Toward a risk-based strategy for managing the COVID-19 epidemic: A modelling analysis
- Alex van den Heever
Given the protracted nature of the risk posed by the COVID-19, this paper seeks to address the need to match health prevention and a viable economy.
The central premise of this paper is that there are no zero-sum options. By this it is meant that the health prevention strategy most compatible with the maintenance of continued economic activity is an unavoidable policy imperative for South Africa.
This paper addresses this discussion in three stages. First, it examines the factors that should influence the main strategic choices. Second, it examines the consequences of two alternative pathways leading to a preferred approach. Third, it offers an overview of the key features of a preferred approach.
The paper engages with the above through the use of a model (van den Heever, 2020) which attempts to compare alternative health prevention strategies. As a consequence, part of this paper involves a brief write-up of the methodology used.
Introduction
As yet, there are no proven formula to balancing the effort to fight the Covid-19 pandemic with the simultaneous and equally important need to sustain livelihoods and keep open pathways to economic participation. Whereas these objectives are sometimes argued to be in opposition – save lives versus save the economy – crude distinctions are not helpful when facing the complex set of risks implied by the prospect of a protracted struggle to contain the epidemic.
As a preventive strategy for COVID-19, according to emerging experience, mass testing and contact tracing should occur together with social distancing measures, border closures and the observance of health protocols (such as the requirement to wear masks when outside the home) where people cannot avoid some form of social contact. The distinction between the lockdown approach and mass testing and contract tracing is that the former shuts down a substantial part of the economy while the latter is compatible with continued economic activity.
This distinction is an important consideration where the direct effects of a lockdown disproportionately harm vulnerable workers and businesses. While Government can attempt to support the vulnerable, the extent to which this is possible depends on whether the institutional mechanisms exist to identify compromised individuals and businesses sufficiently for them to be supported. It also depends on the length of time for which support is required. The longer the period, the harder it is to keep businesses open, and the harder it is to raise the tax revenues and the debt required to finance support for vulnerable individuals.
In the early phases of the COVID-19 outbreak, it is clear that Government lacked the capabilities to introduce the most effective strategy. The need for urgent action left no opportunity to scale up the measures required to prevent an exponential increase in infections. South Africa was just not geared for an epidemic of this nature. Consequently, the 21-day lockdown implemented on 27 March 2020 was appropriately timed and self-evidently essential.
The extension of the lockdown for a further two weeks however raises important concerns. Two implications can be drawn. First, the extension suggests that the lockdown period has not been adequately exploited to ramp up the testing and contact-tracing regime. Second, it indicates that the narrow testing regime adopted to date (designed to merely identify imported infections rather than community-based outbreaks) cannot be relied upon to confirm whether the lockdown has succeeded outside of the affluent communities where the epidemic started.
While the two-week extension could be argued to provide some breathing space for the implementation of the preferred strategy of mass testing and contact tracing, any continued failure to put in place the required machinery will result in incremental extensions to the lockdown with all the economic and social consequences that will go with it.
An obvious further concern with this trajectory is the high likelihood that a successful lockdown within the South African context is essentially a leaky bucket. While it may prove effective in the more affluent suburbs, it may fail in the townships and informal settlements. The current lockdown may have therefore only reduced, but not prevented, the spread of the disease into the general population. Although these infection levels may be relatively low at present, it won’t take long for them to become uncontrollable.
Background
The pandemic resulting from the SARS-COV-2 virus has elicited an emergency response from virtually all countries around the world. The high levels of transmission, taken in this analysis at 2.5 (over a period of four days)[1] for every infected person, would not be a serious concern if the disease (COVID-19) did not also result in sufficient severity for a proportion of the infected population to require hospitalisation, and, more importantly, access to ventilators that are typically only located in intensive care units (ICUs).
Where ventilators are not available for those who need them, the health outcome will be death. For those that require access to ventilators and obtain treatment, over 70% will in any case die. Patients who develop severe symptoms appear to be associated with weaknesses in the immune system, either due to age or co-morbidities typically correlated with age (hypertension, diabetes, and various cardiac conditions). People with co-morbidities associated with the respiratory system are also at risk regardless of age.
Given this context, to avoid significant preventable levels of morbidity and mortality, the most efficient approach to reduce the spread of the disease is to reduce the reproduction rate of the disease (referred to as R) from 2.5 to below 1 (the rate at which the disease will ultimately be eliminated). This is achieved through various interventions, the most effective being the introduction of a vaccine to a sufficient number of the population such that herd immunity is achieved.[2]
Where a vaccine is not available, and the mortality would be too high to permit herd immunity to occur naturally, the only option is to actively interrupt the spread of the disease from person to person such that R is held below 1 for a long enough period to eliminate the disease. Quite simply, such strategies involve keeping infected people away from uninfected people.
There are two broad options. Either infected people are identified quickly and isolated; or, where infected people have not been identified quickly enough, everyone is separated from everyone else for a sufficient time for the disease to self-eliminate. In practice strategies involve a mix of associated interventions.
Internationally, two distinct approaches have emerged. The first is to test, trace and quarantine at scale. The second, involves a generalised lockdown on the movement of people. The first option tends to be exercised by countries that are well-prepared and intervene at scale at early stages of the epidemic. The second, tends to be applied where countries are poorly prepared to react, and a runaway community-based epidemic is well underway before interventions are considered.
South Africa’s response to the emerging pandemic was slow at first, with no border closures considered, and only very basic forms of border screening applied at airports. Given that we knew early on that many infectious persons are also asymptomatic, this approach was ill-advised and exposed the country to the inevitability of imported infections.
This (arguably) casual response to the emerging pandemic changed when the first cases were diagnosed in South Africa in early March 2020 and also where it had become evident that many other countries were experiencing full-blown epidemics arising from imported infections.
Evidently informed by standard epidemiological modelling of the emerging epidemic, aided by a wealth of information collated by international researchers and the World Health Organisation (WHO), the South African government acted immediately to implement social distancing, followed on 27 March 2020 by a generalised lockdown. However, as the modelling has never been made public, it is unclear what scenarios were presented. Needless to say the analysis was clearly compelling at the time.
The lockdown was however implemented at an early stage of the epidemic, as there was very limited evidence at the time of a generalised community-based outbreak.[3] This differs from some other countries where lockdown approaches were introduced only when they had lost control of the epidemic and they were all out of options.
However, the countries that avoided lockdowns and managed their epidemics did this through rapid border closures, the rapid development of tests for the disease, generalised testing with rapid turnover (12 to 24 hours), contact tracing and quarantining of infected individuals.[4] Broadly speaking their approach can be characterised as getting ahead of the disease rather than chasing it.
Consistent with countries that have not been able to manage their epidemics, South Africa also adopted the testing regime characterised as “chasing the epidemic”. It did not test the general population, or even those with mild symptoms. Instead it tested only people who had travelled internationally (when they came forward voluntarily), had contact with a traveller or had contact with someone diagnosed with COVID-19. This effectively blinded the testing regime to community-based outbreaks. In addition, the testing programme was so constrained that the public sector had only performed 3% of the total tests, with the remainder performed by the private sector. This has apparently changed, with more generalised testing on the increase, although still low.
So what does this mean for South Africa’s strategy going forward?
- First, we are left without a clear measure of the success or failure of the lockdown. On the one hand we cannot fully trust the incidence reports. On the other hand, the mortality levels appear consistent with a contained or low-level epidemic.
- Second, the economic consequences of a lockdown are so large, that it cannot be relied upon as the principle prevention strategy if the epidemic is protracted. This requires that a health strategy compatible with reopening the economy is imperative.
- Third, the public reports on readiness by the public health team to implement a benchmark strategy are unclear at best, and suggest undisclosed challenges regarding readiness. The question is whether the bottlenecks to a more nuanced strategy can be rapidly addressed.
How effective is a generalised lockdown?
Of considerable concern is the possibility that a generalised lockdown approach applied within the South African context will only be successful in relatively affluent communities, with townships “unlockdownable”.
As mentioned above, the testing protocol applied to date has been biased toward (implicitly) measuring the (imported) outbreak in affluent communities. The publicly reported new infections would therefore accurately reflect the lockdown impact on the relatively affluent population, but not on outbreaks in the general population.
The apparent containment of the epidemic in affluent communities is therefore potentially misleading. It can create the impression that the lockdown is working (false evidence of success), but it may equally fail to offer the required evidence that a generalised lockdown cannot work successfully in South Africa (false evidence of failure).
As the outbreak in South Africa derived from the affluent population, as they tend to travel internationally, the initial lockdown was probably the best available strategy to block transmission from the affluent communities to the population at large. However, to the extent that the population at large has been infected, a general lockdown may prove equivalent to no intervention.
