Respiratory Ward - Hydatid Disease

Cases from the Respiratory Ward
Mrs Z.N.
35 yr old farmer labourer from the Kwazulu-Natal province.
Mrs Z.N. presented with a one week history of right sided pleuritic chest pain. The onset was sudden. This was associated with a warm flushing feeling and dizziness. There was also a pain in the right upper quadrant of her abdomen. There was no history of shortness of breath, cough or wheezing. There were no cardiac symptoms, no symptoms of malaise or loss of weight. No history of fevers. She was not a smoker and drank no alcohol. Of note is that she admitted to eating the entrails of the goats that she keeps.
On examination, the patient was not distressed. She was heamodynamically stable and apyrexial. She was not tachypnoeic. She was clinically pale. Examination of her head and neck showed no abnormalities. Her heart was normal. Her chest was tender to percusson and dull in the right base. On auscultation of the right lung, the breath sounds were reduced in the base with a small area of amphoric breathing above the dullness. The examination of the abdomen was normal with no hepatosplenomegaly present. The neurological examination was normal. There were no skin rashes.
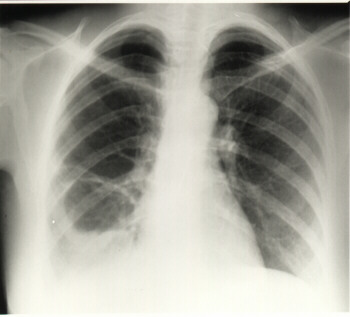
Chest X-Ray revealed;
- A large 7cm cavity occupying the lateral segment of the right middle lobe.
- Its wall thickness varied and it was irregular.
- It contained fluid and air with an undulating, crenated interface.
- Fluid was not present in the right costophrenic angle.
- There was conslidation in the medial segment of the right middle lobe. A diagnosis of a ruptured hydatid cyst was made.
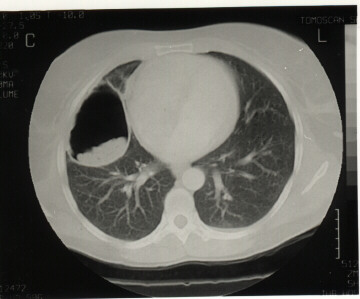
A CT Scan was performed;
- There was an 8x6 cm air filled cavity with membranes in its dependant parts in the RML of the right lung.
- The lesions were clearly seperate from the pericardium.
- The findings were consistant with a ruptured hydatid cyst.
- There was no pericardial effusion and no intra-abdominal cysts.
- The liver was normal.
Blood Tests;
- The full blood count was normal.
- The eosinophil count was slightly raised at 6%
- The hydatid CFT was positive at 1:1024
- Other blood tests were normal
The discussion on the further management of this patient revolved around whether to manage the patient medically or surgically. It was felt that although there was the risk of anaphylaxis and seeding with surgery, surgery offered the best chance for cure. The patient was duly started on albendazole and oral meticorten. She was operated on 10 days later and the cyst was removed without incidence. The patient recovered quickly in the ward and was discharged a week later. She will be followed at out patients and Hydatid CFT s monitored
Further Reading
- Saenz de San Pedro B, Caza?L, Cobo J, et al: Anaphylactic shock by rupture of hydatid hepatic cyst: follow-up by specific IgE serum antibodies. Allergy 47:568, 1992
- Lewall DB, McCorkell SJ: Rupture of echinococcal cysts: diagnosis, classification, and clinical implications. AJR Am J Roentgenol 146:391, 1986
- Wilson JF, Rausch RL: Alveolar hydatid disease: a review of clinical features of 33 indigenous cases of Echinococcus multilocularis infection in Alaskan Eskimos. Am J Trop Med Hyg 29:1340, 1980
- von Sinner WN: New diagnostic signs in hydatid disease: radiography, ultrasound, CT and MRI correlated to pathology. Eur J Radiol 12:150, 1991
- Jerray M, Benzarti M, Garrouche A, et al: Hydatid disease of the lungs: study of 386 cases. Am Rev Respir Dis 146:185, 1992
- Marani SA, Canossi GC, Nicoli FA, et al: Hydatid disease: MR imaging study. Radiology 175:701, 1990
- von Sinner W, te Strake L, Clark D, et al: MR imaging in hydatid disease. AJR Am J Roentgenol 157:741, 1991
- Taourel P, Marty-Ane B, Charasset S, et al: Hydatid cyst of the liver: comparison of CT and MRI. J Comput Assist Tomogr 17:80, 1993
- Gouliamos AD, Kalovidouris A, Papailiou J, et al: CT appearance of pulmonary hydatid disease. Chest 100:1578, 1991
- Kammerer WS, Schantz PM: Echinococcal disease. Infect Dis Clin North Am 7:605, 1993
- Filice C, Di Perri G, Strosselli M, et al: Parasitologic findings in percutaneous drainage of human hydatid liver cysts. J Infect Dis 161:1290, 1990
- Magistrelli P, Masetti R, Coppola R, et al: Surgical treatment of hydatid disease of the liver: a 20-year experience. Arch Surg 126:518, 1991
- Burgos L, Baquerizo A, Munoz W, et al: Experience in the surgical treatment of 331 patients with pulmonary hydatidosis. J Thorac Cardiovasc Surg 102:427, 1991
- Dogan R, Yuksel M, Cetin G, et al: Surgical treatment of hydatid cysts of the lung: report on 1055 patients. Thorax 44:192, 1989
- Morris DL: Pre-operative albendazole therapy for hydatid cyst. Br J Surg 74:805, 1987
- Acunas B, Rozanes I, Celik L, et al: Purely cystic hydatid disease of the liver: treatment with percutaneous aspiration and injection of hypertonic saline. Radiology 182:541, 1992
- Filice C, Pirola F, Brunetti E, et al: A new therapeutic approach for hydatid liver cysts: aspiration and alcohol injection under sonographic guidance. Gastroenterology 98:1366, 1990
- Gargouri M, Ben Amor N, Ben Chehida F, et al: Percutaneous treatment of hydatid cysts (Echinococcus granulosus ). Cardiovasc Intervent Radiol 13:169, 1990
- Khuroo MS, Zargar SA, Mahajan R: Echinococcus granulosus cysts in the liver: management with percutaneous drainage. Radiology 180:141, 1991
- Khuroo MS, Dar MY, Yattoo GN, et al: Percutaneous drainage versus albendazole therapy in hepatic hydatidosis: a prospective, randomized study. Gastroenterology 104:1452, 1993
- Ammann RW, Ilitsch N, Marincek B, et al: Effect of chemotherapy on the larval mass and the long-term course of alveolar echinococcosis. Swiss Echinococcosis Study Group. Hepatology 19:735, 1994
- Wilson JF, Rausch RL, McMahon BJ, et al: Parasiticidal effect of chemotherapy in alveolar hydatid disease: review of experience with mebendazole and albendazole in Alaskan Eskimos. Clin Infect Dis 15:234, 1992
- Aggarwal P, Wali JP: Albendazole in the treatment of pulmonary echinococcosis. Thorax 46:599, 1991