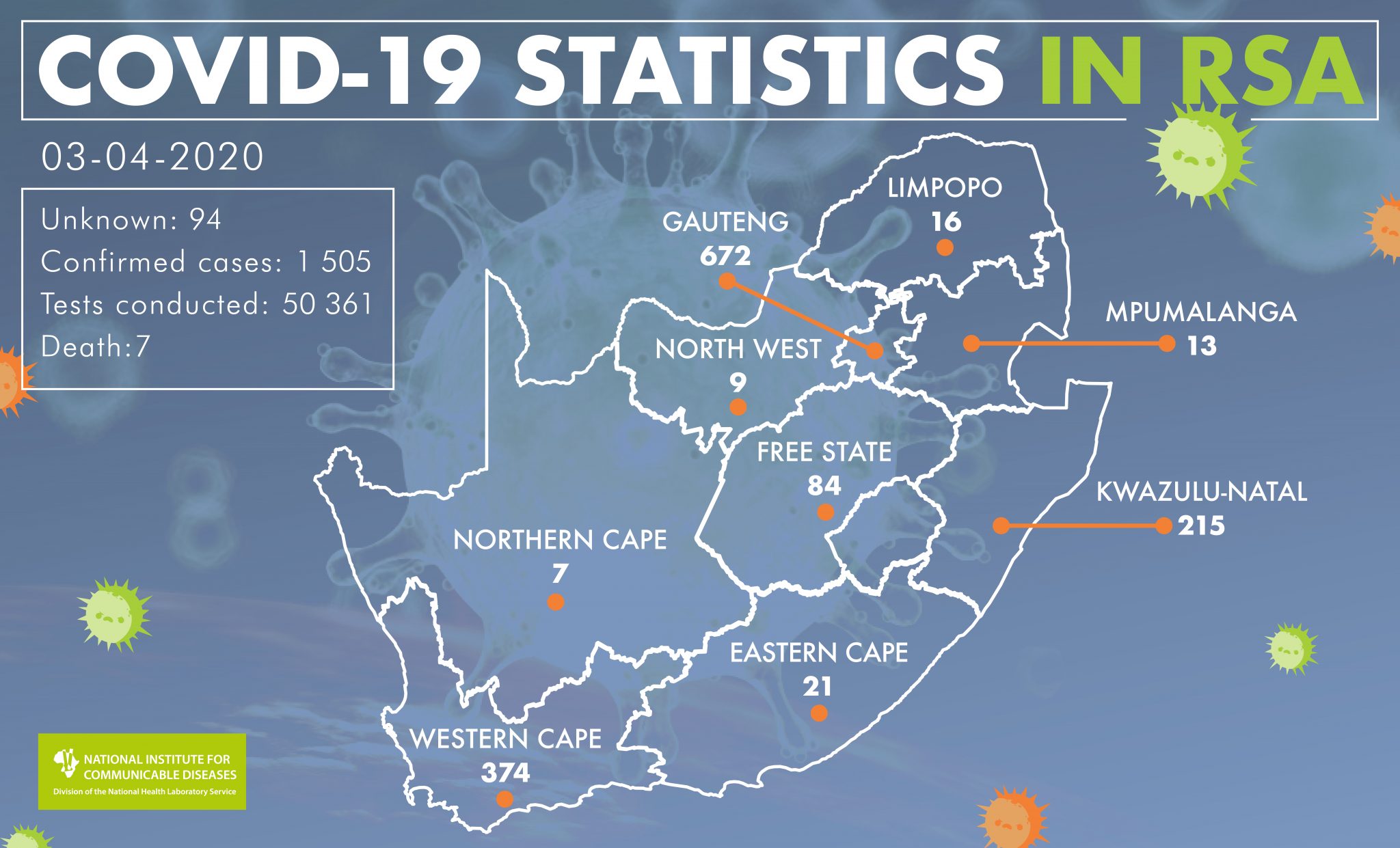{kind=link}