As a form of contingency planning for the South African context, therefore, the following should be noted:
- A lockdown may be a viable prevention strategy, but different approaches would be required for different contexts (i.e. what works in relatively affluent areas may not work in townships or informal settlements); and
- An undetected outbreak may have already occurred in the general population which is invisible to the current testing regime (noting that there are significant moves to expand the testing protocol and programme).
Given the need for a “must not fail” health prevention strategy, it makes sense to prepare for what will work in all scenarios, rather than an approach which will only work if we are very lucky.
Strategic options
Important considerations
There remains considerable uncertainty as to whether the pandemic can be completely eliminated during 2020. Strategies that are successful in bringing country-level epidemics under control therefore face the realistic prospect of a resurgence for an extended period of time. Within the South African context this requires that effective containment of the epidemic will require public health interventions of one form or another throughout 2020.
The need to maintain public health interventions for such an extended period of time therefore has important implications for the design of the 2020 strategy. A brief public health crisis addressed through emergency interventions can be expected to have a different design to a protracted affair. However, if the state of readiness is not adapted to reflect the protracted nature of the crisis, the strategy may unwittingly default into treating the protracted crisis as a series of brief crises.
Two clear strategic options emerge. The first defaults back to generalised lockdowns when surprised by a resurgence, and the second actively manages all the risks associated with a protracted epidemic.
- Option 1 – Lockdown dependent approach, where the lockdown is extended on some basis after the 35-days as the central pillar of any response to contain the epidemic; and
- Option 2 – Risk-based strategy, where a prevention strategy compatible with the local domestic social context and a safe re-opening of the domestic economy is pursued.
A brief description of the methodology required to model the above two options is outlined below.
Method
Approach
The options are examined using a model, the COVID intervention model (van den Heever, 2020), to determine the length of time a particular public health intervention package needs to be in place to keep the local epidemic controlled for the entire 2020 period.
Generating parameters from international contexts
This section examines the trajectories of various country epidemics following the introduction of major prevention strategies and uses them to calibrate the model. First, a range of countries are reviewed to identify those that may exemplify particular interventions. Second, from those countries two are selected, that best reflect a lockdown intervention and a mass testing and contact-tracing intervention.
The selection criteria for the group of countries was based on: those with significant epidemics (United Kingdom, Italy, Spain)[5] that are engaging in lockdowns; countries that have experienced significant epidemics and have successfully contained them using lockdowns (China); and countries that avoided lockdowns through early interventions that made substantial use of mass testing and contact tracing (South Korea).[6] Data on new infections is examined in each country after the first 100 cases.[7]
An attempt is made in Figure 1 to compare all five countries.
The patterns for the three European countries are strikingly similar on the upward trajectory. As the countries are at different stages in their epidemics, only two of them, Italy and Spain, show a downward trajectory after the introduction of the lockdown. The United Kingdom is yet to reach a turning point (at the time of writing this brief). The post-lockdown downward trajectory for China is however a lot steeper than Italy and Spain, and is as steep as that achieved by South Korea using mass testing and contact tracing.
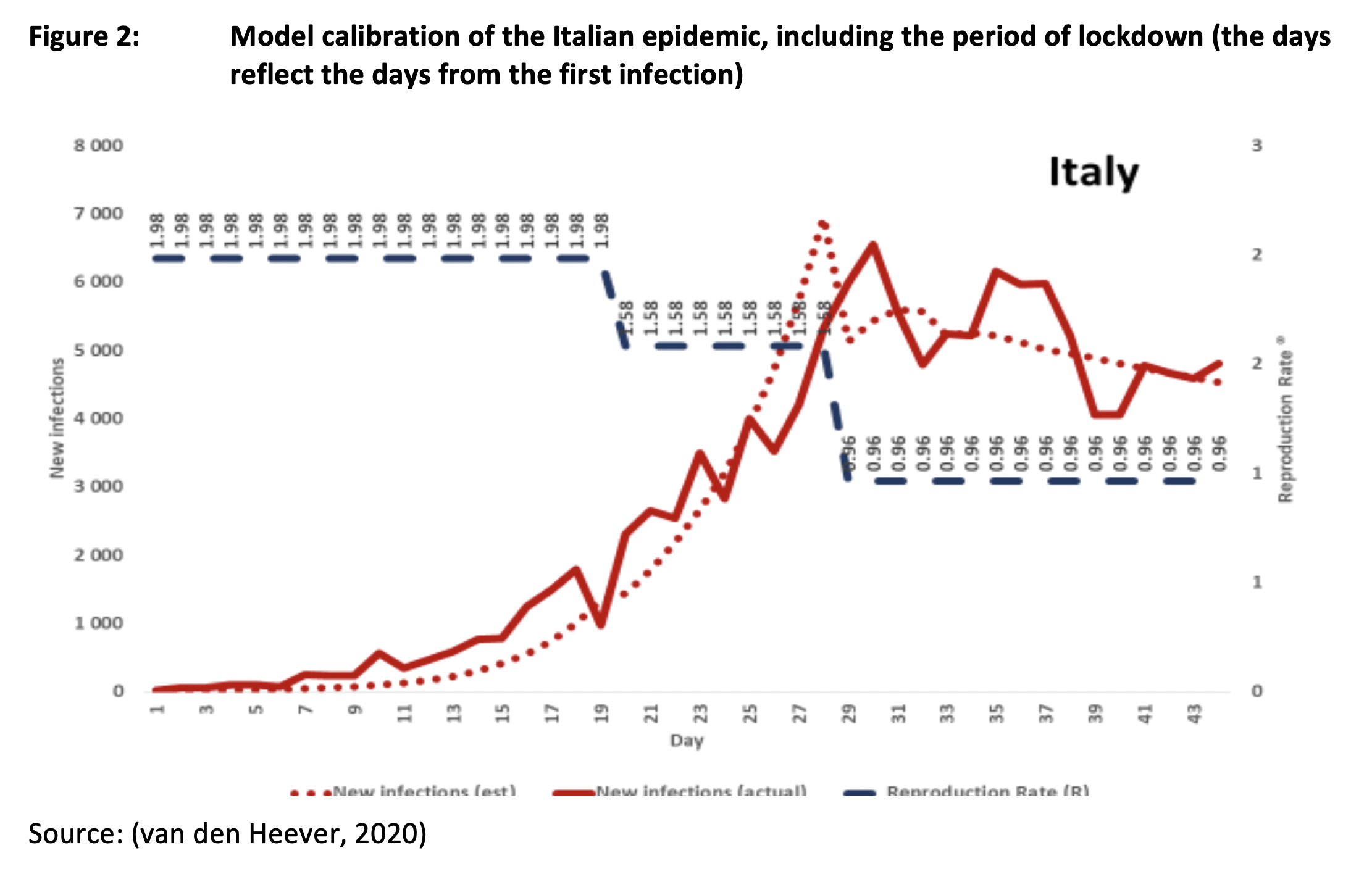
The lockdown trajectories for Spain and Italy are consistent with a relatively high R, although still less than one. The implied intervention Rs for South Korea and China are however more pronounced. It should however be noted that the both Spain and Italy intervened at a very late stage in their epidemics, which may have complicated their outcomes in ways that are not yet understood. With China, there is a question concerning the reliability of their reporting.[8] As a consequence, for the purposes of parametrising the model, it makes more sense to use the more conservative trajectory consistent with either Italy or France. As Italy effectively has a longer time series, it is therefore preferred over France for this purpose.
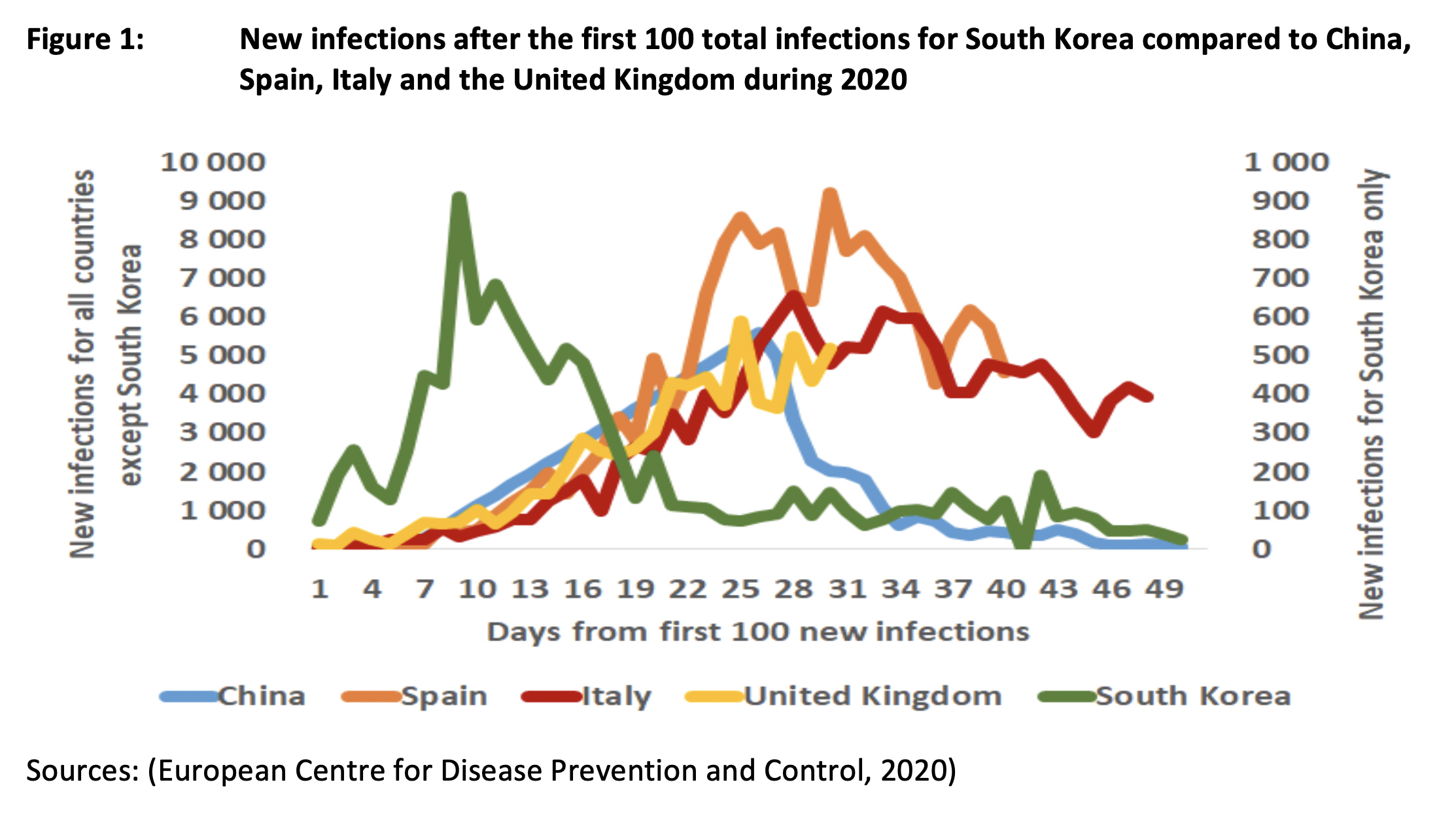
Figure 2 illustrates the Rs that best match the Italian epidemic, both before and after the lockdown intervention. Here different values of R are used to drive a model result that is close to the actual trajectory of all phases of the epidemic. This suggests that a lockdown in cold weather is broadly consistent with an average R of 0,96. The early stages of the epidemic are consistent with an R of 1.98, dropping to 1,58 as a consequence of initial, but inadequate, interventions. The lockdown R is however quite close to 1, suggesting a fairly tenuous impact.
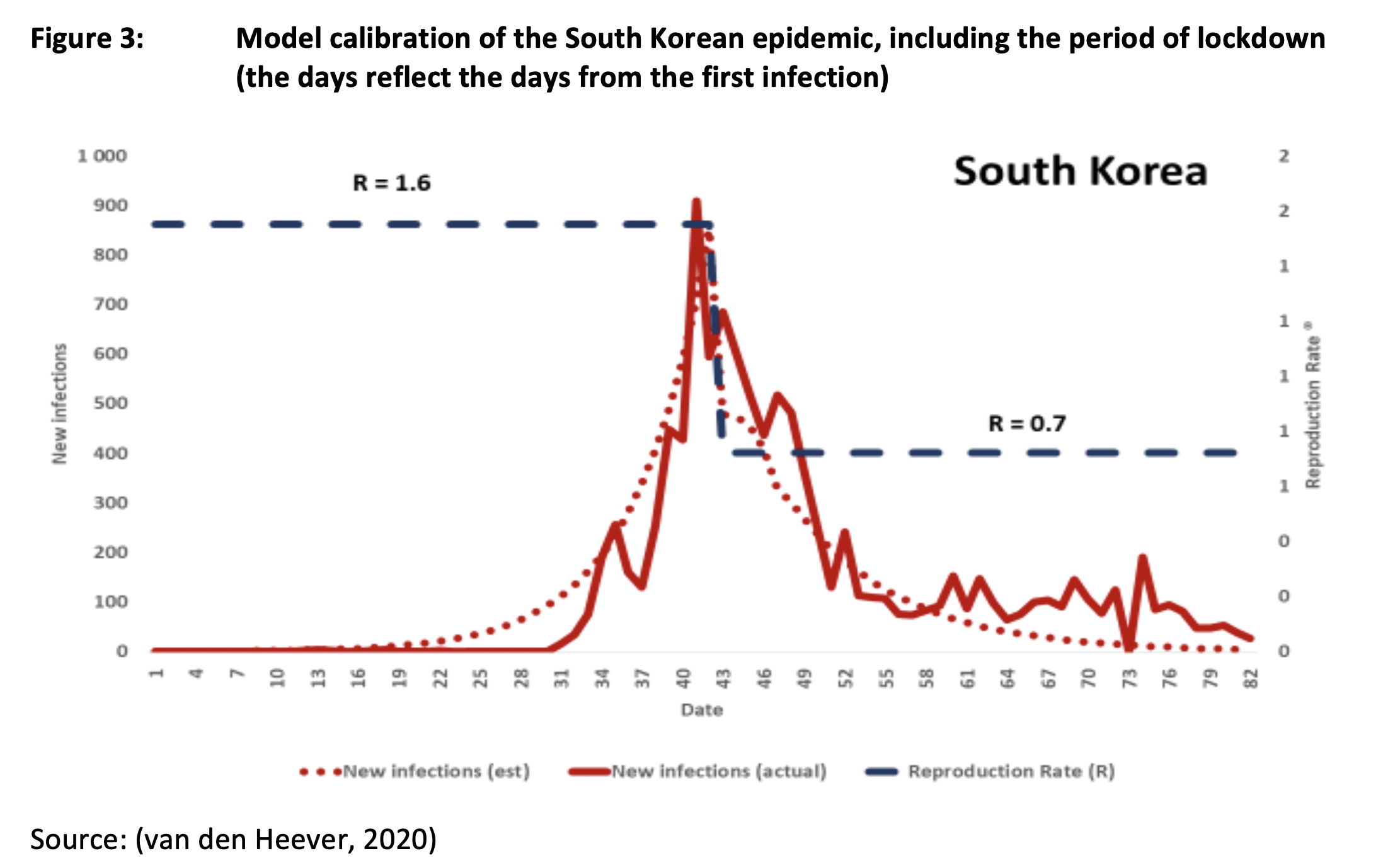
An estimate of the R consistent with the South Korean mass testing and contact tracing intervention is provided in Figure 3. The period prior to the main public health intervention is consistent with an R of 1.6, while the mass testing and tracing intervention results in an R of 0.7 in cold weather. This is a superior result relative to protracted lockdowns in Italy and France. This could be the result of many factors, such as, inter alia, the early stage of the intervention and the efficiency of a well-prepared country response. It is therefore possible that other countries may not implement the same response with the same efficiency. This is however not taken into account in the parametrisation for this exercise.
The intervention packages used by both Italy and South Korea however extend beyond lockdowns and mass testing and contact tracing. For instance, all include border closures, social distancing requirements (including requirements to wear masks when outside the house) and targeted lockdowns (to address disease clusters). The intervention packages generated through the parameterisation exercise take this into account. This is discussed further in the next section.
Model parameters
This section provides an indication of the model parameters used, guided by the analysis of Italy and South Korea discussed above.
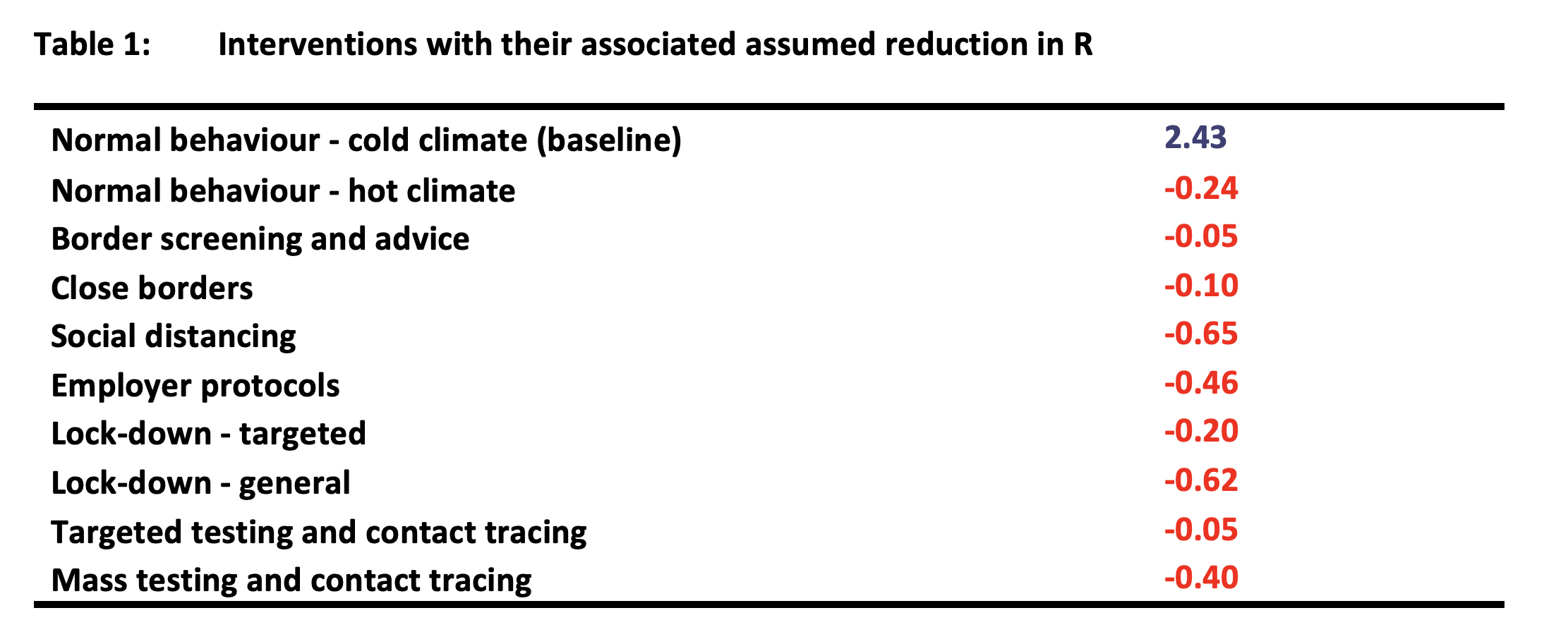
The model parameters are specified at three levels. First there are individual interventions, each with an associated reduction in R (Table 1).[9] Second, there are combinations of interventions, or packages, each resulting in an aggregate R (Table 2). Third, there are scenarios over the 2020 period, where different packages are applied by day of the year, depending on the seriousness of the epidemic.
It is important to note that the Rs for the individual interventions do not have a strong empirical basis. The true test of their usefulness is therefore how well they match the South African epidemic thus far when combined within packages of responses (i.e. no intervention occurs in isolation of some others). To the extent that they do, they can be used to estimate the trajectories resulting from different packages over the full 2020 period.

As indicated in Table 2 there are five overall response levels provided for, from level 0 (L0) (do nothing) to level 4 (L4) (lockdown). There are two versions of each response level depending upon whether or not it occurs in warm or cold weather conditions.
For the purposes of this analysis the package configurations associated with a general lockdown (L4) and mass screening and contact tracing (L3) reflect the outcomes in Italy and South Korea respectively discussed above.
Mass screening and contact tracing is treated as a level 3 (L3) intervention as this is naturally prior to the full lockdown – at least for countries with well-prepared public health response systems. South Africa’s adoption of a level 4 (L4) response before level 3 is assumed to have occurred because it was not prepared for the epidemic and was therefore not in a position to implement mass testing and contact tracing in the natural sequence of escalating responses.
The application of the parameters to the South African epidemic
This section discusses whether the parameters developed for the model are able to predict the known part of the South African epidemic.
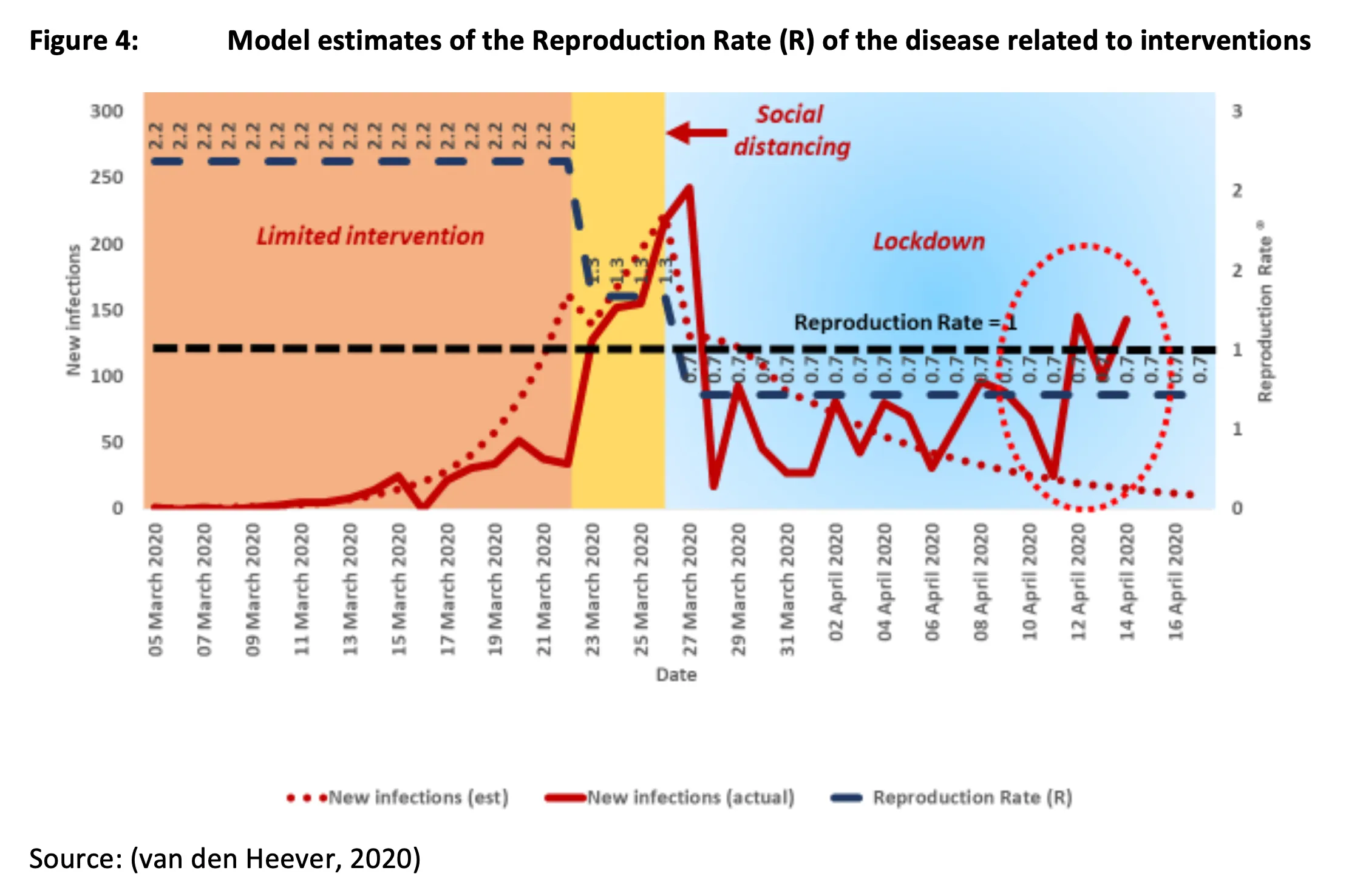
Figure 4 illustrates how interventions associated with assumed reproduction rates (R) generate estimates of new infections for the periods where we have reported information on new infections.
Three intervention packages are applied to specified periods broadly in accordance with actual events.
- First, there is the “limited intervention” from the early period of March 2020 to around 22 March 2020, which has an R of 2.2.[10] Here it is assumed that no meaningful public health prevention intervention is in place. The value of R is reduced to account for the warmer climate.
- Second, there is stepped up “social distancing” (referred to above as a level 2 (L2), or “intermediate”), which occurs from 23 March 2020 to 26 March 2020, with an associated R of 1.6.[11] This period includes the closure of international borders, schools and universities.
- Third, is the 27 March 2020 “lockdown” intervention package, which has an associated R of 0.7 (which is lower than that for Italy to account for the warmer weather). The lockdown period includes the social distancing interventions and border closures. It therefore has the deepest overall impact.
Figure 5 shows that the warm weather and social distancing interventions on their own do not bring R below 1.0 (the rate at which the disease will dissipate). The R of 1.3 for this period therefore appears justified.
The lockdown intervention does however appear bring R to below 1.0, apart from the most recent reported infection data. There is therefore some uncertainty about the trajectory of the lockdown. Whereas during the initial period of the lockdown the reported new infections went into decline as expected, the trend from 29 March onward could be regarded as ambiguous. While the model suggests a more pronounced decline, the actual trend could be consistent with a range of Rs from 1.0 to 0.6.
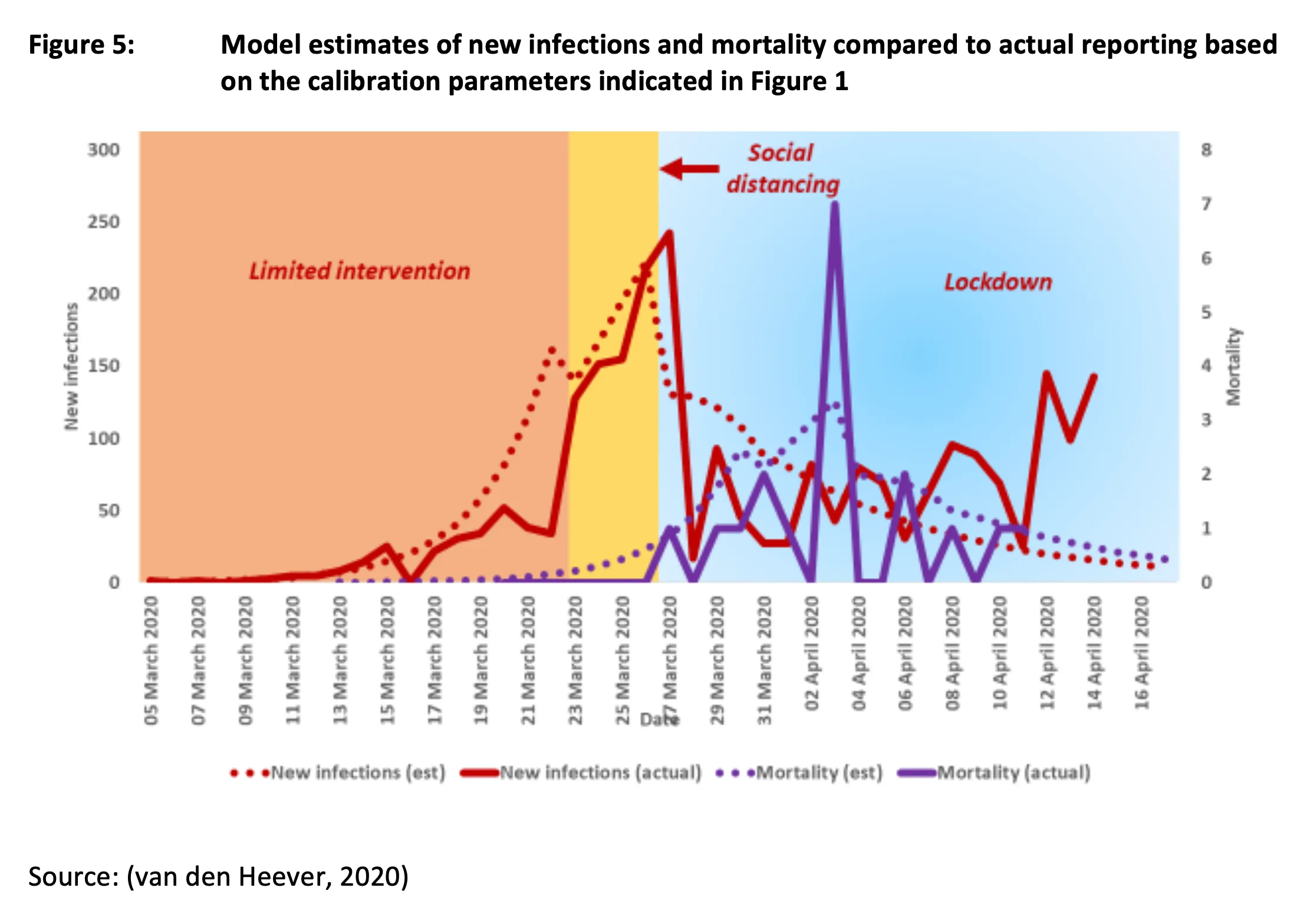
One possible interpretation is that the lockdown, in context, is not sufficient to eliminate the disease. Consistent with this possibility, this trend (i.e. relatively flat after the initial decline) could reflect a transition from the imported outbreak in the affluent community to a domestic community-based outbreak in the general population. While the former may be sensitive to a lockdown, the latter may not, with an R greater than 1.0 even with the lockdown. This period could therefore reflect a simultaneous decline of one outbreak with an increase in another.
Nevertheless, based on information to date, and using the data from the Italian epidemic, an assumed R of 0.7 for a lockdown with warmer weather appears (for now) consistent with the reported information. Using the model to estimate the effectiveness of the Italian lockdown produced an R of 0.96 for winter. The 0.7 assumption used for South Africa includes an adjustment for warm weather and is therefore only applied to the remaining days of summer. The cold weather assumption is applied during winter.
Scenario results – options for 2020
Overview
Two scenario options for 2020 are examined here. Option 1 involves a lockdown-dependent strategy, where any surge in the epidemic involves the package associated with a general lockdown (L4). Option 2 however limits the use of a lockdown to the period already designated for lockdown in South Africa. Thereafter, it reverts to periods of mass testing and tracing (L3), with periodic reversions to L2 (intermediate interventions). Both options are required to eliminate the risk of a serious epidemic during 2020.
It is important to note that the model results are stylised reflections of the trajectory of the epidemic and unknown real world factors would also be expected to play a role.
Option 1 – Lockdown-dependent strategy
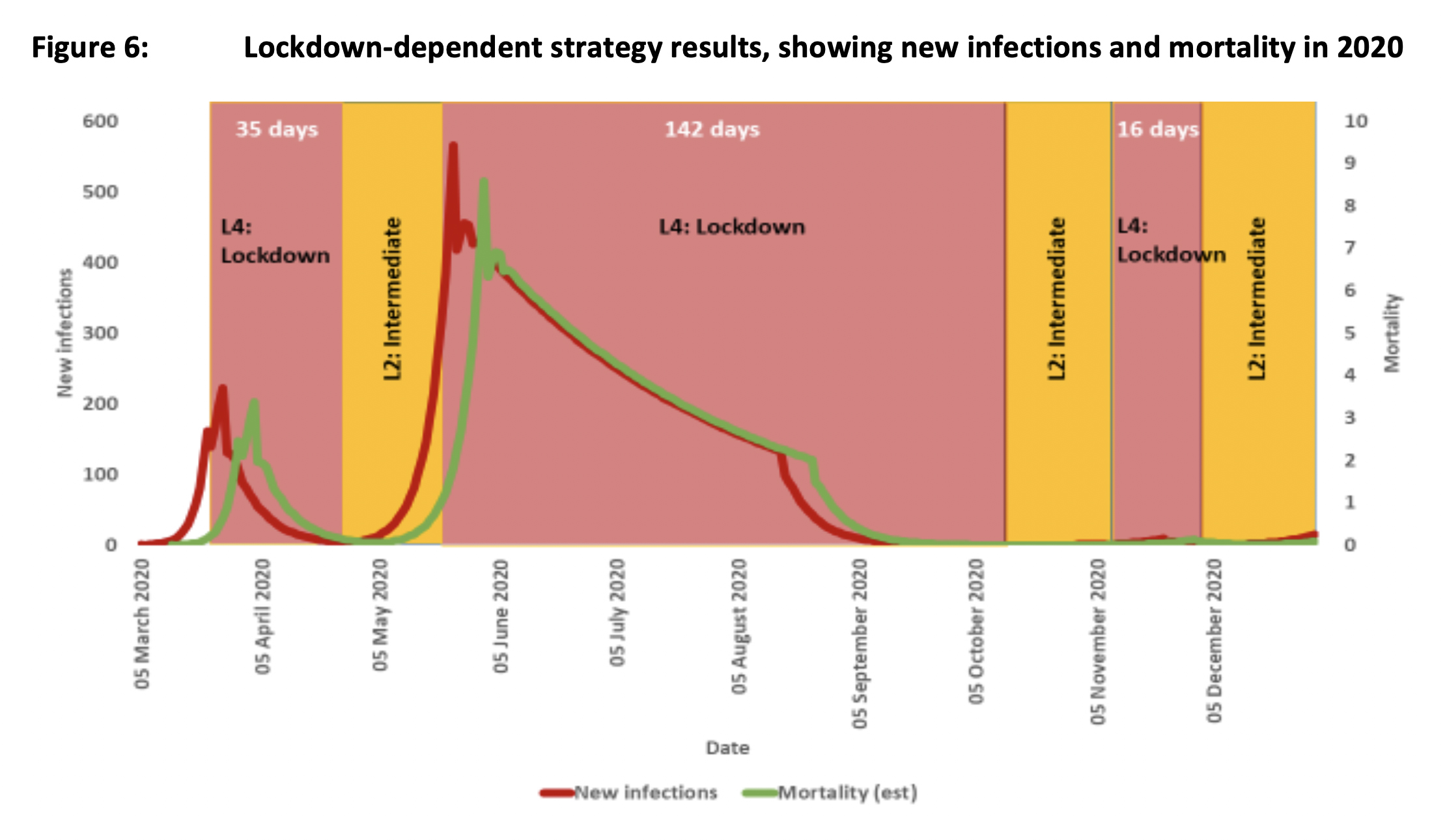
In this scenario option the lockdown is permitted to end from 1 May, with a reversion back to an intermediate intervention package. However, according to the model, the disease resurges and requires a further lockdown toward the end of May, extending all the way to October (Figure 6). During October an intermediate package is implemented. A further lockdown of 16 days is required in November/December to prevent a further resurgence. The required overall number of days for lockdowns is 193 days.
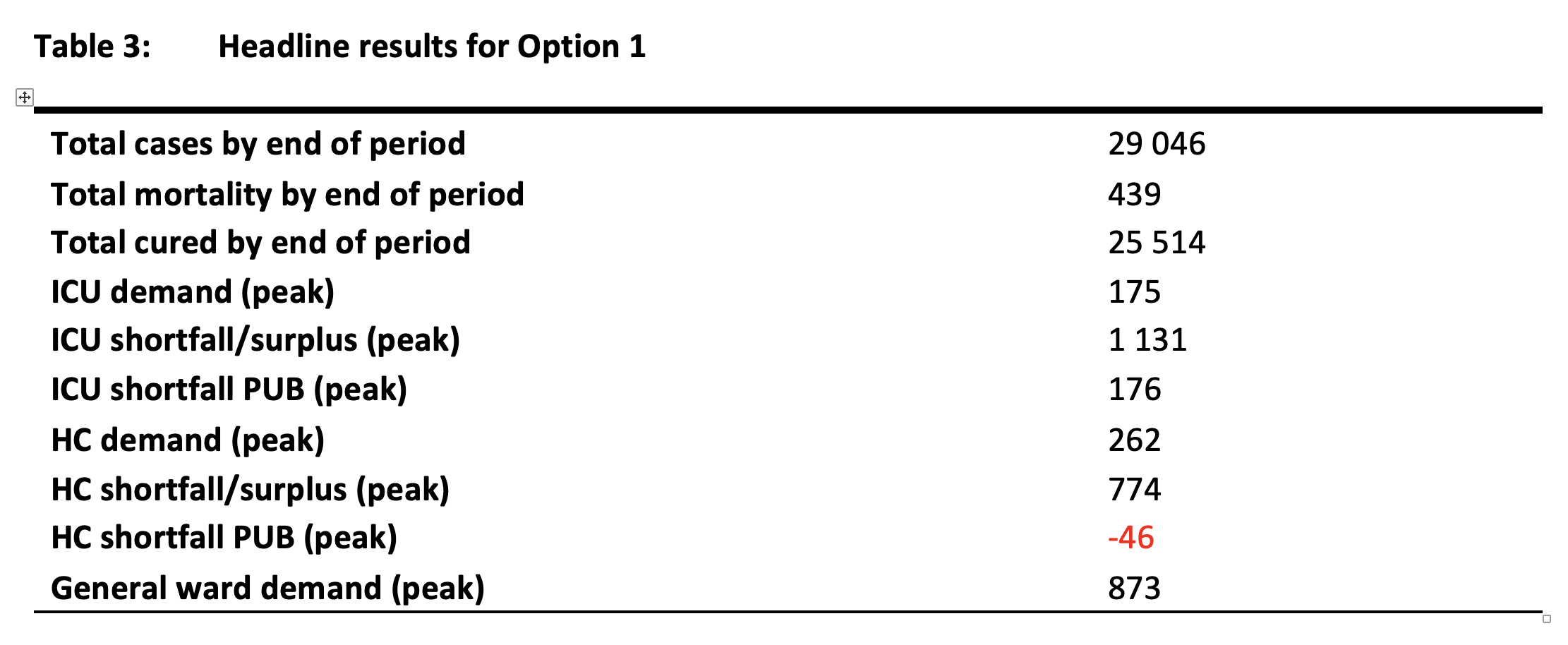
The headline results, reflected in Table 3, are consistent with an overall strategy that keeps the epidemic in check for 2020. In total 29,046 people test positive with mortality of 439. The demand peak for ICU beds (used as a proxy for ventilators) is 175, which would be well within the capability of the overall health system. There would only be a slight risk of insufficient High Care (HC) beds in the public sector. When seen together with the private sector capacity and the timely reorganisation of public sector beds, there are sufficient beds.
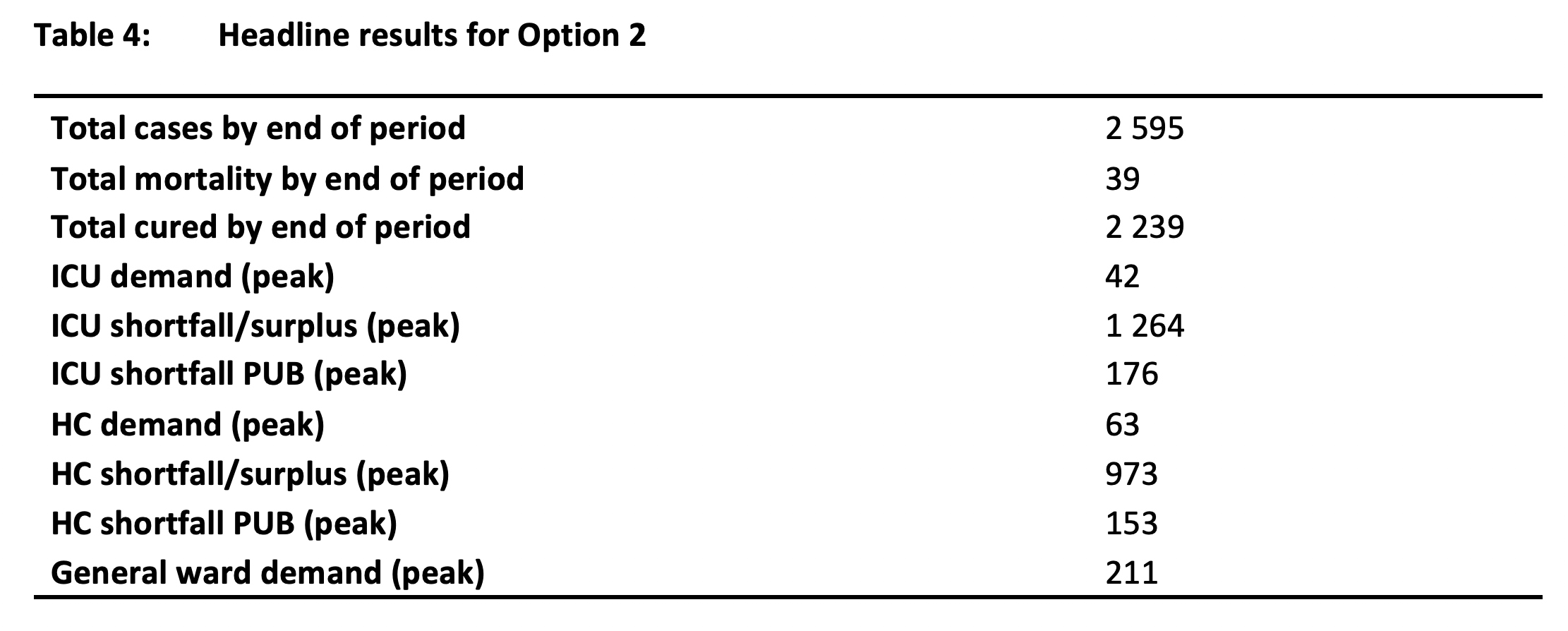
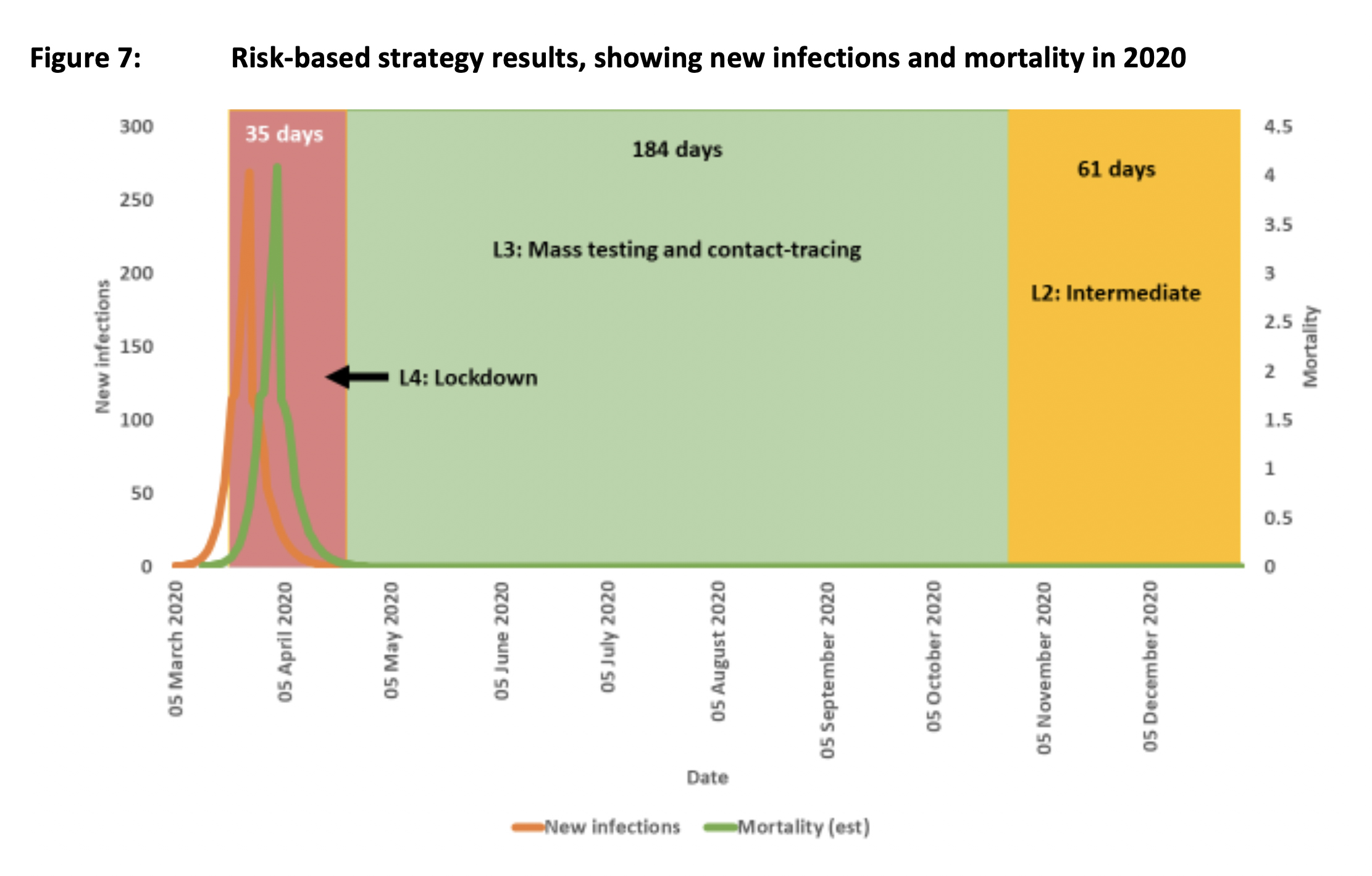
Option 2 – Risk-based strategy
The risk-based strategy looks to minimise the use of lockdowns as the primary measure required to bring the epidemic under control. Although it retains the lockdown as implemented to date from 27 March to 30 April, it moves to an aggressive mass testing and contact-tracing regime thereafter. This lasts until the epidemic is brought under control. In total there are 35 days of lockdown, 184 days of mass testing and contact tracing and 61 days of the intermediate package. (Figure 7)
The headline results shown in Table 2 reflect the total containment of the epidemic, with only 2,595 people infected and total mortality of 39. It should be noted that the actual trajectory of the disease could take the overall totals over these numbers by the end of April. These estimates should therefore be treated as indicative of a direction rather than offering a predicted outcome with a high level of specificity. This scenario indicates that bed demand is kept low, and no crisis of access to critical care beds would materialise. The demand for ICU beds peaks at the relatively low value of 43, with High Care at only 63.
Discussion of results
Both options modelled contain the epidemic, and, to that extent, reflect equivalent levels of success in the management of the health crisis. The differences in headline results (reported in Tables 3 and 4) should be disregarded, as they reflect an artificial structuring of option 1 – to fit a pattern of reverting to lockdowns when the disease resurges. Option 1 could also be structured without significant resurgence. This would however require a slight increase to the number of lockdown days.
The main result from this exercise is the number of days required to control the epidemic in 2020 using lockdowns as the primary intervention package. In total, the requirement for 193 days in 2020 is significant, and raises serious questions about the sustainability of this approach as the default strategy. While an economic analysis would provide concrete information on the implications for South Africa’s gross domestic product (GDP) of option 1, it is self-evident that this option would be ruinous.
The model indicates that the epidemic will resurge after a lag when the most effective interventions are withdrawn. In the real world, a resurgence would occur if merely one asymptomatic positive case was left in the community, or where a failure to eliminate the pandemic internationally resulted in a single undetected imported infection. In the former instance, the resurgence would be expected to be faster than the model suggests (as the model trajectory escalates based on fraction of a residual single person).
Given the protracted nature of the public health risk, the analysis suggests that an economically viable health prevention strategy will be required for most of 2020. As the implications of option 1 cannot be shouldered by the South African economy, the selected health strategy should be designed to be compatible with as broad an opening of the economy as is possible. Under these circumstance, a strategy broadly consistent with option 2 appears necessary. The specific features of such a strategy are broadly outlined in the next section.
Features of a risk-adjusted strategy
Overview
The COVID-19 epidemic poses a complex set of risks for South Africa over-and-above the morbidity and mortality associated with the disease itself. The knock-on effects of border closures, restricted movement and closed businesses, if not well addressed, will have long-term consequences for the economy.
While it could be argued that economic considerations should not be given precedence over health risks, in reality economic failure on the envisaged scale will have serious short- and medium-term implications for society at large, well before we get to the long-term. Shocks to employment levels will shift many into poverty, including many who were on a pathway out of poverty.
While Government could provide an economic bridge for some (but not all) where the periods of economic closure are limited, protracted lockdowns and business closures will result in a fiscal death spiral, with tax revenues falling precipitously while expenditure commitments rise precipitously.
The only viable pathway out of the COVID-19 crisis is therefore to integrate the health and economic strategies into a single all-of-government approach. This requires a total strategy of Government – one that is weighted proportionately to address the principal risks facing the country at this time.
There are five strategic considerations to such an all-of-government risk-adjusted approach.
- First, the health prevention strategy must be organised with two objectives in mind: first, it must be compatible with an opening of the economy; and second, it should be designed to have positive economic spinoffs.
- Second, social programmes aimed at income protection, such as social grants and unemployment insurance, should be implemented at scale to simultaneously address social protection needs and the need for domestic economic demand stimulation.
- Third, non-health-related economic strategies need to address the shocks to both the demand and supply sides of the domestic economy.
- Fourth, those parts of the strategy that require ongoing rapid decisions and the deployment of resources need to be supported by an all-of-government command structure that is fit-for-purpose.
- Fifth, all parts of the strategy require rapid feedback on performance and constant useful public communication.
Once the only viable strategic approach has been determined by Government, it has to adopt it together with all the associated interventions with a high degree of urgency, commitment and adaptability.
An indicative approach to the health prevention strategy
This section provides a brief overview of a strategic approach to the risk-adjusted health prevention strategy. This involves a five-level response framework, a post-lockdown approach, transparency requirements and the achievement of operational integrity.
Five-level response-framework: Consideration should be given to a formalised five-level response framework for this epidemic and all future epidemics. The lowest level would be activated when an epidemic risk is identified. A set of pre-prepared responses would then be triggered. Each subsequent (triggered) level would involve increases in risk and urgency. A lockdown would only be considered as a last resort (last level) if the interventions in the previous levels fails to cope.
South Africa should have had a level 3 option, mass testing and contact tracing, but was not adequately prepared. As a consequence, arguably two levels were skipped, at great cost to the economy. While this may be seen as a long-term issue, it is relatively easy[12] to implement in the current crisis, and would prove to be a useful tool for decision-making in 2020. This is because there may be a need to move up and down levels all through the year depending on the success or failure of a response level. These movements up or down could also be area or cluster-specific, rather than seen purely at a national level.
- Level 0: Routine surveillance of risks. When there are no threats, redundant capacity in infectious disease responses needs to be readied. This can involve: the identification of quarantine sites; the maintenance of contact-tracing machinery; and the preparation of a legislative framework for infectious disease outbreaks. This legislation should, inter alia, cater for emergency test development, requisitioning of equipment, rapid contact-tracing frameworks and preparations for mandatory quarantining of suspected and confirmed cases. Both public and private hospitals should be required to maintain a minimum number of isolation wards.
- Level 1: Trigger – identification of a threat, by which is meant a highly infectious disease with significant morbidity and mortality. This may involve: the implementation of a central response platform for Government; the development of tests; the identification of possible shortfalls in testing equipment; the preparation of treatment facilities; the maintenance of basic border surveillance; the identification of high risk transport routes; mandatory testing and quarantining for people from high risk zones; the establishment of testing machinery for all persons presenting with symptoms; and where no test has yet been developed, suspected cases should be quarantined for appropriate periods. In all this, it would be important to coordinate with the private health system to agree on aspects that require a joint response.
- Level 2: Trigger – imported infections identified together with first community-based infections. This would involve: border closures, together with mandatory across-the board testing and quarantining of travellers entering the country; the mandatory wearing of masks (if the disease has an airborne elements; mandatory social distancing; and mandatory (pre-prepared) health protocols implemented at workplaces, transport hubs and bulk transport; the temporary closure of schools and universities; the prohibition of mass meetings of any form (funerals, church gatherings, etc.); and an expansion of the testing framework to be able to detect community-based infections.
- Level 3: Trigger – significant increase in community-based infections, but below 100. In addition to the level 1 and 2 interventions, implement mass testing and contact tracing, together with the quarantining of suspected cases and those identified as positive. This testing regime supplements the testing of suspected cases introduced from level 1.
- Level 4: Trigger – community-based infections continue to increase exponentially. This would involve: general lockdowns initiated in areas with identified disease clusters; the closure of all non-essential businesses; and the closure of all bulk transport systems.
Post-lockdown health strategy: It is imperative that from 1 May 2020 South Africa is ready to implement a health prevention strategy that allows for a measured and safe movement from a level 4 response framework to level 3. The key elements of this approach could be expected to include:
- Mass testing and contact tracing. This needs to be complemented with the rapid identification and follow-up of outbreak clusters.
- All laboratory results must be available within 12 to 24 hours after the test.
- Ambulances need to be in place for the transportation of confirmed cases.
- At all times doctors, nurses and paramedics working in clinical areas should wear three layered surgical masks as well as gloves. Where close contact with patients are anticipated, full PPE is required, including N95 masks.
- Health protocols must be developed for all organisations. A compliance framework to ensure adherence is also required.
- Health protocols are required for all transport hubs and all forms of mass transport.
- Health protocols are required for all places of education.
- A distance learning framework needs to be developed for scholars without appropriate access to the internet and online teaching platforms.
- Health protocols are required for social grant collection sites. This includes sites for food parcel distribution. These are also appropriate sites for mass testing and the distribution of masks.
- The general public requires access to basic methods of personal protection. This includes hand sanitisers, masks (reusable) and gloves.
- During the entire period of the emergency, it should be mandatory for all to wear a mask outside of their homes.
Transparency
The successful pursuit of a public health strategy relies on a high degree of voluntary consent to comply with appropriate public health measures as well as personal preventive conduct. In addition, researchers and businesses constantly need to make sense of the epidemic. This requires that detailed information on the trajectory of every aspect of the epidemic needs to be made public. Furthermore, the actions taken by Government need to be justified through the disclosure of the information upon which major decisions are made.
Operational integrity
An epidemic is a moving target which requires a whole-of-government response. However, the platform established to make rapid decisions needs to be fit-for-purpose and regularly reviewed. It is presently unclear how effective the current command structure is. In particular, whether it is able to constantly adjust to changing circumstances and configurations of risk and priorities.
Conclusion
This brief has provided an overview of the possible trajectory of the COVID-19 disease in South Africa under different intervention scenarios using an intervention model. The purpose of the modelling approach is to support decision-making in the face of the complex set of risks facing the country in 2020, and possibly beyond.
The modelling analysis suggests that it is unlikely that the disease will be eliminated as a risk in 2020. Given the protracted nature of the emergency, the public health strategies need to be designed to be compatible with continued economic activity.
Were South Africa to rely exclusively on lockdowns to contain the epidemic, a total lockdown period of 193 days may be required. This assumes, however, that lockdowns actually work in the South African context. At this stage it cannot be confirmed that the lockdown approach works in the densely populated informal settlements and townships. A total lockdown period of 193 days is however inconceivable from an economic perspective, and an alternative risk-based approach is therefore appropriate.
A risk-based approach seeks to manage all the risks associated with the epidemic, and not only the disease itself. The current health strategy places the economic welfare of more than 70% of the population in jeopardy, with Government only in a position to provide remedial support to only a subset of the group at risk of destitution. The sustainability of the programmes of support also ultimately depend on the sustainability of government finances, which in turn depend on the existence of a working economy. A lockdown-dependent strategy substantially erodes the ability of Government to bridge the social and economic impacts.[13]
Given this, strategic decisions are required at this point in the emergency which favour a risk-based approach rather than a lockdown dependent approach. However, a risk-based approach requires that the groundwork is properly laid. It is far from clear, however, that this necessary work has been done. But there is still time. But much depends on what use is made of the limited time.
References
European Centre for Disease Prevention and Control. (2020). Geographic ditribution of COVID-19 cases worldwide. Retrieved from: https://www.ecdc.europa.eu/en/publications-data/download-todays-data-geographic-distribution-covid-19-cases-worldwide
Kim, H. J. (2020, 4 February 2020). South Korea learned its successful Covid-19 strategy from a previous coronavirus outbreak: MERS, Online article. Bulletin of the Atomic Scientists. Retrieved from https://thebulletin.org/2020/03/south-korea-learned-its-successful-covid-19-strategy-from-a-previous-coronavirus-outbreak-mers/
Liu, Y., Gayle, A. A., Wilder-Smith, A., & Rocklöv, J. (2020). The reproductive number of COVID-19 is higher compared to SARS coronavirus. Journal of Travel Medicine, 27(2). doi:10.1093/jtm/taaa021
van den Heever, A. (2020). COVID-19 Intervention Model for South Africa.
Zhang, S., Diao, M., Yu, W., Pei, L., Lin, Z., & Chen, D. (2020). Estimation of the reproductive number of novel coronavirus (COVID-19) and the probable outbreak size on the Diamond Princess cruise ship: A data-driven analysis. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases, 93, 201-204. doi:10.1016/j.ijid.2020.02.033
[1] There are numerous attempts to estimate R for COVID-1 (Liu, Gayle, Wilder-Smith, & Rocklöv, 2020; Zhang et al., 2020), Estimates do range from below 2 to around 3. The baseline assumption used in the report is merely used as the point-of-departure for assumed reductions in R due to interventions.
[2] This is where immunity levels are sufficiently high that R is always significantly below 1.
[3] The number of infected individuals totalled only 1,170 on 27 March 2020 when the lockdown began.
[4] See for instance (Kim, 2020)
[5] The United States was excluded as the lockdown is incomplete (or partial) and the peak of the epidemic has not been reached. It therefore cannot assist in the development of parameters for the model.
[6] Note that the South Korean data in Figure 1 is presented on a different scale to that for the other countries. This is because the size of the epidemic in Korea was far less than for the other countries, making it difficult to compare them side-by-side.
[7] The data source for international trends was from (European Centre for Disease Prevention and Control, 2020).
[8] The new infection data from China reflected so many inconsistencies however that it was necessary to smooth its upward trajectory. The new infection data from China has also been adjusted to iron out clear timing errors in reporting. This involved developing a linear equation for a period of apparent consistent reporting and extrapolating for the period of inconsistent reporting. The total number of infections was however retained. Only the trajectories were smoothed.
[9] These reductions in R effectively work back from the overall R totals developed using the Italian and South Korean epidemics.
[10] The 2.2 assumption is lower than the assumed average in cold climates of 2.43. The reduction from this baseline of approximately 0.3 is to account for the warmer climate at this time in South Africa.
[11] While this is shorter than the official intervention period, it is assumed that actual social distancing occurred with a lag of a few days.
[12] This is however subject to the release of public information indicating whether there are any fatal bottlenecks to the timeous expansion of testing to the scale required to manage the epidemic.
[13] It is worth noting that conventional views of deficit-financing rescue packages don’t fully apply to the current economic situation. The indefinite closure of businesses raises the uncomfortable prospect that the sale of government treasury bills could dry up – leaving the Government in a state of default. Virtually every revenue source for Government is compromised by a lockdown. Maintaining a posture of uncertainty regarding future lockdowns clearly places government finances in an untenable position. It should also be noted that industrialised countries can withstand these circumstances for a far longer period than South Africa.
Professor Alex van den Heever holds the Chair in the field of Social Security Systems Administration and Management Studies at the Wits School of Governance. This paper has been published in full on Maverick Citizen/Daily Maverick.